
The Relevance of Pharmacokinetic Biomarkers in Response to Methadone Treatment: A Systematic Review

 , ,
, ,  , , and
, , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Desing and Registration
2.2. Search Strategy
2.3. Inclusion Criteria
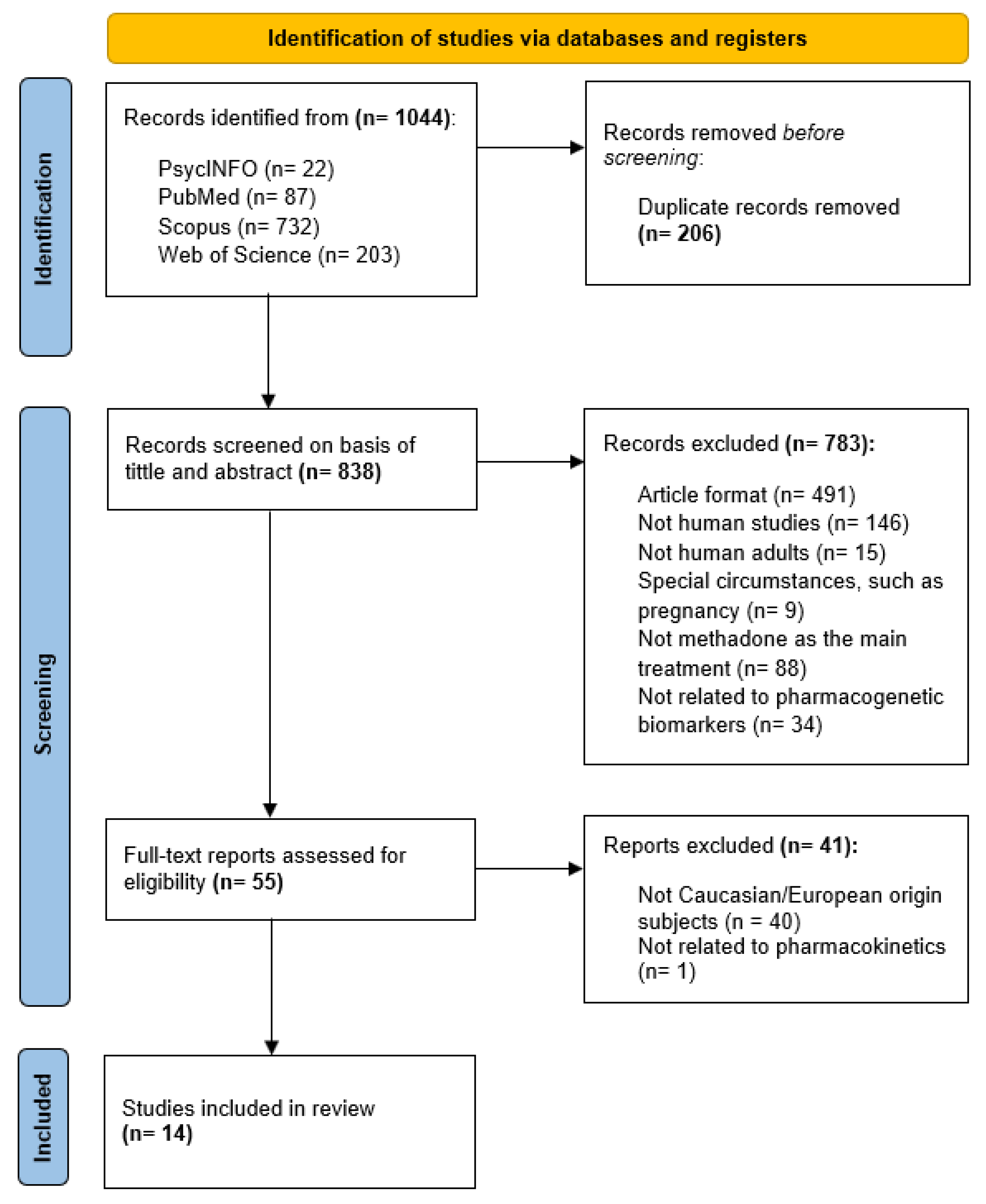
2.4. Screening Process and Study Selection
2.5. Assessment of Study Quality
2.6. Data Extraction
2.7. Data Analysis
3. Results
3.1. Characteristics of Included Articles
3.2. Patients Included
3.3. Assessment of Risk of Bias
3.4. Genetic Variants Analyzed
3.4.1. CYP2B6 Gene
3.4.2. ABCB1 Gene
3.4.3. CYP2D6 Gene
3.4.4. Other Assessed Genes: CYP3A4, CYP3A5, CYP1A2, CYP2C8, CYP2C9, CYP2C19, and UGT2B7
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OUD | Opioid use disorder |
| CBT | Cognitive Behavioral Therapy |
| CM | Contingency Management |
| MOR | µ-opioid receptor |
| NMDA | N-methyl-D-aspartate |
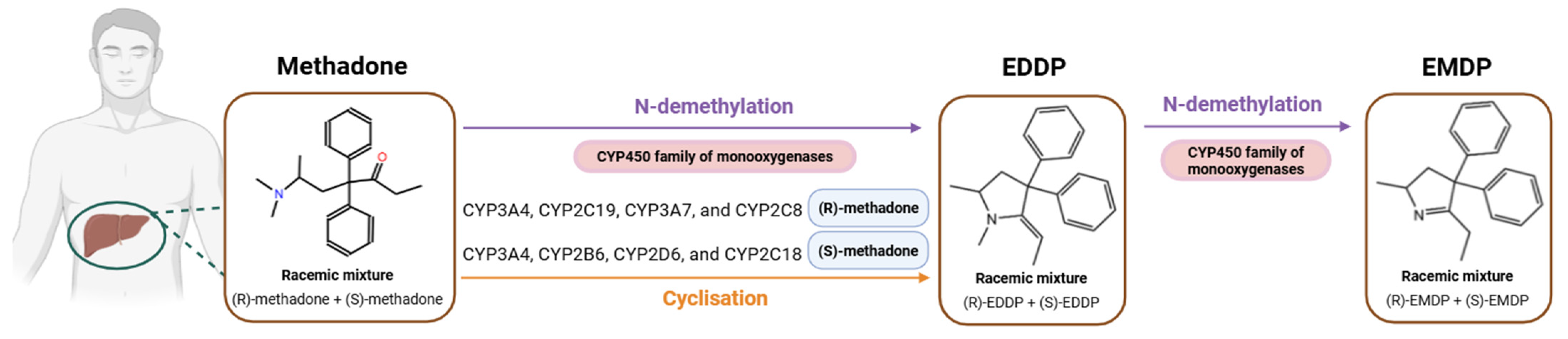
| CYP450 | Cytochrome P450 |
| EDDP | 2-ethylidene-1,5-dimethyl-3,3-diphenylpyrrolidine |
| EMDP | 2-ethyl-5-methyl-3,3-diphenyl-1-pyrroline |
| SNP | Single Nucleotide Polymorphism |
| GWAS | Genome-Wide Association Study |
| MMT | Methadone Maintenance Treatment |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| NHLBI | National Heart, Lung, and Blood Institute |
| QTc | QT interval of the cardiac cycle |
| SD | Standard deviation |
| UMs | Ultrarapid metabolizers |
| RMs | Rapid metabolizers |
| PMs | Poor metabolizers |
| IMs | Intermediate metabolizers |
| NMs | Normal metabolizers |
| ABC | ATP-binding cassette |
| CPIC® | Clinical Pharmacogenetics Implementation Consortium |
| PharmGKB | Pharmacogenomics Knowledge Base |
| POR | Cytochrome P450 oxidoreductase |
| NADPH | Nicotinamide adenine dinucleotide phosphate oxidase |
| PXR | Pregnane X receptor |
| MetS | Metabolic syndrome |
| AEMPS | Spanish Agency of Drugs and Medical Products |
References
- Savage, S.R.; Joranson, D.E.; Covington, E.C.; Schnoll, S.H.; Heit, H.A.; Gilson, A.M. Definitions related to the medical use of opioids: Evolution towards universal agreement. J. Pain. Symptom Manag. 2003, 26, 655–667. [Google Scholar] [CrossRef]
- Koob, G.F.; Le Moal, M. Plasticity of reward neurocircuitry and the ‘dark side’ of drug addiction. Nat. Neurosci. 2005, 8, 1442–1444. [Google Scholar] [CrossRef]
- Tiffany, S.T.; Wray, J.M. The clinical significance of drug craving. Ann. N. Y. Acad. Sci. 2012, 1248, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Bunachita, S.; Agarwal, A.A.; Lyon, A.; Patel, U.K. Opioid Use Disorder: Treatments and Barriers. Cureus 2021, 13, e13173. [Google Scholar] [CrossRef]
- Elman, I.; Borsook, D. Common Brain Mechanisms of Chronic Pain and Addiction. Neuron 2016, 89, 11–36. [Google Scholar] [CrossRef] [PubMed]
- Strang, J.; Volkow, N.D.; Degenhardt, L.; Hickman, M.; Johnson, K.; Koob, G.F.; Marshall, B.D.L.; Tyndall, M.; Walsh, S.L. Opioid use disorder. Nat. Rev. Dis. Prim. 2020, 6, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Elman, I.; Howard, M.; Borodovsky, J.T.; Mysels, D.; Rott, D.; Borsook, D.; Albanese, M. Metabolic and Addiction Indices in Patients on Opioid Agonist Medication-Assisted Treatment: A Comparison of Buprenorphine and Methadone. Sci. Rep. 2020, 10, 5617. [Google Scholar] [CrossRef]
- United Nations: Office on Drugs and Crime. World Drug Report 2024—Special Points of Interest. Available online: www.unodc.org/unodc/en/data-and-analysis/wdr2024-special-points-of-interest.html (accessed on 26 January 2025).
- Ministerio de Sanidad, Consumo y Bienestar Social. Memoria Plan Nacional sobre Drogas 2017. Disponible en. Available online: https://pnsd.sanidad.gob.es/pnsd/memorias/docs/2019_MEMORIA_2017.pdf (accessed on 26 January 2025).
- Sharma, B.; Bruner, A.; Barnett, G.; Fishman, M. Opioid Use Disorders. Child Adolesc. Psychiatr. Clin. 2016, 25, 473–487. [Google Scholar] [CrossRef]
- Panday, S.K.; Shankar, V.; Lyman, R.A.; Alexov, E. Genetic Variants Linked to Opioid Addiction: A Genome-Wide Association Study. Int. J. Mol. Sci. 2024, 25, 12516. [Google Scholar] [CrossRef]
- Gelernter, J.; Kranzler, H.R.; Sherva, R.; Koesterer, R.; Almasy, L.; Zhao, H.; Farrer, L.A. Genome-wide association study of opioid dependence: Multiple associations mapped to calcium and potassium pathways. Biol. Psychiatry 2014, 76, 66–74. [Google Scholar] [CrossRef]
- Koob, G.F.; Le Moal, M. Addiction and the brain antireward system. Annu. Rev. Psychol. 2008, 59, 29–53. [Google Scholar] [CrossRef] [PubMed]
- Santo, T.; Campbell, G.; Gisev, N.; Martino-Burke, D.; Wilson, J.; Colledge-Frisby, S.; Clark, B.; Tran, L.T.; Degenhardt, L. Prevalence of mental disorders among people with opioid use disorder: A systematic review and meta-analysis. Drug Alcohol Depend. 2022, 238, 109551. [Google Scholar] [CrossRef] [PubMed]
- Altable, M.; De la Serna, J.M.; Akram, M. Comorbidity in Opioid Addiction: A Brief Review. J. Drug Alcohol. Res. 2023, 12, 3–5. [Google Scholar] [CrossRef]
- Sofuoglu, M.; DeVito, E.E.; Carroll, K.M. Pharmacological and Behavioral Treatment of Opioid Use Disorder. Psychiatr. Res. Clin. Pr. 2018, 1, 4–15. [Google Scholar] [CrossRef]
- Kreek, M.J.; Borg, L.; Ducat, E.; Ray, B. Pharmacotherapy in the Treatment of Addiction: Methadone. J. Addict. Dis. 2010, 29, 200–216. [Google Scholar] [CrossRef]
- Sheen, S.; Choo, J.; Huh, B.; Chung, M. The effect of oral methadone on the QTc interval in cancer pain patients. Pain Manag. 2025, 15, 21–25. [Google Scholar] [CrossRef]
- McClain, M.R.; Subramaniam, K.; Cheema, R.; Lavage, D.R.; Lin, H.H.S.; Sultan, I.; Sadhasivam, S.; Howard-Quijano, K. Intraoperative Methadone in Adult Cardiac Surgical Patients and Risks for Postoperative QTc Prolongation. J. Cardiothorac. Vasc. Anesth. 2024, 39, 406–413. [Google Scholar] [CrossRef]
- Rickli, A.; Liakoni, E.; Hoener, M.C.; Liechti, M.E. Opioid-induced inhibition of the human 5-HT and noradrenaline transporters in vitro: Link to clinical reports of serotonin syndrome. Br. J. Pharmacol. 2018, 175, 532–543. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine; Action Collaborative on Countering the U.S. Opioid Epidemic; Health and Medicine Division; Board on Health Care Services; Board on Health Sciences Policy; Stroud, C.; Posey Norris, S.M.; Bain, L. (Eds.) The History of Methadone and Barriers to Access for Different Populations. In Methadone Treatment for Opioid Use Disorder: Improving Access Through Regulatory and Legal Change: Proceedings of a Workshop; National Academies Press (US): Washington, DC, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK585210/ (accessed on 26 January 2025).
- Hanna, V.; Senderovich, H. Methadone in Pain Management: A Systematic Review. J. Pain 2021, 22, 233–245. [Google Scholar] [CrossRef]
- Chang, Y.; Fang, W.B.; Lin, S.N.; Moody, D.E. Stereo-Selective Metabolism of Methadone by Human Liver Microsomes and cDNA-Expressed Cytochrome P450s: A Reconciliation. Basic Clin. Pharmacol. Toxicol. 2011, 108, 55–62. [Google Scholar] [CrossRef]
- Fredheim, O.M.S.; Moksnes, K.; Borchgrevink, P.C.; Kaasa, S.; Dale, O. Clinical pharmacology of methadone for pain. Acta Anaesthesiol. Scand. 2008, 52, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Gerber, J.G.; Rhodes, R.J.; Gal, J. Stereoselective metabolism of methadone N-demethylation by cytochrome P4502B6 and 2C19. Chirality 2004, 16, 36–44. [Google Scholar] [CrossRef]
- Totah, R.A.; Sheffels, P.; Roberts, T.; Whittington, D.; Thummel, K.; Kharasch, E.D. Role of CYP2B6 in stereoselective human methadone metabolism. Anesthesiology 2008, 108, 363–374. [Google Scholar] [CrossRef]
- Eap, C.B.; Buclin, T.; Baumann, P. Interindividual Variability of the Clinical Pharmacokinetics of Methadone. Clin. Pharmacokinet. 2002, 41, 1153–1193. [Google Scholar] [CrossRef]
- Li, Y.; Kantelip, J.P.; Schieveen, P.G.; van Davani, S. Interindividual Variability of Methadone Response. Mol. Diagn. Ther. 2008, 12, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.J.; Wang, S.C.; Liu, S.W.; Ho, I.K.; Chang, Y.S.; Tsai, Y.T.; Lin, K.-M.; Liu, Y.-L. Assessment of CYP450 Genetic Variability Effect on Methadone Dose and Tolerance. Pharmacogenomics 2014, 15, 977–986. [Google Scholar] [CrossRef]
- Bart, G.; Lenz, S.; Straka, R.J.; Brundage, R.C. Ethnic and genetic factors in methadone pharmacokinetics: A population pharmacokinetic study. Drug Alcohol. Depend. 2014, 145, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Richards-Waugh, L.L.; Primerano, D.A.; Dementieva, Y.; Kraner, J.C.; Rankin, G.O. Fatal methadone toxicity: Potential role of CYP3A4 genetic polymorphism. J. Anal. Toxicol. 2014, 38, 541–547. [Google Scholar] [CrossRef]
- Yang, H.C.; Chu, S.K.; Huang, C.L.; Kuo, H.W.; Wang, S.C.; Liu, S.W.; Ho, I.-K.; Liu, Y.-L. Genome-Wide Pharmacogenomic Study on Methadone Maintenance Treatment Identifies SNP rs17180299 and Multiple Haplotypes on CYP2B6, SPON1, and GSG1L Associated with Plasma Concentrations of Methadone R- and S-enantiomers in Heroin-Dependent Patients. PLoS Genet. 2016, 12, e1005910. [Google Scholar] [CrossRef]
- Baldo, B.A.; Rose, M.A. The anaesthetist, opioid analgesic drugs, and serotonin toxicity: A mechanistic and clinical review. Br. J. Anaesth. 2020, 124, 44–62. [Google Scholar] [CrossRef]
- Perananthan, V.; Buckley, N.A. Opioids and antidepressants: Which combinations to avoid. Aust. Prescr. 2021, 44, 41–44. [Google Scholar] [CrossRef]
- Crist, R.C.; Li, J.; Doyle, G.A.; Gilbert, A.; Dechairo, B.M.; Berrettini, W.H. Pharmacogenetic analysis of opioid dependence treatment dose and dropout rate. Am. J. Drug Alcohol Abus. 2018, 44, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Khokhar, J.Y.; Ferguson, C.S.; Zhu, A.Z.X.; Tyndale, R.F. Pharmacogenetics of Drug Dependence: Role of Gene Variations in Susceptibility and Treatment. Annu. Rev. Pharmacol. Toxicol. 2010, 50, 39–61. [Google Scholar] [CrossRef] [PubMed]
- Ficha Técnica Eptadone 100 mg Solución Oral. Agencia Española de Medicamentos y Productos Sanitarios. Available online: https://cima.aemps.es/cima/pdfs/es/ft/69909/fichatecnica_69909.html.pdf (accessed on 7 February 2025).
- PRISMA Statement. PRISMA Statement. Available online: https://www.prisma-statement.org (accessed on 7 February 2025).
- Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 7 February 2025).
- Eap, C.B.; Broly, F.; Mino, A.; Hämmig, R.; Déglon, J.J.; Uehlinger, C.; Meili, D.; Chevalley, A.F.; Bertschy, G.; Zullino, D.; et al. Cytochrome P450 2D6 genotype and methadone steady-state concentrations. J. Clin. Psychopharmacol. 2001, 21, 229–234. [Google Scholar] [CrossRef]
- Crettol, S.; Déglon, J.J.; Besson, J.; Croquette-Krokkar, M.; Gothuey, I.; Hämmig, R.; Monnat, M.; Hüttemann, H.; Baumann, P.; Eap, C.B. Methadone enantiomer plasma levels, CYP2B6, CYP2C19, and CYP2C9 genotypes, and response to treatment. Clin. Pharmacol. Ther. 2005, 78, 593–604. [Google Scholar] [CrossRef]
- Lötsch, J.; Skarke, C.; Wieting, J.; Oertel, B.G.; Schmidt, H.; Brockmöller, J.; Geisslinger, G. Modulation of the central nervous effects of levomethadone by genetic polymorphisms potentially affecting its metabolism, distribution, and drug action. Clin. Pharmacol. Ther. 2006, 79, 72–89. [Google Scholar] [CrossRef]
- Crettol, S.; Déglon, J.J.; Besson, J.; Croquette-Krokar, M.; Hämmig, R.; Gothuey, I.; Monnat, M.; Eap, C. ABCB1 and cytochrome P450 genotypes and phenotypes: Influence on methadone plasma levels and response to treatment. Clin. Pharmacol. Ther. 2006, 80, 668–681. [Google Scholar] [CrossRef]
- Eap, C.B.; Crettol, S.; Rougier, J.S.; Schläpfer, J.; Sintra, G.L.; Déglon, J.J.; Besson, J.; Croquette-Krokar, M.; Carrupt, P.-A.; Abriel, H. Stereoselective block of hERG channel by (S)-methadone and QT interval prolongation in CYP2B6 slow metabolizers. Clin. Pharmacol. Ther. 2007, 81, 719–728. [Google Scholar] [CrossRef]
- Pérez de los Cobos, J.; Siñol, N.; Trujols, J.; del Río, E.; Bañuls, E.; Luquero, E.; Menoyo, A.; Queraltó, J.M.; Baiget, M.; Álvarez, E. Association of CYP2D6 ultrarapid metabolizer genotype with deficient patient satisfaction regarding methadone maintenance treatment. Drug Alcohol Depend. 2007, 89, 190–194. [Google Scholar] [CrossRef]
- Bunten, H.; Liang, W.J.; Pounder, D.; Seneviratne, C.; Osselton, M.D. CYP2B6 and OPRM1 gene variations predict methadone-related deaths. Addict. Biol. 2011, 16, 142–144. [Google Scholar] [CrossRef]
- Fonseca, F.; de la Torre, R.L.; Pastor, A.; Cuyàs, E.; Pizarro, N.; Khymenets, O.; Farré, M.; Torrens, M. Contribution of cytochrome P450 and ABCB1 genetic variability on methadone pharmacokinetics, dose requirements, and response. PLoS ONE 2011, 6, e19527. [Google Scholar] [CrossRef] [PubMed]
- Dobrinas, M.; Crettol, S.; Oneda, B.; Lahyani, R.; Rotger, M.; Choong, E.; Lubomirov, R.; Csajka, C.; Eap, C.B. Contribution of CYP2B6 alleles in explaining extreme (S)-methadone plasma levels: A CYP2B6 gene resequencing study. Pharmacogenetics Genom. 2013, 23, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Mouly, S.; Bloch, V.; Peoc’h, K.; Houze, P.; Labat, L.; Ksouda, K.; Simoneau, G.; Declèves, X.; Bergmann, J.F.; Scherrmann, J.; et al. Methadone dose in heroin-dependent patients: Role of clinical factors, comedications, genetic polymorphisms and enzyme activity. Br. J. Clin. Pharmacol. 2015, 79, 967–977. [Google Scholar] [CrossRef]
- Carlquist, J.F.; Moody, D.E.; Knight, S.; Johnson, E.G.; Fang, W.B.; Huntinghouse, J.A.; Rollo, J.S.; Webster, L.R.; Anderson, J.L. A Possible Mechanistic Link Between the CYP2C19 Genotype, the Methadone Metabolite Ethylidene-1,5-Dimethyl-3,3-Diphenylpyrrolidene (EDDP), and Methadone-Induced Corrected QT Interval Prolongation in a Pilot Study. Mol. Diagn. Ther. 2015, 19, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Christoffersen, D.J.; Damkier, P.; Feddersen, S.; Möller, S.; Thomsen, J.L.; Brasch-Andersen, C.; Brøsen, K. The ABCB1, rs9282564, AG and TT Genotypes and the COMT, rs4680, AA Genotype are Less Frequent in Deceased Patients with Opioid Addiction than in Living Patients with Opioid Addiction. Basic Clin. Pharmacol. Toxicol. 2016, 119, 381–388. [Google Scholar] [CrossRef]
- Ahmad, T.; Sabet, S.; Primerano, D.A.; Richards-Waugh, L.L.; Rankin, G.O. Tell-Tale SNPs: The Role of CYP2B6 in Methadone Fatalities. J. Anal. Toxicol. 2017, 41, 325–333. [Google Scholar] [CrossRef]
- Iwersen-Bergmann, S.; Plattner, S.; Hischke, S.; Müller, A.; Andresen-Streichert, H.; Jungen, H.; Erb, R.; Beer-Sandner, B. Brain/blood ratios of methadone and ABCB1 polymorphisms in methadone-related deaths. Int. J. Leg. Med. 2021, 135, 473–482. [Google Scholar] [CrossRef]
- PubChem. CYP2B6—Cytochrome P450 Family 2 Subfamily B Member 6 (Human). Available online: https://pubchem.ncbi.nlm.nih.gov/gene/CYP2B6/human (accessed on 7 February 2025).
- PharmVar. Available online: https://www.pharmvar.org/gene/CYP2B6 (accessed on 7 February 2025).
- ABCB1 ATP Binding Cassette Subfamily B Member 1 [Homo Sapiens (Human)]—Gene—NCBI. Available online: https://www.ncbi.nlm.nih.gov/gene/5243 (accessed on 7 February 2025).
- Nofziger, C.; Turner, A.J.; Sangkuhl, K.; Whirl-Carrillo, M.; Agúndez, J.A.G.; Black, J.L.; Dunnenberger, H.M.; Ruano, G.; Kennedy, M.A.; Phillips, M.S.; et al. PharmVar GeneReview: CYP2D6. Clin. Pharmacol. Ther. 2020, 107, 154–170. [Google Scholar] [CrossRef]
- CYP2D6 Cytochrome P450 Family 2 Subfamily D Member 6 (Gene/Pseudogene) [Homo Sapiens (Human)]—Gene—NCBI. Available online: https://www.ncbi.nlm.nih.gov/gene/1565 (accessed on 7 February 2025).
- Kharasch, E.D.; Regina, K.J.; Blood, J.; Friedel, C. Methadone pharmacogenetics: CYP2B6 polymorphisms determine plasma concentrations, clearance and metabolism. Anesthesiology 2015, 123, 1142–1153. [Google Scholar] [CrossRef]
- Kringen, M.K.; Chalabianloo, F.; Bernard, J.P.; Bramness, J.G.; Molden, E.; Høiseth, G. Combined Effect of CYP2B6 Genotype and Other Candidate Genes on a Steady-State Serum Concentration of Methadone in Opioid Maintenance Treatment. Ther. Drug Monit. 2017, 39, 550–555. [Google Scholar] [CrossRef]
- Desta, Z.; El-Boraie, A.; Gong, L.; Somogyi, A.A.; Lauschke, V.M.; Dandara, C.; Klein, K.; Miller, N.A.; Klein, T.E.; Tyndale, R.F.; et al. PharmVar GeneFocus: CYP2B6. Clin. Pharmacol. Ther. 2021, 110, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Robinson, K.M.; Eum, S.; Desta, Z.; Tyndale, R.F.; Gaedigk, A.; Crist, R.C.; Haidar, C.E.; Myers, A.L.; Samer, C.F.; Somogyi, A.A.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2B6 Genotype and Methadone Therapy. Clin. Pharmacol. Ther. 2024, 116, 932–938. [Google Scholar] [CrossRef]
- PharmGKB. Gene-Specific Information Tables for CYP2B6. Available online: https://www.pharmgkb.org/page/cyp2b6RefMaterials (accessed on 7 February 2025).
- Shah, R.R.; Smith, R.L. Addressing phenoconversion: The Achilles’ heel of personalized medicine. Br. J. Clin. Pharmacol. 2015, 79, 222–240. [Google Scholar] [CrossRef] [PubMed]
- Mangó, K.; Kiss, Á.F.; Fekete, F.; Erdős, R.; Monostory, K. CYP2B6 allelic variants and non-genetic factors influence CYP2B6 enzyme function. Sci. Rep. 2022, 12, 2984. [Google Scholar] [CrossRef]
- De Leon, J. The effects of antiepileptic inducers in neuropsychopharmacology, a neglected issue. Part II: Pharmacological issues and further understanding. Rev. Psiquiatr. Salud Ment. 2015, 8, 167–188. [Google Scholar] [CrossRef] [PubMed]
- McCance-Katz, E.F. Drug interactions associated with methadone, buprenorphine, cocaine, and HIV medications: Implications for pregnant women. Life Sci. 2011, 88, 953–958. [Google Scholar] [CrossRef]
- McCance-Katz, E.F.; Sullivan, L.E.; Nallani, S. Drug interactions of clinical importance among the opioids, methadone and buprenorphine, and other frequently prescribed medications: A review. Am. J. Addict. 2010, 19, 4–16. [Google Scholar] [CrossRef]
- Begré, S.; von Bardeleben, U.; Ladewig, D.; Jaquet-Rochat, S.; Cosendai-Savary, L.; Golay, K.P.; Kosel, M.; Baumann, P.; Eap, C.B. Paroxetine increases steady-state concentrations of (R)-methadone in CYP2D6 extensive but not poor metabolizers. J. Clin. Psychopharmacol. 2002, 22, 211–215. [Google Scholar] [CrossRef]
- Uehlinger, C.; Crettol, S.; Chassot, P.; Brocard, M.; Koeb, L.; Brawand-Amey, M.; Eap, C.B. Increased (R)-methadone plasma concentrations by quetiapine in cytochrome P450s and ABCB1 genotyped patients. J. Clin. Psychopharmacol. 2007, 27, 273–278. [Google Scholar] [CrossRef]
- Hamilton, S.P.; Nunes, E.V.; Janal, M.; Weber, L. The effect of sertraline on methadone plasma levels in methadone-maintenance patients. Am. J. Addict. 2000, 9, 63–69. [Google Scholar] [CrossRef]
- Irwin, M.N.; Ellingrod, V.L.; Smith, M.A. Pharmacogenetics of Methadone for Pain Management in Palliative Care. J. Pain Symptom Manag. 2022, 63, e142–e145. [Google Scholar] [CrossRef]
- Grimsrud, K.N.; Davis, R.R.; Tepper, C.G.; Palmieri, T.L. Pharmacogenetic Gene-Drug Associations in Pediatric Burn and Surgery Patients. J. Burn. Care Res. 2022, 43, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Whirl-Carrillo, M.; Huddart, R.; Gong, L.; Sangkuhl, K.; Thorn, C.F.; Whaley, R.; Klein, T.E. An Evidence-Based Framework for Evaluating Pharmacogenomics Knowledge for Personalized Medicine. Clin. Pharmacol. Ther. 2021, 110, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Kharasch, E.D.; Stubbert, K. Role of cytochrome P4502B6 in methadone metabolism and clearance. J. Clin. Pharmacol. 2013, 53, 305–313. [Google Scholar] [CrossRef]
- Oneda, B.; Crettol, S.; Jaquenoud Sirot, E.; Bochud, M.; Ansermot, N.; Eap, C.B. The P450 oxidoreductase genotype is associated with CYP3A activity in vivo as measured by the midazolam phenotyping test. Pharmacogenetics Genom. 2009, 19, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Rojas Velazquez, M.N.; Therkelsen, S.; Pandey, A.V. Exploring Novel Variants of the Cytochrome P450 Reductase Gene (POR) from the Genome Aggregation Database by Integrating Bioinformatic Tools and Functional Assays. Biomolecules 2023, 13, 1728. [Google Scholar] [CrossRef]
- Wang, P.F.; Sharma, A.; Montana, M.; Neiner, A.; Juriga, L.; Reddy, K.N.; Tallchief, D.; Blood, J.; Kharasch, E.D. Methadone pharmacogenetics in vitro and in vivo: Metabolism by CYP2B6 polymorphic variants and genetic variability in paediatric disposition. Br. J. Clin. Pharmacol. 2022, 88, 4881–4893. [Google Scholar] [CrossRef]
- Levran, O.; Peles, E.; Hamon, S.; Randesi, M.; Adelson, M.; Kreek, M.J. CYP2B6 SNPs are associated with methadone dose required for effective treatment of opioid addiction. Addict. Biology 2013, 18, 709–716. [Google Scholar] [CrossRef]
- Takemura, M.; Niki, K.; Okamoto, Y.; Kawamura, T.; Kohno, M.; Matsuda, Y.; Ikeda, K. Comparison of the Effects of OPRM1 A118G Polymorphism Using Different Opioids: A Prospective Study. J. Pain Symptom Manag. 2024, 67, 39–49.e5. [Google Scholar] [CrossRef]
- Chiang, Y.; Wang, R.; Huang, C.; Chen, S.; Ho, W.; Lane, H.; Ho, I.; Yang, H.; Ma, W. Reduced dosing and liability in methadone maintenance treatment by targeting oestrogen signal for morphine addiction. J. Cell. Mol. Med. 2017, 21, 3552–3564. [Google Scholar] [CrossRef]
- Huhn, A.S.; Berry, M.S.; Dunn, K.E. Review: Sex-based Differences in Treatment Outcomes for Persons with Opioid Use Disorder. Am. J. Addict. 2019, 28, 246–261. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Authors and Year | Sample Size (n) | Mean Age | Ethnicity/Recruitment Country | PK Genes Included | Findings | p-Value |
|---|---|---|---|---|---|---|
| Eap et al., 2001 [40] | 256 | 31 (SD not available) | Switzerland | CYP2D6 |
|
|
| Crettol et al., 2005 [41] | 209 | 36 ± 8 | Switzerland | CYP2B6 |
|
|
| CYP2C19 |
|
| ||||
| CYP2C9 |
|
| ||||
| Lötsch et al., 2006 [42] | 51 | 27.2 ± 5.3 | Germany | ABCB1, CYP2B6, CYP1A2, CYP3A5, CYP2C8, CYP2C9, CYP2C19, CYP2D6 |
|
|
| Crettol et al., 2006 [43] | 245 | 36 ± 8 | 95% Caucasian, Switzerland | CYP3A4 |
|
|
| ABCB1 |
|
| ||||
| CYP2B6 |
|
| ||||
| CYP2D6 |
|
| ||||
| UGT2B7, CYP1A2, CYP2C9, CYP2C19 |
| Respectively,
| ||||
| Eap et al., 2007 [44] | 179 | 36 ± 8 | 98% Caucasian, Switzerland | CYP2B6 |
|
|
| Pérez de los Cobos et al., 2007 [45] | 205 | 36.8 ± 6 | Spain | CYP2D6 |
|
|
| Bunten et al., 2010 [46] | 67 | 31 ± 1.67 | United Kingdom | CYP2B6 |
|
|
| Fonseca et al., 2011 [47] | 105 | 38 ± 8 | Spain | CYP2D6 |
|
|
| CYP2B6 |
|
| ||||
| CYP3A5, CYP2C9, CYP2C19, ABCB1 |
|
| ||||
| Dobrinas et al., 2013 [48] | 276 | Not available | Switzerland | CYP2B6 |
|
|
| Mouly et al., 2014 [49] | 81 | 43.7 ± 8.1 | 85.2% Caucasian, France | ABCB1, CYP2B6, CYP3A5, CYP2C19, CYP2D6 |
| Respectively,
|
| Carlquist et al., 2015 [50] | 42 | 30.3 ± 9.9 | 74 % Caucasian, United States of America | CYP2C19 |
|
|
| Christoffersen et al., 2016 [51] | 977 | 42 (SD not available) | Denmark | ABCB1 |
|
|
| CYP2B6, CYP2D6, CYP3A5, CYP2C19, UGT2B7 |
| Respectively,
| ||||
| Ahmad et al., 2017 [52] | 380 | 34.08 ± 11.40 | 100 % Caucasian, United States of America | CYP2B6 |
|
|
| Iwersen-Bergmann et al., 2020 [53] | 107 | 41 (SD not available) | Germany | ABCB1 |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Recarey-Rama, S.; Gómez-Trigo, J.; Gil-Rodriguez, A.; Dominguez, E.; Sánchez-Martínez, I.; Riveiro-Recimil, Á.; Barral-Raña, A.; de Leon, J.; Rodriguez-Viyuela, A.; Arrojo, M.; et al. The Relevance of Pharmacokinetic Biomarkers in Response to Methadone Treatment: A Systematic Review. Pharmaceuticals 2025, 18, 623. https://doi.org/10.3390/ph18050623
Recarey-Rama S, Gómez-Trigo J, Gil-Rodriguez A, Dominguez E, Sánchez-Martínez I, Riveiro-Recimil Á, Barral-Raña A, de Leon J, Rodriguez-Viyuela A, Arrojo M, et al. The Relevance of Pharmacokinetic Biomarkers in Response to Methadone Treatment: A Systematic Review. Pharmaceuticals. 2025; 18(5):623. https://doi.org/10.3390/ph18050623
Chicago/Turabian StyleRecarey-Rama, Sheila, Jesús Gómez-Trigo, Almudena Gil-Rodriguez, Eduardo Dominguez, Inés Sánchez-Martínez, Ángela Riveiro-Recimil, Alba Barral-Raña, Jose de Leon, Ana Rodriguez-Viyuela, Manuel Arrojo, and et al. 2025. "The Relevance of Pharmacokinetic Biomarkers in Response to Methadone Treatment: A Systematic Review" Pharmaceuticals 18, no. 5: 623. https://doi.org/10.3390/ph18050623
APA StyleRecarey-Rama, S., Gómez-Trigo, J., Gil-Rodriguez, A., Dominguez, E., Sánchez-Martínez, I., Riveiro-Recimil, Á., Barral-Raña, A., de Leon, J., Rodriguez-Viyuela, A., Arrojo, M., Carracedo, A., & Maroñas, O. (2025). The Relevance of Pharmacokinetic Biomarkers in Response to Methadone Treatment: A Systematic Review. Pharmaceuticals, 18(5), 623. https://doi.org/10.3390/ph18050623