
Accuracy Report on a Handheld 3D Ultrasound Scanner Prototype Based on a Standard Ultrasound Machine and a Spatial Pose Reading Sensor

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measuring and Verifying the CAD/CAM Manufactured Object, the Mouth Guard, Using a Method with Known and Determined Measurement Error (Intraoral Optical Scanning Method)
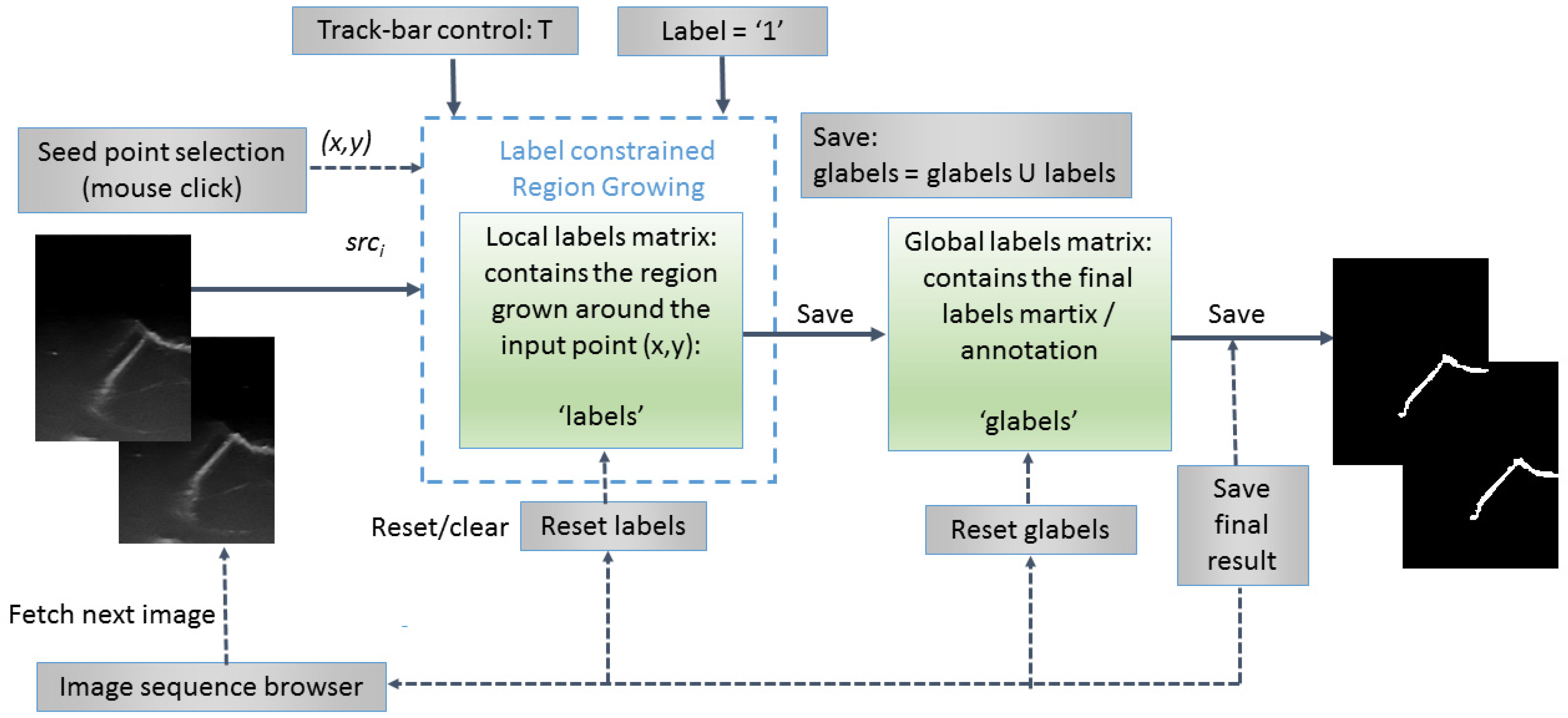
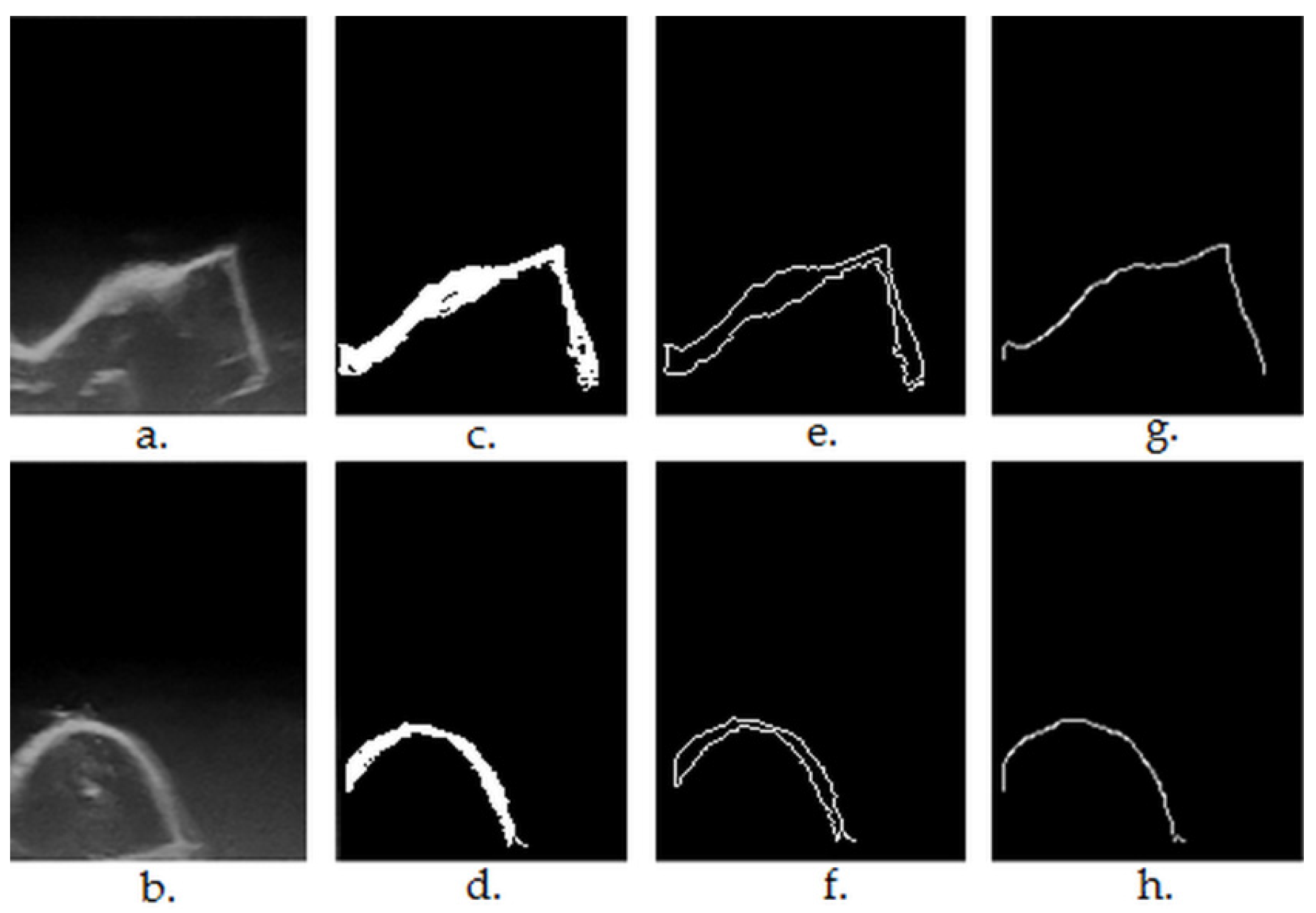
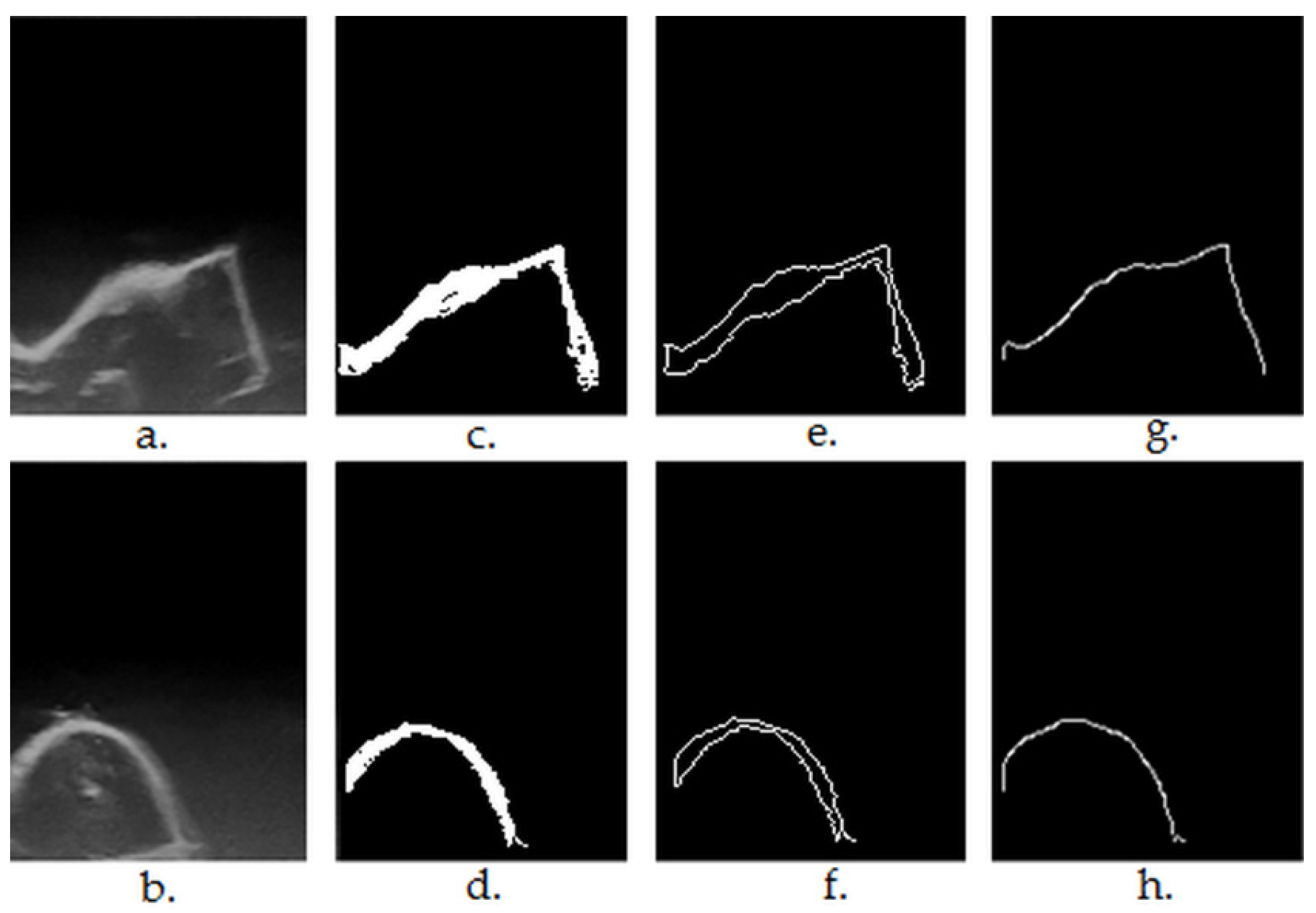
2.2. Semiautomatic Segmentation of the 2D Ultrasound Images
| Algorithm 1 Label Constrained Region Growing | ||
| 1: 2: 3: 4: 5: 6: 7: 8: 9: 10: 11: 12: 13: 14: 15: 16: 17: 18: 19: 20: 21: 22: 23: 24: 25: 26: 27: 28: 29: 30: 31: 32: 33: 34: | procedure Grow(src; local_labels; label = 1; x; y; T; applyMorph) h ← src height w ← src width Q ← [ ] W ← 3 d ← W/2 avgColor ← average(src(y − d: y + d; x − d: x + d)) d ← 1 N ← 1 Q:append((y,x)) if labels(y,x) = 0 then labels(y,x) = label end if while Q is not empty do oldest ← Q.pop() for m ← −d to d, n ← −d to d do i ← oldest.y + m j ← oldest.x + n if (i,j) inside of src then color ← src(i,j) if |color – avgColor| < T and labels(i,j) = 0 and glabels(i,j) = 0 then labels(i,j) ← label Q.append(i,j)) avgColor ← (avgColor × N +color)/(N + 1) N ← N + 1 end if end if end for end while dst ← labels if applyMorpho = true then dst ← Dilate(dst,R,label) dst ← Erode(dst,R,label) end if return dst end procedure | > Empty queue > Averaging window size > No. of pixels in the region > If pixel is unlabeled > Take out the oldest element from the queue > Search across its neighbors and add them to the queue if they are not labeled and are similar in terms of color with the region > Update the average color of the region > Convert the local labels matrix into the destination image > Post-process the result by morphological operations |
2.3. Morphological Post-Processing
| Algorithm 2 Label Constrained Dilation | ||
| 1: 2: 3: 4: 5: 6: 7: 8: 9: 10: 11: 12: 13: 14: 15: 16: 17: 18: 19: 20: 21: | procedure Dilate(src, R, label = 1) dst ← copy(src) h ← img height w ← img width for i ← R to h − R − 1, j ← R to w − R − 1 do if src(i,j) = label then for m ← −R to R, n ← −R to R do if R > 2 then radius ← if radius < R and src(i + m, j + n) = 0 then dst(i + m,j + n) ← label end if else if src(i + m; j + n) = 0 then dst(i + m; j + n) ← label end if end if end for end if end for return dst end procedure | > Clone source image into the destination > Image scan with safety border > Apply dilation using a circular structuring element of radius R (R > 2) only on pixels with the specified label. All pixels in the neighborhood masked by the structuring element are marked with the current label > If R ≤ 2, the structuring element has a square shape |
| Algorithm 3 Label Constrained Erosion | ||
| 1: 2: 3: 4: 5: 6: 7: 8: 9: 10: 11: 12: 13: 14: 15: 16: 17: 18: 19: 20: 21: 22: 22: 22: | procedure Erode(src, R, label = 1) dst ← copy(src) h ← img height w ← img width for i ← R to h − R − 1, j ← R to w − R − 1 do frontier ← false if src(i,j) = label then for m ← −R to R, n ← −R to R do if R > 2 then radius ← if radius < R and src(i + m, j + n) = 0 then frontier ← true end if else if src(i + m; j + n) = 0 then frontier ← true end if end if end for end if if frontier ← true then dst(i,j) ← 0 end for return dst end procedure | > Clone source image into the destination > Image scan with safety border > Apply erosion using a circular structuring element of radius R (R > 2) only on pixels with the specified label. If there is a background pixel in the neighborhood masked by the structuring element, a flag (frontier) is set > If R ≤ 2, the structuring element has a square shape > If a flag is set, the current pixel is removed from the result |
2.4. Upper Envelop/Contour Extraction of the Segmented Objects
| Algorithm 4 Find Upper Envelope | ||
| 1: 2: 3: 4: 5: 6: 7: 8: 9: 10: 11: 12: 13: 14: 15: 16: | procedure FindEnvelope(src) contours ← findExternalContours(src) h ← img height w ← img width dst ← (h,w,0) for j ← 0 to w − 1 do while contours(i,j) = 0 and i < h − 1 do i ← I + 1 end while while contours(i,j) = 255 and i < h − 1 do dst(i,j) ← 255 i ← I + 1 break end while end for return dst end procedure | > Detect external contours in the binary source image and store them (as white pixels) in the contours image > Create a black destination image > Scan the binary contour image contours on columns > Skip the first vertical sequence of black pixels > Store the first vertical sequence of white (object/contour) pixels in the destination image dst > At the end of the sequence, break the for loop (j ← j + 1, i ←0) |
2.5. Generating 3D Ultrasound Reconstructions
2.6. Evaluating the Accuracy of the 3D Ultrasound Reconstructions
3. Results
3.1. Measuring and Verifying the CAD/CAM Manufactured Object, the Mouth Guard, Using a Method with Known and Determined Measurement Error (Intraoral Optical Scanning Method)
3.2. Preparing the 2D Ultrasonographic Images, Performing 3D Ultrasound Reconstructions and Aligning Them with the Reference Object for Statistical Analysis
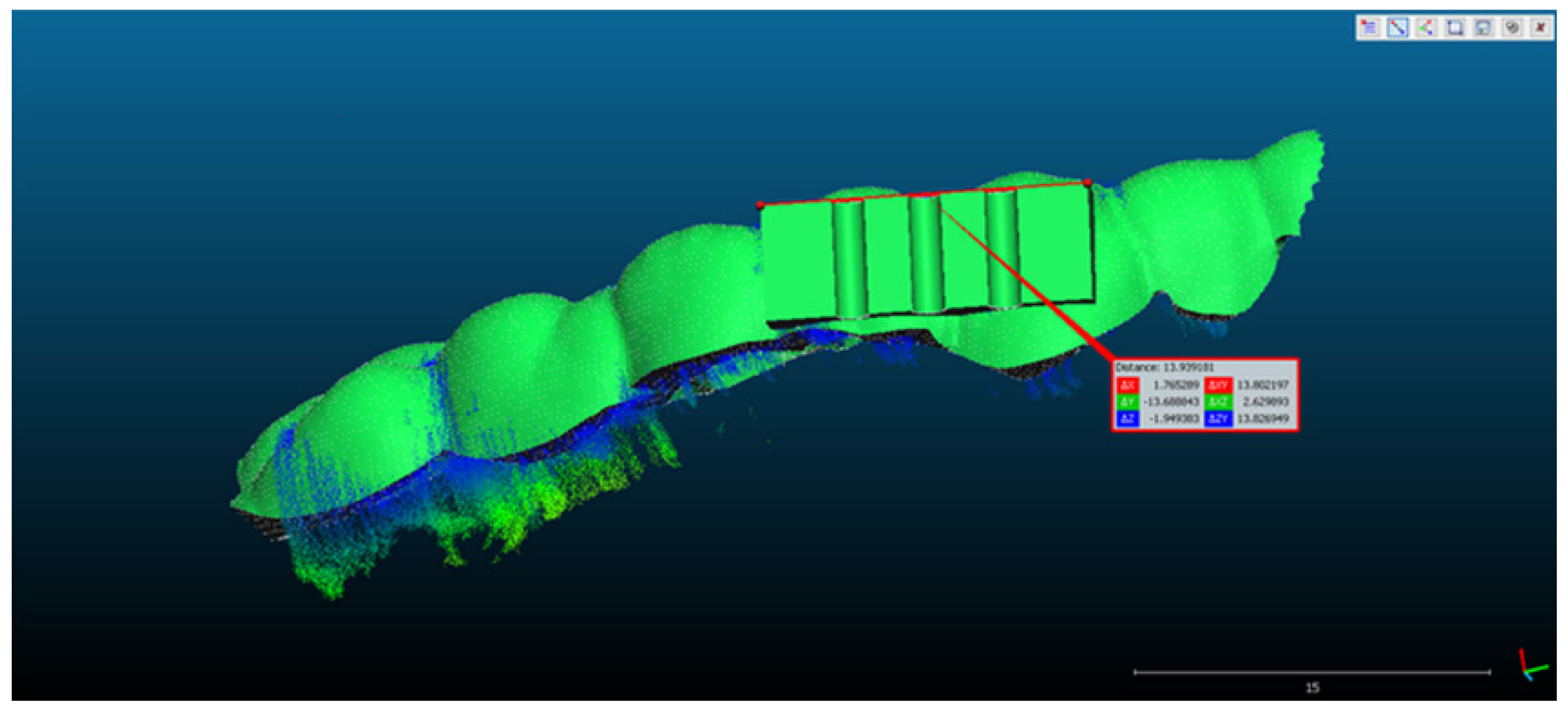
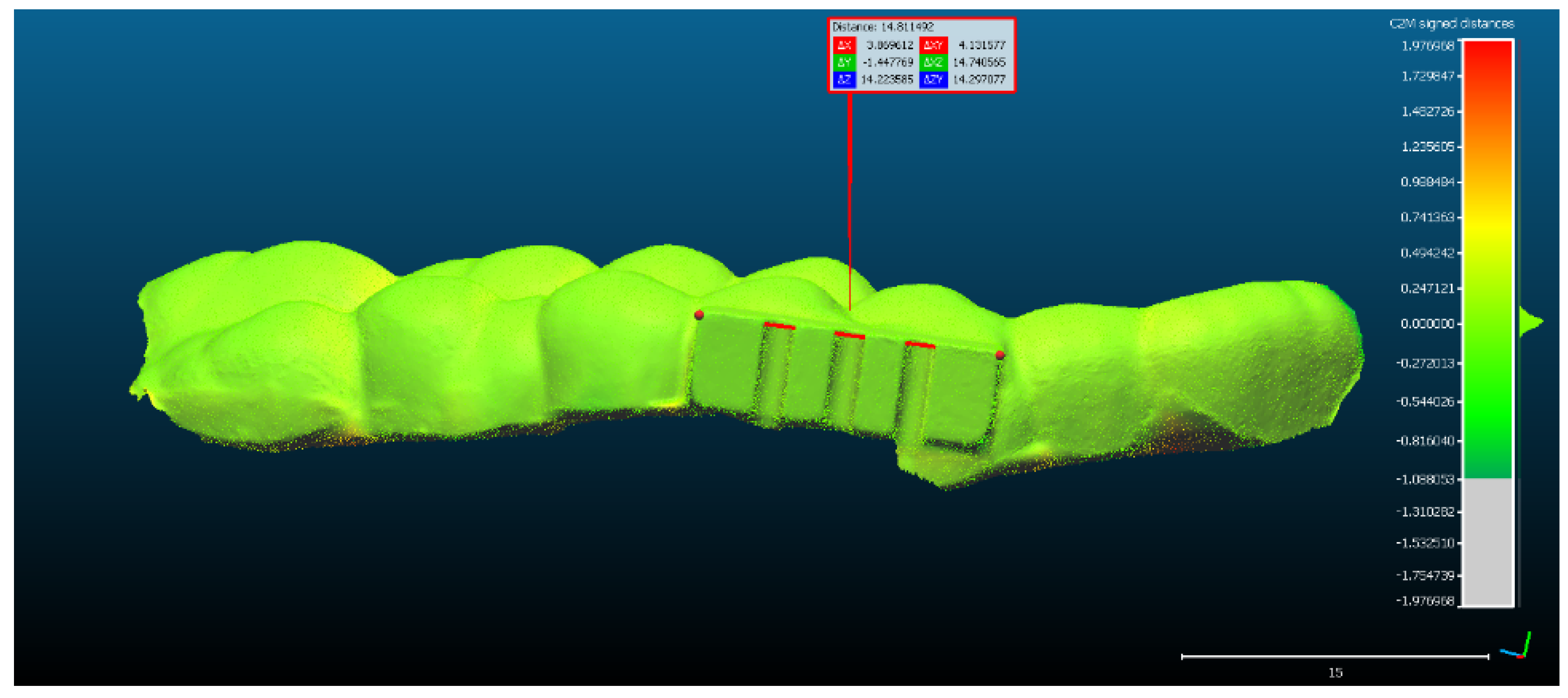
- The rectangular landmark, used for scaling the objects, measures in real world 15 mm in length. Its length in CCOSS after alignment was 13.939. Thus, 1 mm length in real world equaled 1.07 in CCOSS (Figure 6).
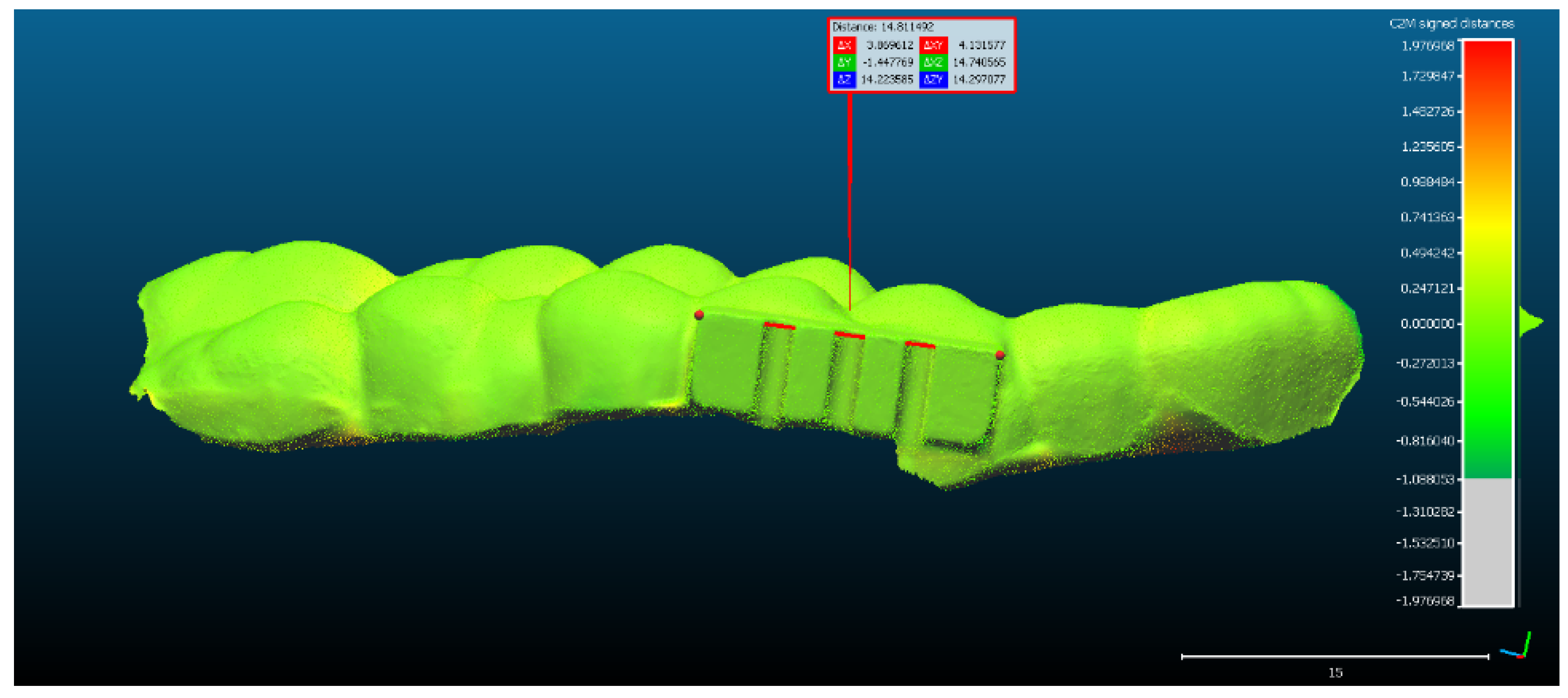
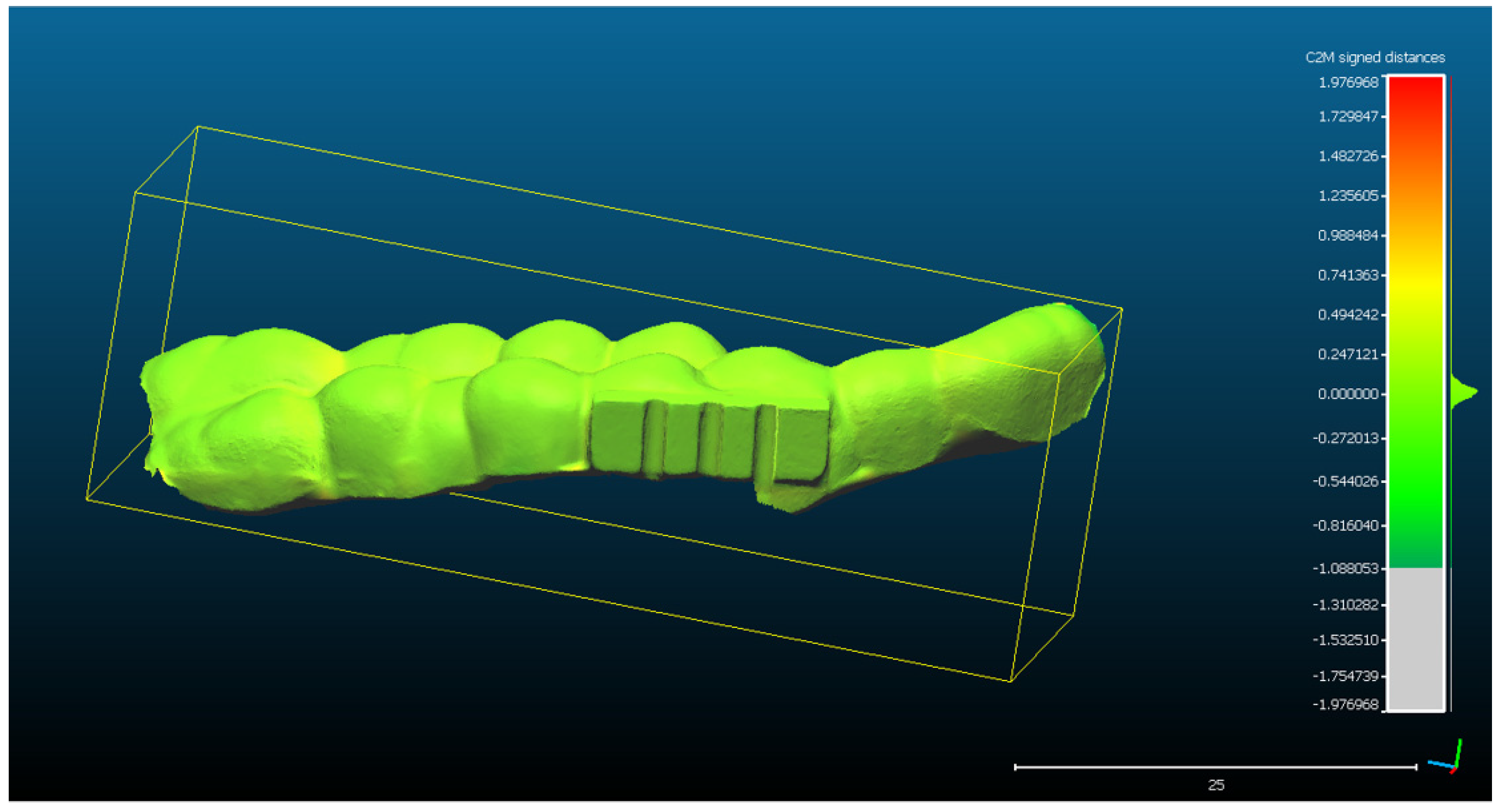
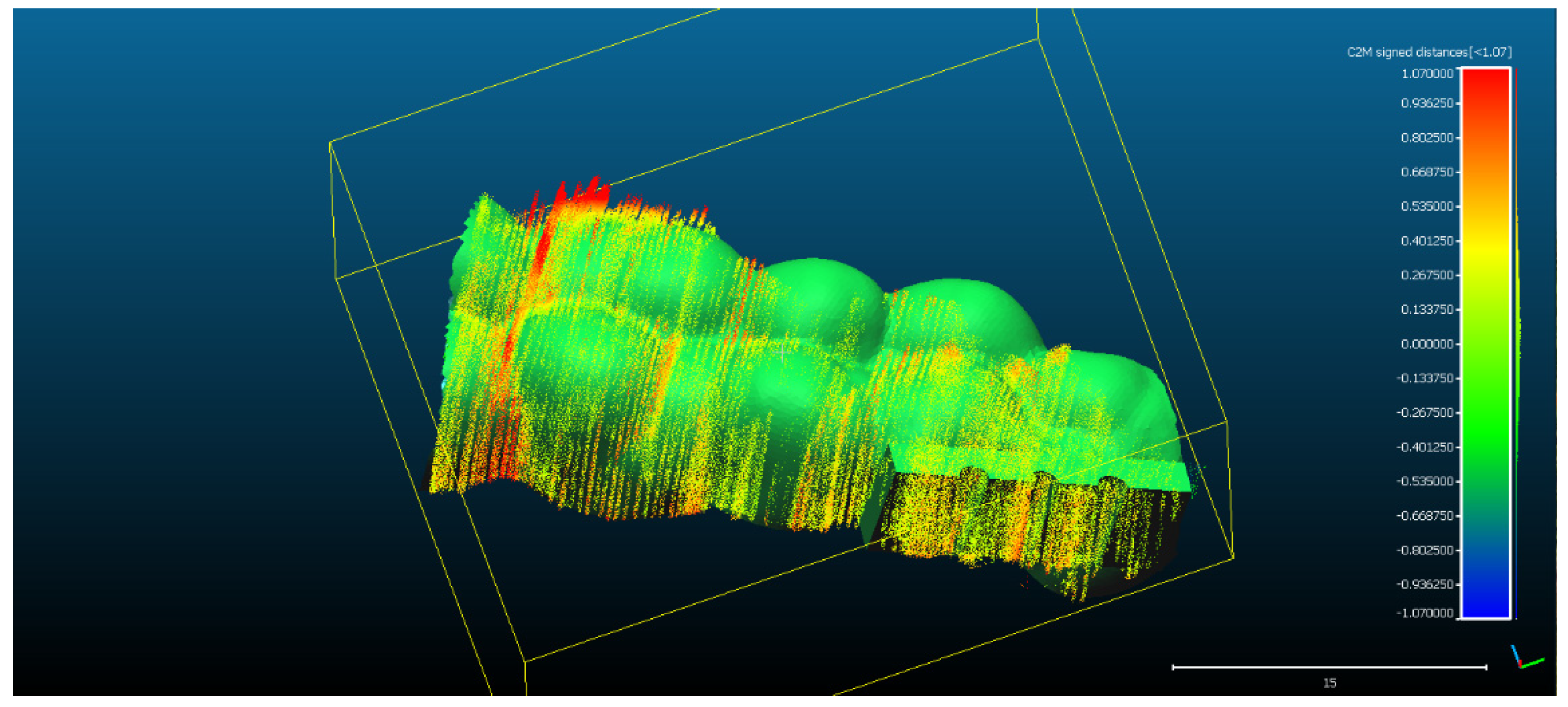
- The spatial distribution of the 272,189 3D ultrasonographic points was compared to the reference object (CAD project in STL format) after alignment. The distance errors of the 3D ultrasonographic points were uniformly distributed, meaning that the reconstruction respected the shape of the scanned object (Figure 7). The mean distance of the 3D ultrasonographic points from the reference object was 0.033 mm and the standard deviation equaled 0.387 mm (Table 1). The deviations were most probably due to the artifacts and to the noise in the 2D ultrasound original frames.
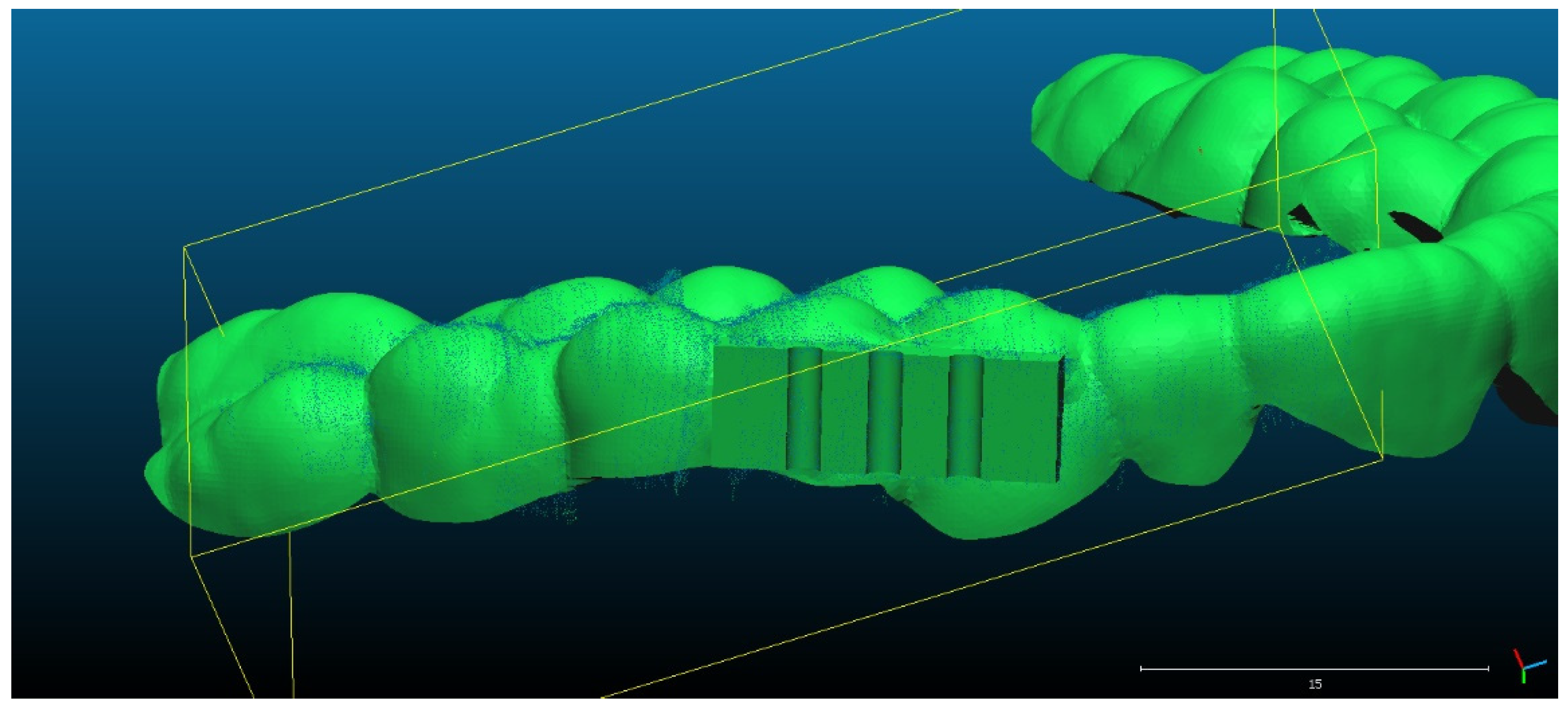
- Scan 2. After segmentation of the 2D images, the contours were extracted, before reconstructing the 3D object. The total number of 3D ultrasonographic points (masked by the segmented contours) was significantly lower (46,537) compared to the scan 1 (279,189 3D points as they were obtained without extracting the contours); the obtained 3D point cloud was aligned with the reference object (STL project), as shown in Figure 8, and the computed mean distance was 0.031 mm and the standard deviation was 0.287 mm (Figure 9a and Table 1). The deviations/errors were isolated to certain areas, probably due to the artifacts in some of the 2D original frames.
- For Scans 3 to 5, the alignment errors are presented in Figure 9b–d. The mean distance between the 3D points of the ultrasonographic reconstructions (obtained by masking the 3D point cloud with the segmented contours) and the reference scanned object varied in the range between 0.019 mm to 0.05 mm (Table 1).
3.3. Quantitative Evaluation by Statistical Error Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Zardi, E.M.; Franceschetti, E.; Giorgi, C.; Palumbo, A.; Franceschi, F. Accuracy and Performance of a New Handheld Ultrasound Machine with Wireless System. Sci. Rep. 2019, 9, 14599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stasi, G.; Ruoti, E.M. A Critical Evaluation in the Delivery of the Ultrasound Practice: The Point of View of the Radiologist. Ital. J. Med. 2015, 9, 5. [Google Scholar] [CrossRef] [Green Version]
- Huang, Q.; Zeng, Z. A Review on Real-Time 3D Ultrasound Imaging Technology. Biomed. Res. Int. 2017, 2017, 6027029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Q.H.; Zheng, Y.P.; Lu, M.H.; Chi, Z.R. Development of a Portable 3D Ultrasound Imaging System for Musculoskeletal Tissues. Ultrasonics 2005, 43, 153–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, J.; Huh, J.; Kim, M.; Hyun An, S.; Oh, Y.; Kim, D.; Chung, K.; Cho, S.; Lee, R. Accuracy of Volume Measurement Using 3D Ultrasound and Development of CT-3D US Image Fusion Algorithm for Prostate Cancer Radiotherapy: Volume Measurement and Dual-Modality Image Fusion Using 3D US. Med. Phys. 2013, 40, 021704. [Google Scholar] [CrossRef] [PubMed]
- Scorza, A.; Conforto, S.; D’Anna, C.; Sciuto, S.A. A Comparative Study on the Influence of Probe Placement on Quality Assurance Measurements in B-Mode Ultrasound by Means of Ultrasound Phantoms. Open Biomed. Eng. J. 2015, 9, 164–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Praça, L.; Pekam, F.C.; Rego, R.O.; Radermacher, K.; Wolfart, S.; Marotti, J. Accuracy of Single Crowns Fabricated from Ultrasound Digital Impressions. Dent. Mater. 2018, 34, e280–e288. [Google Scholar] [CrossRef] [PubMed]
- Le, L.H.; Nguyen, K.-C.T.; Kaipatur, N.R.; Major, P.W. Ultrasound for Periodontal Imaging. In Dental Ultrasound in Periodontology and Implantology; Chan, H.-L., Kripfgans, O.D., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 115–129. ISBN 978-3-030-51287-3. [Google Scholar]
- Slapa, R.; Jakubowski, W.; Slowinska-Srzednicka, J.; Szopinski, K. Advantages and Disadvantages of 3D Ultrasound of Thyroid Nodules Including Thin Slice Volume Rendering. Thyroid. Res. 2011, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buia, A.; Stockhausen, F.; Filmann, N.; Hanisch, E. 3D vs. 2D Imaging in Laparoscopic Surgery—An Advantage? Results of Standardised Black Box Training in Laparoscopic Surgery. Langenbecks Arch. Surg. 2017, 402, 167–171. [Google Scholar] [CrossRef] [PubMed]
- von Haxthausen, F.; Böttger, S.; Wulff, D.; Hagenah, J.; García-Vázquez, V.; Ipsen, S. Medical Robotics for Ultrasound Imaging: Current Systems and Future Trends. Curr. Robot. Rep. 2021, 2, 55–71. [Google Scholar] [CrossRef] [PubMed]
- Silvela, J.; Portillo, J. Breadth-First Search and Its Application to Image Processing Problems. IEEE Trans. Image Process. 2001, 10, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Shih, F.Y. Image Processing and Pattern Recognition: Fundamentals and Techniques; IEEE Press: Piscataway, NJ, USA; Wiley: Hoboken, NJ, USA, 2010; ISBN 978-0-470-40461-4. [Google Scholar]
- Open Computer Vision Library. Available online: https://Docs.Opencv.Org/3.4.17/Index.Html (accessed on 20 January 2022).
- Chifor, R.; Li, M.; Nguyen, K.-C.T.; Arsenescu, T.; Chifor, I.; Badea, A.F.; Badea, M.E.; Hotoleanu, M.; Major, P.W.; Le, L.H. Three-Dimensional Periodontal Investigations Using a Prototype Handheld Ultrasound Scanner with Spatial Positioning Reading Sensor. Med. Ultrason. 2021, 23, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.-W.; Prager, R.W.; Gee, A.H.; Treece, G.M. Freehand 3D Ultrasound Calibration: A Review. In Advanced Imaging in Biology and Medicine; Sensen, C.W., Hallgrímsson, B., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 47–84. ISBN 978-3-540-68992-8. [Google Scholar]
- Beddard, T. Registration RMS-CloudCompare ForumRegistration RMS-CloudCompare Forum. Available online: https://www.Danielgm.Net/Cc/Forum/Viewtopic.Php?T=1296 (accessed on 20 January 2022).
- Align-CloudCompareWiki. Available online: https://www.Cloudcompare.Org/Doc/Wiki/Index.Php?Title=Align (accessed on 20 January 2022).
- Alignment and Registration-CloudCompareWiki. Available online: https://www.Cloudcompare.Org/Doc/Wiki/Index.Php?Title=Alignment_and_Registration (accessed on 20 January 2022).
- Herickhoff, C.D.; Morgan, M.R.; Broder, J.S.; Dahl, J.J. Low-Cost Volumetric Ultrasound by Augmentation of 2D Systems: Design and Prototype. Ultrason. Imaging 2018, 40, 35–48. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Kang, D.-H.; Shim, S.; Im, M.; Seo, B.K.; Kim, H.; Lee, B.C. Versatile Low-Cost Volumetric 3D Ultrasound Imaging Using Gimbal-Assisted Distance Sensors and an Inertial Measurement Unit. Sensors 2020, 20, 6613. [Google Scholar] [CrossRef] [PubMed]
- Chuembou Pekam, F.; Marotti, J.; Wolfart, S.; Tinschert, J.; Radermacher, K.; Heger, S. High-Frequency Ultrasound as an Option for Scanning of Prepared Teeth: An in Vitro Study. Ultrasound Med. Biol. 2015, 41, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Marotti, J.; Broeckmann, J.; Chuembou Pekam, F.; Praça, L.; Radermacher, K.; Wolfart, S. Impression of Subgingival Dental Preparation Can Be Taken with Ultrasound. Ultrasound Med. Biol. 2019, 45, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Winkler, J.; Gkantidis, N. Trueness and Precision of Intraoral Scanners in the Maxillary Dental Arch: An in Vivo Analysis. Sci Rep. 2020, 10, 1172. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scan | Range of 2D Ultrasound Frames | Segmentation Mode | Scanning Time | Number of 3D Points | Mean Distance | Std Deviation |
|---|---|---|---|---|---|---|
| 1 | 300–752 | Segmentation without contour extraction | 13.69 s | 279,189 | 0.033 mm | 0.387 mm |
| 2 | 232–611 | Segmentation and contour extraction | 11.48 s | 46,537 | 0.031 mm | 0.287 mm |
| 3 | 252–703 | Segmentation and contour extraction | 13.66 s | 65,535 | 0.050 mm | 0.350 mm |
| 4 | 260–779 | Segmentation and contour extraction | 15.72 s | 70,774 | 0.014 mm | 0.352 mm |
| 5 | 220–674 | Segmentation and contour extraction | 13.75 s | 54,378 | 0.023 mm | 0.372 mm |
| 6 | 400–979 | Segmentation and contour extraction | 17.54 s | 76,735 | 0.019 mm | 0.565 mm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chifor, R.; Marita, T.; Arsenescu, T.; Santoma, A.; Badea, A.F.; Colosi, H.A.; Badea, M.-E.; Chifor, I. Accuracy Report on a Handheld 3D Ultrasound Scanner Prototype Based on a Standard Ultrasound Machine and a Spatial Pose Reading Sensor. Sensors 2022, 22, 3358. https://doi.org/10.3390/s22093358
Chifor R, Marita T, Arsenescu T, Santoma A, Badea AF, Colosi HA, Badea M-E, Chifor I. Accuracy Report on a Handheld 3D Ultrasound Scanner Prototype Based on a Standard Ultrasound Machine and a Spatial Pose Reading Sensor. Sensors. 2022; 22(9):3358. https://doi.org/10.3390/s22093358
Chicago/Turabian StyleChifor, Radu, Tiberiu Marita, Tudor Arsenescu, Andrei Santoma, Alexandru Florin Badea, Horatiu Alexandru Colosi, Mindra-Eugenia Badea, and Ioana Chifor. 2022. "Accuracy Report on a Handheld 3D Ultrasound Scanner Prototype Based on a Standard Ultrasound Machine and a Spatial Pose Reading Sensor" Sensors 22, no. 9: 3358. https://doi.org/10.3390/s22093358
APA StyleChifor, R., Marita, T., Arsenescu, T., Santoma, A., Badea, A. F., Colosi, H. A., Badea, M.-E., & Chifor, I. (2022). Accuracy Report on a Handheld 3D Ultrasound Scanner Prototype Based on a Standard Ultrasound Machine and a Spatial Pose Reading Sensor. Sensors, 22(9), 3358. https://doi.org/10.3390/s22093358