
An Overview of Cancer in Djibouti: Current Status, Therapeutic Approaches, and Promising Endeavors in Local Essential Oil Treatment

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection of Information
2.2. Medicinal Plants of Djibouti: Study Area and Identification
2.3. Data Analysis
3. Results and Discussion
3.1. Analysis of Cancer Incidence Statistics in Djibouti
3.2. Cancer Risk Factors
3.2.1. Tobacco
3.2.2. Obesity
3.2.3. Air Pollution
3.2.4. Genetics
3.2.5. Infectious Agents
3.2.6. Occupational Exposure
3.2.7. Ionizing Radiation
3.3. Comprehensive Cancer Control: A Holistic Approach to Management and Care
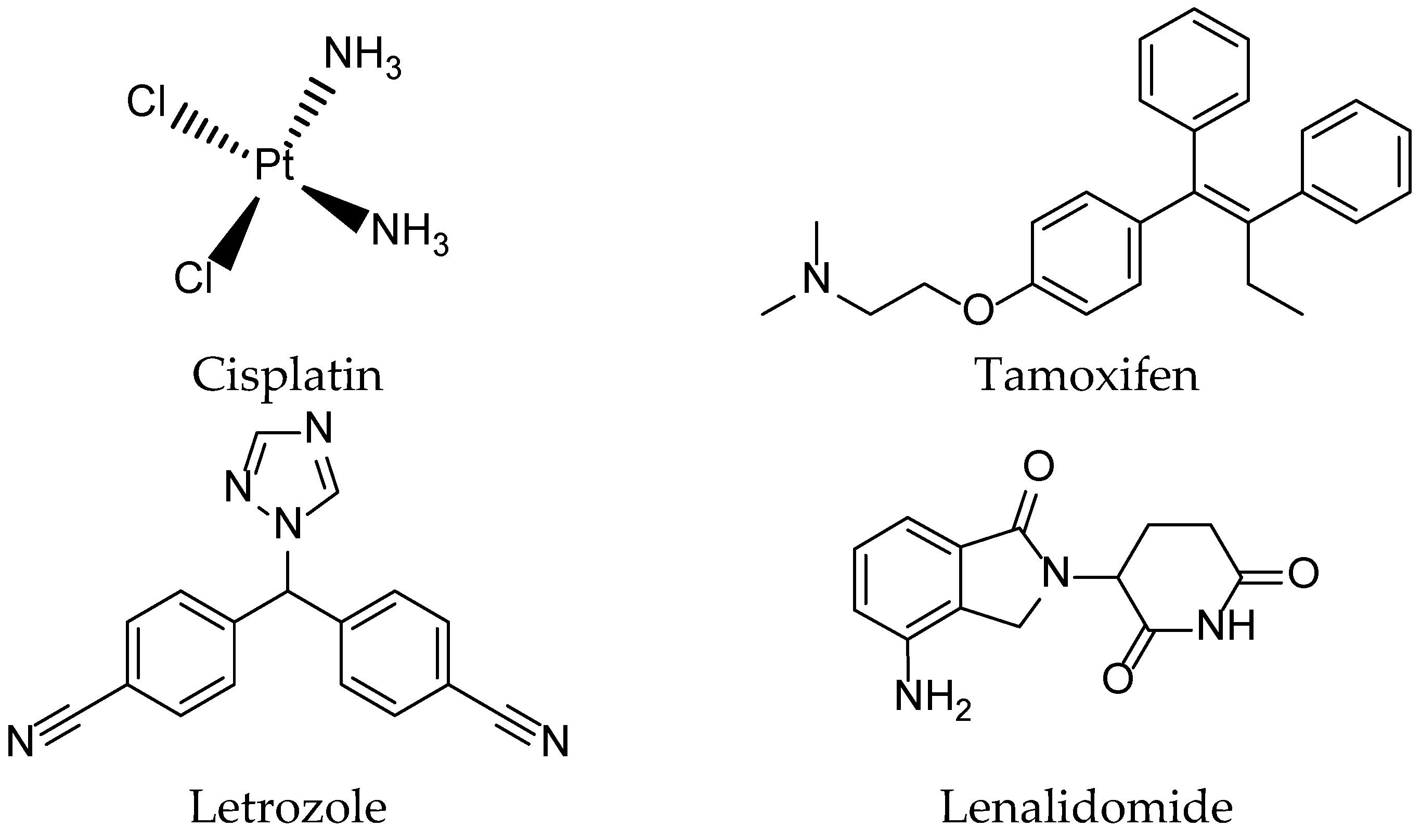
3.4. Medical Treatment of Cancer
3.5. Drugs in Clinical Stages
3.6. Complementary and Alternative Medicine and Dietary Patterns in Prevention and Supportive Cancer Care
3.6.1. Complementary and Alternative Medicine (CAM): A Synergy of Tradition and Innovation
3.6.2. Dietary Patterns: A Nutritional Tapestry for Health
3.7. Natural Productsfor Cancer Treatment
3.8. Use of Essential Oils from Djibouti in Cancer Treatments (In Vitro)
- Group 1: Contains the three active principles, namely Combrestatin A4, Doxorubicin, MMAE, and Vinblastine, used in cancer treatment, indicating the efficacy of this group in yielding positive cancer outcomes.
- Group 2: Encompasses the six essential oils Cymbopogon schoenanthus (L.) Spreng., Lavandula coronopifolia Poir., Nepeta azurea R.Br., Ocimum americanum L., Ocimum basilicum L. and Tagetes minuta L., suggesting promising results across all cell lines.
- Group 3: Comprises the MMAE active principle and the essential oil from Ruta chalepensis subsp. fumariifolia (Boiss. & Heldr.) Nyman, indicating a similarity in activity against all cell lines tested.
3.9. Limitations of the Current Knowledge in Djibouti—Perspectives
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yu, X.; Qin, W.; Lin, X.; Shan, Z.; Huang, L.; Shao, Q.; Chen, M. Synergizing the enhanced RIME with fuzzy k-nearest neighbor for diagnose of pulmonary hypertension. Comput. Biol. Med. 2023, 165, 107408. [Google Scholar] [CrossRef]
- Yuan, C.; Kim, J.; Wang, Q.L.; Lee, A.A.; Babic, A.; Amundadottir, L.T.; Stampfer, M.J. The age-dependent association of risk factors with pancreatic cancer. Ann. Oncol. 2022, 33, 693–701. [Google Scholar] [CrossRef]
- Jakobsen, E.; Olsen, K.E.; Bliddal, M.; Hornbak, M.; Persson, G.F.; Green, A. Forecasting lung cancer incidence, mortality, and prevalence to year 2030. BMC Cancer 2021, 21, 985. [Google Scholar] [CrossRef]
- Gutiérrez-Cuevas, J.; Lucano-Landeros, S.; López-Cifuentes, D.; Santos, A.; Armendariz-Borunda, J. Epidemiologic, genetic, pathogenic, metabolic, epigenetic aspects involved in Nash-hcc: Current therapeutic strategies. Cancers 2022, 15, 23. [Google Scholar] [CrossRef]
- Yu, Z.; Zhou, X.; Wang, X. Metabolic reprogramming in hematologic malignancies: Advances and clinical perspectives. Cancer Res. 2022, 82, 2955–2963. [Google Scholar] [CrossRef]
- Wang, Z.; Yang, B. Polypharmacology in Clinical Applications—Anticancer Polypharmacology. In Polypharmacology: Principles and Methodologies; Springer International Publishing: Cham, Switzerland, 2022; pp. 73–132. [Google Scholar]
- Lei, Z.N.; Tian, Q.; Teng, Q.X.; Wurpel, J.N.; Zeng, L.; Pan, Y.; Chen, Z.S. Understanding and targeting resistance mechanisms in cancer. MedComm 2023, 4, e265. [Google Scholar] [CrossRef]
- Zeichner, S.B.; Terawaki, H.; Gogineni, K. A review of systemic treatment in metastatic triple-negative breast cancer. Breast Cancer Basic Clin. Res. 2016, 10, BCBCR-S32783. [Google Scholar] [CrossRef]
- Florea, A.M.; Büsselberg, D. Cisplatin as an anti-tumor drug: Cellular mechanisms of activity, drug resistance and induced side effects. Cancers 2011, 3, 1351–1371. [Google Scholar] [CrossRef]
- Shlyakhtina, Y.; Moran, K.L.; Portal, M.M. Genetic and non-genetic mechanisms underlying cancer evolution. Cancers 2021, 13, 1380. [Google Scholar] [CrossRef]
- Ainane, T.; Abourriche, A.; Oukkache, N.; Lamdini, H.; Hammouti, B.; Bennamara, A. DNA affinity screening of extracts tunicate Cynthia squamulata from the Atlantic coast. Der Pharma Chemica 2015, 7, 45–49. [Google Scholar]
- Ganesh, K.; Massague, J. Targeting metastatic cancer. Nat. Med. 2021, 27, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Zafar, F.; Asif, H.M.; Shaheen, G.; Ghauri, A.O.; Rajpoot, S.R.; Tasleem, M.W.; Shamim, T.; Hadi, F.; Noor, R.; Ali, T.; et al. A comprehensive review on medicinal plants possessing antioxidant potential. Clin. Exp. Pharmacol. Physiol. 2023, 50, 205–217. [Google Scholar] [CrossRef]
- Khammassi, M.; Ayed, R.B.; Khedhiri, S.; Souihi, M.; Hanana, M.; Amri, I.; Hamrouni, L. Crude extracts and essential oil of Platycladus orientalis (L.) Franco: A source of phenolics with antioxidant and antibacterial potential as assessed through a chemometric approach. Turk. J. Agric. For. 2022, 46, 477–487. [Google Scholar] [CrossRef]
- Çelebi, Ö.; Fidan, H.; Iliev, I.; Petkova, N.; Dincheva, I.; Gandova, V.; Stankov, S.; Stoyanova, A. Chemical composition, biological activities, and surface tension properties of Melissa officinalis L. essential oil. Turk. J. Agric. For. 2023, 47, 67–78. [Google Scholar] [CrossRef]
- Soleimani, N.; Javadi, M.M. Future prospects of bacteria-mediated cancer therapies: Affliction or opportunity? Microb. Pathog. 2022, 172, 105795. [Google Scholar] [CrossRef] [PubMed]
- Ainane, A.; Abdoul-Latif, F.M.; Ali, A.M.; Mohamed, J.; Shybat, Z.L.; Ainane, T. Chemical composition of Juniperus communis L. essential oil and evaluation of its antifungal activity in vitro against Ascochyta rabiei. J. Anal. Sci. Appl. Biotechnol. 2022, 4, 108–115. [Google Scholar]
- Abdoul-Latif, F.M.; Elmi, A.; Merito, A.; Nour, M.; Risler, A.; Ainane, A.; Ainane, T. Essential oils of Tagetes minuta and Lavandula coronopifolia from Djibouti: Chemical composition, antibacterial activity and cytotoxic activity against various human cancer cell lines. Int. J. Plant Biol. 2022, 13, 315–329. [Google Scholar] [CrossRef]
- Abdoul-Latif, F.M.; Elmi, A.; Merito, A.; Nour, M.; Risler, A.; Ainane, A.; Ainane, T. Essential oils of Ocimum basilicum L. and Ocimum americanum L. from Djibouti: Chemical composition, antimicrobial and cytotoxicity evaluations. Processes 2022, 10, 1785. [Google Scholar] [CrossRef]
- Mohamed Abdoul-Latif, F.; Elmi, A.; Merito, A.; Nour, M.; Risler, A.; Ainane, A.; Ainane, T. Chemical Analysis of Essential Oils of Cymbopogon schoenanthus (L.) Spreng. and Nepeta azurea R. Br. ex Benth from Djbouti In-Vitro Cytotoxicity against Cancer Cell Lines and Antibacterial Activities. Appl. Sci. 2022, 12, 8699. [Google Scholar] [CrossRef]
- Abdoul-Latif, F.M.; Elmi, A.; Merito, A.; Nour, M.; Risler, A.; Ainane, A.; Ainane, T. Essential oil of Ruta chalepensis L. from Djibouti: Chemical Analysis and Modeling of In Vitro Anticancer Profiling. Separations 2022, 9, 387. [Google Scholar] [CrossRef]
- Mohamed Abdoul-Latif, F.; Ainane, A.; Houmed Aboubaker, I.; Merito Ali, A.; El Montassir, Z.; Kciuk, M.; Ainane, T. Chemical Composition of the Essential Oil of Catha edulis Forsk from Djibouti and Its Toxicological Investigations In Vivo and In Vitro. Processes 2023, 11, 1324. [Google Scholar] [CrossRef]
- Chhikara, B.S.; Parang, K. Global Cancer Statistics 2022: The trends projection analysis. Chem. Biol. Lett. 2023, 10, 451. [Google Scholar]
- Kashyap, D.; Pal, D.; Sharma, R.; Garg, V.K.; Goel, N.; Koundal, D.; Belay, A. Global increase in breast cancer incidence: Risk factors and preventive measures. BioMed Res. Int. 2022, 2022, 9605439. [Google Scholar] [CrossRef]
- Gupta, A.K.; Kanaan, M.; Siddiqi, K.; Sinha, D.N.; Mehrotra, R. Oral cancer risk assessment for different types of smokeless tobacco products sold worldwide: A review of reviews and meta-analyses. Cancer Prev. Res. 2022, 15, 733–746. [Google Scholar] [CrossRef]
- Basu, A.K. DNA damage, mutagenesis and cancer. Int. J. Mol. Sci. 2018, 19, 970. [Google Scholar] [CrossRef]
- Weng, M.W.; Lee, H.W.; Park, S.H.; Hu, Y.; Wang, H.T.; Chen, L.C.; Rom, W.N.; Huang, W.C.; Lepor, H.; Wu, X.R. Aldehydes are the predominant forces inducing DNA damage and inhibiting DNA repair in tobacco smoke carcinogenesis. Proc. Natl. Acad. Sci. USA 2018, 115, E6152–E6161. [Google Scholar] [CrossRef] [PubMed]
- Franchini, F.; Palatucci, G.; Colao, A.; Ungaro, P.; Macchia, P.E.; Nettore, I.C. Obesity and thyroid cancer risk: An update. Int. J. Environ. Res. Public Health 2022, 19, 1116. [Google Scholar] [CrossRef]
- Carroll, K.K. Obesity as a risk factor for certain types of cancer. Lipids 1998, 33, 1055–1059. [Google Scholar] [CrossRef]
- Xue, Y.; Wang, L.; Zhang, Y.; Zhao, Y.; Liu, Y. Air pollution: A culprit of lung cancer. J. Hazard. Mater. 2022, 434, 128937. [Google Scholar] [CrossRef]
- Ding, R.; Jin, Y.; Liu, X.; Zhu, Z.; Zhang, Y.; Wang, T.; Xu, Y. Characteristics of DNA methylation changes induced by traffic-related air pollution. Mutat. Res./Genet. Toxicol. Environ. Mutagen. 2016, 796, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Møller, P.; Folkmann, J.K.; Forchhammer, L.; Bräuner, E.V.; Danielsen, P.H.; Risom, L.; Loft, S. Air pollution, oxidative damage to DNA, and carcinogenesis. Cancer Lett. 2008, 266, 84–97. [Google Scholar] [CrossRef]
- Dai, Y.; Li, X.; Shi, J.; Leng, J. A review of the risk factors, genetics and treatment of endometriosis in Chinese women: A comparative update. Reprod. Health 2018, 15, 82. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.L.; Yu, S.J. Esophageal cancer: Risk factors, genetic association, and treatment. Asian J. Surg. 2018, 41, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Vineis, P.; Chuang, S.C.; Vaissière, T.; Cuenin, C.; Ricceri, F.; Genair/EPIC Collaborators; Johansson, M.; Ueland, P.; Brennan, P.; Herceg, Z. DNA methylation changes associated with cancer risk factors and blood levels of vitamin metabolites in a prospective study. Epigenetics 2011, 6, 195–201. [Google Scholar] [CrossRef] [PubMed]
- El-Zimaity, H.; Di Pilato, V.; Novella Ringressi, M.; Brcic, I.; Rajendra, S.; Langer, R.; Riddell, R. Risk factors for esophageal cancer: Emphasis on infectious agents. Ann. N. Y. Acad. Sci. 2018, 1434, 319–332. [Google Scholar] [CrossRef]
- Antonic, V.; Stojadinovic, A.; Kester, K.E.; Weina, P.J.; Brücher, B.L.; Protic, M.; Avital, I.; Izadjoo, M. Significance of infectious agents in colorectal cancer development. J. Cancer 2013, 4, 227. [Google Scholar] [CrossRef]
- Weiderpass, E.; Meo, M.; Vainio, H. Risk factors for breast cancer, including occupational exposures. Saf. Health Work. 2011, 2, 1–8. [Google Scholar] [CrossRef]
- Delclos, G.L.; Lerner, S.P. Occupational risk factors. Scand. J. Urol. Nephrol. 2008, 42 (Suppl. 218), 58–63. [Google Scholar] [CrossRef]
- Olfert, S.M.; Felknor, S.A.; Delclos, G.L. An updated review of the literature: Risk factors for bladder cancer with focus on occupational exposures. South. Med. J. 2006, 99, 1256–1264. [Google Scholar] [CrossRef]
- Rühm, W.; Laurier, D.; Wakeford, R. Cancer risk following low doses of ionising radiation—Current epidemiological evidence and implications for radiological protection. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2022, 873, 503436. [Google Scholar] [CrossRef] [PubMed]
- Goodman, J.E.; Nascarella, M.A.; Valberg, P.A. Ionizing radiation: A risk factor for mesothelioma. Cancer Causes Control 2009, 20, 1237–1254. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.J.; Smith, T.R.; Miller, M.S.; Lohman, K.; Case, L.D. Genetic regulation of ionizing radiation sensitivity and breast cancer risk. Environ. Mol. Mutagen. 2002, 39, 208–215. [Google Scholar] [CrossRef]
- Mao, J.J.; Pillai, G.G.; Andrade, C.J.; Ligibel, J.A.; Basu, P.; Cohen, L.; Salicrup, L.A. Integrative oncology: Addressing the global challenges of cancer prevention and treatment. CA Cancer J. Clin. 2022, 72, 144–164. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.L.; Banegas, M.P.; Acquati, C.; Chang, S.; Chino, F.; Conti, R.M.; Greenup, R.A.; Kroll, J.L.; Liang, M.I.; Pisu, M. Navigating financial toxicity in patients with cancer: A multidisciplinary management approach. CA Cancer J. Clin. 2022, 72, 437–453. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.E.; Bower, J.E.; Ganz, P.A. Cancer-related accelerated ageing and biobehavioural modifiers: A framework for research and clinical care. Nat. Rev. Clin. Oncol. 2022, 19, 173–187. [Google Scholar] [CrossRef]
- Akhoundova, D.; Rubin, M.A. Clinical application of advanced multi-omics tumor profiling: Shaping precision oncology of the future. Cancer Cell 2022, 40, 920–938. [Google Scholar] [CrossRef]
- Krishnasamy, M.; Hassan, H.; Jewell, C.; Moravski, I.; Lewin, T. Perspectives on Emotional Care: A Qualitative Study with Cancer Patients, Carers, and Health Professionals. Healthcare 2023, 11, 452. [Google Scholar] [CrossRef]
- Bussmann, S.; Vaganian, L.; Gerlach, A.L.; Kusch, M.; Labouvie, H.; Cwik, J.C. Screening and assessment for cancer patients’ psychosocial support needs: Development and validation of the psychosocial risk questionnaire. Eur. J. Oncol. Nurs. 2023, 63, 102240. [Google Scholar] [CrossRef]
- Tanay, M.A.L.; Roberts, J.; Ream, E. Humour in adult cancer care: A concept analysis. J. Adv. Nurs. 2013, 69, 2131–2140. [Google Scholar] [CrossRef]
- Goldingay, S.; Dieppe, P.; Farias, M. ‘And the pain just disappeared into insignificance’: The healing response in Lourdes–Performance, psychology and caring. Int. Rev. Psychiatry 2014, 26, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Rieger, K.L.; Hack, T.F.; Duff, M.A.; Campbell-Enns, H.J.; West, C.H. Integrating mindfulness and the expressive arts for meaning making in cancer care: A grounded theory of the processes, facilitators, and challenges. Support. Care Cancer 2023, 31, 475. [Google Scholar] [CrossRef] [PubMed]
- Zaszczyńska, A.; Niemczyk-Soczynska, B.; Sajkiewicz, P. A Comprehensive Review of Electrospun Fibers, 3D-Printed Scaffolds, and Hydrogels for Cancer Therapies. Polymers 2022, 14, 5278. [Google Scholar] [CrossRef] [PubMed]
- John, P.; Hodges, M.P.; Shah, G.; Dickerson, U.; Dreadin-Pulliam, J.; Smith, J.; Hendricks, C.B.; Mohamed, A.M. A quality improvement initiative to increase screening for financial coverage for breast cancer patients to decrease financial toxicity. J. Clin. Oncol. 2021, 39, 259. [Google Scholar] [CrossRef]
- Sawyers, C. Targeted cancer therapy. Nature 2004, 432, 294–297. [Google Scholar] [CrossRef]
- Mohamed Abdoul-Latif, F.; Ainane, A.; Houmed Aboubaker, I.; Mohamed, J.; Ainane, T. Exploring the Potent Anticancer Activity of Essential Oils and Their Bioactive Compounds: Mechanisms and Prospects for Future Cancer Therapy. Pharmaceuticals 2023, 16, 1086. [Google Scholar] [CrossRef]
- Iacopetta, D.; Ceramella, J.; Baldino, N.; Sinicropi, M.S.; Catalano, A. Targeting breast cancer: An overlook on current strategies. Int. J. Mol. Sci. 2023, 24, 3643. [Google Scholar] [CrossRef]
- Peng, Z. Current status of gendicine in China: Recombinant human Ad-p53 agent for treatment of cancers. Hum. Gene Ther. 2005, 16, 1016–1027. [Google Scholar] [CrossRef]
- Matuszak, N.; Suchorska, W.M.; Milecki, P.; Kruszyna-Mochalska, M.; Misiarz, A.; Pracz, J.; Malicki, J. FLASH Radiotherapy: An emerging approach in radiation therapy. Rep. Pract. Oncol. Radiother. 2022, 27, 343–351. [Google Scholar] [CrossRef]
- Lovelace, D.L.; McDaniel, L.R.; Golden, D. Long-term effects of breast cancer surgery, treatment, and survivor care. J. Midwifery Women’s Health 2019, 64, 713–724. [Google Scholar] [CrossRef]
- Joshi, S.S.; Badgwell, B.D. Current treatment and recent progress in gastric cancer. CA Cancer J. Clin. 2021, 71, 264–279. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, B.S.; Pawelke, J.; Bauer, J.; Burnet, N.G.; Dasu, A.; Høyer, M.; Lühr, A. Does the uncertainty in relative biological effectiveness affect patient treatment in proton therapy? Radiother. Oncol. 2021, 163, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Wang, G.; Huang, D.; Sui, M.; Xu, Y. Cancer immunotherapy based on natural killer cells: Current progress and new opportunities. Front. Immunol. 2019, 10, 1205. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Han, X.; Xiong, H.; Gao, Y.; Xu, B.; Zhu, G.; Li, J. Cancer Nanomedicine: Emerging Strategies and Therapeutic Potentials. Molecules 2023, 28, 5145. [Google Scholar] [CrossRef] [PubMed]
- Link, W. Principles of Cancer Treatment and Anticancer Drug Development; Springer International Publishing: Cham, Switzerland, 2019. [Google Scholar]
- Esfahani, K.; Roudaia, L.; Buhlaiga, N.A.; Del Rincon, S.V.; Papneja, N.; Miller, W.H. A review of cancer immunotherapy: From the past, to the present, to the future. Curr. Oncol. 2020, 27 (Suppl. 2), 87–97. [Google Scholar] [CrossRef]
- Dancey, J.; Sausville, E.A. Issues and progress with protein kinase inhibitors for cancer treatment. Nat. Rev. Drug Discov. 2003, 2, 296–313. [Google Scholar] [CrossRef]
- Shah, S.P.; Lonial, S.; Boise, L.H. When cancer fights back: Multiple myeloma, proteasome inhibition, and the heat-shock response. Mol. Cancer Res. 2015, 13, 1163–1173. [Google Scholar] [CrossRef]
- Steck, S.E.; Murphy, E.A. Dietary patterns and cancer risk. Nat. Rev. Cancer 2020, 20, 125–138. [Google Scholar] [CrossRef]
- Enitan, S.S.; Avwioro, G.; Adejumo, E.N. A review of complementary and alternative medicine used in cancer care: Challenges and prospects. TMR Integr. Med. 2023, 7, e23021. [Google Scholar] [CrossRef]
- Zia-Ul-Haq, M.; Marc, R.A.; Riaz, M. Natural products, medicinal foods and complementary and alternative medicine as cancer-preventive agents. Front. Pharmacol. 2023, 14, 1232249. [Google Scholar] [CrossRef]
- Balogh, L.C.; Matthews, T.W.; Schrag, C.; Elebro, K.A. Clinical outcomes of head and neck cancer patients who refuse curative therapy in pursuit of alternative medicine. Laryngoscope Investig. Otolaryngol. 2021, 6, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Castro-Espin, C.; Agudo, A. The role of diet in prognosis among cancer survivors: A systematic review and meta-analysis of dietary patterns and diet interventions. Nutrients 2022, 14, 348. [Google Scholar] [CrossRef] [PubMed]
- Tojjari, A.; Choucair, K.; Sadeghipour, A.; Saeed, A.; Saeed, A. Anti-Inflammatory and Immune Properties of Polyunsaturated Fatty Acids (PUFAs) and Their Impact on Colorectal Cancer (CRC) Prevention and Treatment. Cancers 2023, 15, 4294. [Google Scholar] [CrossRef] [PubMed]
- Morishima, T.; Sato, A.; Nakata, K.; Miyashiro, I. Geriatric assessment domains to predict overall survival in older cancer patients: An analysis of functional status, comorbidities, and nutritional status as prognostic factors. Cancer Med. 2020, 9, 5839–5850. [Google Scholar] [CrossRef]
- Reddy, L.; Odhav, B.; Bhoola, K.D. Natural products for cancer prevention: A global perspective. Pharmacol. Ther. 2003, 99, 1–13. [Google Scholar] [CrossRef]
- Huang, M.; Lu, J.J.; Ding, J. Natural products in cancer therapy: Past, present and future. Nat. Prod. Bioprospecting 2021, 11, 5–13. [Google Scholar] [CrossRef]
- Zhou, G.B.; Zhang, J.; Wang, Z.Y.; Chen, S.J.; Chen, Z. Treatment of acute promyelocytic leukaemia with all-trans retinoic acid and arsenic trioxide: A paradigm of synergistic molecular targeting therapy. Philos. Trans. R. Soc. B Biol. Sci. 2007, 362, 959–971. [Google Scholar] [CrossRef]
- Garcia-Oliveira, P.; Otero, P.; Pereira, A.G.; Chamorro, F.; Carpena, M.; Echave, J.; Prieto, M.A. Status and challenges of plant-anticancer compounds in cancer treatment. Pharmaceuticals 2021, 14, 157. [Google Scholar] [CrossRef]
- Shah, S.M.A.; Mehmood, Z.; Munir, N.; Jahangeer, M.; Qamar, S.A.; Fatema, G.; Sultana, S. Herbal treatment of viral cancer. Pak. J. Med. Biol. Sci. 2018, 2, 36–44. [Google Scholar]
- Jain, S.; Dwivedi, J.; Jain, P.K.; Satpathy, S.; Patra, A. Medicinal plants for treatment of cancer: A brief review. Pharmacogn. J. 2016, 8, 87–102. [Google Scholar] [CrossRef]
- Cragg, G.M.; Newman, D.J. Plants as a source of anti-cancer agents. J. Ethnopharmacol. 2005, 100, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Lichota, A.; Gwozdzinski, K. Anticancer activity of natural compounds from plant and marine environment. Int. J. Mol. Sci. 2018, 19, 3533. [Google Scholar] [CrossRef]
- Gezici, S.; Şekeroğlu, N. Current perspectives in the application of medicinal plants against cancer: Novel therapeutic agents. Anti-Cancer Agents Med. Chem. (Former. Curr. Med. Chem.-Anti-Cancer Agents) 2019, 19, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Mazumder, K.; Aktar, A.; Roy, P.; Biswas, B.; Hossain, M.E.; Sarkar, K.K.; Fukase, K. A review on mechanistic insight of plant derived anticancer bioactive Phytocompounds and their structure activity relationship. Molecules 2022, 27, 3036. [Google Scholar] [CrossRef] [PubMed]
- Elfer, K.N.; Sholl, A.B.; Wang, M.; Tulman, D.B.; Mandava, S.H.; Lee, B.R.; Brown, J.Q. DRAQ5 and eosin (‘D&E’) as an analog to hematoxylin and eosin for rapid fluorescence histology of fresh tissues. PLoS ONE 2016, 11, e0165530. [Google Scholar]
- Ali, K.; Ahmed, B.; Ansari, S.M.; Saquib, Q.; Al-Khedhairy, A.A.; Dwivedi, S.; Alshaeri, M.; Khan, M.S.; Musarrat, J. Comparative in situ ROS mediated killing of bacteria with bulk analogue, Eucalyptus leaf extract (ELE)-capped and bare surface copper oxide nanoparticles. Mater. Sci. Eng. C 2019, 100, 747–758. [Google Scholar] [CrossRef]
- Jardat, M.S.; Noonan, D.J.; Wu, B.; Avery, M.A.; Feller, D.R. Pseudolaric acid analogs as a new class of peroxisome proliferator-activated receptor agonists. Planta Medica 2002, 68, 667–671. [Google Scholar] [CrossRef]
- Carlisi, D.; Lauricella, M.; D’Anneo, A.; De Blasio, A.; Celesia, A.; Pratelli, G.; Emanuele, S. Parthenolide and its soluble analogues: Multitasking compounds with antitumor properties. Biomedicines 2022, 10, 514. [Google Scholar] [CrossRef]
- Demain, A.L.; Vaishnav, P. Natural products for cancer chemotherapy. Microb. Biotechnol. 2011, 4, 687–699. [Google Scholar] [CrossRef]
- Wali, A.F.; Majid, S.; Rasool, S.; Shehada, S.B.; Abdulkareem, S.K.; Firdous, A.; Beigh, S.; Shakeel, S.; Mushtaq, S.; Akbar, I.; et al. Natural products against cancer: Review on phytochemicals from marine sources in preventing cancer. Saudi Pharm. J. 2019, 27, 767–777. [Google Scholar] [CrossRef]
- Zuo, W.; Kwok, H.F. Development of marine-derived compounds for cancer therapy. Mar. Drugs 2021, 19, 342. [Google Scholar] [CrossRef] [PubMed]
- Thomas, T.R.A.; Kavlekar, D.P.; LokaBharathi, P.A. Marine drugs from sponge-microbe association—A review. Mar. Drugs 2010, 8, 1417–1468. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concentration (µg/mL) | [0; 1] | [1; 5] | [5; 10] | [10; 20] | [20; 100] | >100 |
|---|---|---|---|---|---|---|
| Code | 5 | 4 | 3 | 2 | 1 | 0 |
| Statistics | Males | Females | Both Sexes |
|---|---|---|---|
| New cancer cases (‰) | 0.29 | 0.48 | 0.77 |
| Age-standardized incidence rate (world) | 71.5 | 112.9 | 91.0 |
| Risk of developing cancer before the age of 75 years (%) | 7.9 | 11.7 | 9.7 |
| Cancer deaths (‰) | 0.22 | 0.32 | 0.54 |
| Age-standardized mortality rate (world) | 55.2 | 76.9 | 65.3 |
| Risk of dying from cancer before the age of 75 years (%) | 6.4 | 8.5 | 7.4 |
| 5-year prevalent cases (‰) | 0.48 | 0.87 | 1.35 |
| Top 5 most frequent cancers (*) | Prostate Colorectum Non-Hodgkin lymphoma Leukemia Liver | Breast Cervix uteri Ovary Colorectum Thyroid | Breast Cervix uteri Colorectum Non-Hodgkin lymphoma Leukemia |
| Prevention and Education | Promoting awareness about modifiable risk factors such as tobacco use, unhealthy diet, and sedentary lifestyles plays a pivotal role. Public health campaigns, education initiatives, and policies targeting lifestyle changes are essential. |
| Screening and Early Detection | Implementing efficient screening programs for high-risk populations aids in identifying cancer at its nascent stage. Regular screenings for breast, cervical, colorectal, and other cancers enable timely interventions, significantly improving survival rates. |
| Treatment Access and Quality Care | Ensuring equitable access to quality cancer treatment is imperative. A robust healthcare infrastructure, skilled medical professionals, and up-to-date treatment protocols are critical to enhancing patient outcomes. |
| Research and Innovation | Continuous research fosters advancements in cancer prevention, diagnosis, and treatment. Investment in research infrastructure and clinical trials fuels progress in oncology. |
| Policy of collaboration | Effective policies facilitate cancer control efforts. Collaborations with governments, organizations, and stakeholders can drive policy changes that support cancer prevention and care. |
| Diagnosis and Staging | Accurate diagnosis is paramount for designing personalized treatment plans. State-of-the-art diagnostic tools, including imaging techniques, biopsies, and molecular profiling, aid in precisely determining cancer type and stage. |
| Multidisciplinary Treatment | A multidisciplinary approach involving medical, surgical, and radiation oncologists, along with supportive care professionals, ensures a comprehensive treatment strategy tailored to the patient’s unique needs. |
| Precision Medicine | Molecular profiling guides treatment decisions by identifying genetic alterations driving cancer growth. Targeted therapies and immunotherapies maximize treatment efficacy while minimizing side effects. |
| Pain and Symptom Management | Palliative care focuses on alleviating pain and improving the quality of life for cancer patients. Comprehensive symptom management ensures comfort and enhances overall well-being. |
| Psychosocial Support | Cancer takes a toll on patients’ mental and emotional well-being. Access to counseling, support groups, and psychosocial services helps patients and their families cope with the challenges of diagnosis and treatment. |
| Medicinal Plant | Place of Collection | Major Composition |
|---|---|---|
| Cymbopogon schoenanthus (L.) Spreng. | Mouloud | 3-isopropenyl-5-methyl-1-cyclohexene (32.3%) D-limonene (11.3%) |
| Lavandula coronopifolia Poir. | Day | cis-caryophyllene (18.9%) Dehydronerolidol (12.8%) Isolongifolanone (11.2%) |
| Nepeta azurea R.Br | Day | Methyl (2E)-2-nonenoate (53.2%) |
| Ocimum americanum L. | Day | Carvotanacetol (38.4%) Estragole (27.5%) |
| Ocimum basilicum L. | Ambouli | Linalool (41.2%) Estragole (30.1%) |
| Ruta chalepensis subsp. fumariifolia | Day | 2-undecanone (51.3%) Octyl acetate (17.3%) |
| Tagetes minuta L. | Day | Dihydrotagetone (20.8%) Artemisia (17.9%) (Z)-Tagetenone (12.4%) (-)-Spathulenol (11%) |
| Cell Lines | Origin | Source |
|---|---|---|
| A2780 | Ovarian carcinoma | ECACC-93112517 |
| A549 | Lung carcinoma | ATCC®-CCL-185TM |
| HCT116 | Colorectal carcinoma | ATCC®-CCL-247TM |
| HEK-293 | Embryonic kidney | ATCC®-CRL-1573TM |
| JIMT-T1 | Breast carcinoma | DSMZ-ACC 589 |
| K562 | Myelogenous leukemia | ATCC®-CCL-243TM |
| MIA-Paca2 | Pancreas carcinoma | ATCC®-CRL-1420TM |
| MRC5 | Lung normal | ATCC®-CCL-171TM |
| NCI-N87 | Gastric carcinoma | ATCC®-CRL-5822TM |
| PC3 | Prostate carcinoma | ATCC®-CRL-1435TM |
| RT4 | Urinary bladder | ATCC®-HTB-2TM |
| U2OS | Bone osteosarcoma | ATCC®-HTB-96TM |
| U87-MG | Brain glioblastoma | ATCC®-HTB-14TM |
| Cell Line | C. schoenanthus | L. coronopifolia | N. azurea | O. americanum | O. basilicum | R. chalepensis | T. minuta | Combrestatin A4 | Doxorubicin | MMAE | Vinblastine |
|---|---|---|---|---|---|---|---|---|---|---|---|
| A2780 | 0.14 ± 0.03 | 0.21 ± 0.01 | 0.62 ± 0.09 | 0.69 ± 0.02 | 1.01 ± 0.11 | >100 | 0.36 ± 0.05 | - | - | 0.45 ± 0.01 | - |
| A549 | 0.49 ± 0.23 | 0.92 ± 0.14 | 0.07 ± 0.01 | 0.87 ± 0.06 | 5.37 ± 0.16 | 8.22 ± 0.73 | 1.57 ± 0.73 | 20.00 ± 0.10 | 56.60 ± 0.84 | 0.46 ± 0.05 | - |
| HCT116 | 0.65 ± 0.03 | 0.25 ± 0.03 | 0.11 ± 0.01 | 1.01 ± 0.01 | 1.77 ± 0.07 | >100 | 0.47 ± 0.04 | 2.00 ± 0.10 | - | 2.07 ± 0.02 | 35.00 ± 0.84 |
| HEK293 | 0.19 ± 0.05 | 0.12 ± 0.05 | 0.83 ± 0.11 | 0.25 ± 0.03 | 1.40 ± 0.11 | 1.39 ± 0.27 | 1.20 ± 0.32 | - | - | - | - |
| JIMT-T1 | 1.50 ± 0.30 | 0.71 ± 0.03 | 2.07 ± 0.20 | 0.92 ± 0.03 | 5.46 ± 0.051 | 6.66 ± 0.15 | 2.13 ± 0.38 | - | - | - | - |
| K562 | 0.99 ± 0.01 | 0.67 ± 0.15 | 1.00 ± 0.01 | 1.01 ± 0.01 | 3.67 ± 0.65 | 3.08 ± 0.59 | 1.06 ± 0.05 | 5.00 ± 0.30 | - | 3.12 ± 0.2 | 20.00 ± 0.12 |
| MIA-Paca2 | 0.55 ± 0.02 | 0.45 ± 0.06 | 0.86 ± 0.01 | 0.99 ± 0.03 | 5.31 ± 0.17 | 4.84 ± 0.04 | 1.61 ± 0.06 | - | - | 4.36 ± 0.2 | - |
| MRC-5 | 0.83 ± 0.09 | 0.12 ± 0.01 | 0.09 ± 0.01 | 1.34 ± 0.16 | 5.48 ± 0.182 | 7.85 ± 0.13 | 1.33 ± 0.14 | - | 39.88 ± 1.22 | - | - |
| NCI-N87 | 3.26 ± 1.52 | 4.22 ± 1.38 | 0.90 ± 0.27 | 4.28 ± 0.83 | 3.43 ± 0.12 | 2.31 ± 1.28 | 1.48 ± 0.10 | - | - | 1.65 ± 0.07 | - |
| PC3 | 0.29 ± 0.01 | 0.97 ± 0.07 | 0.80 ± 0.07 | 0.95 ± 0.02 | 4.37 ± 1.02 | 8.97 ± 0.17 | 1.71 ± 0.18 | 2.09 ± 0.03 | 0.36 ± 0.03 | - | |
| RT4 | 4.75 ± 1.24 | 1.57 ± 0.73 | 0.53 ± 0.01 | 0.86 ± 0.02 | 6.89 ± 1.52 | >100 | 1.37 ± 0.29 | - | 36.29 ± 1.20 | 0.50 ± 0.01 | - |
| U2OS | 0.24 ± 0.02 | 1.28 ± 0.14 | 0.67± 0.05 | 0.68 ± 0.05 | 4.29 ± 0.97 | 5.45 ± 0.76 | 1.16 ± 0.04 | - | - | - | - |
| U87-MG | 0.59 ± 0.09 | 0.34 ± 0.04 | 1.13 ± 0.22 | 1.31 ± 0.62 | 4.29 ± 0.65 | 6.03 ± 0.49 | 1.01 ± 0.12 | 9.00 ± 0.50 | 99.61 ± 2.34 | 0.21 ± 0.03 | 2.00 ± 0.04 |
| Cell Line | C. schoenanthus | L. coronopifolia | N. azurea | O. americanum | O. basilicum | R. chalepensis | T. minuta | Combrestatin A4 | Doxorubicin | MMAE | Vinblastine |
|---|---|---|---|---|---|---|---|---|---|---|---|
| A2780 | 5 | 5 | 5 | 5 | 4 | 0 | 5 | 0 | 0 | 5 | 0 |
| A549 | 5 | 5 | 5 | 5 | 3 | 3 | 4 | 1 | 1 | 5 | 0 |
| HCT116 | 5 | 5 | 5 | 4 | 4 | 0 | 5 | 4 | 0 | 4 | 1 |
| HEK293 | 5 | 5 | 5 | 5 | 4 | 4 | 4 | 0 | 0 | 0 | 0 |
| JIMT-T1 | 4 | 5 | 4 | 5 | 3 | 3 | 4 | 0 | 0 | 0 | 0 |
| K562 | 5 | 5 | 4 | 4 | 4 | 4 | 4 | 4 | 0 | 4 | 1 |
| MIA-Paca2 | 5 | 5 | 5 | 5 | 3 | 4 | 4 | 0 | 0 | 4 | 0 |
| MRC-5 | 5 | 5 | 5 | 4 | 4 | 3 | 4 | 0 | 1 | 0 | 0 |
| NCI-N87 | 4 | 4 | 5 | 4 | 3 | 4 | 4 | 0 | 0 | 4 | 0 |
| PC3 | 5 | 5 | 5 | 5 | 4 | 3 | 4 | 0 | 4 | 5 | 0 |
| RT4 | 4 | 4 | 5 | 5 | 3 | 0 | 4 | 0 | 1 | 5 | 0 |
| U2OS | 5 | 4 | 5 | 5 | 4 | 3 | 4 | 0 | 0 | 0 | 0 |
| U87-MG | 5 | 5 | 4 | 4 | 4 | 3 | 4 | 3 | 1 | 5 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdoul-Latif, F.M.; Ainane, A.; Houmed Aboubaker, I.; Mohamed, J.; Ainane, T. An Overview of Cancer in Djibouti: Current Status, Therapeutic Approaches, and Promising Endeavors in Local Essential Oil Treatment. Pharmaceuticals 2023, 16, 1617. https://doi.org/10.3390/ph16111617
Abdoul-Latif FM, Ainane A, Houmed Aboubaker I, Mohamed J, Ainane T. An Overview of Cancer in Djibouti: Current Status, Therapeutic Approaches, and Promising Endeavors in Local Essential Oil Treatment. Pharmaceuticals. 2023; 16(11):1617. https://doi.org/10.3390/ph16111617
Chicago/Turabian StyleAbdoul-Latif, Fatouma Mohamed, Ayoub Ainane, Ibrahim Houmed Aboubaker, Jalludin Mohamed, and Tarik Ainane. 2023. "An Overview of Cancer in Djibouti: Current Status, Therapeutic Approaches, and Promising Endeavors in Local Essential Oil Treatment" Pharmaceuticals 16, no. 11: 1617. https://doi.org/10.3390/ph16111617
APA StyleAbdoul-Latif, F. M., Ainane, A., Houmed Aboubaker, I., Mohamed, J., & Ainane, T. (2023). An Overview of Cancer in Djibouti: Current Status, Therapeutic Approaches, and Promising Endeavors in Local Essential Oil Treatment. Pharmaceuticals, 16(11), 1617. https://doi.org/10.3390/ph16111617