
Clinical Investigation of Leukocyte DNA Damage in COVID-19 Patients

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Total Mononuclear Cell Isolation
2.2. DNA Damage Analysis
2.3. Statistical Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel. Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID-19 Response Team. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)-United States, February 12-March 16, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.M.; Brigham, E.; Connolly, B.; McPeake, J.; Agranovich, A.V.; Kenes, M.T.; Casey, K.; Reynolds, C.; Schmidt, K.F.; Kim, S.Y.; et al. Addressing the post-acute sequelae of SARS-CoV-2 infection: A multidisciplinary model of care. Lancet Respir. Med. 2021, 9, 1328–1341. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yang, L. Post-acute Sequelae of SARS-CoV-2 Infection: A Neglected Public Health Issue. Front. Public Health 2022, 10, 908757. [Google Scholar] [CrossRef]
- Henry, B.M. COVID-19, ECMO, and lymphopenia: A word of caution. Lancet Respir. Med. 2020, 8, e24. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Tao, Z.W.; Wang, L.; Yuan, M.L.; Liu, K.; Zhou, L.; Wei, S.; Deng, Y.; Liu, J.; Liu, H.G.; et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin. Med. J. (Engl.) 2020, 133, 1032–1038. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, Y.; Zhang, C.; Huang, F.; Wang, F.; Yuan, J.; Wang, Z.; Li, J.; Li, J.; Feng, C.; et al. Clinical and biochemical indexes from 2019-nCoV infected patients linked to viral loads and lung injury. Sci. China Life Sci. 2020, 63, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Thevarajan, I.; Nguyen, T.H.O.; Koutsakos, M.; Druce, J.; Caly, L.; van de Sandt, C.E.; Jia, X.; Nicholson, S.; Catton, M.; Cowie, B.; et al. Breadth of concomitant immune responses prior to patient recovery: A case report of non-severe COVID-19. Nat. Med. 2020, 26, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef] [PubMed]
- Kerget, B.; Çelik, E.; Kerget, F.; Aksakal, A.; Uçar, E.Y.; Araz, Ö.; Akgün, M. Evaluation of 3-month follow-up of patients with postacute COVID-19 syndrome. J. Med. Virol. 2022, 94, 2026–2034. [Google Scholar] [CrossRef]
- Ahmad, R.; Haque, M. Surviving the Storm: Cytokine Biosignature in SARS-CoV-2 Severity Prediction. Vaccines 2022, 10, 614. [Google Scholar] [CrossRef]
- Fathi, N.; Rezaei, N. Lymphopenia in COVID-19: Therapeutic opportunities. Cell Biol. Int. 2020, 44, 1792–1797. [Google Scholar] [CrossRef] [PubMed]
- Basheer, M.; Saad, E.; Kananeh, M.; Asad, L.; Khayat, O.; Badarne, A.; Abdo, Z.; Arraf, N.; Milhem, F.; Bassal, T.; et al. Cytokine Patterns in COVID-19 Patients: Which Cytokines Predict Mortality and Which Protect Against? Curr. Issues Mol. Biol. 2022, 44, 4735–4747. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, B.; Li, Q.; Wen, L.; Zhang, R. Clinical Features of 69 Cases With Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Li, T.; Han, M.; Li, X.; Wu, D.; Xu, Y.; Zhu, Y.; Liu, Y.; Wang, X.; Wang, L. Diagnostic utility of clinical laboratory data determinations for patients with the severe COVID-19. J. Med. Virol. 2020, 92, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Mo, P.; Xing, Y.; Xiao, Y.; Deng, L.; Zhao, Q.; Wang, H.; Xiong, Y.; Cheng, Z.; Gao, S.; Liang, K.; et al. Clinical Characteristics of Refractory Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2021, 73, e4208–e4213. [Google Scholar] [CrossRef] [PubMed]
- Cameron, M.J.; Ran, L.; Xu, L.; Danesh, A.; Bermejo-Martin, J.F.; Cameron, C.M.; Muller, M.P.; Gold, W.L.; Richardson, S.E.; Poutanen, S.M.; et al. Interferon-mediated immunopathological events are associated with atypical innate and adaptive immune responses in patients with severe acute respiratory syndrome. J. Virol. 2007, 81, 8692–8706. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Hui, D.; Wu, A.; Chan, P.; Cameron, P.; Joynt, G.M.; Ahuja, A.; Yung, M.Y.; Leung, C.B.; To, K.F.; et al. A major outbreak of severe acute respiratory syndrome in Hong Kong. N. Engl. J. Med. 2003, 348, 1986–1994. [Google Scholar] [CrossRef]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 33. [Google Scholar] [CrossRef]
- El-Amine, R.; Germini, D.; Zakharova, V.V.; Tsfasman, T.; Sheval, E.V.; Louzada, R.A.N.; Dupuy, C.; Bilhou-Nabera, C.; Hamade, A.; Najjar, F.; et al. HIV-1 Tat protein induces DNA damage in human peripheral blood B-lymphocytes via mitochondrial ROS production. Redox Biol. 2018, 15, 97–108. [Google Scholar] [CrossRef]
- Bhargava, A.; Khan, S.; Panwar, H.; Pathak, N.; Punde, R.P.; Varshney, S.; Mishra, P.K. Occult hepatitis B virus infection with low viremia induces DNA damage, apoptosis and oxidative stress in peripheral blood lymphocytes. Virus Res. 2010, 153, 143–150. [Google Scholar] [CrossRef]
- Harper, J.W.; Elledge, S.J. The DNA damage response: Ten years after. Mol. Cell 2007, 28, 739–745. [Google Scholar] [CrossRef]
- Jackson, S.P.; Bartek, J. The DNA-damage response in human biology and disease. Nature 2009, 461, 1071–1078. [Google Scholar] [CrossRef]
- Karaşör, Ö.F.; Bucak, M.N.; Cenariu, M.; Bodu, M.; Taşpınar, M.; Taşpınar, F. The Effects of Different Doses of ROCK Inhibitor, Antifreeze Protein III, and Boron Added to Semen Extender on Semen Freezeability of Ankara Bucks. Molecules 2022, 27, 8070. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, C.; Rapti, V.; Stellas, D.; Stefanou, D.T.; Syrigos, K.; Pavlakis, G.N.; Souliotis, V.L. Delineating the SARS-CoV-2 Induced Interplay between the Host Immune System and the DNA Damage Response Network. Vaccines 2022, 10, 1764. [Google Scholar] [CrossRef]
- Ghaebi, M.; Tahmasebi, S.; Jozghorbani, M.; Sadeghi, A.; Thangavelu, L.; Zekiy, A.O.; Esmaeilzadeh, A. Risk factors for adverse outcomes of COVID-19 patients: Possible basis for diverse responses to the novel coronavirus SARS-CoV-2. Life Sci. 2021, 277, 119503. [Google Scholar] [CrossRef]
- Gu, X.; Sha, L.; Zhang, S.; Shen, D.; Zhao, W.; Yi, Y. Neutrophils and Lymphocytes Can Help Distinguish Asymptomatic COVID-19 From Moderate COVID-19. Front. Cell. Infect. Microbiol. 2021, 11, 654272. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Mittal, S.; Gollapudi, S.; Butzmann, A.; Kumar, J.; Ohgami, R.S. A meta-analysis of SARS-CoV-2 patients identifies the combinatorial significance of D-dimer, C-reactive protein, lymphocyte, and neutrophil values as a predictor of disease severity. Int. J. Lab. Hematol. 2021, 43, 324–328. [Google Scholar] [CrossRef]
- Han, H.; Xu, Z.; Cheng, X.; Zhong, Y.; Yuan, L.; Wang, F.; Li, Y.; Liu, F.; Jiang, Y.; Zhu, C.; et al. Descriptive, Retrospective Study of the Clinical Characteristics of Asymptomatic COVID-19 Patients. mSphere 2020, 5, e00922-20. [Google Scholar] [CrossRef] [PubMed]
- Tomo, S.; Karli, S.; Dharmalingam, K.; Yadav, D.; Sharma, P. The Clinical Laboratory: A Key Player in Diagnosis and Management of COVID-19. EJIFCC 2020, 31, 326–346. [Google Scholar]
- Jia, Z.; Gong, W. Will Mutations in the Spike Protein of SARS-CoV-2 Lead to the Failure of COVID-19 Vaccines? J. Korean Med. Sci. 2021, 36, e124. [Google Scholar] [CrossRef]
- Sharma, A.; Ahmad Farouk, I.; Lal, S.K. COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses 2021, 13, 202. [Google Scholar] [CrossRef]
- Zella, D.; Giovanetti, M.; Cella, E.; Borsetti, A.; Ciotti, M.; Ceccarelli, G.; D’Ettorre, G.; Pezzuto, A.; Tambone, V.; Campanozzi, L.; et al. The importance of genomic analysis in cracking the coronavirus pandemic. Expert Rev. Mol. Diagn. 2021, 21, 547–562. [Google Scholar] [CrossRef] [PubMed]
- Machhi, J.; Herskovitz, J.; Senan, A.M.; Dutta, D.; Nath, B.; Oleynikov, M.D.; Blomberg, W.R.; Meigs, D.D.; Hasan, M.; Patel, M.; et al. The Natural History, Pathobiology, and Clinical Manifestations of SARS-CoV-2 Infections. J. Neuroimmune Pharmacol. 2020, 15, 359–386. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Control (n = 42) | Study (n = 50) | p Value |
|---|---|---|---|
| Sex, n (I%) | |||
| Male | 31 (73.8) | 30 (60.0) | 0.120 a |
| Female | 11 (26.2) | 20 (40.0) | |
| Age (Year) | 59.29 ± 16.99 | 62.36 ± 18.18 | 0.408 b |
| WBC (103/μL) | 9.38 ± 5.02 | 10.08 ± 4.18 | 0.116 c |
| RBC (106/μL) | 3.60 ± 0.80 | 4.56 ± 0.76 | <0.05 c |
| HGB (g/dL) | 10.24 ± 2.25 | 12.91 ± 2.09 | <0.05 c |
| NEU (103/μL) | 6.51 ± 4.38 | 8.45 ± 4.15 | <0.05 b |
| LYM (103/μL) | 1.72 ± 0.73 | 0.99 ± 0.86 | <0.05 c |
| EO (103/μL) | 0.29 ± 0.69 | 0.03 ± 0.07 | <0.05 c |
| MONO (103/μL) | 0.83 ± 0.55 | 0.53 ± 0.29 | <0.05 b |
| BASO (103/μL) | 0.04 ± 0.08 | 0.02 ± 0.02 | 0.645 c |
| PLT (103/μL) | 226.67 ± 95.54 | 236.88 ± 79.49 | 0.577 b |
| NLR (Ratio) | 4.61 ± 3.79 | 15.62 ± 17.56 | <0.05 c |
| Group | Control (n = 42) | Study (n = 50) | p Value a |
|---|---|---|---|
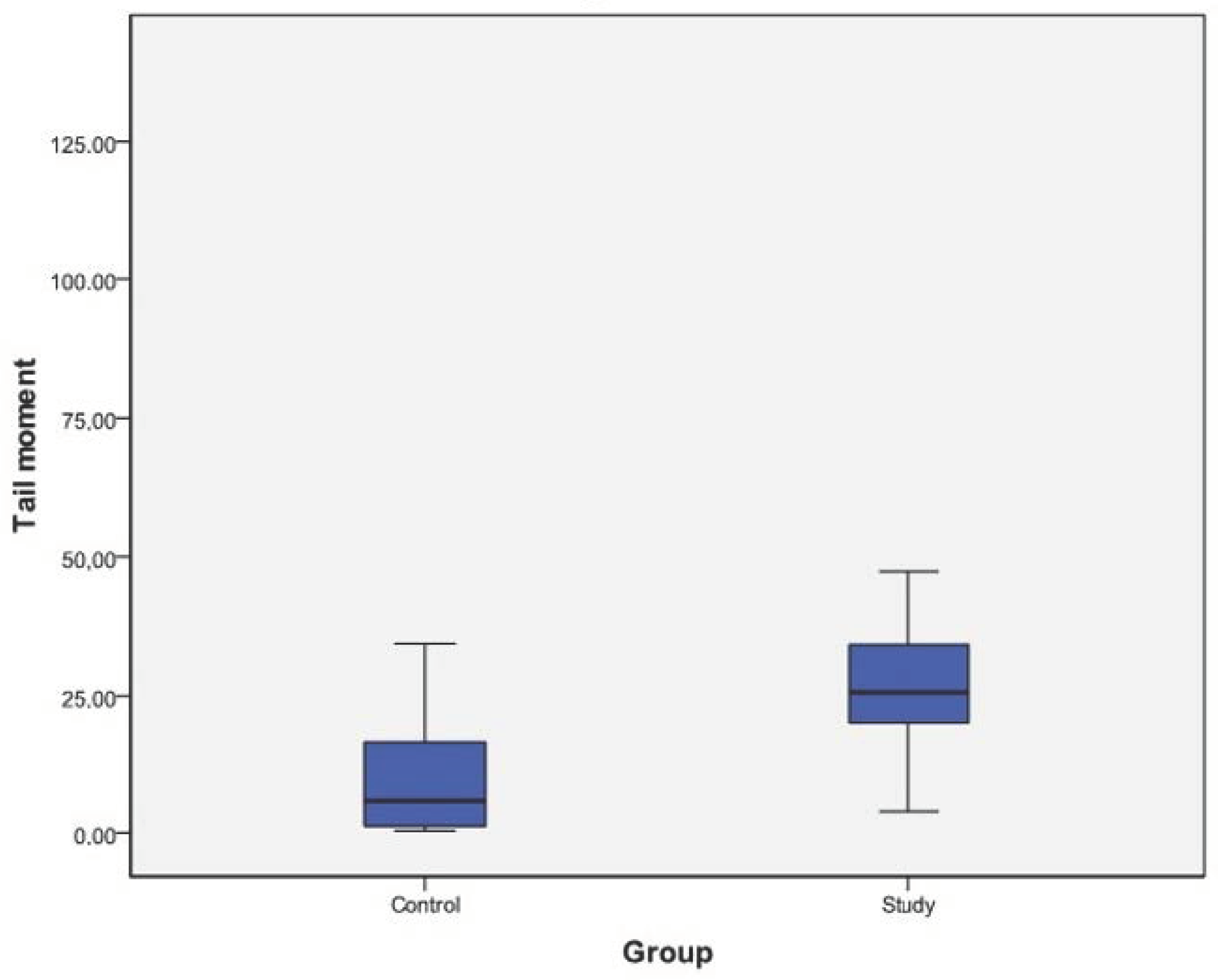
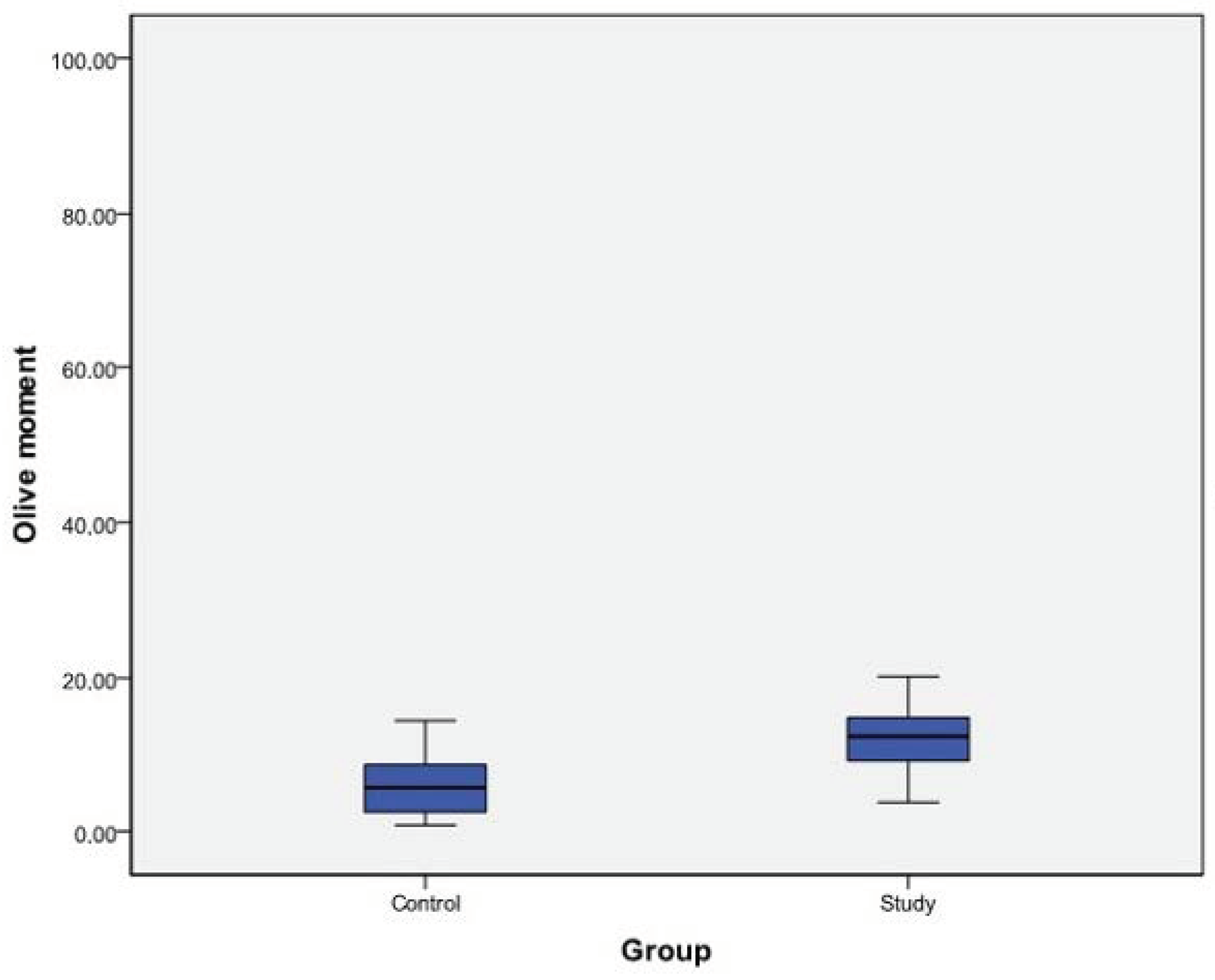
| Tail moment | 10.30 ± 11.38 | 30.00 ± 21.21 | <0.05 |
| Olive moment | 5.99 ± 4.28 | 13.87 ± 11.64 | <0.05 |
| Group | r | p |
|---|---|---|
| RBC (106/μL) | −0.863 ** | <0.05 |
| HGB (g/dL) | 0.863 ** | <0.05 |
| NEU (103/μL) | 0.307 ** | <0.05 |
| LYM (103/μL) | −0.542 ** | <0.05 |
| EO (103/μL) | −0.686 ** | <0.05 |
| MONO (103/μL) | −0.385 ** | <0.05 |
| Tail moment | 0.598 ** | <0.05 |
| Olive moment | 0.582 ** | <0.05 |
| NLR (Ratio) | 0.525 ** | <0.05 |
| Tail Moment | Olive Moment | |
|---|---|---|
| COVID-19 | 0.598 ** | 0.582 ** |
| Sex | 0.058 | 0.107 |
| Age (Year) | 0.018 | 0.057 |
| WBC (103/μL) | 0.147 | 0.210 * |
| RBC (106/μL) | −0.489 ** | −0.484 ** |
| HGB (g/dL) | 0.573 ** | 0.535 ** |
| NEU (103/μL) | 0.201 | 0.263 * |
| LYM (103/μL) | −0.288 ** | −0.281 ** |
| EO (103/μL) | −0.373 ** | −0.385 ** |
| MONO (103/μL) | −0.154 | −0.124 |
| BASO (103/μL) | 0.062 | 0.075 |
| PLT (103/μL) | −0.054 | −0.075 |
| NLR (Ratio) | 0.297 ** | 0.330 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doğan, H.; Kara, A.; Çankaya, E.; Balkan, E.; Gürbüz, M.A.; Kızılkaya, M.; Aykaç, M. Clinical Investigation of Leukocyte DNA Damage in COVID-19 Patients. Curr. Issues Mol. Biol. 2023, 45, 963-974. https://doi.org/10.3390/cimb45020062
Doğan H, Kara A, Çankaya E, Balkan E, Gürbüz MA, Kızılkaya M, Aykaç M. Clinical Investigation of Leukocyte DNA Damage in COVID-19 Patients. Current Issues in Molecular Biology. 2023; 45(2):963-974. https://doi.org/10.3390/cimb45020062
Chicago/Turabian StyleDoğan, Hasan, Aslı Kara, Erdem Çankaya, Eda Balkan, Muhammet Ali Gürbüz, Murat Kızılkaya, and Merve Aykaç. 2023. "Clinical Investigation of Leukocyte DNA Damage in COVID-19 Patients" Current Issues in Molecular Biology 45, no. 2: 963-974. https://doi.org/10.3390/cimb45020062
APA StyleDoğan, H., Kara, A., Çankaya, E., Balkan, E., Gürbüz, M. A., Kızılkaya, M., & Aykaç, M. (2023). Clinical Investigation of Leukocyte DNA Damage in COVID-19 Patients. Current Issues in Molecular Biology, 45(2), 963-974. https://doi.org/10.3390/cimb45020062