

The Role of Pharmaceutical Compounding in Promoting Medication Adherence


Abstract
:1. Introduction
2. Pharmaceutical Compounding and Regulatory Framework
2.1. Compounding Regulatory Framework in the European Union
- i.
- magistral formula: any medicinal product prepared in a pharmacy in accordance with a prescription for an individual patient;
- ii.
- official formula: any medicinal product which is prepared in a pharmacy in accordance with the prescriptions of a pharmacopoeia and is intended to be supplied directly to the patients served by the pharmacy in question.
- i.
- extemporaneous preparations, i.e., pharmaceutical preparations individually prepared for a specific patient or patient group, supplied after preparation;
- ii.
- stock preparations, i.e., pharmaceutical preparations prepared in advance and stored until a request for a supply is received.
2.2. Compounding Regulatory Framework in the United States
- i.
- Pharmacies (section 503A): State-licensed pharmacies that traditionally prepare compounded medicines for a specific patient prescription and that are overseen by the State Boards of Pharmacy.
- ii.
- Outsourcing facilities (section 503B): a new type of designation for those compounding facilities that stand in between the traditional compounding pharmacies and the large pharmaceutical manufacturers. These facilities are not required to be licensed pharmacies but must be supervised by a pharmacist or physician. Importantly, all 503Bs must comply with the current good manufacturing practices (cGMP) and undergo regular FDA inspections on a risk-based schedule. In addition, all products compounded, which may or may not be patient-specific, must be reported to the FDA every 6 months [19]. As of 15th February 2021, there were 69 facilities registered as human drug compounding outsourcing facilities in the USA [21].
3. Compounding Formulations Addressing Patient Needs and Preferences
3.1. Special Patient Populations
3.1.1. Pediatric Patients
Age-Appropriate Dosage Strengths
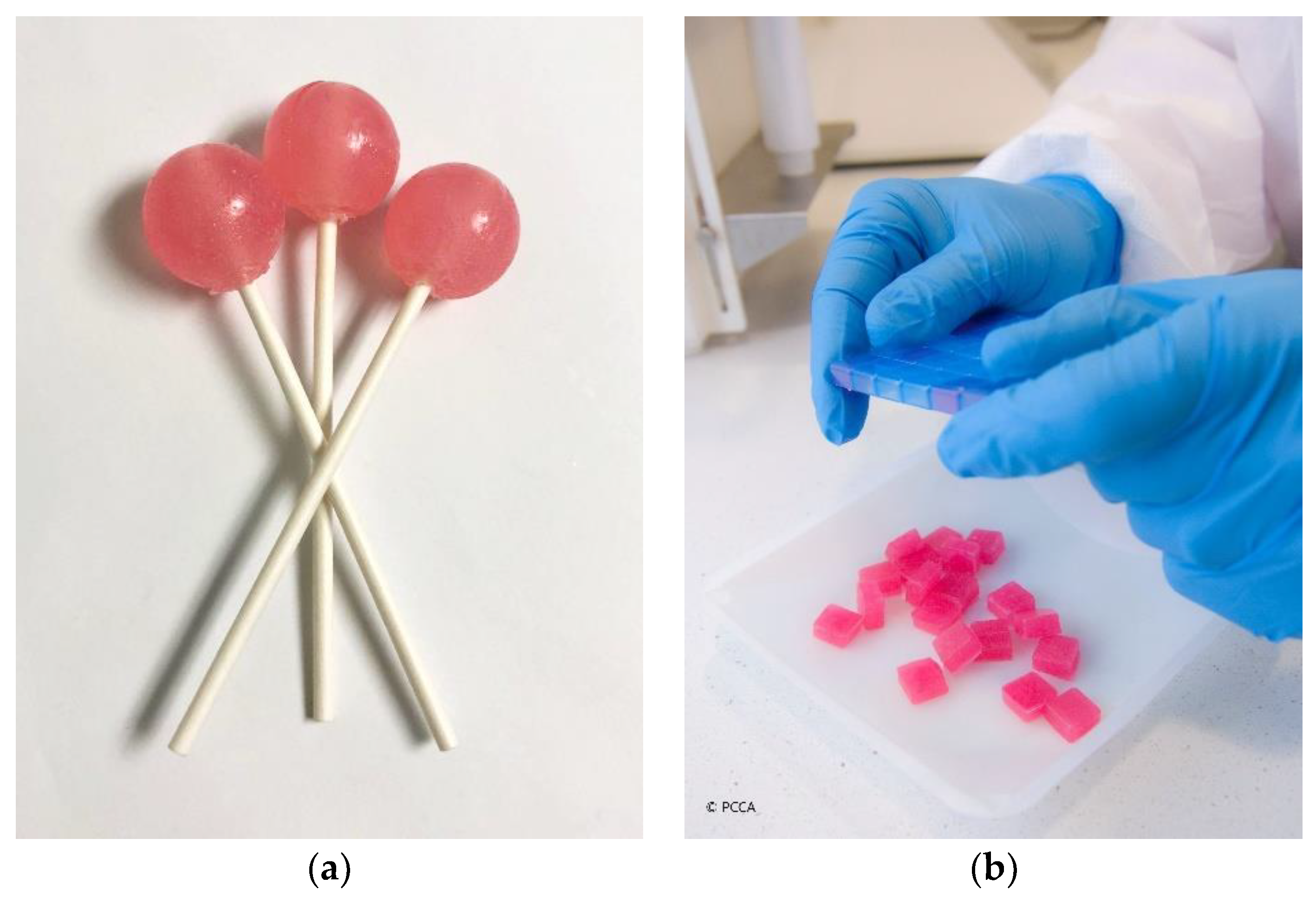
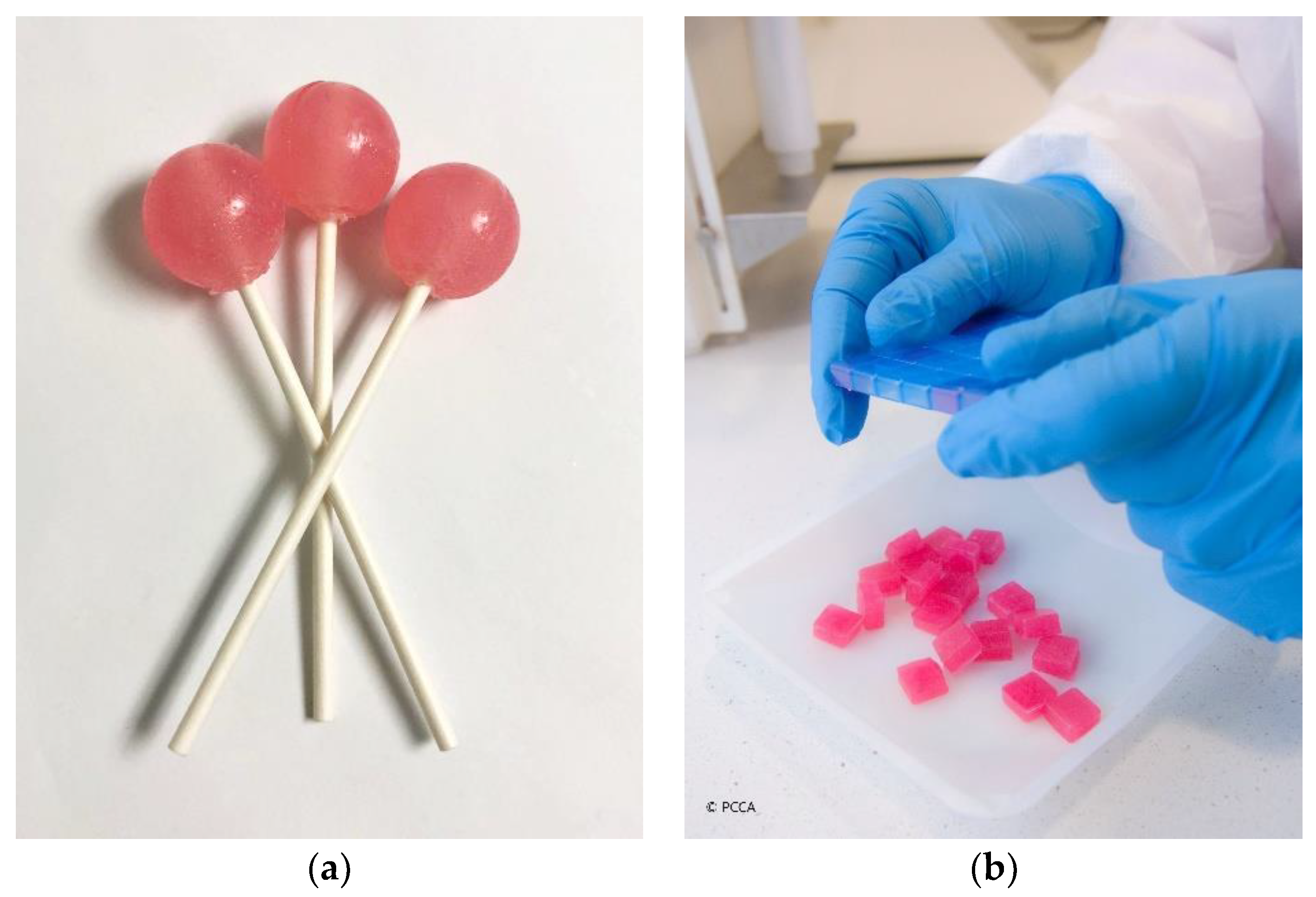
Child-Friendly Dosage Forms
Flavoring and Sweetening
3.1.2. Geriatric Patients
Polypharmacy
Dysphagia
Packaging
3.2. Patient-Specific Needs
3.2.1. Allergies and Intolerances
3.2.2. Orphan Medicines
3.3. Other Specific needs
3.3.1. Medicines Shortages
3.3.2. Discontinued Medicines
3.3.3. Economic Considerations
4. The Impact of Compounding on Medication Adherence
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vrijens, B.; De Geest, S.; Hughes, D.A.; Przemyslaw, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; et al. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 2012, 73, 691–705. [Google Scholar] [CrossRef]
- Khan, R.; Socha-Dietrich, K. Investing in Medication Adherence Improves Health Outcomes and Health System Efficiency: Adherence to Medicines for Diabetes, Hypertension, and Hyperlipidaemia; OECD Health Working Papers; 2018; Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/investing-inmedication-adherence-improves-health-outcomes-and-health-systemefficiency_8178962c-en (accessed on 16 April 2021).
- WHO. Adherence to Long-Term Therapies: Evidence for Action; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Menditto, E.; Cahir, C.; Aza-Pascual-Salcedo, M.; Bruzzese, D.; Poblador-Plou, B.; Malo, S.; Costa, E.; Rubio, F.G.; Gimeno-Miguel, A.; Orlando, V.; et al. Adherence to chronic medication in older populations: Application of a common protocol among three European cohorts. Patient Prefer. Adherence 2018, 12, 1975–1987. [Google Scholar] [CrossRef]
- Teixeira, A.; Teixeira, M.; Almeida, V.; Gaio, R.; Torres, T.; Magina, S.; Cunha, C.; Lobo, J.M.S.; Almeida, I.F. Does the Vehicle Matter? Real-World Evidence on Adherence to Topical Treatment in Psoriasis. Pharmaceutics 2021, 13, 1539. [Google Scholar] [CrossRef] [PubMed]
- Menditto, E.; Orlando, V.; De Rosa, G.; Minghetti, P.; Musazzi, U.M.; Cahir, C.; Kurczewska-Michalak, M.; Kardas, P.; Costa, E.; Lobo, J.M.S.; et al. Patient Centric Pharmaceutical Drug Product Design—The Impact on Medication Adherence. Pharmaceutics 2020, 12, 44. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Ghaffur, A.; Bains, J.; Hamdy, S. Acceptability of oral solid medicines in older adults with and without dysphagia: A nested pilot validation questionnaire based observational study. Int. J. Pharm. 2016, 512, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Itter, I.; Treuer, T.; Dilbaz, N.; Oyffe, I.; Ciorabai, E.M.; Gonzalez, S.L.; Ruschel, S.; Salburg, J.; Dyachkova, Y. Patients’ preference for olanzapine orodispersible tablet compared with conventional oral tablet in a multinational, randomized, crossover study. World J. Boil. Psychiatry 2010, 11, 894–903. [Google Scholar]
- Eastman, W.J.; Malahias, S.; Delconte, J.; Di Benedetti, D. Assessing attributes of topical vehicles for the treatment of acne, atopic dermatitis, and plaque psoriasis. Cutis 2014, 94, 46–53. [Google Scholar]
- Draelos, Z.; Blair, A.; Tanghetti, E. Vehicle Formulation Impacts Tolerability and Patient Preference: Comparison of Tretinoin Branded Lotion and Generic Cream. Ski. J. Cutan. Med. 2022, 6, s44. [Google Scholar] [CrossRef]
- De Carvalho, M.J.R. Extemporaneously Compounded Oral Medicines in European Hospital Pharmacies. Ph.D. Thesis, (UCL) University College London, London, UK, 2013. [Google Scholar]
- Allen, L.V. The Art, Science, and Technology of Pharmaceutical Compounding, 6th ed.; APhA: Washington, DC, USA, 2020. [Google Scholar]
- Cabaleiro, J. New England Compounding Center Indictment. Int. J. Pharm. Compd. 2015, 19, 94–102. [Google Scholar]
- Watson, C.J.; Whitledge, J.D.; Siani, A.M.; Burns, M.M. Pharmaceutical Compounding: A History, Regulatory Overview, and Systematic Review of Compounding Errors. J. Med. Toxicol. 2020, 17, 197–217. [Google Scholar] [CrossRef]
- Council of Europe. Pharmaceutical Preparations. In European Pharmacopoeia, 7th ed.; Council of Europe: Strasbourg, 2013. [Google Scholar]
- Council of Europe. Pharmaceutical Preparations. In European Pharmacopoeia, 10th ed.; Council of Europe: Strasbourg, 2019. [Google Scholar]
- CompoundingToday. Editorial: What is Compounding Pharmacy, Part IV. 2014. Available online: https://compoundingtoday.com/Newsletter/Newsletter11_21.cfm (accessed on 15 February 2021).
- United States Pharmacopeial Convention. USP General Chapter <795> Pharmaceutical Compounding-Nonsterile Preparations. In USP 43-NF 38 as of June 1, 2020; United States Pharmacopeial Convention: Rockville, MD, USA, 2020. [Google Scholar]
- Gabay, M. The Drug Quality and Security Act. Hosp. Pharm. 2014, 49, 615–676. [Google Scholar] [CrossRef] [PubMed]
- Public Law 113-54, 113th Congress, H.R. 3204: Drug Quality and Security Act. 2013. Available online: https://www.congress.gov/113/plaws/publ54/PLAW-113publ54.pdf (accessed on 20 February 2021).
- FDA. Registered Outsourcing Facilities. 2021. Available online: https://www.fda.gov/drugs/human-drug-compounding/registered-outsourcing-facilities (accessed on 15 February 2021).
- United States Pharmacopeial Convention. Compounding Compendium. In Current with USP 43-NF 38 through Second Supplement; United States Pharmacopeial Convention: Rockville, MD, USA, 2020. [Google Scholar]
- United States Pharmacopeial Convention. USP General Chapter <797> Pharmaceutical Compounding-Sterile Preparations. In USP 43-NF 38 as of June 1, 2020; United States Pharmacopeial Convention: Rockville, MD, USA, 2020. [Google Scholar]
- United States Pharmacopeial Convention. USP General Chapter <800> Hazardous Drugs-Handling in Healthcare Settings. In USP 43-NF 38 as of June 1, 2020; United States Pharmacopeial Convention: Rockville, MD, USA, 2020. [Google Scholar]
- El-Rachidi, S.; Larochelle, J.M.; Morgan, J.A. Pharmacists and Pediatric Medication Adherence: Bridging the Gap. Hosp. Pharm. 2017, 52, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Paediatric Formulary Committee. BNF for Children 2020–2021 (Online); BMJ Group, Pharmaceutical Press, and RCPCH Publications: London, UK; Available online: https://ebookcentral.proquest.com/ (accessed on 18 March 2022).
- Juárez-Hernández, J.E.; Carleton, B.C. Paediatric oral formulations: Why don’t our kids have the medicines they need? Br. J. Clin. Pharmacol. 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hejaz, H.A.; Kanan, A.; Al Mohtaseb, M.; Ja’Bari, A. Development and characterization of paracetamol medicated lollipops. Pharm. Technol. Hosp. Pharm. 2020, 5, 20200012. [Google Scholar] [CrossRef]
- Allen, L.V. Tetracycline Compound Troche. Int. J. Pharm. Compd. 1997, 1, 113. [Google Scholar]
- Muller, G.; Case, T.; Deen, G.L. Tetracaine lollipops for the suppression of extreme gag reflex in dental patients. Int. J. Pharm. Compd. 2013, 14, 395. [Google Scholar]
- Davies, E.H.; Tuleu, C. Medicines for Children: A Matter of Taste. J. Pediatrics 2008, 153, 599–604. [Google Scholar] [CrossRef]
- FLAVORx Pediatric System. Available online: https://www.flavorx.com/flavorx-pediatric-system/ (accessed on 16 February 2021).
- Amos, S.R.; Baker, C.; Gueye, Y. Improving the Palatability of Medications to Help Children be more Compliant. In Proceedings of the 3rd European Paediatric Formulation Initiative (EuPFI) Conference: Formulating Better Medicines for Children, Poster Presentation, Strasbourg, France, 20–21 September 2011. [Google Scholar]
- McElhiney, L. Compounding Challenges for Immunocompromised Patients. Int. J. Pharm. Compd. 2008, 12, 482–487. [Google Scholar] [PubMed]
- Bucher, C.V.; Day, A.J.; Carvalho, M. The Role of Transdermal Compounding in Opioid Safety. J. Opioid Manag. 2018, 14, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Bassani, A.S.; Banov, D. Evaluation of the Percutaneous Absorption of Ketamine HCl, Gabapentin, Clonidine HCl, and Baclofen, in Compounded Transdermal Pain Formulations, Using the Franz Finite Dose Model. Pain Med. 2015, 17, 230–238. [Google Scholar] [CrossRef]
- Adkins, C.; Takakura, W.; Spiegel, B.M.; Lu, M.; Vera-Llonch, M.; Williams, J.; Almario, C.V. Prevalence and Characteristics of Dysphagia Based on a Population-Based Survey. Clin. Gastroenterol. Hepatol. 2019, 18, 1970–1979.e2. [Google Scholar] [CrossRef]
- Bramwell, B.L. Compliance to treatment in elderly dysphagic patients: Potential benefits of alternative dosage forms. Int. J. Pharm. Compd. 2013, 11, 498–505. [Google Scholar]
- Beckman, A.; Bernsten, C.; Parker, M.G.; Thorslund, M.; Fastbom, J. The Difficulty of Opening Medicine Containers in Old Age: A Population-Based Study. Pharm. Weekbl. Sci. Ed. 2005, 27, 393–398. [Google Scholar] [CrossRef] [PubMed]
- CSS Health. Medicine-On-Time. 2021. Available online: https://medicineontime.com/ (accessed on 17 February 2021).
- Pellagatti, T.; Ternelli, M.; Frascio, D.; Bettini, R. Warfarin Personalized Dosage: Re-compounding for a More Suitable Therapy and Better Compliance. Int. J. Pharm. Compd. 2017, 21, 247–250. [Google Scholar]
- Lonza. Coni-Snap® Sprinkle Capsules. 2021. Available online: https://www.capsugel.com/consumer-health-nutrition-products/coni-snap-sprinkle-capsules (accessed on 16 February 2021).
- Nagel-Edwards, K.M.; Ko, J.Y. Excipient choices for special populations. Int. J. Pharm. Compd. 2013, 12, 426–430. [Google Scholar]
- Hendrickx, K.; Dooms, M. Orphan Drugs, Compounded Medication and Pharmaceutical Commons. Front. Pharmacol. 2021, 12, 738458. [Google Scholar] [CrossRef]
- Dooms, M.; Carvalho, M. Compounded medication for patients with rare diseases. Orphanet J. Rare Dis. 2018, 13, 1. [Google Scholar] [CrossRef]
- Vanhoorne, V.; Peeters, E.; Van Tongelen, I.; Boussery, K.; Wynendaele, E.; De Spiegeleer, B.; Vervaet, C. Pharmaceutical compounding of orphan active ingredients in Belgium: How community and hospital pharmacists can address the needs of patients with rare diseases. Orphanet J. Rare Dis. 2019, 14, 186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendel, A.; Bernatsky, S.; Thorne, J.C.; Lacaille, D.; Johnson, S.R.; Vinet, E. Hydroxychloroquine shortages during the COVID-19 pandemic. Ann. Rheum. Dis. 2021, 80, e31. [Google Scholar] [CrossRef]
- FDA. Current and Resolved Drug Shortages and Discontinuations Reported to FDA. 2021. Available online: https://www.accessdata.fda.gov/scripts/drugshortages/ (accessed on 19 February 2021).
- Morgan, S.G.; Bathula, H.S.; Moon, S. Pricing of pharmaceuticals is becoming a major challenge for health systems. BMJ 2020, 368, l4627. [Google Scholar] [CrossRef]
- Allen, L.V. Hydroxychloroquine Sulfate 25 mg/mL in Ora-Plus and Ora-Sweet SF. U.S. Pharm. 2020, 45, 60-CV3. [Google Scholar]
- Song, G.; Banov, D.; Bassani, A.S. Effects of Compounded Stanford Modified Oral Rinse (MucoLox) on the Survival and Migration of Oral Keratinocytes and Fibroblasts: Implications for Wound Healing. Int. J. Pharm. Compd. 2018, 22, 60–65. [Google Scholar] [PubMed]
- Ip, K.; Carvalho, M.; Shan, A.; Banov, D. Physical and Chemical Stability of Budesonide Mucoadhesive Oral Suspensions (MucoLox). Int. J. Pharm. Compd. 2017, 21, 322–329. [Google Scholar] [PubMed]
- Allen, L.V. Ursodiol 150 mg Capsules. Int. J. Pharm. Compd. 2003, 7, 382. [Google Scholar]
- Pramar, Y.V.; Mandal, T.K.; Bostanian, L.A.; Nguyen, A.T.Q.; Miller, V.; Morris, T.C.; Graves, R.A. Stability of Compounded Ursodiol Suspensions in PCCA Base, SuspendIt. Int. J. Pharm. Compd. 2019, 23, 70–76. [Google Scholar] [PubMed]
- Loh, A.; Leonhart, R.; Wills, C.E.; Simon, D.; Härter, M. The impact of patient participation on adherence and clinical outcome in primary care of depression. Patient Educ. Couns. 2007, 65, 69–78. [Google Scholar] [CrossRef] [PubMed]
- McPherson, T.; Fontane, P.; Iyengar, R.; Henderson, R. Utilization and Costs of Compounded Medications for Commercially Insured Patients, 2012–2013. J. Manag. Care Spéc. Pharm. 2016, 22, 172–181. [Google Scholar] [CrossRef]
- Reed-Kane, D.; Vasquez, K.; Pavlik, A.; Peragine, J.; Sandberg, M. E-prescription errors and their resolution in a community compounding pharmacy. Int. J. Pharm. Compd. 2014, 18, 159–161. [Google Scholar]
- Kristina, S.A.; Wiedyaningsih, C.; Widyakusuma, N.N.; Aditama, H. Extemporaneous compounding practice by pharmacists: A systematic review. Int. J. Pharm. Pharm. Sci. 2017, 9, 42. [Google Scholar] [CrossRef]
- McPherson, T.B.; Fontane, P.E.; Jackson, K.D.; Berry, T.; Chereson, R.; Bilger, R.; Martin, K.S. Prevalence of Compounding in Independent Community Pharmacy Practice. J. Am. Pharm. Assoc. 2006, 46, 568–573. [Google Scholar] [CrossRef]
- National Community Pharmacy Association. Community Pharmacy-Compounding Survey; National Community Pharmacist Association: Alexandria, VA, USA, 2012. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Compounded Medicines | Formulas |
|---|---|
| Hydroxychloroquine sulfate 25 mg/mL oral suspension (adapted from [50]) | Hydroxychloroquine sulfate.............................. 2.5 g Vehicle: Ora-Plus® and Ora-Sweet® SF (1:1) to 100 mL |
| Stanford modified oral rinse (adapted from [51]) | Diphenhydramine hydrochloride........................ 0.0625 g Lidocaine hydrochloride monohydrate............ 0.533 g Nystatin (2,500,000 units)................................... 0.407 g Magnesium hydroxide..................................... 1 g Aluminum hydroxide gel .................................... 1 g Steviol glycosides 95%............................................. 0.1 g Acesulfame potassium FCC............................ 0.1 g Simethicone ............................................... 0.1 g Flavor, Crème DeMenthe ............................ 0.2 mL Purified water............................................ 15 mL Base, PCCA Mucolox™ .......................... to 100 mL |
| Transdermal pain medication (adapted from [36]) | Ketamine hydrochloride.................................. 5 g Gabapentin.................................................. 10 g Clonidine hydrochloride............................... 0.2 g Baclofen....................................................... 2 g Ethoxy diglycol............................................. 10 g Base, PCCA Lipoderm®............................. to 100 g |
| Budesonide 1 mg/10 mL oral suspension (adapted from [52]) | Budesonide................................................ 0.01 g Steviol glycosides 95%............................................. 0.2 g Parabens preserved water............................ 20 mL Base, PCCA Mucolox™ ............................ to 100 mL |
| Ursodiol 150 mg capsules (adapted from [53]) | Ursodiol...................................................... 15 g Starch..........................................................to 100 capsules |
| Ursodiol 50 mg/mL oral suspension (adapted from [54]) | Ursodiol....................................................... 25 g Acesulfame potassium .................................. 2.5 g Steviol glycosides 95%.............................................. 2.5 g Base, PCCA Suspendit®........................... to 500 mL |
| Anti-gag lollipops (adapted from [12]) | Sodium chloride......................................... 46.56 g Potassium chloride......................................... 3 g Calcium lactate............................................. 6.12 g Magnesium citrate........................................ 2.04 g Sodium bicarbonate..................................... 22.44 g Sodium phosphate monobasic........................... 3.84 g Silica gel...................................................... 3.60 g Polyethylene glycol 1450.....................qs 36 lollipops |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carvalho, M.; Almeida, I.F. The Role of Pharmaceutical Compounding in Promoting Medication Adherence. Pharmaceuticals 2022, 15, 1091. https://doi.org/10.3390/ph15091091
Carvalho M, Almeida IF. The Role of Pharmaceutical Compounding in Promoting Medication Adherence. Pharmaceuticals. 2022; 15(9):1091. https://doi.org/10.3390/ph15091091
Chicago/Turabian StyleCarvalho, Maria, and Isabel F. Almeida. 2022. "The Role of Pharmaceutical Compounding in Promoting Medication Adherence" Pharmaceuticals 15, no. 9: 1091. https://doi.org/10.3390/ph15091091
APA StyleCarvalho, M., & Almeida, I. F. (2022). The Role of Pharmaceutical Compounding in Promoting Medication Adherence. Pharmaceuticals, 15(9), 1091. https://doi.org/10.3390/ph15091091