
Establishing Accelerometer Cut-Points to Classify Walking Speed in People Post Stroke


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Data Collection
2.3. Data Management and Analysis
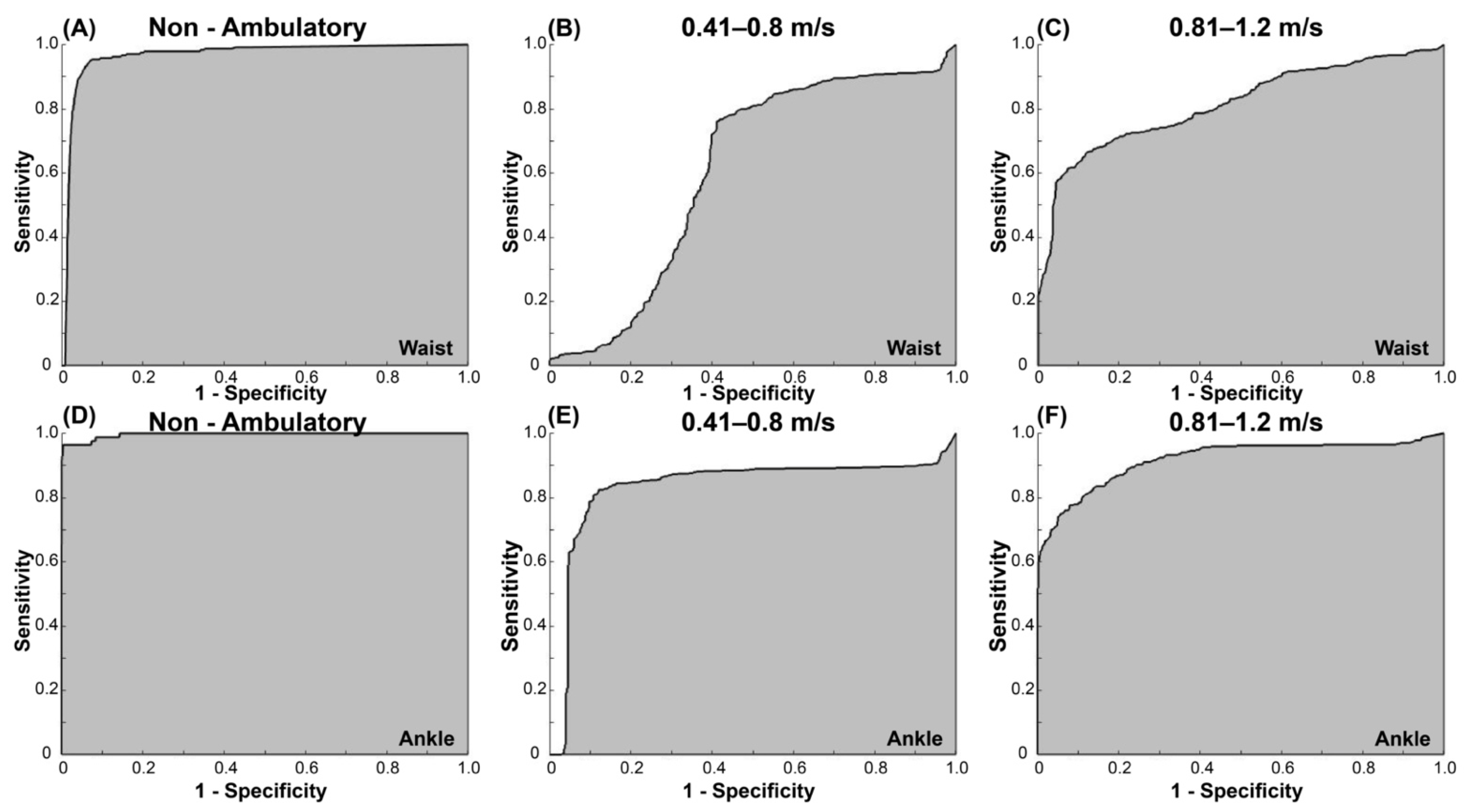
3. Results
3.1. Study Participants
3.2. Cut-Points
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Perera, S.; Patel, K.V.; Rosano, C.; Rubin, S.M.; Satterfield, S.; Harris, T.; Ensrud, K.; Orwoll, E.; Lee, C.G.; Chandler, J.M.; et al. Gait Speed Predicts Incident Disability: A Pooled Analysis. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Kritchevsky, S.; Newman, A.B.; Simonsick, E.M.; Harris, T.B.; Penninx, B.W.; Pt, J.S.B.; Tylavsky, F.A.; Satterfield, S.; Bauer, D.C.; et al. Added Value of Physical Performance Measures in Predicting Adverse Health-Related Events: Results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2009, 57, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait Speed and Survival in Older Adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, S.E.; McPherson, K.; McNaughton, H.K.; Rochester, L.; Weatherall, M. Community ambulation after stroke: How important and obtainable is it and what measures appear predictive? Arch. Phys. Med. Rehabil. 2004, 85, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Fulk, G.D.; He, Y.; Boyne, P.; Dunning, K. Predicting Home and Community Walking Activity Poststroke. Stroke 2017, 48, 406–411. [Google Scholar] [CrossRef]
- Rabadi, M.H.; Blau, A. Admission Ambulation Velocity Predicts Length of Stay and Discharge Disposition Following Stroke in an Acute Rehabilitation Hospital. Neurorehabilit. Neural Repair 2005, 19, 20–26. [Google Scholar] [CrossRef]
- Fulk, G.D.; Echternach, J.L.; Nof, L.; O’Sullivan, S. Clinometric properties of the six-minute walk test in individuals undergoing rehabilitation poststroke. Physiother. Theory Pract. 2008, 24, 195–204. [Google Scholar] [CrossRef]
- John, D.; Freedson, P. ActiGraph and Actical physical activity monitors: A peek under the hood. Med. Sci. Sports Exerc. 2012, 44 (Suppl. S1), S86–S89. [Google Scholar] [CrossRef] [Green Version]
- Barriera, T.V.; Tudor-Locke, C.; Champagne, C.M.; Broyles, S.T.; Johnson, W.D.; Katzmarzyk, P.T. Comparison of GT3X accelerometer and YAMAX pedometer steps/day in a free-living sample of overweight and obese adults. J. Phys. Act. Health 2013, 10, 263–270. [Google Scholar] [CrossRef]
- Korpan, S.M.; Schafer, J.L.; Wilson, K.C.; Webber, S. Effect of ActiGraph GT3X+ Position and Algorithm Choice on Step Count Accuracy in Older Adults. J. Aging Phys. Act. 2015, 23, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Bianchim, M.S.; McNarry, M.A.; Larun, L.; Mackintosh, K.A. Calibration and validation of accelerometry to measure physical activity in adult clinical groups: A systematic review. Prev. Med. Rep. 2019, 16, 101001. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Reed, J.; Mark, A.E.; Blanchard, C.M.; Grace, S.; Reid, R.D. A Comparison of Accelerometer Cut-Points among Individuals with Coronary Artery Disease. PLoS ONE 2015, 10, e0137759. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Welk, G.J. Criterion Validity of Competing Accelerometry-Based Activity Monitoring Devices. Med. Sci. Sports Exerc. 2015, 47, 2456–2463. [Google Scholar] [CrossRef]
- Rothney, M.P.; Schaefer, E.V.; Neumann, M.M.; Choi, L.; Chen, K. Validity of Physical Activity Intensity Predictions by ActiGraph, Actical, and RT3 Accelerometers. Obesity 2008, 16, 1946–1952. [Google Scholar] [CrossRef]
- Wetten, A.A.; Batterham, M.; Tan, S.-Y.; Tapsell, L. Relative Validity of 3 Accelerometer Models for Estimating Energy Expenditure During Light Activity. J. Phys. Act. Health 2014, 11, 638–647. [Google Scholar] [CrossRef] [Green Version]
- Corder, K.; Brage, S.; Ekelund, U. Accelerometers and pedometers: Methodology and clinical application. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 597–603. [Google Scholar] [CrossRef]
- Compagnat, M.; Mandigout, S.; Chaparro, D.; Daviet, J.C.; Salle, J.Y. Validity of the Actigraph GT3x and influence of the sensor positioning for the assessment of active energy expenditure during four activities of daily living in stroke subjects. Clin. Rehabil. 2018, 32, 1696–1704. [Google Scholar] [CrossRef]
- Mandigout, S.; Lacroix, J.; Ferry, B.; Vuillerme, N.; Compagnat, M.; Daviet, J.C. Can energy expenditure be accurately assessed using accelerometry-based wearable motion detectors for physical activity monitoring in post-stroke patients in the subacute phase? Eur. J. Prev. Cardiol. 2017, 24, 2009–2016. [Google Scholar] [CrossRef]
- Jayaraman, C.; Mummidisetty, C.K.; Mannix-Slobig, A.; Koch, L.M.; Jayaraman, A. Variables influencing wearable sensor outcome estimates in individuals with stroke and incomplete spinal cord injury: A pilot investigation validating two research grade sensors. J. Neuroeng. Rehabil. 2018, 15, 19. [Google Scholar] [CrossRef]
- Richards, C.L.; Malouin, F.; Dean, C. Gait in Stroke: Assessment and Rehabilitation. Clin. Geriatr. Med. 1999, 15, 833–856. [Google Scholar] [CrossRef]
- Faria, G.S.; Polese, J.C.; Ribeiro-Samora, G.A.; Scianni, A.A.; Faria, C.; Teixeira-Salmela, L.F. Validity of the accelerometer and smartphone application in estimating energy expenditure in individuals with chronic stroke. Braz. J. Phys. Ther. 2019, 23, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Campos, C.; DePaul, V.G.; Knorr, S.; Wong, J.S.; Mansfield, A.; Patterson, K.K. Validity of the ActiGraph activity monitor for individuals who walk slowly post-stroke. Top. Stroke Rehabil. 2018, 25, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Polese, J.C.; E Faria, G.S.; Ribeiro-Samora, G.A.; Lima, L.P.; Faria, C.; Scianni, A.A.; Teixeira-Salmela, L.F. Google fit smartphone application or Gt3X Actigraph: Which is better for detecting the stepping activity of individuals with stroke? A validity study. J. Bodyw. Mov. Ther. 2019, 23, 461–465. [Google Scholar] [CrossRef]
- Aguilar-Farias, N.; Brown, W.J.; Peeters, G. ActiGraph GT3X+ cut-points for identifying sedentary behaviour in older adults in free-living environments. J. Sci. Med. Sport 2013, 17, 293–299. [Google Scholar] [CrossRef]
- Handlery, R.; Fulk, G.; Pellegrini, C.; Stewart, J.C.; Monroe, C.; Fritz, S. Stepping After Stroke: Walking Characteristics in People With Chronic Stroke Differ on the Basis of Walking Speed, Walking Endurance, and Daily Steps. Phys. Ther. 2020, 100, 807–817. [Google Scholar] [CrossRef]
- Lyden, P. Using the National Institutes of Health Stroke Scale: A Cautionary Tale. Stroke 2017, 48, 513–519. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Hermodsson, Y.; Ekdahl, C. Early planning of care and rehabilitation after amputation for vascular disease by means of Katz Index of Activities of Daily Living. Scand. J. Caring Sci. 1999, 13, 234–239. [Google Scholar] [CrossRef]
- Butland, R.J.; Pang, J.; Gross, E.R.; Woodcock, A.A.; Geddes, D.M. Two-, six-, and 12-minute walking tests in respiratory disease. Br. Med. J. 1982, 284, 1607–1608. [Google Scholar] [CrossRef] [Green Version]
- Webber, S.C.; John, P.D.S. Comparison of ActiGraph GT3X+ and StepWatch Step Count Accuracy in Geriatric Rehabilitation Patients. J. Aging Phys. Act. 2016, 24, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Joseph, C.; Rhoda, A.; Conradsson, D.M. Levels and patterns of physical activity in stroke survivors with different ambulation status living in low-income areas of Cape Town, South Africa. Top. Stroke Rehabil. 2020, 27, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, C.; Strömbäck, B.; Hagströmer, M.; Conradsson, D. Accelerometry: A feasible method to monitor physical activity during sub-acute rehabilitation of persons with stroke. J. Rehabil. Med. 2018, 50, 429–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bezuidenhout, L.; Joseph, C.; Einarsson, U.; Thurston, C.; Hagströmer, M.; Conradsson, D.M. Accelerometer assessed upper limb activity in people with stroke: A validation study considering ambulatory and non-ambulatory activities. Disabil. Rehabil. 2021, 2021, e2012838. [Google Scholar] [CrossRef] [PubMed]
- Brønd, J.C.; Andersen, L.B.; Arvidsson, D. Generating ActiGraph Counts from Raw Acceleration Recorded by an Alternative Monitor. Med. Sci. Sports Exerc. 2017, 49, 2351–2360. [Google Scholar] [CrossRef] [PubMed]
- Feito, Y.; Garner, H.R.; Bassett, D.R. Evaluation of ActiGraph’s Low-Frequency Filter in Laboratory and Free-Living Environments. Med. Sci. Sports Exerc. 2015, 47, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Feito, Y.; Hornbuckle, L.M.; Reid, L.A.; Crouter, S.E. Effect of ActiGraph’s low frequency extension for estimating steps and physical activity intensity. PLoS ONE 2017, 12, e0188242. [Google Scholar] [CrossRef] [Green Version]
- Cain, K.L.; Conway, T.L.; Adams, M.A.; Husak, L.E.; Sallis, J.F. Comparison of older and newer generations of ActiGraph accelerometers with the normal filter and the low frequency extension. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Perry, J.; Garrett, M.; Gronley, J.K.; Mulroy, S.J. Classification of Walking Handicap in the Stroke Population. Stroke 1995, 26, 982–989. [Google Scholar] [CrossRef]
- Bezuidenhout, L.; Thurston, C.; Hagströmer, M.; Conradsson, D.M. Validity of Hip and Ankle Worn Actigraph Accelerometers for Measuring Steps as a Function of Gait Speed during Steady State Walking and Continuous Turning. Sensors 2021, 21, 3154. [Google Scholar] [CrossRef]
- Holmlund, T.; Ekblom-Bak, E.; Franzén, E.; Hultling, C.; Wahman, K. Defining accelerometer cut-points for different intensity levels in motor-complete spinal cord injury. Spinal Cord 2020, 58, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Nero, H.; Wallén, M.B.; Franzén, E.; Ståhle, A.; Hagstromer, M. Accelerometer Cut Points for Physical Activity Assessment of Older Adults with Parkinson’s Disease. PLoS ONE 2015, 10, e0135899. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Fees, B.S.; Haar, S.J.; Murray, A.D.; Crowe, L.K. Identification and Validity of Accelerometer Cut-Points for Toddlers. Obesity 2012, 20, 2317–2319. [Google Scholar] [CrossRef] [PubMed]
- Copeland, J.L.; Esliger, D.W. Accelerometer Assessment of Physical Activity in Active, Healthy Older Adults. J. Aging Phys. Act. 2009, 17, 17–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, V.L.; Perry, L.A.; Mercado, M.W.; Kautz, S.A.; Patten, C. Gait asymmetry pattern following stroke determines acute response to locomotor task. Gait Posture 2020, 77, 300–307. [Google Scholar] [CrossRef]
- Lamont, R.M.; Morris, M.E.; Woollacott, M.H.; Brauer, S.G. Community walking in people with Parkinson’s disease. Parkinsons Dis. 2012, 2012, 856237. [Google Scholar] [CrossRef]
- Treacy, D.; Hassett, L.; Schurr, K.; Chagpar, S.; Paul, S.S.; Sherrington, C. Validity of Different Activity Monitors to Count Steps in an Inpatient Rehabilitation Setting. Phys. Ther. 2017, 97, 581–588. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; Brookes, D.S.K.; Ahmadi, M.N. Evaluation of Wrist Accelerometer Cut-Points for Classifying Physical Activity Intensity in Youth. Front. Digit. Health 2022, 4, 884307. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Task | Description and Instructions |
|---|---|
| Non-ambulatory 1 | |
| Sitting (5 min) | The test leader conducted structured interviews related to demographics and personal factors while the participants were seated on a regular chair in front of a table. |
| Setting the table (3 min) | Participants sat on a chair with three kitchen crockery set placed in front of them and were asked to align all items as if they were setting the table for dinner. After completing this, participants returned the items back to the starting position and repeated the task. |
| Washing dishes (6 min) | Participants were equipped with a dish-cleaning brush and stood in front of a kitchen sink with a kitchen crockery set positioned on the left-hand side of the sink. The participants were asked to wash the dishes, dry the dishes with a cloth and position them on the right-hand side of the sink. This process was repeated, this time while moving the dishes from the right to the left-hand side. |
| Walking 2 | |
| Self-selected walking speed (6 min) | Participants were asked to “walk at their normal comfortable walking speed for 6 min”. |
| Brisk walking speed (6 min) | Participants were asked to “walk as fast as they can in a safe manner, without running, for 6 min”. |
| Variables | People Post Stroke (n = 42) |
|---|---|
| Male sex, n (%) | 19 (45) |
| Age (years), mean (SD) | 63.4 (12.4) |
| Living alone, n (%) | 15 (36) |
| Body mass index, mean (SD) | 25.8 (3.5) |
| Mobility status, n (%) | |
| Unaided | 30 (71) |
| Walking aid | 12 (29) |
| Years since stroke, mean (SD) | 2.4 (3.9) |
| Type of stroke, n (%) | |
| Ischemic | 31 (74) |
| Hemorrhage | 11 (26) |
| Affected side, n (%) | |
| Right | 15 (36) |
| Left | 27 (64) |
| NIHS stroke scale | 2.1 (1.6) |
| MOCA score, mean (SD) | 24.6 (3.5) |
| KATZ, n (%) | |
| Independent Primary ADL | 35 (83) |
| Independent Instrumental ADL | 20 (48) |
| 15 s Epoch | ||||||
|---|---|---|---|---|---|---|
| Waist | Ankle | |||||
| n | Median (95% CI) | n | Median (95% CI) | |||
| Vertical | VM | Vertical | VM | |||
| Non-amb. | 107 | 0 (7–39) | 0 (15–70) | 93 | 0 (7–22) | 0 (15–39) |
| 0.41–0.8 m/s | 20 | 338 (283–441) | 519 (495–790) | 16 | 912 (724–1421) | 1394 (1135–1890) |
| 0.81–1.2 m/s | 28 | 423 (341–477) | 759 (621–847) | 24 | 1898 (1444–2140) | 2546 (2021–2774) |
| >1.2 m/s | 22 | 555 (456–653) | 1147 (976–1285) | 15 | 3456 (2961–4354) | 4045 (3479–4876) |
| 1 min Epoch | ||||||
| Non-amb. | 107 | 17 (41–157) | 44 (78–280) | 93 | 14 (41–89) | 37 (78–158) |
| 0.41–0.8 m/s | 20 | 1204 (997–1634) | 1908 (1735–2932) | 16 | 3496 (2593–5287) | 5393 (4029–7064) |
| 0.81–1.2 m/s | 28 | 1628 (1265–1793) | 2758 (2287–3181) | 24 | 6777 (5265–8037) | 9660 (7392–10,474) |
| >1.2 m/s | 22 | 2099 (1580–2450) | 4244 (3348–4839) | 15 | 13,178 (10,023–16,569) | 15,576 (11,774–18,619) |
| 15 s | |||||||||
| Waist | Ankle | ||||||||
| Axis | Cat. | Sen. | Spec. | AUC | Cut-Point | Sen. | Spec. | AUC | Cut-Point |
| V | Non-amb. | 0.80 | 0.87 | 0.92 | ≤41 | 0.96 | 0.99 | 0.99 | ≤184 |
| 0.41–0.8 | 0.70 | 0.57 | 0.60 | 42–372 | 0.75 | 0.83 | 0.79 | 185–1363 | |
| 0.81–1.2 | 0.58 | 0.74 | 0.66 | 373–502 | 0.79 | 0.91 | 0.91 | 1364–2851 | |
| VM | |||||||||
| Non-amb. | 0.95 | 0.93 | 0.97 | ≤140 | 0.96 | 0.99 | 0.99 | ≤401 | |
| 0.41–0.8 | 0.76 | 0.59 | 0.61 | 141–572 | 0.82 | 0.88 | 0.83 | 402–1862 | |
| 0.81–1.2 | 0.71 | 0.81 | 0.81 | 573–990 | 0.83 | 0.86 | 0.92 | 1863–3265 | |
| 1 min | |||||||||
| Waist | Ankle | ||||||||
| Axis | Cat. | Sen. | Spec. | AUC | Cut-Point | Sen. | Spec. | AUC | Cut-Point |
| V | Non-amb. | 0.77 | 0.92 | 0.91 | ≤270 | 0.92 | 0.99 | 0.98 | ≤570 |
| 0.41–0.8 | 0.65 | 0.65 | 0.60 | 271–1458 | 0.76 | 0.76 | 0.76 | 571–4445 | |
| 0.81–1.2 | 0.53 | 0.79 | 0.63 | 1459–2055 | 0.73 | 0.89 | 0.84 | 4446–10,793 | |
| VM | |||||||||
| Non-amb. | 0.92 | 0.91 | 0.95 | ≤491 | 0.96 | 0.92 | 0.98 | ≤779 | |
| 0.41–0.8 | 0.72 | 0.66 | 0.61 | 492–2254 | 0.75 | 0.89 | 0.80 | 780–7200 | |
| 0.81–1.2 | 0.64 | 0.90 | 0.76 | 2255–4058 | 0.80 | 0.86 | 0.84 | 7201–12,487 | |
| Waist VM Counts /15 s | Ankle VM Counts /15 s | |
|---|---|---|
| Non-ambulation | ≤140 | ≤401 |
| 0.41–0.8 m/s | 141–572 | 402–1862 |
| 0.81–1.2 m/s | 573–990 | 1863–3265 |
| >1.2 m/s | ≥991 | ≥3266 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moulaee Conradsson, D.; Bezuidenhout, L.J.-R. Establishing Accelerometer Cut-Points to Classify Walking Speed in People Post Stroke. Sensors 2022, 22, 4080. https://doi.org/10.3390/s22114080
Moulaee Conradsson D, Bezuidenhout LJ-R. Establishing Accelerometer Cut-Points to Classify Walking Speed in People Post Stroke. Sensors. 2022; 22(11):4080. https://doi.org/10.3390/s22114080
Chicago/Turabian StyleMoulaee Conradsson, David, and Lucian John-Ross Bezuidenhout. 2022. "Establishing Accelerometer Cut-Points to Classify Walking Speed in People Post Stroke" Sensors 22, no. 11: 4080. https://doi.org/10.3390/s22114080
APA StyleMoulaee Conradsson, D., & Bezuidenhout, L. J.-R. (2022). Establishing Accelerometer Cut-Points to Classify Walking Speed in People Post Stroke. Sensors, 22(11), 4080. https://doi.org/10.3390/s22114080