
2023 FDA TIDES (Peptides and Oligonucleotides) Harvest

 ,
,  ,
,  and
and 
Abstract
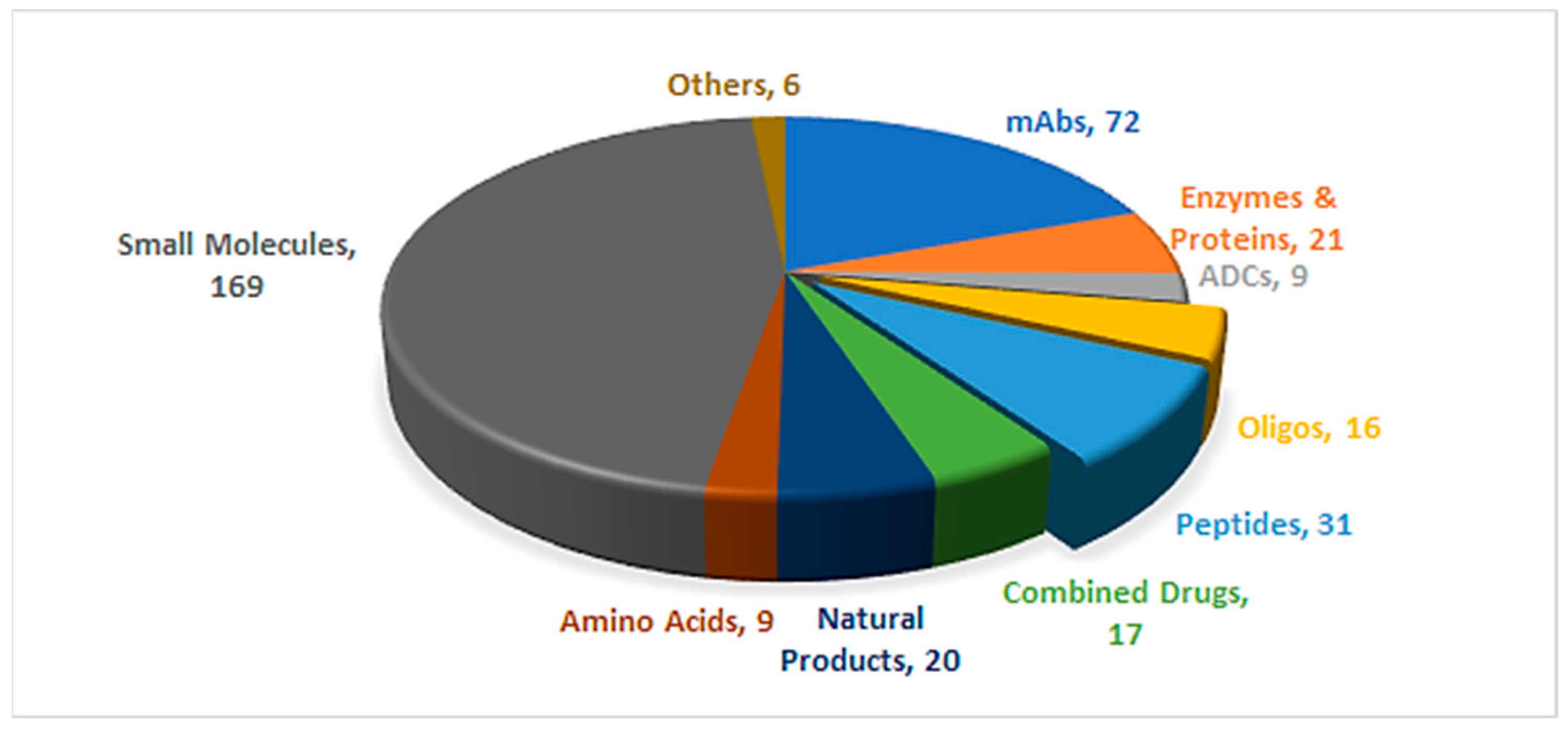
1. Introduction
2. Oligonucleotides
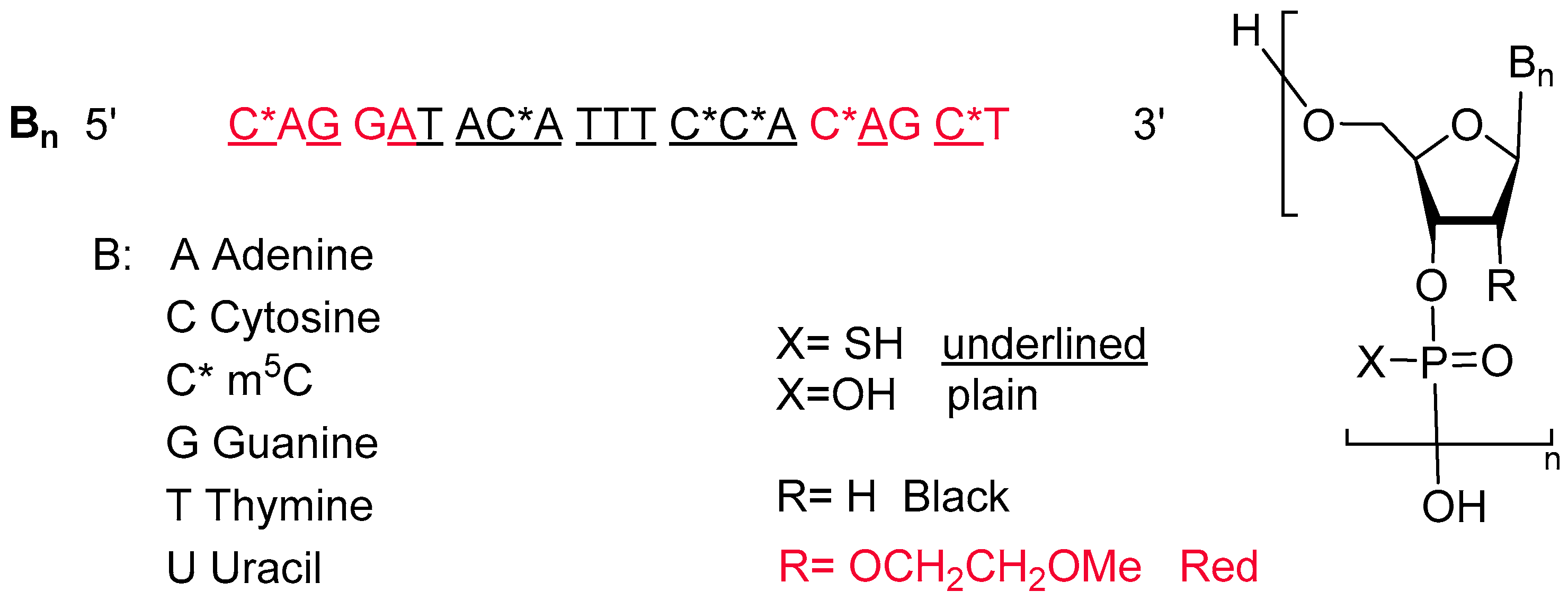
2.1. Tofersen (QalsodyTM)
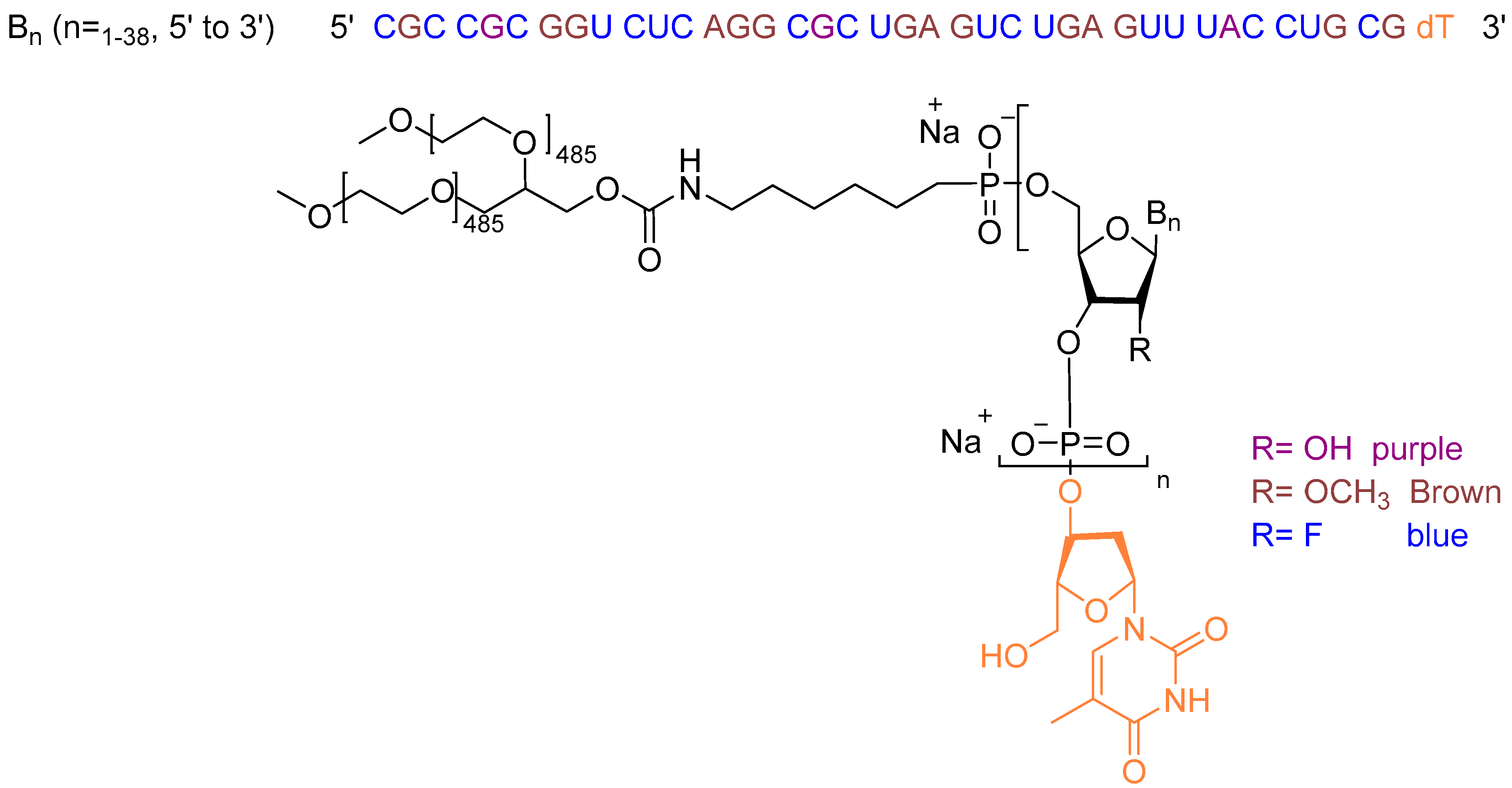
2.2. Avacincaptad Pegol (IzervayTM)
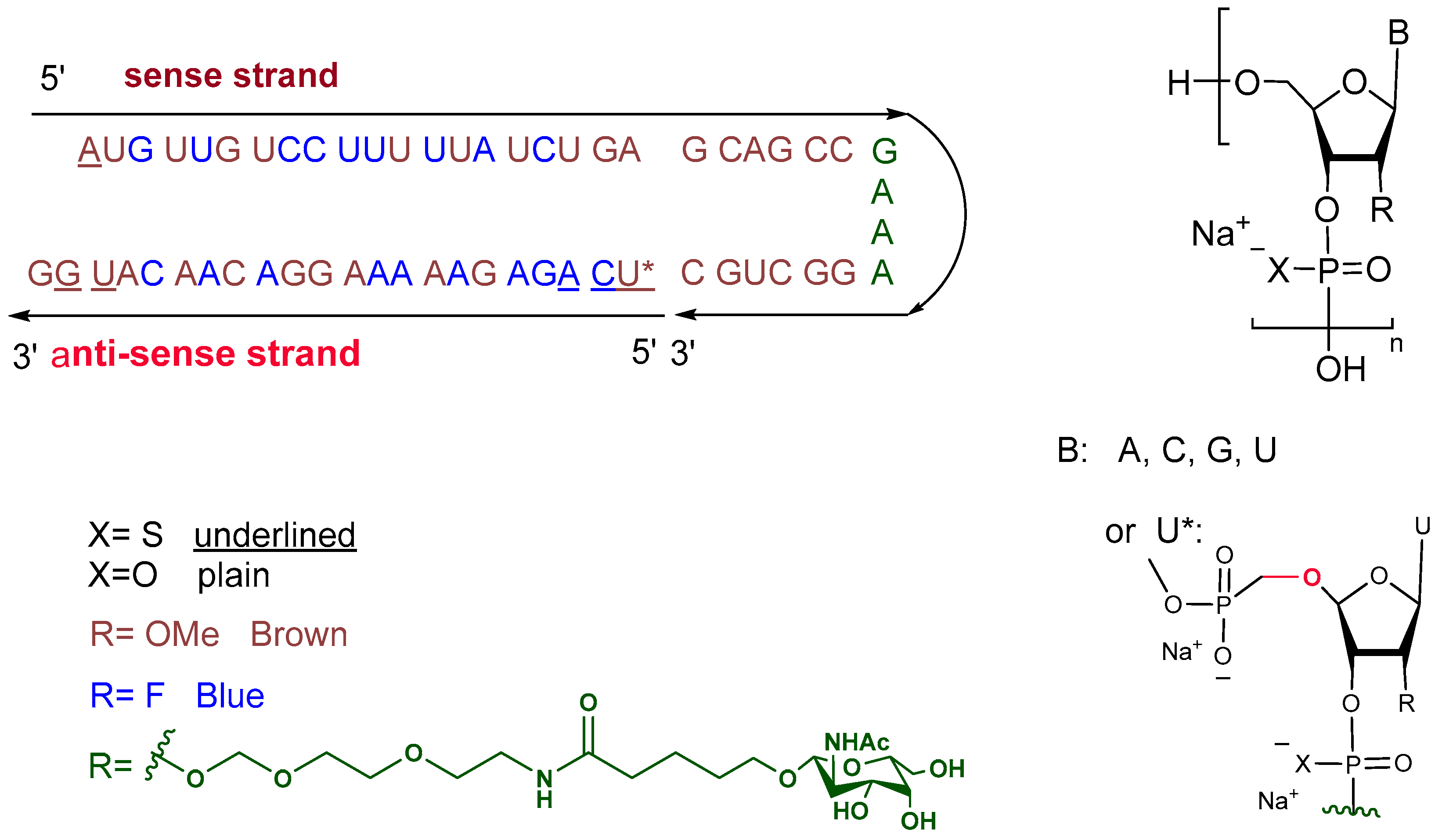
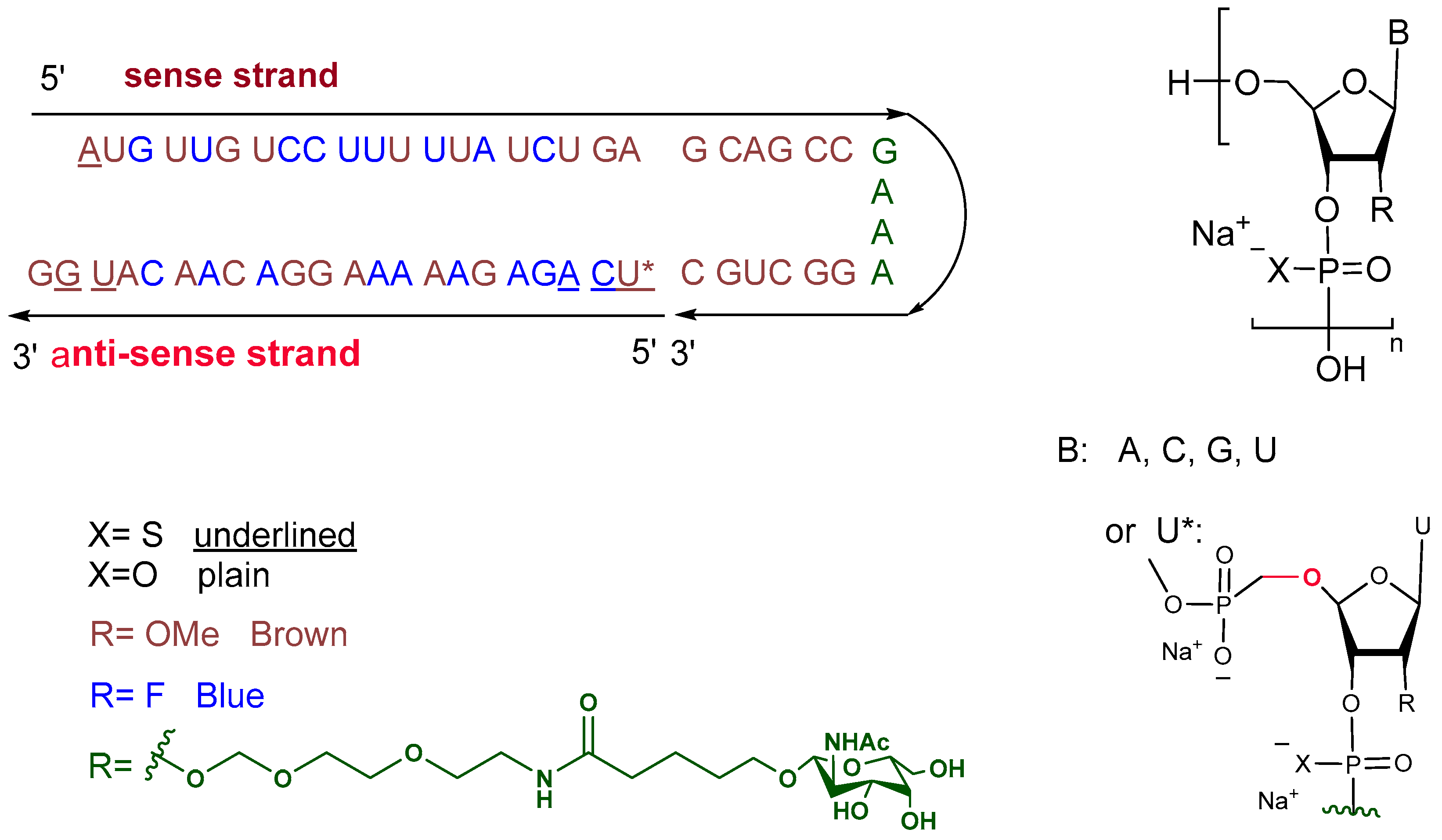
2.3. Nedosiran (RivflozaTM)
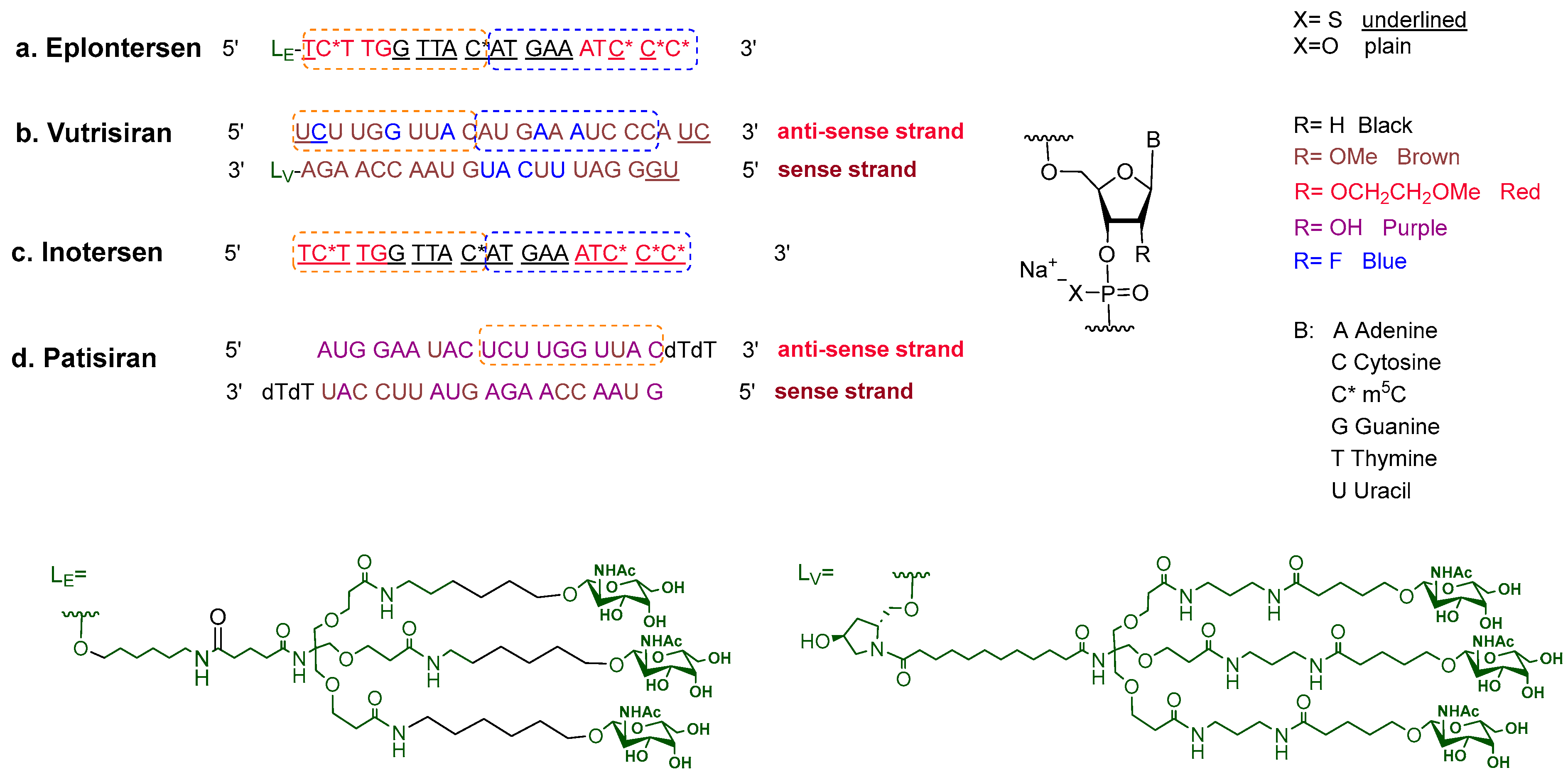
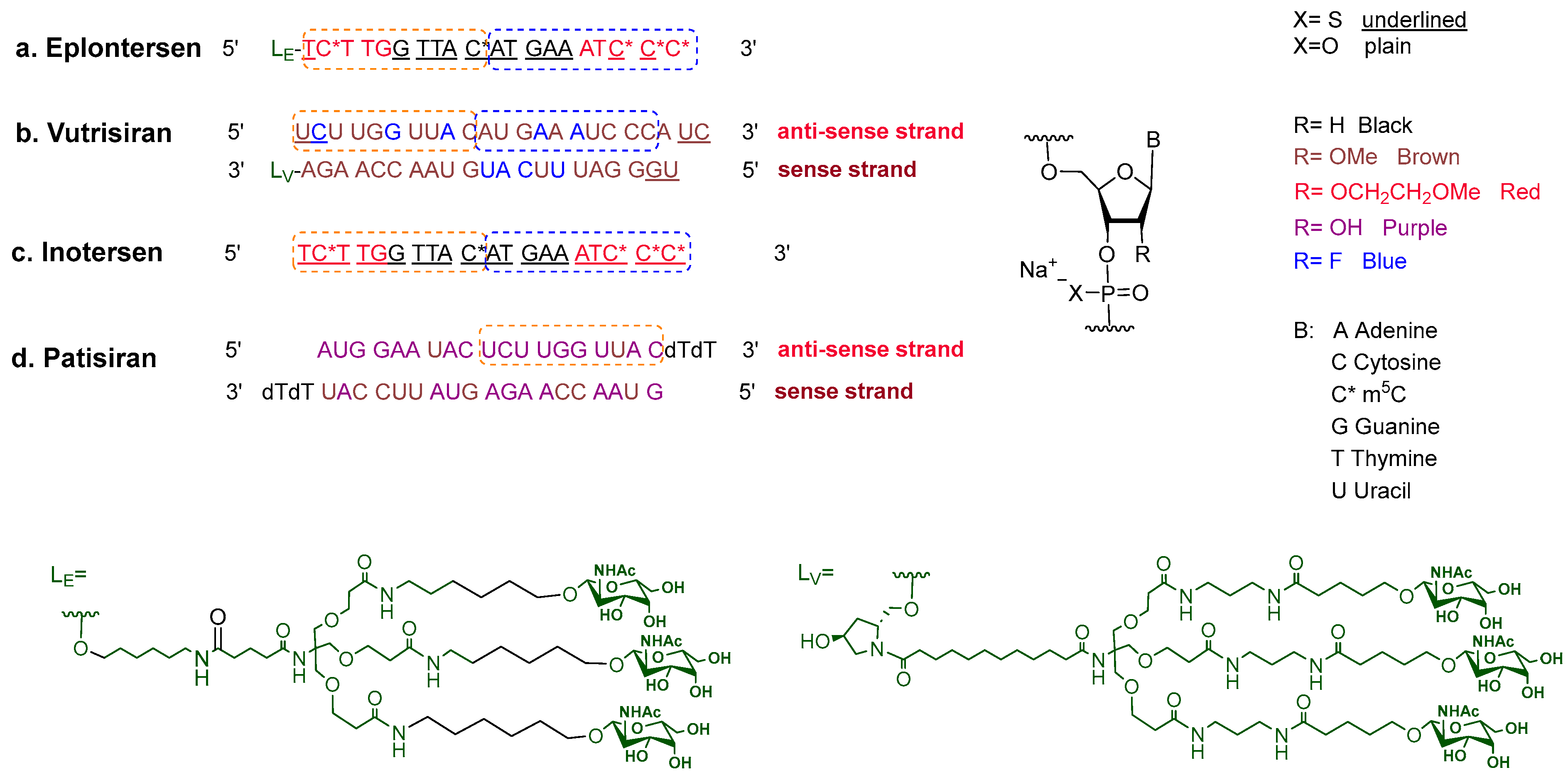
2.4. Eplontersen (WainuaTM)
3. Peptides
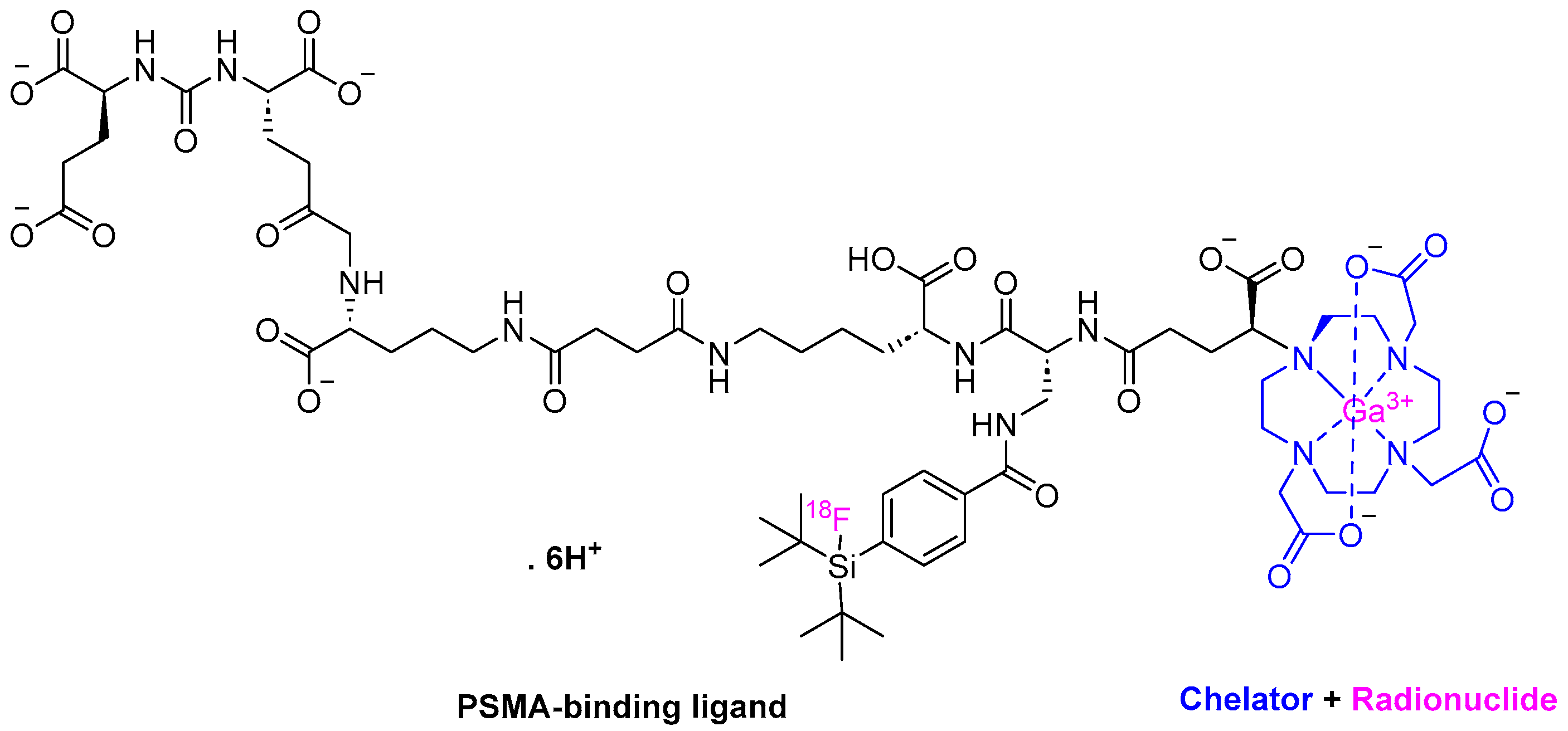
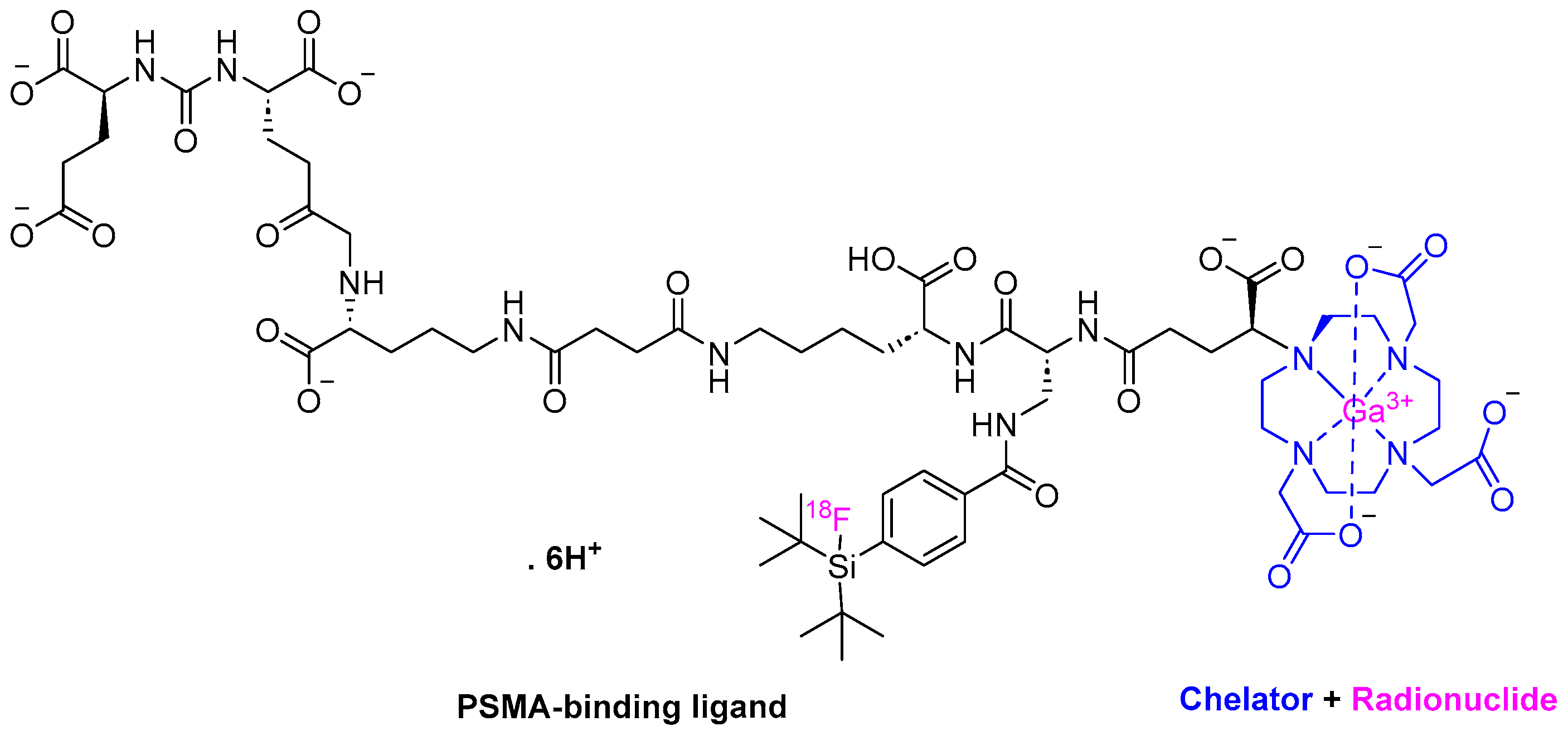
3.1. Flotufolastat F 18 (PoslumaTM)
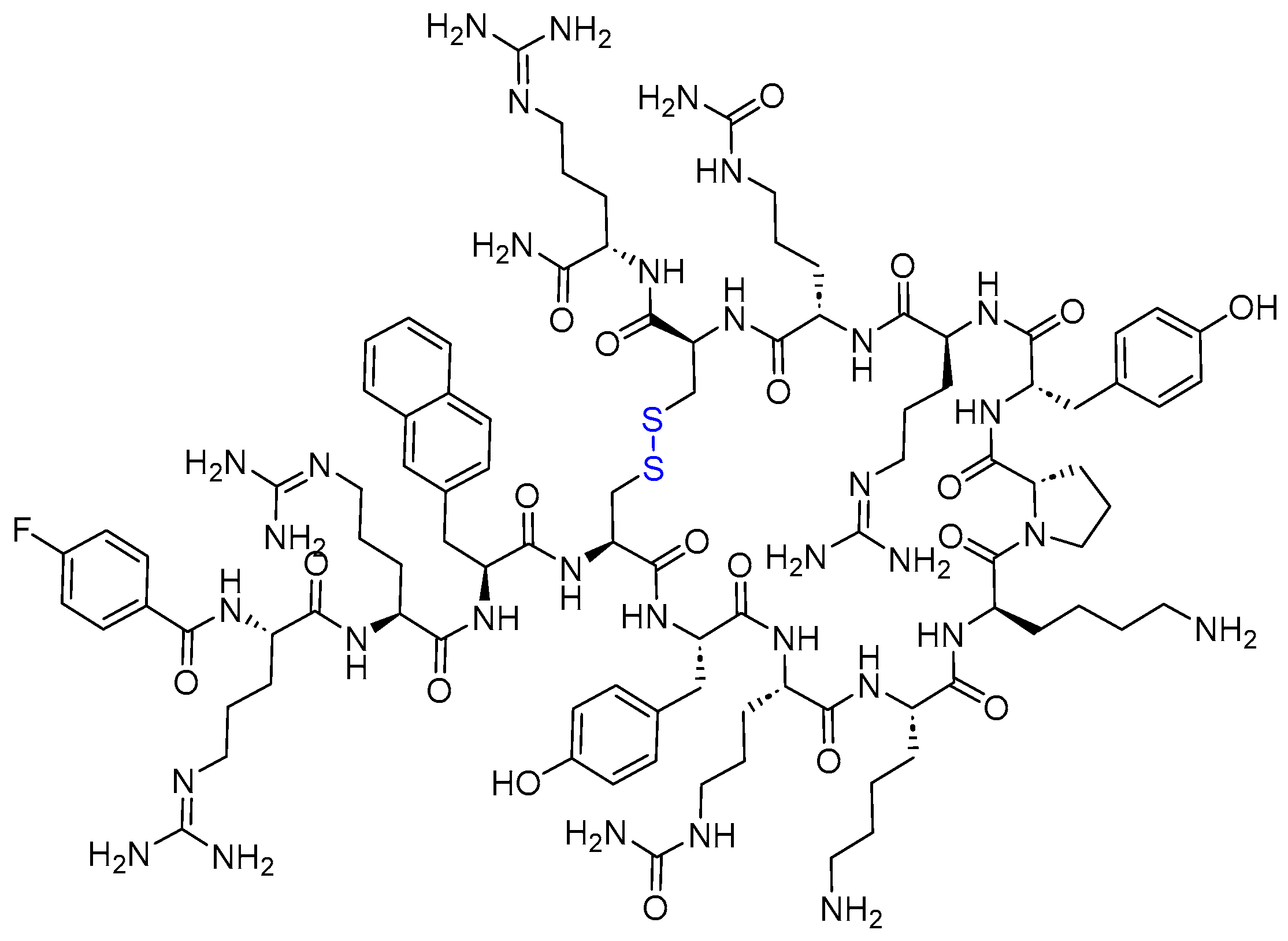
3.2. Motixafortide (AphexdaTM)
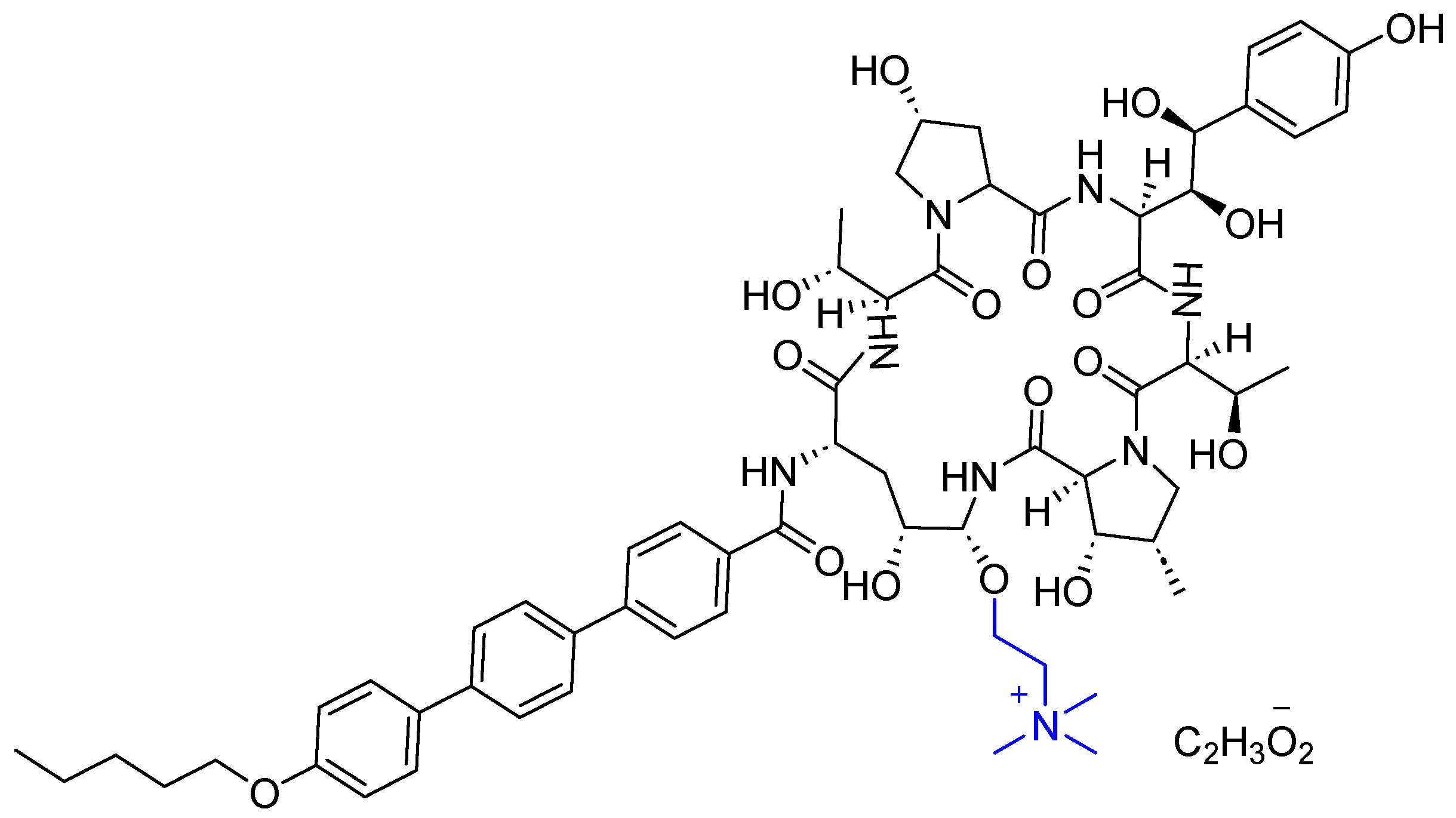
3.3. Rezafungin (RezzayoTM)
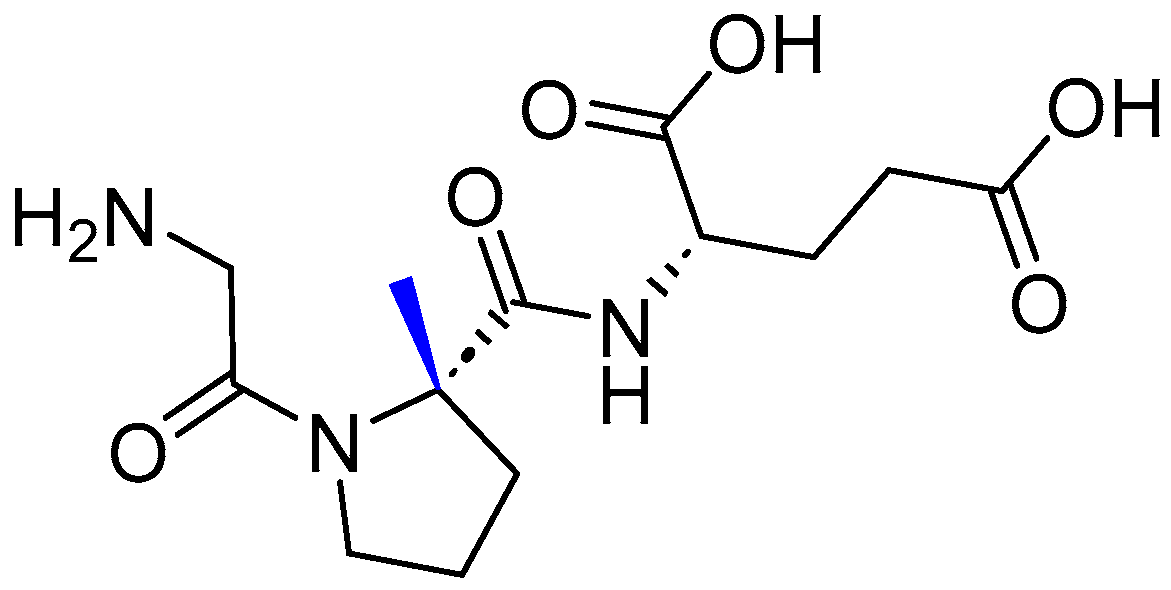
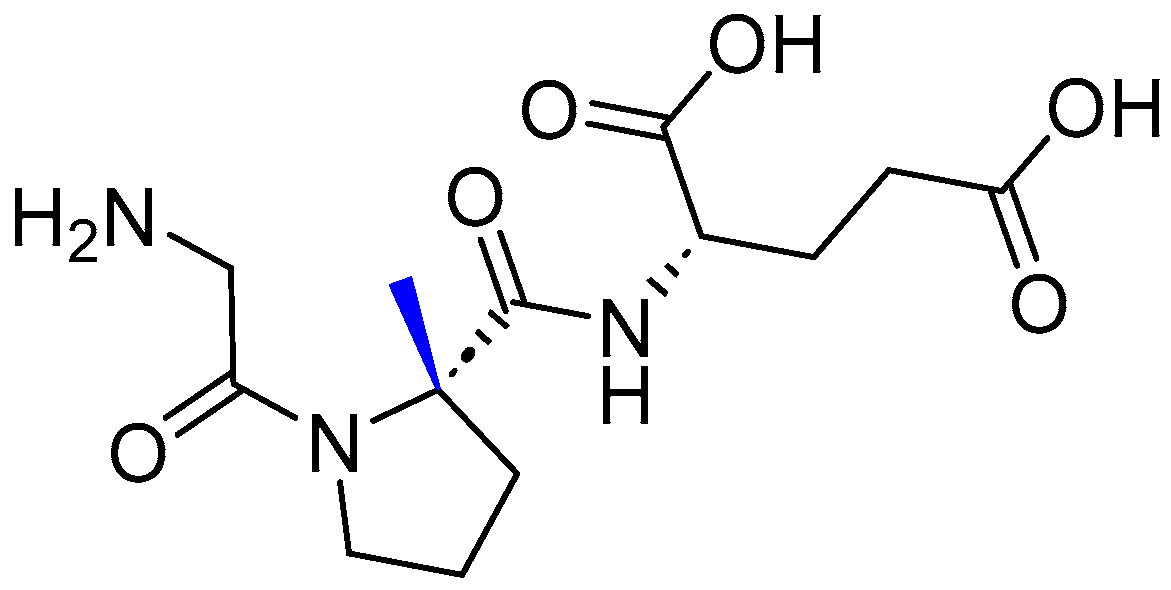
3.4. Trofinetide (DaybueTM)
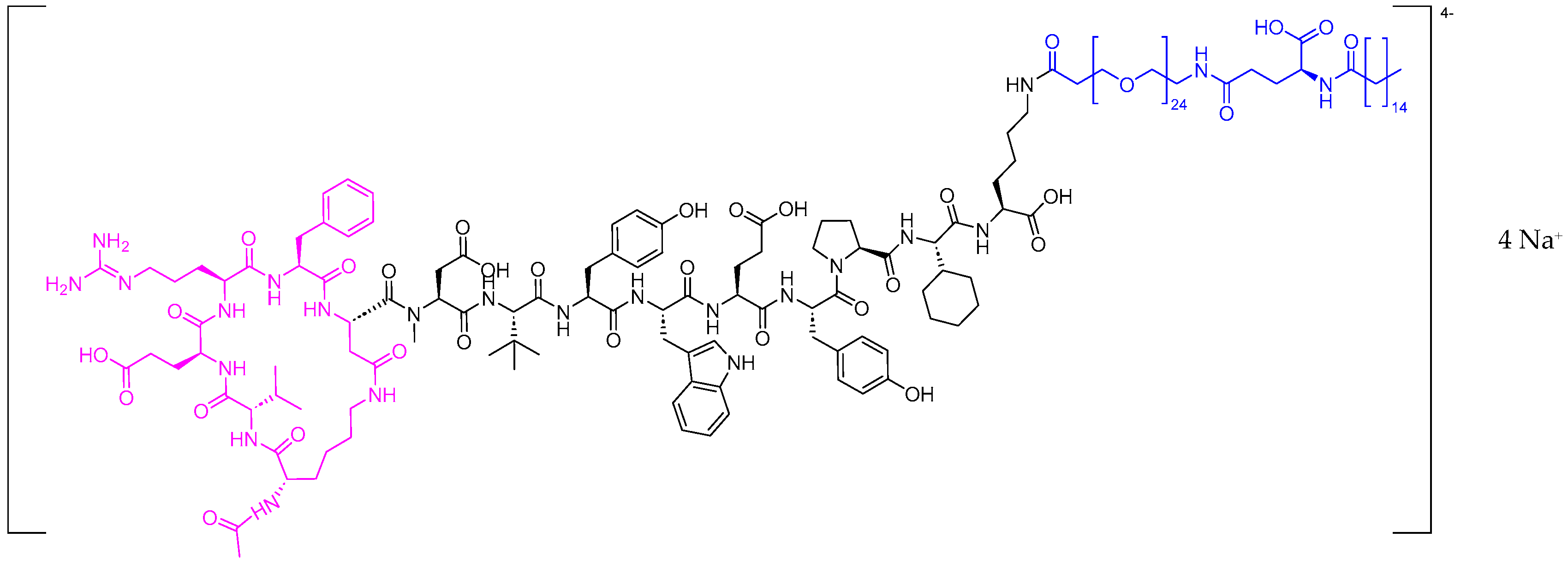
3.5. Zilucoplan (ZilbrysqTM)
4. Conclusions
Funding
Conflicts of Interest
References
- Mullard, A. 2023 FDA approvals. Nat. Rev. 2024. [Google Scholar] [CrossRef] [PubMed]
- Al Musaimi, O.; Al Shaer, D.; Albericio, F.; de la Torre, B.G. 2022 FDA TIDES (Peptides and Oligonucleotides) Harvest. Pharmaceuticals 2023, 16, 336. [Google Scholar] [CrossRef]
- de la Torre, B.G.; Albericio, F. The Pharmaceutical Industry in 2023: An Analysis of FDA Drug Approvals from the Perspective of Molecules. Molecules 2024, 29, 585. [Google Scholar] [CrossRef]
- Dicerna Pharmaceuticals GalXC™ and GalXC-Plus™ Technologies. Available online: https://www.novonordisk-us.com/ (accessed on 8 February 2024).
- Al Shaer, D.; Al Musaimi, O.; Albericio, F.; de la Torre, B.G. 2019 FDA TIDES (Peptides and Oligonucleotides) Harvest. Pharmaceuticals 2020, 13, 40. [Google Scholar] [CrossRef]
- Al Musaimi, O.; Lombardi, L.; Williams, D.R.; Albericio, F. Strategies for Improving Peptide Stability and Delivery. Pharmaceuticals 2022, 15, 1283. [Google Scholar] [CrossRef] [PubMed]
- Al Shaer, D.; Al Musaimi, O.; Albericio, F.; de la Torre, B.G. 2021 FDA TIDES (Peptides and Oligonucleotides) Harvest. Pharmaceuticals 2022, 15, 222. [Google Scholar] [CrossRef] [PubMed]
- QALSODY Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215887s000lbl.pdf (accessed on 8 February 2024).
- Blair, H.A. Tofersen: First Approval. Drugs 2023, 83, 1039–1043. [Google Scholar] [CrossRef]
- IZERVAY Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217225s000lbl.pdf (accessed on 8 February 2024).
- Kang, C. Avacincaptad Pegol: First Approval. Drugs 2023, 83, 1447–1453. [Google Scholar] [CrossRef]
- Jaffe, G.J.; Westby, K.; Csaky, K.G.; Monés, J.; Pearlman, J.A.; Patel, S.S.; Joondeph, B.C.; Randolph, J.; Masonson, H.; Rezaei, K.A. C5 Inhibitor Avacincaptad Pegol for Geographic Atrophy Due to Age-Related Macular Degeneration: A Randomized Pivotal Phase 2/3 Trial. Ophthalmology 2021, 128, 576–586. [Google Scholar] [CrossRef]
- RIVFLOZA Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/215842s000lbl.pdf (accessed on 8 February 2024).
- Syed, Y.Y. Nedosiran: First Approval. Drugs 2023, 83, 1729–1733. [Google Scholar] [CrossRef]
- Lai, C.; Pursell, N.; Gierut, J.; Saxena, U.; Zhou, W.; Dills, M.; Diwanji, R.; Dutta, C.; Koser, M.; Nazef, N.; et al. Specific Inhibition of Hepatic Lactate Dehydrogenase Reduces Oxalate Production in Mouse Models of Primary Hyperoxaluria. Mol. Ther. 2018, 26, 1983–1995. [Google Scholar] [CrossRef]
- Oxlumo Approval Letter. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2020/214103Orig1s000ltr.pdf (accessed on 16 January 2021).
- WAINU Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217388s000lbl.pdf (accessed on 8 February 2024).
- WAINUA™ (Eplontersen). Available online: https://www.astrazeneca.com/media-centre/press-releases/2023/wainua-eplontersen-granted-first-ever-regulatory-approval-us-treatment-of-adults-with-polyneuropathy-hereditary-transthyretin-mediated-amyloidosis.html. (accessed on 8 February 2024).
- Mazzeo, A.; Russo, M.; Di Bella, G.; Minutoli, F.; Stancanelli, C.; Gentile, L.; Baldari, S.; Carerj, S.; Toscano, A.; Vita, G. Transthyretin-Related Familial Amyloid Polyneuropathy (TTR-FAP): A Single-Center Experience in Sicily, an Italian Endemic Area. J. Neuromuscul. Dis. 2015, 2, S39–s48. [Google Scholar] [CrossRef]
- Luigetti, M.; Romano, A.; Di Paolantonio, A.; Bisogni, G.; Sabatelli, M. Diagnosis and Treatment of Hereditary Transthyretin Amyloidosis (hATTR) Polyneuropathy: Current Perspectives on Improving Patient Care. Ther. Clin. Risk Manag. 2020, 16, 109–123. [Google Scholar] [CrossRef]
- Al Shaer, D.; Al Musaimi, O.; Albericio, F.; de la Torre, B.G. 2018 FDA Tides Harvest. Pharmaceuticals 2019, 12, 52. [Google Scholar] [CrossRef]
- Butler, J.S.; Chan, A.; Costelha, S.; Fishman, S.; Willoughby, J.L.; Borland, T.D.; Milstein, S.; Foster, D.J.; Goncalves, P.; Chen, Q.; et al. Preclinical evaluation of RNAi as a treatment for transthyretin-mediated amyloidosis. Amyloid 2016, 23, 109–118. [Google Scholar] [CrossRef]
- Coelho, T.; Maia, L.F.; Martins da Silva, A.; Waddington Cruz, M.; Planté-Bordeneuve, V.; Lozeron, P.; Suhr, O.B.; Campistol, J.M.; Conceição, I.M.; Schmidt, H.H.; et al. Tafamidis for transthyretin familial amyloid polyneuropathy: A randomized, controlled trial. Neurology 2012, 79, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Heo, Y.-A. Flotufolastat F 18: Diagnostic First Approval. Mol. Diagn. Ther. 2023, 27, 631–636. [Google Scholar] [CrossRef]
- Posluma Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/216023s000lbl.pdf (accessed on 8 February 2024).
- Murthy, V.; Aggarwal, R.; Koo, P.J. The Emerging Role of Next-Generation Imaging in Prostate Cancer. Curr. Oncol. Rep. 2022, 24, 33–42. [Google Scholar] [CrossRef]
- Werner, R.A.; Derlin, T.; Lapa, C.; Sheikbahaei, S.; Higuchi, T.; Giesel, F.L.; Behr, S.; Drzezga, A.; Kimura, H.; Buck, A.K.; et al. (18)F-Labeled, PSMA-Targeted Radiotracers: Leveraging the Advantages of Radiofluorination for Prostate Cancer Molecular Imaging. Theranostics 2020, 10, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Iwata, Y.; Kawamoto, M.; Yoshizawa, Y. Half-life of 68Ga. Appl. Radiat. Isot. 1983, 34, 1537–1540. [Google Scholar] [CrossRef]
- Al Musaimi, O.; Al Shaer, D.; Albericio, F.; de la Torre, B.G. 2020 FDA TIDES (Peptides and Oligonucleotides) Harvest. Pharmaceuticals 2021, 14, 145. [Google Scholar] [CrossRef]
- Wurzer, A.; Di Carlo, D.; Schmidt, A.; Beck, R.; Eiber, M.; Schwaiger, M.; Wester, H.J. Radiohybrid Ligands: A Novel Tracer Concept Exemplified by (18)F- or (68)Ga-Labeled rhPSMA Inhibitors. J. Nucl. Med. 2020, 61, 735–742. [Google Scholar] [CrossRef]
- Kroenke, M.; Schweiger, L.; Horn, T.; Haller, B.; Schwamborn, K.; Wurzer, A.; Maurer, T.; Wester, H.J.; Eiber, M.; Rauscher, I. Validation of (18)F-rhPSMA-7 and (18)F-rhPSMA-7.3 PET Imaging Results with Histopathology from Salvage Surgery in Patients with Biochemical Recurrence of Prostate Cancer. J. Nucl. Med. 2022, 63, 1809–1814. [Google Scholar] [CrossRef]
- Rauscher, I.; Karimzadeh, A.; Schiller, K.; Horn, T.; D’Alessandria, C.; Franz, C.; Wörther, H.; Nguyen, N.; Combs, S.E.; Weber, W.A.; et al. Detection efficacy of (18)F-rhPSMA-7.3 PET/CT and impact on patient management in patients with biochemical recurrence of prostate cancer after radical prostatectomy and prior to potential salvage treatment. J. Nucl. Med. 2021, 62, 1719–1726. [Google Scholar] [CrossRef]
- Langbein, T.; Wang, H.; Rauscher, I.; Kroenke, M.; Knorr, K.; Wurzer, A.; Schwamborn, K.; Maurer, T.; Horn, T.; Haller, B.; et al. Utility of (18)F-rhPSMA-7.3 PET for Imaging of Primary Prostate Cancer and Preoperative Efficacy in N-Staging of Unfavorable Intermediate- to Very High-Risk Patients Validated by Histopathology. J. Nucl. Med. 2022, 63, 1334–1342. [Google Scholar] [CrossRef] [PubMed]
- Hoy, S.M. Motixafortide: First Approval. Drugs 2023, 83, 1635–1643. [Google Scholar] [CrossRef]
- Aphexda Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217159s000lbl.pdf (accessed on 8 February 2024).
- Miao, M.; De Clercq, E.; Li, G. Clinical significance of chemokine receptor antagonists. Expert Opin. Drug Metab. Toxicol. 2020, 16, 11–30. [Google Scholar] [CrossRef]
- Crees, Z.D.; Rettig, M.P.; DiPersio, J.F. Innovations in hematopoietic stem-cell mobilization: A review of the novel CXCR4 inhibitor motixafortide. Ther. Adv. Hematol. 2023, 14, 20406207231174304. [Google Scholar] [CrossRef]
- Abraham, M.; Pereg, Y.; Bulvik, B.; Klein, S.; Mishalian, I.; Wald, H.; Eizenberg, O.; Beider, K.; Nagler, A.; Golan, R.; et al. Single Dose of the CXCR4 Antagonist BL-8040 Induces Rapid Mobilization for the Collection of Human CD34(+) Cells in Healthy Volunteers. Clin. Cancer Res. 2017, 23, 6790–6801. [Google Scholar] [CrossRef] [PubMed]
- Rebolledo-Bustillo, M.; Garcia-Gomez, D.; Dávila, E.M.; Castro, M.E.; Caballero, N.A.; Melendez, F.J.; Baizabal-Aguirre, V.M.; Sanchez-Gaytan, B.L.; Perez-Aguilar, J.M. Structural Basis of the Binding Mode of the Antineoplastic Compound Motixafortide (BL-8040) in the CXCR4 Chemokine Receptor. Int. J. Mol. Sci. 2023, 24, 4393. [Google Scholar] [CrossRef] [PubMed]
- Bockorny, B.; Semenisty, V.; Macarulla, T.; Borazanci, E.; Wolpin, B.M.; Stemmer, S.M.; Golan, T.; Geva, R.; Borad, M.J.; Pedersen, K.S.; et al. BL-8040, a CXCR4 antagonist, in combination with pembrolizumab and chemotherapy for pancreatic cancer: The COMBAT trial. Nat. Med. 2020, 26, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Rezafungin: First Approval. Drugs 2023, 83, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Micafungin Approval Letter. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2005/21-506_Mycamine_Approv.pdf (accessed on 8 February 2024).
- Anidulafungin Approval Letter. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2006/21948s000_Eraxis_Approv.pdf (accessed on 8 February 2024).
- Caspofungin Approval Letter. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2001/21227_Cancidas_Approv.pdf (accessed on 8 February 2024).
- Rezzayo Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217417s000lbl.pdf (accessed on 8 February 2024).
- Garcia-Effron, G. Rezafungin-Mechanisms of Action, Susceptibility and Resistance: Similarities and Differences with the Other Echinocandins. J. Fungi 2020, 6, 262. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., 3rd; Soriano, A.; Cornely, O.A.; Kullberg, B.J.; Kollef, M.; Vazquez, J.; Honore, P.M.; Bassetti, M.; Pullman, J.; Chayakulkeeree, M.; et al. Rezafungin versus caspofungin for treatment of candidaemia and invasive candidiasis (ReSTORE): A multicentre, double-blind, double-dummy, randomised phase 3 trial. Lancet 2023, 401, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R.; Soriano, A.; Skoutelis, A.; Vazquez, J.A.; Honore, P.M.; Horcajada, J.P.; Spapen, H.; Bassetti, M.; Ostrosky-Zeichner, L.; Das, A.F.; et al. Rezafungin Versus Caspofungin in a Phase 2, Randomized, Double-blind Study for the Treatment of Candidemia and Invasive Candidiasis: The STRIVE Trial. Clin. Infect. Dis. 2021, 73, e3647–e3655. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R., III; Soriano, A.; Honore, P.M.; Bassetti, M.; Cornely, O.A.; Kollef, M.; Kullberg, B.J.; Pullman, J.; Hites, M.; Fortún, J.; et al. Efficacy and safety of rezafungin and caspofungin in candidaemia and invasive candidiasis: Pooled data from two prospective randomised controlled trials. Lancet Infect. Dis. 2023. [Google Scholar] [CrossRef]
- Neul, J.L.; Percy, A.K.; Benke, T.A.; Berry-Kravis, E.M.; Glaze, D.G.; Marsh, E.D.; Lin, T.; Stankovic, S.; Bishop, K.M.; Youakim, J.M. Trofinetide for the treatment of Rett syndrome: A randomized phase 3 study. Nat. Med. 2023, 29, 1468–1475. [Google Scholar] [CrossRef]
- Bickerdike, M.J.; Thomas, G.B.; Batchelor, D.C.; Sirimanne, E.S.; Leong, W.; Lin, H.; Sieg, F.; Wen, J.; Brimble, M.A.; Harris, P.W.; et al. NNZ-2566: A Gly–Pro–Glu analogue with neuroprotective efficacy in a rat model of acute focal stroke. J. Neurol. Sci. 2009, 278, 85–90. [Google Scholar] [CrossRef]
- Rett, A. On a unusual brain atrophy syndrome in hyperammonemia in childhood. Wien Med. Wochenschr. 1966, 116, 723–726. [Google Scholar]
- Jeffrey, L.N.; Kaufmann, W.E.; Glaze, D.G.; Christodoulou, J.; Clarke, A.J.; Bahi-Buisson, N.; Leonard, H.; Bailey, M.E.S.; Schanen, N.C.; Zappella, M.; et al. Rett syndrome: Revised diagnostic criteria and nomenclature. Ann. Neurol. 2010, 68, 944–950. [Google Scholar] [CrossRef]
- Motil, K.J.; Caeg, E.; Barrish, J.O.; Geerts, S.; Lane, J.B.; Percy, A.K.; Annese, F.; McNair, L.; Skinner, S.A.; Lee, H.S.; et al. Gastrointestinal and nutritional problems occur frequently throughout life in girls and women with Rett syndrome. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 292–298. [Google Scholar] [CrossRef]
- Valenti, D.; Vacca, R.A. Brain Mitochondrial Bioenergetics in Genetic Neurodevelopmental Disorders: Focus on Down, Rett and Fragile X Syndromes. Int. J. Mol. Sci. 2023, 24, 12488. [Google Scholar] [CrossRef]
- Daybue Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217026s000lbl.pdf (accessed on 8 February 2024).
- Zilbrysq Drug Label. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/216834s000lbl.pdf (accessed on 8 February 2024).
- Menon, D.; Bril, V. Pharmacotherapy of Generalized Myasthenia Gravis with Special Emphasis on Newer Biologicals. Drugs 2022, 82, 865–887. [Google Scholar] [CrossRef] [PubMed]
- Gilhus, N.E.; Tzartos, S.; Evoli, A.; Palace, J.; Burns, T.M.; Verschuuren, J. Myasthenia gravis. Nat. Rev. Dis. Primers 2019, 5, 30. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.Q.; Tang, Y.; Dhamnaskar, K.; Hoarty, M.D.; Vyasamneni, R.; Vadysirisack, D.D.; Ma, Z.; Zhu, N.; Wang, J.G.; Bu, C.; et al. Zilucoplan, a macrocyclic peptide inhibitor of human complement component 5, uses a dual mode of action to prevent terminal complement pathway activation. Front. Immunol. 2023, 14, 1213920. [Google Scholar] [CrossRef] [PubMed]
- Krisinger, M.J.; Goebeler, V.; Lu, Z.; Meixner, S.C.; Myles, T.; Pryzdial, E.L.; Conway, E.M. Thrombin generates previously unidentified C5 products that support the terminal complement activation pathway. Blood 2012, 120, 1717–1725. [Google Scholar] [CrossRef] [PubMed]
- Foley, J.H.; Walton, B.L.; Aleman, M.M.; O’Byrne, A.M.; Lei, V.; Harrasser, M.; Foley, K.A.; Wolberg, A.S.; Conway, E.M. Complement Activation in Arterial and Venous Thrombosis is Mediated by Plasmin. EBioMedicine 2016, 5, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.F., Jr.; Bresch, S.; Genge, A.; Hewamadduma, C.; Hinton, J.; Hussain, Y.; Juntas-Morales, R.; Kaminski, H.J.; Maniaol, A.; Mantegazza, R.; et al. Safety and efficacy of zilucoplan in patients with generalised myasthenia gravis (RAISE): A randomised, double-blind, placebo-controlled, phase 3 study. Lancet Neurol. 2023, 22, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Karpova, D.; Bräuninger, S.; Wiercinska, E.; Krämer, A.; Stock, B.; Graff, J.; Martin, H.; Wach, A.; Escot, C.; Douglas, G.; et al. Mobilization of hematopoietic stem cells with the novel CXCR4 antagonist POL6326 (balixafortide) in healthy volunteers-results of a dose escalation trial. J. Transl. Med. 2017, 15, 2. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Active Ingredient (Trade Name) | Indication | Therapeutic Target | Administration Route |
|---|---|---|---|---|
| Oligonucleotides | ||||
| 1 | Tofersen (QalsodyTM) | To treat amyotrophic lateral sclerosis in adults who have an SOD1 gene mutation | Superoxide dismutase 1 (SOD1) mRNA | Intrathecally |
| 2 | Avacincaptad pegol (IzervayTM) | To treat geographic atrophy secondary to age-related macular degeneration | C5 complement protein | Intravitreally |
| 3 | Nedosiran (RivflozaTM) | To lower urinary oxalate levels in patients 9 years and older with primary hyperoxaluria type 1 and relatively preserved kidney function | RNA-induced silencing complex (RISC) | Subcutaneously |
| 4 | Eplontersen (WainuaTM) | To treat polyneuropathy of hereditary transthyretin-mediated amyloidosis | Transthyretin (TTR) mRNA | Subcutaneously |
| Peptides | ||||
| 5 | Flotufolastat F-18 (PoslumaTM) | To use with positron emission tomography (PET) imaging in certain patients with prostate cancer | Prostate-specific membrane antigen (PSMA) | Intravenously |
| 6 | Motixafortide (AphexdaTM) | To use with filgrastim (G-CSF) to mobilize hematopoietic stem cells to the peripheral blood for collection and subsequent autologous transplantation in patients with multiple myeloma | Chemokine receptor 4 (CXCR4) | Intramuscularly |
| 7 | Rezafungin (RezzayoTM) | To treat candidemia and invasive candidiasis | 1,3-β-D-glucan synthase enzyme | Intravenously |
| 8 | Trofinetide (DaybueTM) | To treat Rett syndrome | Inflammatory cytokines | Orally |
| 9 | Zilucoplan (ZilbrysqTM) | To treat generalized myasthenia gravis in adults who are anti-acetylcholine receptor (AChR) antibody-positive | C5 protein | Subcutaneously |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Shaer, D.; Al Musaimi, O.; Albericio, F.; de la Torre, B.G. 2023 FDA TIDES (Peptides and Oligonucleotides) Harvest. Pharmaceuticals 2024, 17, 243. https://doi.org/10.3390/ph17020243
Al Shaer D, Al Musaimi O, Albericio F, de la Torre BG. 2023 FDA TIDES (Peptides and Oligonucleotides) Harvest. Pharmaceuticals. 2024; 17(2):243. https://doi.org/10.3390/ph17020243
Chicago/Turabian StyleAl Shaer, Danah, Othman Al Musaimi, Fernando Albericio, and Beatriz G. de la Torre. 2024. "2023 FDA TIDES (Peptides and Oligonucleotides) Harvest" Pharmaceuticals 17, no. 2: 243. https://doi.org/10.3390/ph17020243
APA StyleAl Shaer, D., Al Musaimi, O., Albericio, F., & de la Torre, B. G. (2024). 2023 FDA TIDES (Peptides and Oligonucleotides) Harvest. Pharmaceuticals, 17(2), 243. https://doi.org/10.3390/ph17020243