Relationship between Food Dependence and Nicotine Dependence in Smokers: A Cross-Sectional Study of Staff and Students at Medical Colleges

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
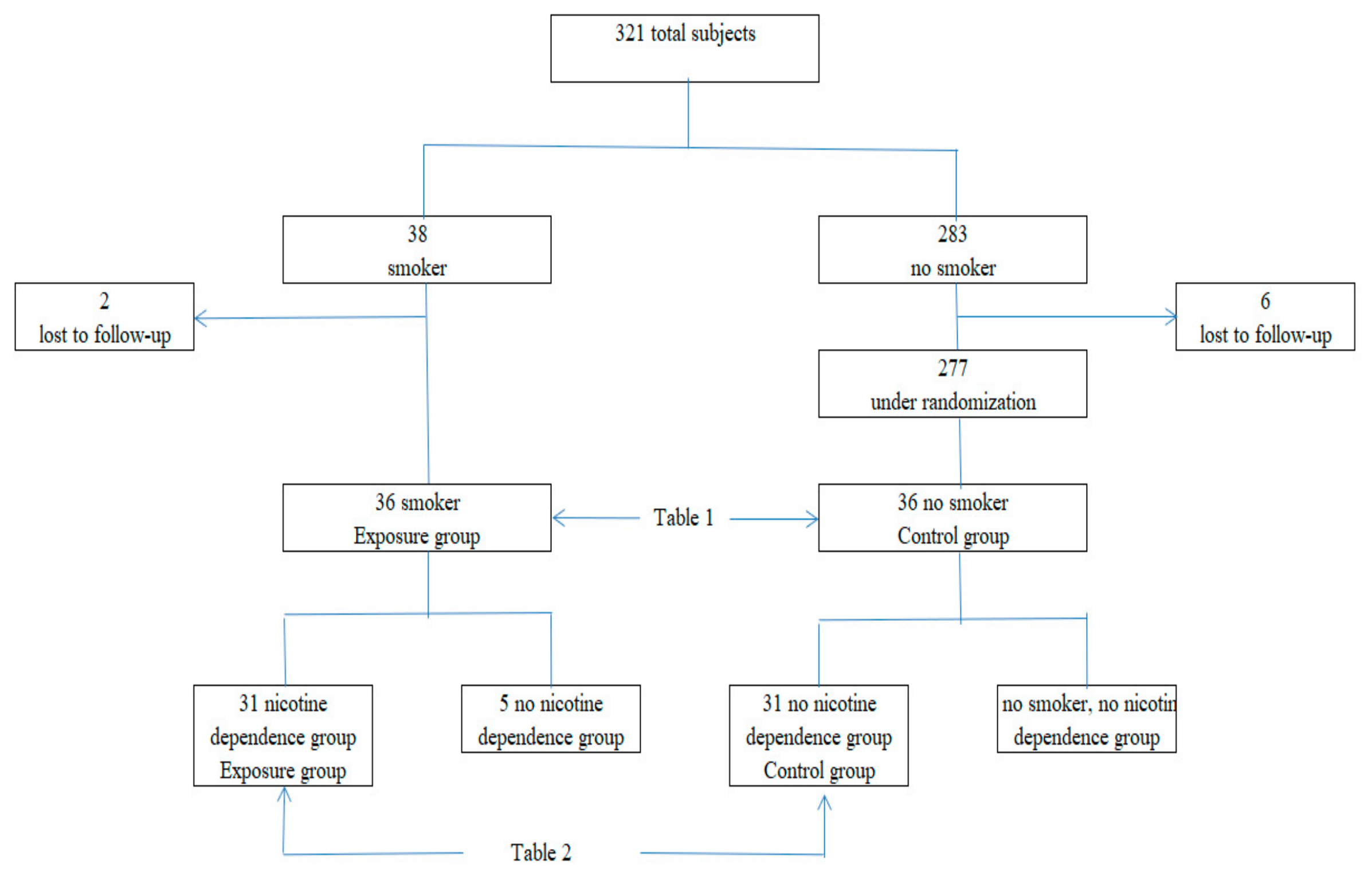
2.2. Subjects
2.3. Clinical Parameters and Measurements
2.4. Smoking Habits
2.5. Nicotine Dependence
2.6. Food Dependence
2.7. Time Discount Rate
2.8. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ministry of Health, Labor and Welfare. Available online: http://www.mhlw.go.jp/file/05-Shingikai-10901000-Kenkoukyoku-Soumuka/0000172687.pdf (accessed on 1 April 2019).
- Mitchell, S.H. Measures of imtpulsivity in cigarette smokers and non-smokers. Psychopharmacology 1999, 146, 455–464. [Google Scholar]
- Kuriyama, S.; Tsuji, I.; Ohkubo, T.; Anzai, Y.; Takahashi, K.; Watanabe, Y; Nishino, Y.; Hisamichi, S. Medical care expenditure associated with body mass index in Japan: The Ohsaki Study. Int. Obes. Relat. Metab. Disord. 2002, 26, 1069–1074. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Alan, J.F. Food-addiction scale measurement in 2 cohorts of middle-aged and older women. Am. J. of Clin. Nur. 2014, 99, 578–586. [Google Scholar]
- Odum, A.L.; Madden, G.J.; Bickel, W.K. Discounting of delayed health gains and losses by current, never-and ex-smokers of cigarettes. Nicotine Tob. Res. 2002, 4, 295–303. [Google Scholar] [CrossRef]
- Baker, F.; Johnson, M.W.; Bickel, W.K. Delay discounting in current and never-before cigarette smokers: Similarities and differences across commodity, sign, and magnitude. J. Abnorm. Psychol. 2003, 112, 382–392. [Google Scholar]
- Reynolds, B.; Karraker, K.; Horn, K.; Richards, J.B. Delay and probability discounting as related to different stages of adolescent smoking and non-smoking. Behav. Process. 2003, 64, 333–344. [Google Scholar] [CrossRef]
- Komlos, J.; Smith, P.K.; Bogin, B. Obesity and the rate of time preference: Is there a connection? J. Biosoc. Sci. 2004, 36, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Borghans, L.; Golsteyn, B. Time discounting and the body mass index: Evidence from the Netherlands. Econ. and Hum. Biol. 2006, 4, 39–61. [Google Scholar]
- Cutler, D.M.; Glaeser, E. What explains differences in smoking, drinking, and other health-related behaviors. AER 2005, 95, 238–242. [Google Scholar] [CrossRef]
- Tang, D.W.; Fellws, L.K.; Small, D.M.; Dagher, A.D. Food and drug cues activate similar brains: A meta-analysis of functional MRI studies. Physiol. Behav. 2012, 3, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Nakamura, K.; Takano, T. Socioeconomic pattern of smoking in Japan: Income inequality and gender and age differences. Ann. Epidemiol. 2005, 15, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Pampel, F.C.; Denney, J.T. Cross-national sources of health inequality: Education and tobacco use in the World Health Survey. Demography 2011, 48, 653–674. [Google Scholar] [CrossRef]
- Hiscock, R.; Bauld, L.; Amos, A.; Filder, J.A.; Munafo, M. Socioeconomic status and smoking: A review. Ann. N. Y. Acad. Sci. 2012, 1248, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Lynn, R.; Julie, R.P.; Samuel, S. Decline in the Risk of Myocardial Infarction among Women Who Stop Smoking. N. Engl. J. Med. 1990, 322, 213–217. [Google Scholar]
- Hirayama, T. Life-Style and Mortality: A Large-Scale Census-Based Cohort Study in Japan. Life-Style and Mortality. Karger AG: Basel, Switzerland, 1990; Volume 6. [Google Scholar]
- Kawakami, N.; Takatsuka, N.; Inaba, S.; Shimizu, H. Development of a screening questionnaire for tobacco/nicotine according to ICD-10, DSM-III-R, and DSM-IV. Addict. Behav. 1999, 24, 155–166. [Google Scholar] [CrossRef]
- Brinkman, G.L.; Coates, E.O., Jr. The effect of bronchitis, smoking, and occupation on ventilation. Am. Rev. Respir. Dis. 1963, 87, 684–693. [Google Scholar]
- The Rudd Center. Available online: http://www.uconnruddcenter.org/resources/upload/docs/what/addiction/foodaddictionsale09.pdf (accessed on 1 April 2019).
- Gearhardt, A.N.; Corbin, W.R.; Brownell, K.D. Preliminary Validation of the Yale Food Addiction Scale. Appetite 2009, 52, 430–436. [Google Scholar] [CrossRef]
- Brunault, P.; Ballon, N.; Gaillard, P.; Reveillere, C.; Courtois, R. Validation of the French Version of the Yale Food Addiction Scale: An Examination of its Factor Structure, Reliability, and Construct Validity in a Nonclinical Sample. Can. J. Psychiat. 2014, 59, 276–284. [Google Scholar] [CrossRef]
- Ohnishi, M. Processed foods are prone to addiction, 2015. Available online: http://trendy.nikkeibp.co.jp/article/column/20150305/1062986/?rt=nocnt. (accessed on 1 April 2019).
- Samuelson, P. A note on measurement of utility. Rev Econ. Stud. 1937, 4, 155–161. [Google Scholar] [CrossRef]
- Casey, B.J.; Somerville, L.H.; Gotlib, I.H.; Ayduk, O.; Franklin, N.T.; Askren, M.K.; Jonides, J.; Berman, M.G.; Wilson, N.L.; Teslovich, T.; et al. Behavioral and neural correlates of delay of gratification 40 years later. Proc. Natl. Acad. Sci. USA 2011, 108, 14998–15003. [Google Scholar] [CrossRef] [PubMed]
- Daw, N.D.; Kakade, S.; Dayan, P. Opponent interactions between serotonin and dopamine. Neural Netw. 2002, 15, 603–616. [Google Scholar] [CrossRef]
- Tanaka, S. Computational model of dopamine in decision making. Jpn. J. Biol. Psychiat. 2013, 24, 80–88. [Google Scholar]
- Efron, B. Bootstrap methods: Another look at the jackknife. Ann. Stat. 1979, 7, 1–26. [Google Scholar] [CrossRef]
- Arnaud, C.; David, F.P.; Jacques, C. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am. J. Nutr. 2008, 87, 801–809. [Google Scholar]
- Ariana, M.C.; Marney, A.W.; Carlos, M.G.; Rajita, S. Examining the effects of cigarette smoking on food cravings and intake, depressive symptoms, and stress. Eat. Behav. 2016, 24, 61–65. [Google Scholar]
- Eliza, L.G.; Aiva, H.A.D.; Viviana, B.; Lisa, J.M. What is the evidence for “food addiction?” A systematic review. Nutrients 2018, 10, 477. [Google Scholar]
- Mason, S.M.; Flint, A.J.; Field, A.E.; Austin, S.; Rich-Edwards, J.W. Abuse victimization in childhood or adolescence and risk of food addiction in adult women. Obesity 2013, 21, E775–E781. [Google Scholar] [CrossRef]
- Flint, A.J.; Gearhardt, A.; Corbin, W.; Brownell, K.; Field, A.; Rimm, E. Food addiction scale measurement in two cohorts of middleaged and older women. Am. J. Clin. Nutr. 2014, 99, 578–586. [Google Scholar] [CrossRef]


{kind=link}
| Total | Smoking | Nonsmoking | Welch’s t-test | |||||
| Number of subjects | 36 | 36 | ||||||
| Age (years) | 41.7 | ± | 17.7 | 40.4 | ± | 20.0 | ||
| Body mass index (BMI) (kg/m2) | 22.2 | ± | 3.0 | 22.4 | ± | 3.7 | ||
| Food dependence | 4.7 | ± | 6.1 | 2.1 | ± | 2.0 | 0.0411 | |
| Time discount rate (%) | 11.3 | ± | 19.7 | 2.4 | ± | 2.4 | 0.0107 | |
| Brinkman index | 334.3 | ± | 323.4 | |||||
| Tobacco dependence screener (TDS) | 5.9 | ± | 2.6 | |||||
| Nicotine dependence (presence) | 31 | |||||||
| Income (/year) (number) | 1:15, 2:19, 3:2 | |||||||
| Educational background (number) | 1:26, 2:10 | |||||||
| Men | Smoking | Nonsmoking | Welch’s t-test | |||||
| Number of subjects | 24 | 24 | ||||||
| Age (years) | 37.4 | ± | 16.6 | 36.3 | ± | 19.1 | ||
| Body mass index (BMI) (kg/m2) | 22.5 | ± | 3.1 | 22.4 | ± | 3.7 | ||
| Food dependence | 4.0 | ± | 4.7 | 2.0 | ± | 2.1 | 0.0490 | |
| Time discount rate (%) | 9.0 | ± | 14.3 | 2.9 | ± | 2.6 | 0.0107 | |
| Brinkman index | 327.9 | ± | 336.2 | |||||
| Tobacco dependence screener (TDS) | 5.9 | ± | 2.9 | |||||
| Nicotine dependence (presence) | 19 | |||||||
| Income (/year) (number) | 1:11, 2:12, 3:1 | |||||||
| Education background (number) | 1:18, 2:6 | |||||||
| Women | Smoking | Nonsmoking | Mann–Whitney U test | |||||
| Number of subjects | 12 | 12 | ||||||
| Age (years) | 49.3 | ± | 17.6 | 48.8 | ± | 19.1 | ||
| Body mass index (BMI) (kg/m2) | 21.7 | ± | 3.1 | 22.4 | ± | 3.7 | ||
| Food dependence | 6.2 | ± | 8.1 | 2.3 | ± | 2.4 | 0.3618 | |
| Time discount rate (%) | 15.9 | ± | 27.8 | 1.4 | ± | 1.6 | 0.0427 | |
| Brinkman index | 347.3 | ± | 310.2 | |||||
| Tobacco dependence screener (TDS) | 5.9 | ± | 1.9 | |||||
| Nicotine dependence (presence) | 12 | |||||||
| Income (/year) (number) | 1:4, 2:7, 3:1 | |||||||
| Educational background (number) | 1:8, 2:4 | |||||||
| Total | Nicotine dependence | No nicotine dependence | Welch’s t-test | |||||
| Number of subjects | 31 | 31 | ||||||
| Age (years) | 44.1 | ± | 17.4 | 43.4 | ± | 20.3 | ||
| body mass index (BMI) (kg/m2) | 22.3 | ± | 3.1 | 22.6 | ± | 3.8 | ||
| Food dependency tendency | 4.6 | ± | 6.3 | 2.0 | ± | 2.1 | 0.0370 | |
| Time discount rate (%) | 12.3 | ± | 2.1 | 2.3 | ± | 2.1 | 0.0133 | |
| Brinkman index | 377.0 | ± | 328.2 | |||||
| Tobacco dependence screener (TDS) | 6.4 | ± | 2.4 | |||||
| Nicotine dependence (presence) | 31 | |||||||
| Income (/year) (number) | 1: 11, 2: 18, 3: 2 | |||||||
| Educational background (number) | 1: 21, 2: 10 | |||||||
| Men | Nicotine dependence | No nicotine dependence | Mann–Whitney U test | |||||
| Number of subjects | 19 | 19 | ||||||
| Age (years) | 40.8 | ± | 17.0 | 39.5 | ± | 20.1 | ||
| body mass index (BMI) (kg/m2) | 22.6 | ± | 3.2 | 22.7 | ± | 4.0 | ||
| Food dependence | 3.6 | ± | 4.8 | 1.6 | ± | 1.8 | 0.0489 | |
| Time discount rate (%) | 9.9 | ± | 15.8 | 2.8 | ± | 2.3 | 0.0434 | |
| Brinkman index | 395.8 | ± | 346.2 | |||||
| Tobacco dependence screener (TDS) | 6.6 | ± | 2.7 | |||||
| Nicotine dependence (presence) | 19 | |||||||
| Income (/year) (number) | 1: 7, 2: 11, 3:1 | |||||||
| Education background (number) | 1: 13, 2: 6 | |||||||
| Women (smoking = nicotine dependence) | Nicotine dependence | No nicotine dependence | Mann–Whitney U test | |||||
| Number of subjects | 12 | 12 | ||||||
| Age (years) | 49.3 | ± | 17.6 | 48.8 | ± | 19.1 | ||
| body mass index (BMI) (kg/m2) | 21.7 | ± | 3.1 | 22.4 | ± | 3.7 | ||
| Food dependence | 6.2 | ± | 8.1 | 2.3 | ± | 2.4 | 0.3618 | |
| Time discount rate (%) | 15.9 | ± | 27.8 | 1.4 | ± | 1.6 | 0.0427 | |
| Brinkman index | 347.3 | ± | 310.2 | |||||
| Tobacco dependence screener (TDS) | 5.9 | ± | 1.9 | |||||
| Nicotine dependence (presence) | 12 | |||||||
| Income (/year) (number) | 1: 4, 2: 7, 3: 1 | |||||||
| Education background (number) | 1: 8, 2: 4 | |||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owari, Y.; Miyatake, N.; Suzuki, H. Relationship between Food Dependence and Nicotine Dependence in Smokers: A Cross-Sectional Study of Staff and Students at Medical Colleges. Medicina 2019, 55, 202. https://doi.org/10.3390/medicina55050202
Owari Y, Miyatake N, Suzuki H. Relationship between Food Dependence and Nicotine Dependence in Smokers: A Cross-Sectional Study of Staff and Students at Medical Colleges. Medicina. 2019; 55(5):202. https://doi.org/10.3390/medicina55050202
Chicago/Turabian StyleOwari, Yutaka, Nobuyuki Miyatake, and Hiromi Suzuki. 2019. "Relationship between Food Dependence and Nicotine Dependence in Smokers: A Cross-Sectional Study of Staff and Students at Medical Colleges" Medicina 55, no. 5: 202. https://doi.org/10.3390/medicina55050202
APA StyleOwari, Y., Miyatake, N., & Suzuki, H. (2019). Relationship between Food Dependence and Nicotine Dependence in Smokers: A Cross-Sectional Study of Staff and Students at Medical Colleges. Medicina, 55(5), 202. https://doi.org/10.3390/medicina55050202