
Multimodal Imaging in Idiopathic Neuroretinitis with Localized Choroidal Insufficiency: A Case Report


{kind=link}
{kind=link}
Abstract
:1. Introduction
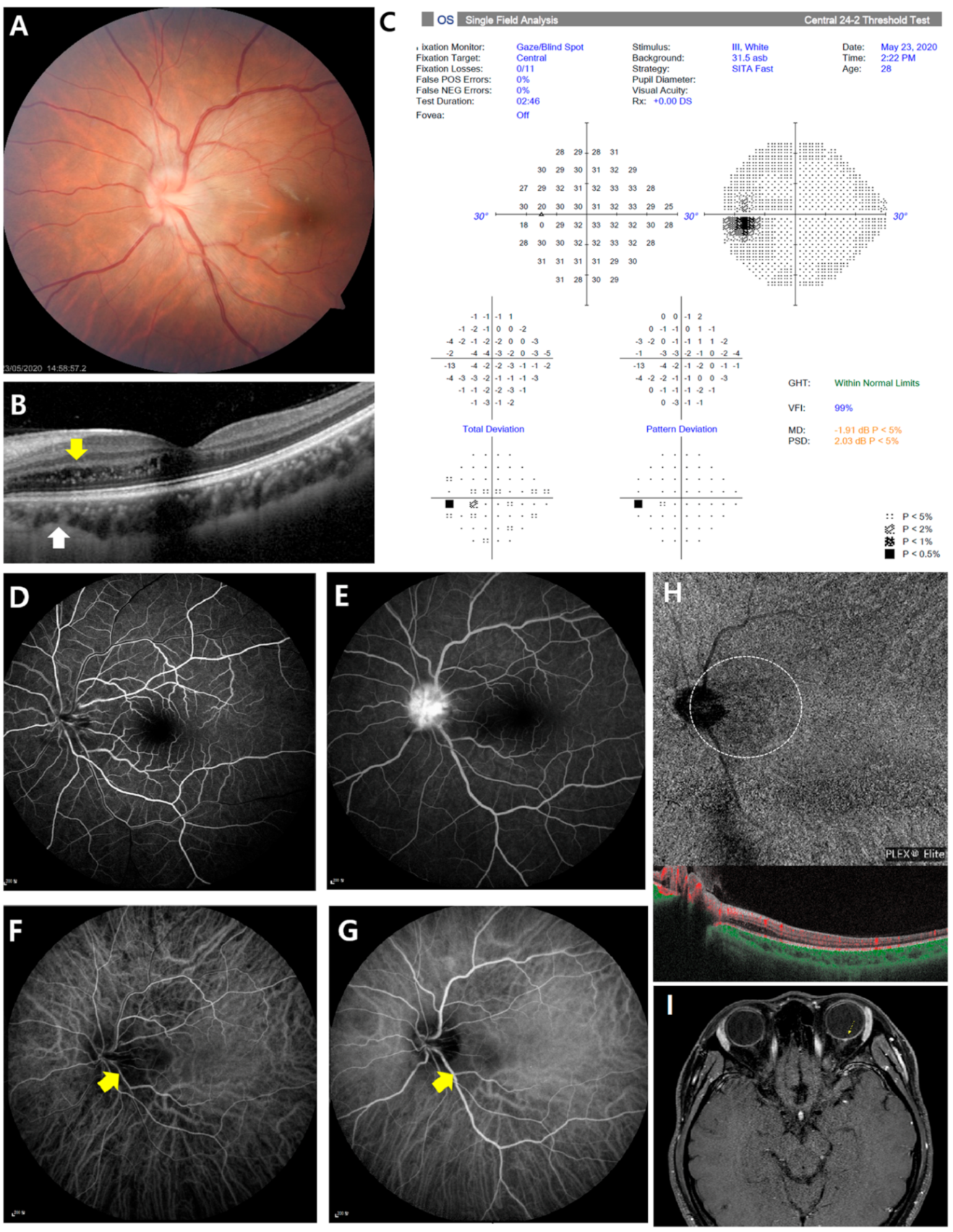
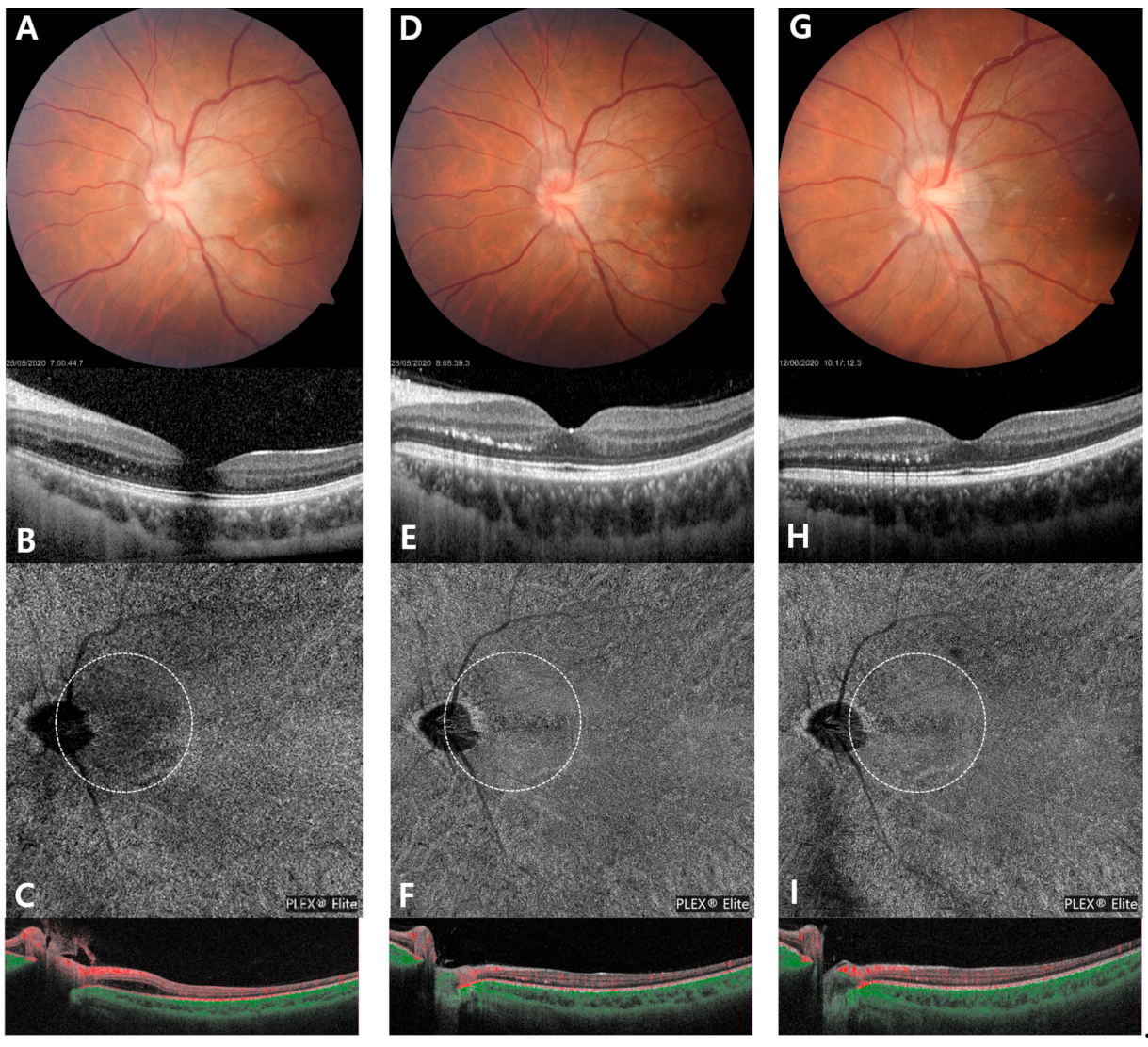
2. Case Presentation
3. Discussion and Conclusions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Maitland, C.G.; Miller, N.R. Neuroretinitis. Arch. Ophthalmol. 1984, 102, 1146–1150. [Google Scholar] [CrossRef] [PubMed]
- Purvin, V.; Sundaram, S.; Kawasaki, A. Neuroretinitis: Review of the Literature and New Observations. J. Neuro Ophthalmol. 2011, 31, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, R.F.; Hopen, G.; Gass, J.D.M.; Smith, J.L. Leber’s Idiopathic Stellate Neuroretinitis. Arch. Ophthalmol. 1984, 102, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Sunil, K.N.; Subashini, K.; Renuka, S. Neuroretinitis, a great mimicker. Ann. Indian Acad. Neurol. 2008, 11, 109–113. [Google Scholar]
- Matsuo, T.; Sato, Y.; Shiraga, F.; Shiragami, C.; Tsuchida, Y. Choroidal abnormalities in behçet disease observed by simultaneous indocyanine green and fluorescein angiography with scanning laser ophthalmoscopy. Ophthalmology 1999, 106, 295–300. [Google Scholar] [CrossRef]
- Herbort, C.P.; LeHoang, P.; Guex-Crosier, Y. Schematic interpretation of indocyanine green angiography in posterior uveitis using a standard angiographic protocol. Ophthalmology 1998, 105, 432–440. [Google Scholar] [CrossRef]
- Singh, R.P.; Tsai, G.; Banaee, T.; Conti, F.F. Optical coherence tomography angiography in eyes with retinal vein occlusion. J. Ophthalmic Vis. Res. 2018, 13, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Sarraf, D.; Freund, K.B.; Sadda, S.R. OCT angiography and evaluation of the choroid and choroidal vascular disorders. Prog. Retin. Eye Res. 2018, 67, 30–55. [Google Scholar] [CrossRef] [PubMed]
- Yuya, E.; Yoshio, H.; Yusuke, Y.; Taneto, T.; Norihiro, S.; Tsutomu, Y.; Yuchiro, O. Multimodal Imaging in a Case of Idiopathic Neuroretinitis. Case Rep. Ophthalmol. 2018, 9, 487–492. [Google Scholar]
- Aliaa, A.; Nailyn, R. Neuroretinitis: A review. Curr. Opin. Ophthalmol. 2018, 29, 514–519. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Kim, K. Multimodal Imaging in Idiopathic Neuroretinitis with Localized Choroidal Insufficiency: A Case Report. Medicina 2021, 57, 697. https://doi.org/10.3390/medicina57070697
Lee J, Kim K. Multimodal Imaging in Idiopathic Neuroretinitis with Localized Choroidal Insufficiency: A Case Report. Medicina. 2021; 57(7):697. https://doi.org/10.3390/medicina57070697
Chicago/Turabian StyleLee, Junwoo, and Kiyoung Kim. 2021. "Multimodal Imaging in Idiopathic Neuroretinitis with Localized Choroidal Insufficiency: A Case Report" Medicina 57, no. 7: 697. https://doi.org/10.3390/medicina57070697
APA StyleLee, J., & Kim, K. (2021). Multimodal Imaging in Idiopathic Neuroretinitis with Localized Choroidal Insufficiency: A Case Report. Medicina, 57(7), 697. https://doi.org/10.3390/medicina57070697