
Synthetic Haemostatic Sealants: Effectiveness, Safety, and In Vivo Applications



 and
and 
Abstract
1. Introduction
2. Results
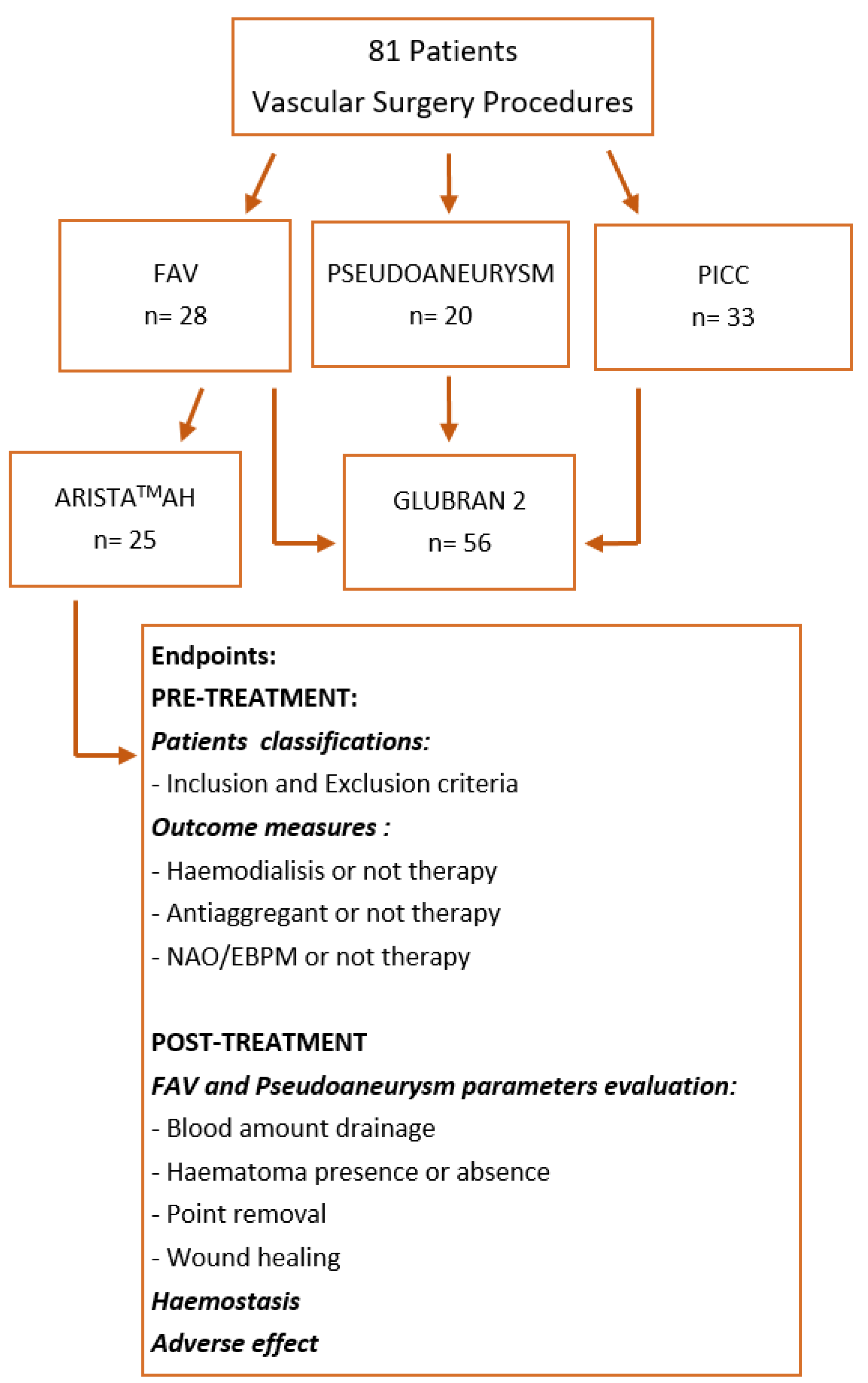
2.1. Study Population
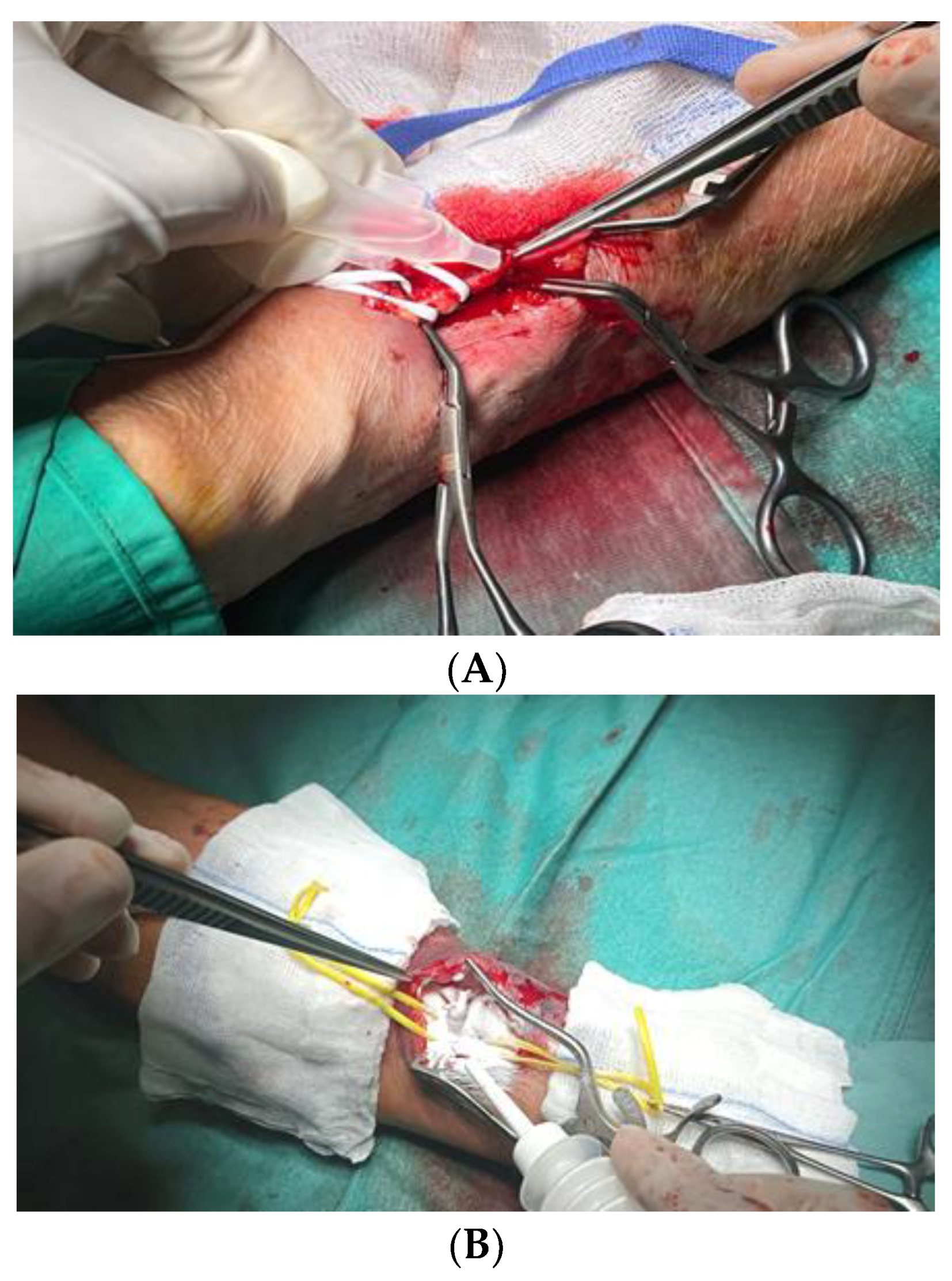
2.2. Procedure Data
2.3. Outcomes and Follow-up
2.4. Haemostasis Evaluation
3. Discussion
4. Materials and Methods
4.1. Study Design
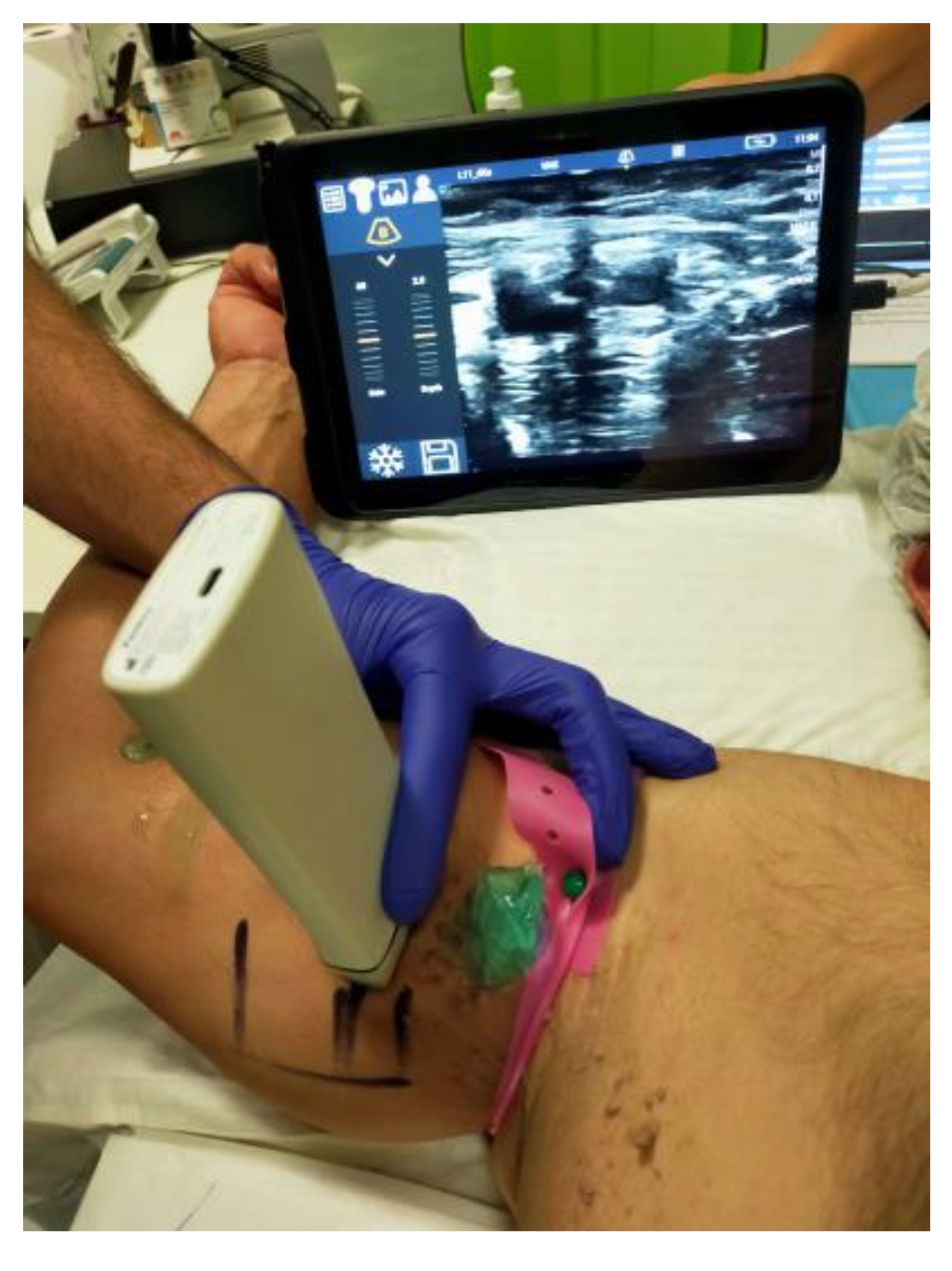
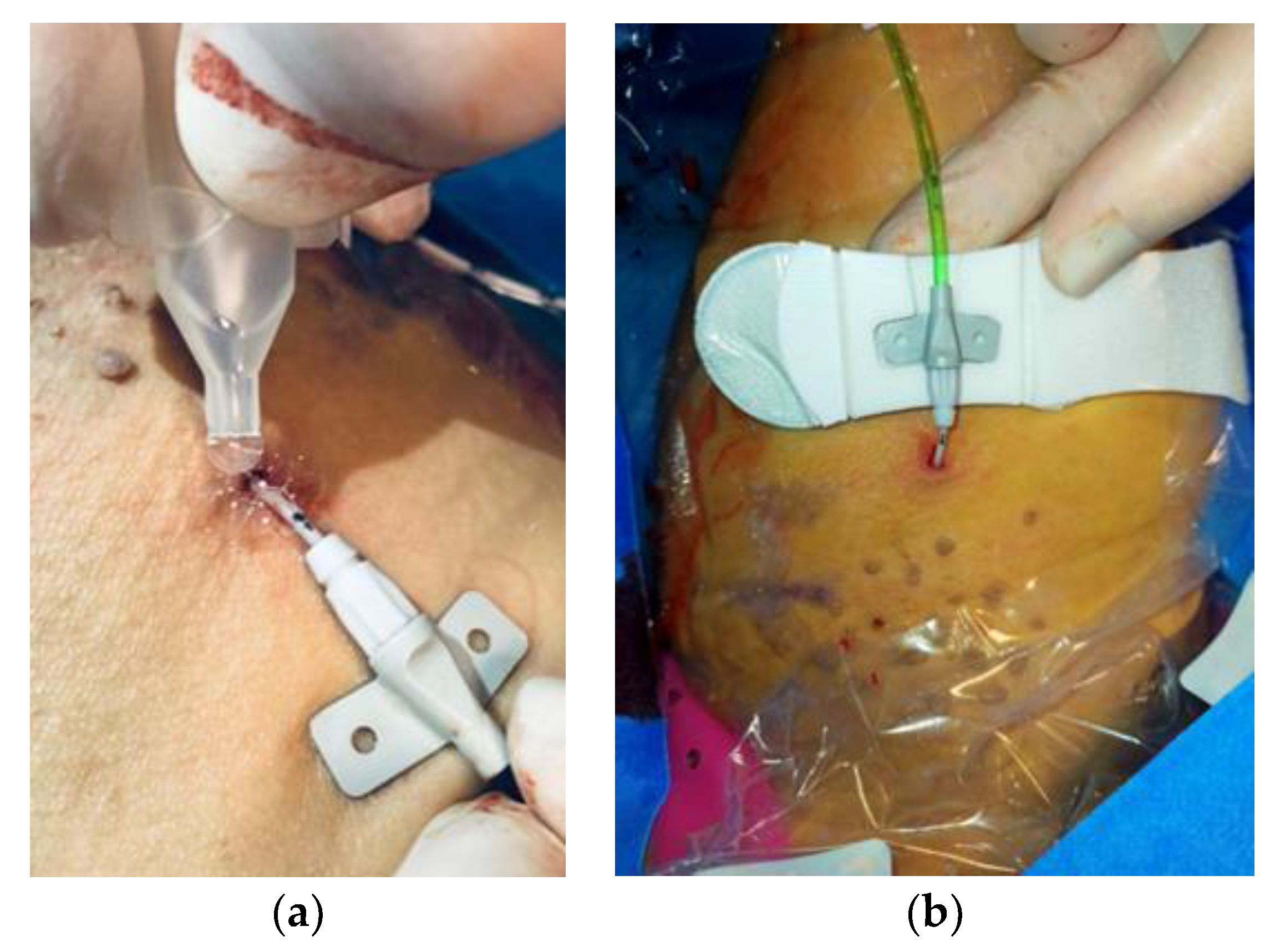
4.2. Data Collections and Procedure
4.3. Outcomes
4.4. Haemostasis Evaluation
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bao, Z.; Gao, M.; Sun, Y.; Nian, R.; Xian, M. The recent progress of tissue adhesives in design strategies, adhesive mechanism and applications. Mater. Sci. Eng. C 2020, 111, 110796. [Google Scholar] [CrossRef] [PubMed]
- Bal-Ozturk, A.; Cecen, B.; Avci-Adali, M.; Topkaya, S.N.; Alarcin, E.; Yasayan, G.; Li, Y.-C.E.; Bulkurcuoglu, B.; Akpek, A.; Avci, H.; et al. Tissue adhesives: From research to clinical translation. Nano Today 2021, 36, 101049. [Google Scholar] [CrossRef] [PubMed]
- Trombino, S.; Sole, R.; Curcio, F.; Cassano, R. Polymeric Based Hydrogel Membranes for Biomedical Applications. Membranes 2023, 13, 576. [Google Scholar] [CrossRef] [PubMed]
- Trombino, S.; Curcio, F.; Cassano, R.; Curcio, M.; Cirillo, G.; Iemma, F. Polymeric Biomaterials for the Treatment of Cardiac Post-Infarction Injuries. Pharmaceutics 2021, 13, 1038. [Google Scholar] [PubMed]
- Cassano, R.; Curcio, F.; Sole, R.; Trombino, S. Chapter 3: Hydrogel based on hyaluronic acid. In Polysaccharide Hydrogels for Drug Delivery and Regenerative Medicine; Elsevier: Amsterdam, The Netherlands, 2023; pp. 35–46. [Google Scholar]
- Serini, S.; Trombino, S.; Curcio, F.; Sole, R.; Cassano, R.; Calviello, G. Hyaluronic Acid-Mediated Phenolic Compound Nano-Delivery for Cancer Targeting. Pharmaceutics 2023, 15, 1751. [Google Scholar] [CrossRef]
- Cassano, R.; Perri, P.; Esposito, A.; Intrieri, F.; Sole, R.; Curcio, F.; Trombino, S. Expanded Polytetrafluoroethylene Membranes for Vascular Stent Coating: Manufacturing, Biomedical and Surgical Applications, Innovations and Case Reports. Membranes 2023, 13, 240. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.; Mooney, D. Polymeric Tissue Adhesives. Chem. Rev. 2021, 121, 11336–11384. [Google Scholar] [CrossRef]
- Dey, A.; Bhattacharya, P.; Neogi, S. Bioadhesives in Biomedical Applications: A Critical Review. In Progress in Adhesion and Adhesives; Mittal, K.L., Ed.; Scrivener Publishing LLC: Beverly, MA, USA, 2021; Volume 6, pp. 131–154. [Google Scholar]
- Athavale, A.; Thao, M.; Sassaki, V.S.; Lewis, M.; Chandra, V.; Fukaya, E. Cyanoacrylate glue reactions: A systematic review, cases, and proposed mechanisms. J. Vasc. Surg. Venous Lymphat. Disord. 2023, 11, 876–888.e1. [Google Scholar] [CrossRef]
- Allotey, J.K.; King, A.H.; Kumins, N.H.; Wong, V.L.; Harth, K.C.; Cho, J.S.; Kashyap, V.S. Systematic review of hemostatic agents used in vascular surgery. J. Vasc. 2021, 73, 6. [Google Scholar] [CrossRef]
- Glubran 2 - GEM Italy. Available online: https://www.gemitaly.it/prodotti/glubran-2/ (accessed on 27 December 2023).
- Thangaraju, P.; Shoban, B.V. ISO 10993: Biological Evaluation of Medical Devices. In Medical Device Guidelines and Regulations Handbook; Springer International Publishing: Cham, Switzerland, 2022; pp. 163–187. [Google Scholar]
- Dhandapani, V.; Saseedharan, P.; Groleau, D.; Vermette, P. Overview of approval procedures for bioadhesives in the United States of America and Canada. J. Biomed. Mater. Res. 2022, 110, 950–966. [Google Scholar] [CrossRef]
- Guillen, K.; Comby, P.-O.; Chevallier, O.; Salsac, A.-V.; Loffroy, R. In Vivo Experimental Endovascular Uses of Cyanoacrylate in Non-Modified Arteries: A Systematic Review. Biomedicines 2021, 9, 1282. [Google Scholar] [CrossRef] [PubMed]
- Zheng, K.; Gu, Q.; Zhou, D.; Zhou, M.; Zhang, L. Recent progress in surgical adhesives for biomedical applications. Smart Mater. Med. 2022, 3, 41–65. [Google Scholar] [CrossRef]
- Malik, A.; Ur Rehman, F.; Ullah Shah, K.; Naz, S.S.; Sara Qaisar, S. Hemostatic strategies for uncontrolled bleeding: A comprehensive update. J. Biomed. Mater. Res. 2021, 109, 1465–1477. [Google Scholar] [CrossRef] [PubMed]
- Comby, P.; Guillen, K.; Chevallier, O.; Lenfant, M.; Pellegrinelli, J.; Falvo, N.; Midulla, M.; Loffroy, R. Endovascular Use of Cyanoacrylate-Lipiodol Mixture for Peripheral Embolization: Properties, Techniques, Pitfalls, and Applications. J. Clin. Med. 2021, 10, 4320. [Google Scholar] [CrossRef]
- Asada, Y.; Yamashita, A.; Sato, Y.; Hatakeyama, K. Pathophysiology of atherothrombosis: Mechanisms of thrombus formation on disrupted atherosclerotic plaques. Pathol. Int. 2020, 70, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Brass, L.F.; Tomaiuolo, M.; Welsh, J.; Poventud-Fuentes, I.; Zhu, L.; Diamond, S.L.; Stalker, T.J. Hemostatic Thrombus Formation in Flowing Blood. In Platelets; Academic Press: Cambridge, MA, USA, 2019; pp. 371–391. [Google Scholar]
- Krüger-Genge, A.; Blocki, A.; Franke, R.P.; Jung, F. Vascular Endothelial Cell Biology: An Update. Int. J. Mol. Sci. 2019, 20, 4411. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Kishimoto, T. Interplay between interleukin-6 signaling and the vascular endothelium in cytokine storms. Exp. Mol. Med. 2021, 53, 1116–1123. [Google Scholar] [CrossRef]
- Medafor. LIT-0057 Rev E Arista® AH Absorbable Hemostatic Particles Microporous Polysaccharide Hemosphere (MPH) Technology; Medafor, Inc.: Minneapolis, MN, USA, 2008. [Google Scholar]
- Biranje, S.S.; Sun, J.; Shi, Y.; Yu, S.; Jiao, H.; Zhang, M.; Wang, Q.; Wang, J.; Liu, J. Polysaccharide-based hemostats: Recent developments, challenges, and future perspectives. Cellulose 2021, 28, 8899–8937. [Google Scholar] [CrossRef]
- Miller, K.J.; Cao, W.; Ibrahim, M.M.; Levinson, H. The effect of microporous polysaccharide hemospheres on wound healing and scarring in wild-type and Db/Db mice. Adv. Ski. Wound Care 2017, 30, 169–180. [Google Scholar] [CrossRef]
- Balakrishnan, B.; Payanam, U.; Laurent, A.; Wassef, M.; Jayakrishnan, A. Efficacy evaluation of an in situ forming tissue adhesive hydrogel as sealant for lung and vascular injury. Biomed. Mater. 2021, 16, 044106. [Google Scholar] [CrossRef]
- Capella-Monsonís, H.; Shridhar, A.; Chirravuri, B.; Figucia, M.; Learn, G.; Greenawalt, K.; Badylak, S.F. A Comparative Study of the Resorption and Immune Response for Two Starch-Based Hemostat Powders. J. Surg. Res. 2023, 282, 210–224. [Google Scholar] [CrossRef] [PubMed]
- Grange, R.; Chevalier-Meilland, C.; Le Roy, B.; Grange, S. Delayed superior epigastric artery pseudoaneurysm following percutaneous radiologic gastrostomy: Treatment by percutaneous embolization with N-butyl cyanoacrylate. Radiol. Case Rep. 2021, 16, 1459–1462. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, S.; Aslanidi, C.; Mamalis, V.; Markogiannakis, G.; Tsanis, A.; Arhontakis, E. Endovascular management of spontaneous intracranial pseudoaneurysms in a pediatric patient with Noonan syndrome. A mere coincidence or a possible association with the disorder? Surg. Neurol. Int. 2021, 12, 537. [Google Scholar] [CrossRef] [PubMed]
- Gleasona, S.; Mehla, D.; Paynea, W.; Parrya, S.; Buros Steinb, A. Microporous polysaccharide hemosphere efficacy and safety in primary total knee arthroplasty. J. Orthop. 2019, 16, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Bruckner, B.A.; Blau, L.N.; Rodriguez, L.; Suarez, E.E.; Ngo, U.Q.; Reardon, M.J.; Loebe, M. Microporous polysaccharide hemosphere absorbable hemostat use in cardiothoracic surgical procedures. J. Cardiothorac. Surg. 2014, 9, 134. [Google Scholar] [CrossRef] [PubMed]
- Rajagopal, P.; Hakim, N. The use of a powdered polysaccharide hemostat (hemostase) in live donor nephrectomies controls bleeding and reduces postoperative complications. Transplant. Proc. 2011, 43, 424–426. [Google Scholar] [CrossRef]
- Antisdel, J.L.; Matijasec, J.L.; Ting, J.Y.; Sindwani, R. Microporous polysaccharide hemispheres do not increase synechiae after sinus surgery: Randomized controlled study. Am. J. Rhinol. Allergy 2011, 25, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Hadi, M.; Walker, C.; Desborough, M.; Basile, A.; Tsetis, D.; Hunt, B.; Müller-Hüllsbeck, S.; Rand, T.; van Delden, O.; Uberoi, R. CIRSE Standards of Practice on Peri-Operative Anticoagulation Management During Interventional Radiology Procedures. Cardiovasc. Interv. Radiol. 2021, 44, 523–536. [Google Scholar] [CrossRef]
- Prasad, R.; Israrahmed, A.; Yadav, R.R.; Singh, S.; Behra, M.R.; Khuswaha, R.S.; Prasad, N.; Lal, H. Endovascular Embolization in Problematic Hemodialysis Arteriovenous Fistulas: A Nonsurgical Technique Indian. J. Nephrol. 2021, 31, 516–523. [Google Scholar] [CrossRef]
- Bertagna, G.; Adami, D.; Del Corso, S. Percutaneous glue embolization of arteriovenous fistula of in situ saphenous vein bypass graft: Case report and literature review. Vascular 2022, 30, 759–763. [Google Scholar] [CrossRef]
- Zhang, S.; Lingle, B.S.; Phelps, S. A Revolutionary, Proven Solution to Vascular Access Concerns: A Review of the Advantageous Properties and Benefits of Catheter Securement Cyanoacrylate Adhesives. J. Infus. Nurs. 2022, 45, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Bergua-Lorente, A.; JFarrero-Mena, J.; Escolà-Nogués, A.; Llauradó-Mateu, M.; Serret-Nuevo, C.; Bellon, F. Effectiveness of cyanoacrylate glue in the fixation of midline catheters and peripherally inserted central catheters in hospitalized adult patients: Randomised clinical trial. SAGE Open Med. 2023, 11. [Google Scholar] [CrossRef]
- Del Corso, A.; Vergaro, G. Percutaneous Treatment of Iatrogenic Pseudoaneurysms by Cyanoacrylate-Based Wall-Gluing. Cardiovasc. Interv. Radiol. 2013, 36, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Kar, H. Surgical treatment of iatrogenic pseudoaneurysms. Turk. J. Vasc. Surg. 2019, 28, 174–179. [Google Scholar] [CrossRef]
- Ferrante, G.; Rao, S.V.; Jüni, P.; Da Costa, B.R.; Reimers, B.; Condorelli, G.; Anzuini, A.; Jolly, S.S.; Bertrand, O.F.; Krucoff, M.W.; et al. Radial Versus Femoral Access for Coronary Interventions Across the Entire Spectrum of Patients With Coronary Artery Disease: A Meta-Analysis of Randomized Trials. JACC Cardiovasc. Interv. 2016, 9, 1419–1434. [Google Scholar] [CrossRef] [PubMed]
- De Luca, M.; Restuccia, D.; Spizzirri, U.G.; Crupi, P.; Ioele, G.; Gorelli, B.; Clodoveo, M.L.; Saponara, S.; Aiello, F. Wine Lees as Source of Antioxidant Molecules: Green Extraction Procedure and Biological Activity. Antioxidants 2023, 12, 622. [Google Scholar] [CrossRef] [PubMed]
- Marrelli, M.; Amodeo, V.; Viscardi, F.; De Luca, M.; Statti, G.; Conforti, F. Essential Oils of Foeniculum vulgare subsp. Piperitum and Their In Vitro Anti-Arthritic Potential. Chem. Biodivers. 2020, 17, 200038. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Picc Patients (n = 28) | FAV Patients (n = 33) | Pseudoaneuriysm Patients (n = 20) |
|---|---|---|---|
| Ages (years) | 68 | 71 | 77 |
| Sex (%M/%F) | 70 (F)/30 (M) | 68 (F)/32 (M) | 20 (F)/80 (M) |
| INR * | 0.92 | 1.18 | 1.06 |
| aPTT ** (s) | 27 | 35 | 32 |
| Platelet count (×106/mL) | 260 | 340 | 290 |
| Haemoglobin (g/dL) | 14 | 8 | 13 |
| Creatinine (mg/dL) | 0.9 | 4.9 | 1.3 |
| Anticoagulant therapy (%) | 7 | 25 | 20 |
| Antiplatelet therapy | (%) 18 | 65 | 50 |
| Haemodialysis therapy (%) | 0 | 50 | 20 |
| (a) | |||||||||
| Outcomes | Control | Not on Anti-Aggregant Therapy (AristaTMAH) | Not on NAO/EBPM Therapy (AristaTMAH) | Not on Anti-Aggregant Therapy (Glubran 2) | Not on NAO/EBPM Therapy (Glubran 2) | Anti-Aggregant Therapy (AristaTMAH) | NAO/EBPM Therapy (AristaTMAH) | Anti-Aggregant Therapy (Glubran 2) | NAO/EBPM Therapy (Glubran 2) |
| Samples of patients (n=) | 20 | 2 | 2 | 2 | 1 | 4 | 3 | 6 | 3 |
| Anticoagulant or antiaggregant administration via os | 20 | no | no | no | no | si | si | si | si |
| Drainage amount at 3 h (cc) | 16 | 2 | 2 | 2 | 2 | 5 | 6 | 5 | 6 |
| Drainage amount at 6 h (cc) | 16 | 2 | 2 | 2 | 2 | 8 | 10 | 8 | 10 |
| Drainage amount at 24 h (cc) | 16 | 3 | 3 | 3 | 3 | 10 | 12 | 10 | 12 |
| Hematoma at 24 h | 16 | no | no | no | no | si | si | si | si |
| Hematoma at 7 days | 16 | no | no | no | no | no | si | no | si |
| Point removal at 7 days (pz.%) | 16 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Wound healing (pz.%) | 16 | 100 | 100 | 100 | 98 | 98 | 93 | 100 | 90 |
| (b) | |||||||||
| Outcomes | Control | Not on Anti-Aggregant Therapy (Arista TMAH) | Not on NAO/EBPM Therapy (AristaTMAH) | Not on Anti-Aggregant Therapy (Glubran 2) | Not on NAO/EBPM Therapy (Glubran 2) | Anti-Aggregant Therapy (AristaTMAH) | NAO/EBPM Therapy (AristaTMAH) | Anti-Aggregant Therapy (Glubran 2) | NAO/EBPM Therapy (Glubran 2) |
| Samples of patients (n=) | 22 | 1 | 1 | 2 | 1 | 4 | 3 | 6 | 3 |
| Anticoagulant or antiaggregant administration via os | 22 | no | no | no | no | si | si | si | si |
| Drainage amount at 3 h (cc) | 17 | 2 | 2 | 2 | 2 | 4 | 6 | 4 | 6 |
| Drainage amount at 6 h (cc) | 17 | 2 | 2 | 2 | 2 | 7 | 10 | 8 | 10 |
| Drainage amount at 24 h (cc) | 17 | 3 | 3 | 3 | 3 | 10 | 12 | 10 | 12 |
| Hematoma at 24 h | 17 | no | no | no | no | si | si | si | si |
| Hematoma at 7 days | 17 | no | no | no | no | no | si | no | si |
| Point removal at 7 days (pz.%) | 17 | 100 | 85 | 100 | 100 | 100 | 100 | 100 | 100 |
| Wound healing (pz.%) | 17 | 100 | 100 | 100 | 100 | 98 | 93 | 100 | 90 |
| (a) | |||||
| Outcomes | Control | Not on Anti-Aggregant Therapy (Glubran 2) | Not on NAO/EBPM Therapy (Glubran 2) | Anti-Aggregant Therapy (Glubran 2) | NAO/EBPM Therapy (Glubran 2) |
| Samples of patients (n=) | 15 | 3 | 2 | 8 | 2 |
| Anticoagulant or antiaggregant administration via os | 15 | no | no | si | si |
| Drainage amount at 3 h (cc) | 10 | 3 | 3 | 7 | 8 |
| Drainage amount at 6 h (cc) | 10 | 3 | 3 | 9 | 11 |
| Drainage amount at 24 h (cc) | 10 | 3 | 3 | 9 | 11 |
| Hematoma at 24 h | 10 | si | si | si | si |
| Hematoma at 7 days | 10 | no | no | si | si |
| Hematomaat 30 days (pz.%) | 10 | no | no | no | no |
| Wound healing Vycryl point (pz.%) | 10 | 100 | 100 | 90 | 90 |
| Wound healing Metal clips (pz.%) | 10 | 100 | 100 | 87 | 88 |
| (b) | |||||
| Outcomes | Control | Not on Anti-Aggregant Therapy (Glubran 2) | Not on NAO/EBPM Therapy (Glubran 2) | Anti-Aggregant Therapy (Glubran 2) | NAO/EBPM Therapy (Glubran 2) |
| Samples of patients (n=) | 13 | 6 | 2 | 4 | 1 |
| Anticoagulant or antiaggregant administration via os | 13 | si | no | si | no |
| Drainage amount at 3 h (cc) | 10 | 3 | 3 | 4 | 4 |
| Drainage amount at 6 h (cc) | 10 | 3 | 3 | 6 | 6 |
| Drainage amount at 24 h (cc) | 10 | 3 | 3 | 6 | 5 |
| Hematoma at 24 h | 10 | si | si | si | si |
| Hematoma at 7 days | 10 | no | no | si | si |
| Hematomaat 30 days (pz.%) | 10 | no | no | no | no |
| Wound healing Vycryl point (pz.%) | 10 | 100 | 100 | 95 | 96 |
| Wound healing Metal clips (pz.%) | 10 | 100 | 100 | 96 | 90 |
| Sealant Types | Haemostatic Success (%) | Haemostasis Time (min) | Haemostatic Insuccess | p-Value |
| ARISTATMAH | 94 | 5 | 6 | 0.018 |
| GLUBRAN 2 | 98 | 2 | 2 | 0.052 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Curcio, F.; Perri, P.; Piro, P.; Galassi, S.; Sole, R.; Trombino, S.; Cassano, R. Synthetic Haemostatic Sealants: Effectiveness, Safety, and In Vivo Applications. Pharmaceuticals 2024, 17, 288. https://doi.org/10.3390/ph17030288
Curcio F, Perri P, Piro P, Galassi S, Sole R, Trombino S, Cassano R. Synthetic Haemostatic Sealants: Effectiveness, Safety, and In Vivo Applications. Pharmaceuticals. 2024; 17(3):288. https://doi.org/10.3390/ph17030288
Chicago/Turabian StyleCurcio, Federica, Paolo Perri, Paolo Piro, Stefania Galassi, Roberta Sole, Sonia Trombino, and Roberta Cassano. 2024. "Synthetic Haemostatic Sealants: Effectiveness, Safety, and In Vivo Applications" Pharmaceuticals 17, no. 3: 288. https://doi.org/10.3390/ph17030288
APA StyleCurcio, F., Perri, P., Piro, P., Galassi, S., Sole, R., Trombino, S., & Cassano, R. (2024). Synthetic Haemostatic Sealants: Effectiveness, Safety, and In Vivo Applications. Pharmaceuticals, 17(3), 288. https://doi.org/10.3390/ph17030288