
Modified Functional Reach Test: Upper-Body Kinematics and Muscular Activity in Chronic Stroke Survivors

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Set-Up and Protocol
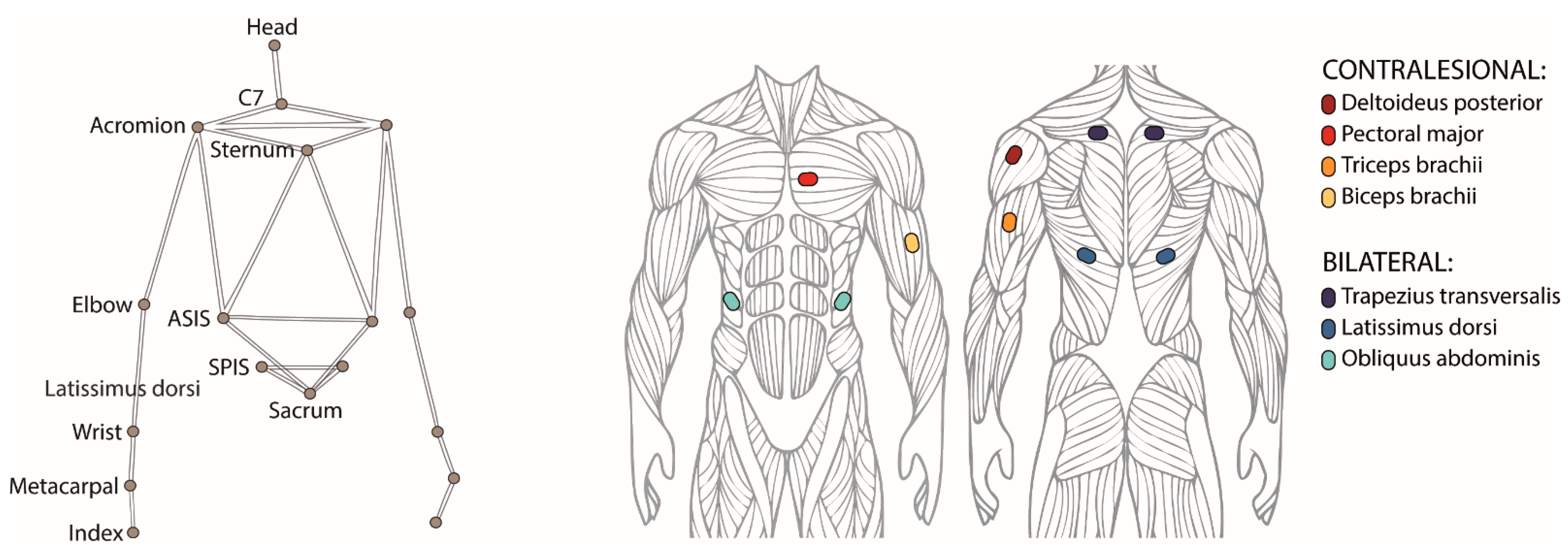
2.3. Data Acquisition
2.4. Data Analysis
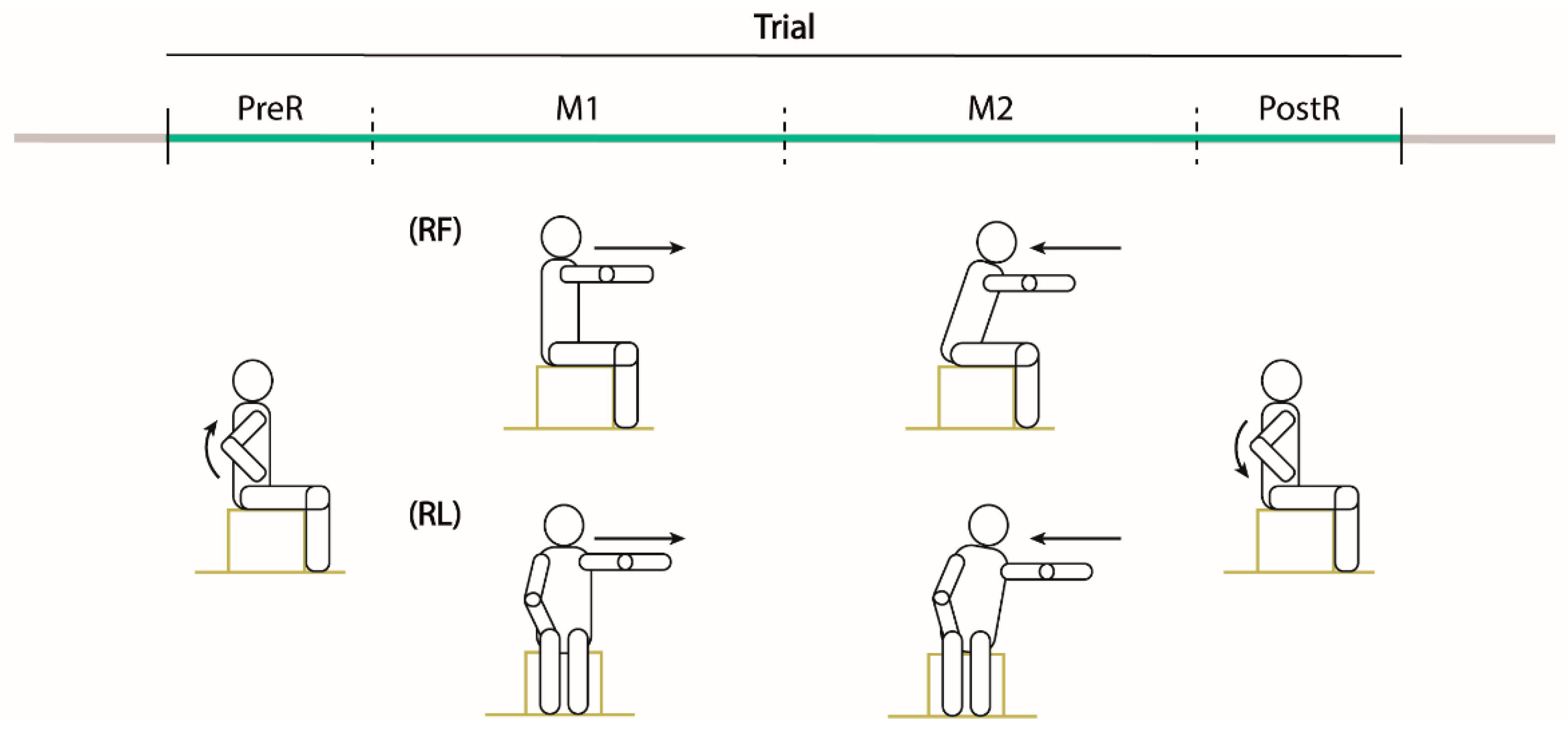
- PreR. The participants raised up the ipsilesional arm. This phase started when the hand speed along the y-axis reached 10% of its peak speed (Hy) and ended when the shoulder speed along the movement direction (x or z for RL and RF, respectively) was higher than 10% of its peak speed (Sx or Sz).
- Reaching movement (M1). The participant performed the reaching movement to the maximum distance. This phase started at the end of the PreR phase and ended when the maximum distance was reached (D).
- Return movement (M2). The participant moved back to the starting position. Specifically, this phase started at the end of the M1 phase and ended when the shoulder speed in the movement direction was lower than 10% of its peak speed (Sx or Sz).
- PostR. The participant lowered the ipsilesional arm. This phase started at the end of the M2 phase and ended when the hand speed along the y-axis was lower than 10% of its peak speed (Hy).
- Normalized reaching distance, i.e., the maximum distance reached by the acromion marker in the movement direction, normalized by the arm length. It is computed as follows:
- Movement time, i.e., the time to complete the M1 and M2 phases of the movement;
- Δpelvis, computed as the mean value, over the M1 and M2 phases, of the absolute difference between coordinates along the vertical y-axis of the contralesional (YC) and ipsilesional (YI) superior iliac spine markers:
Statistical Analysis
- the trunk muscles’ activations in the contra and ipsilesional side;
- the muscles’ activations in the contralesional arm, not actively engaged in the reaching movement;
- the effects of the reaching movement repetition on the muscles’ activations and kinematic performance.
3. Results
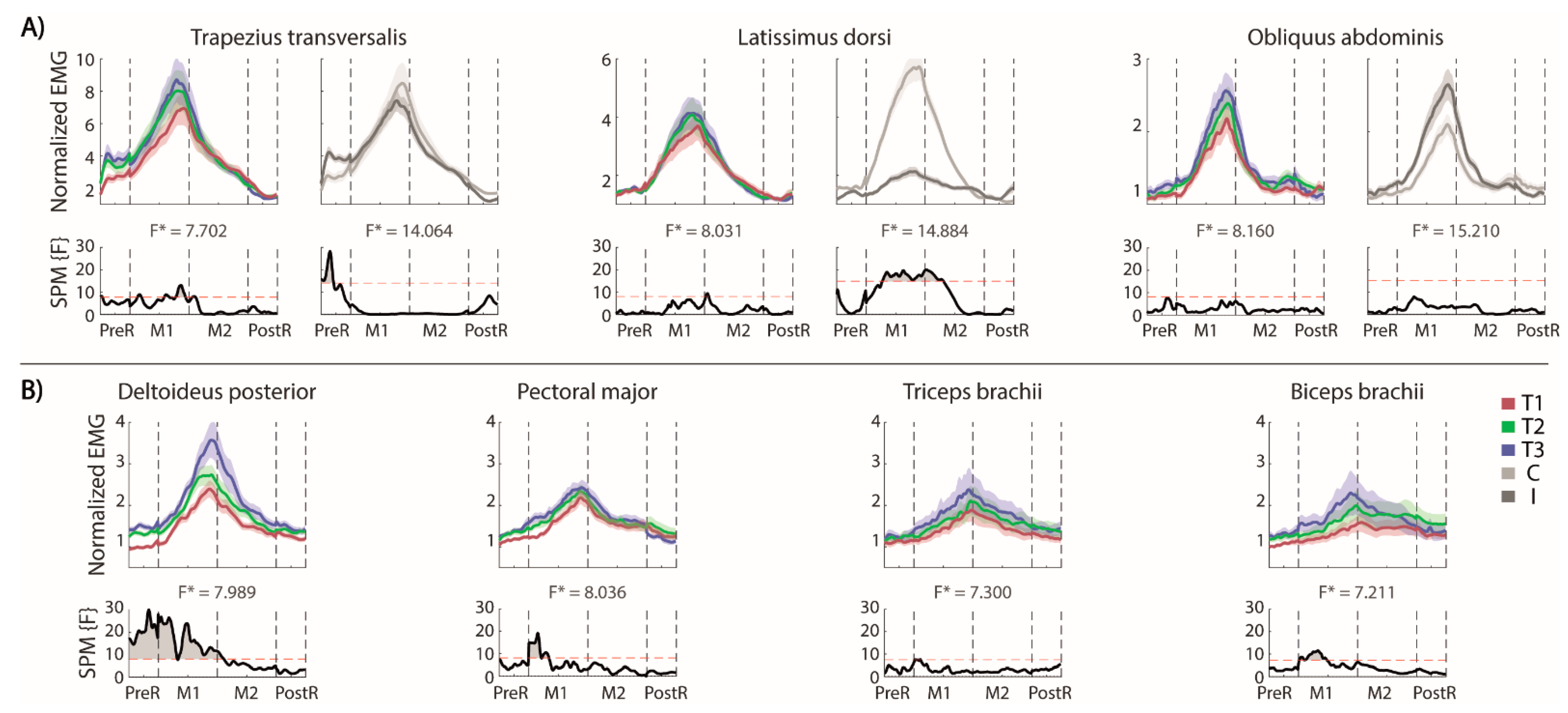
3.1. Frontal Reaching
Muscle Activity
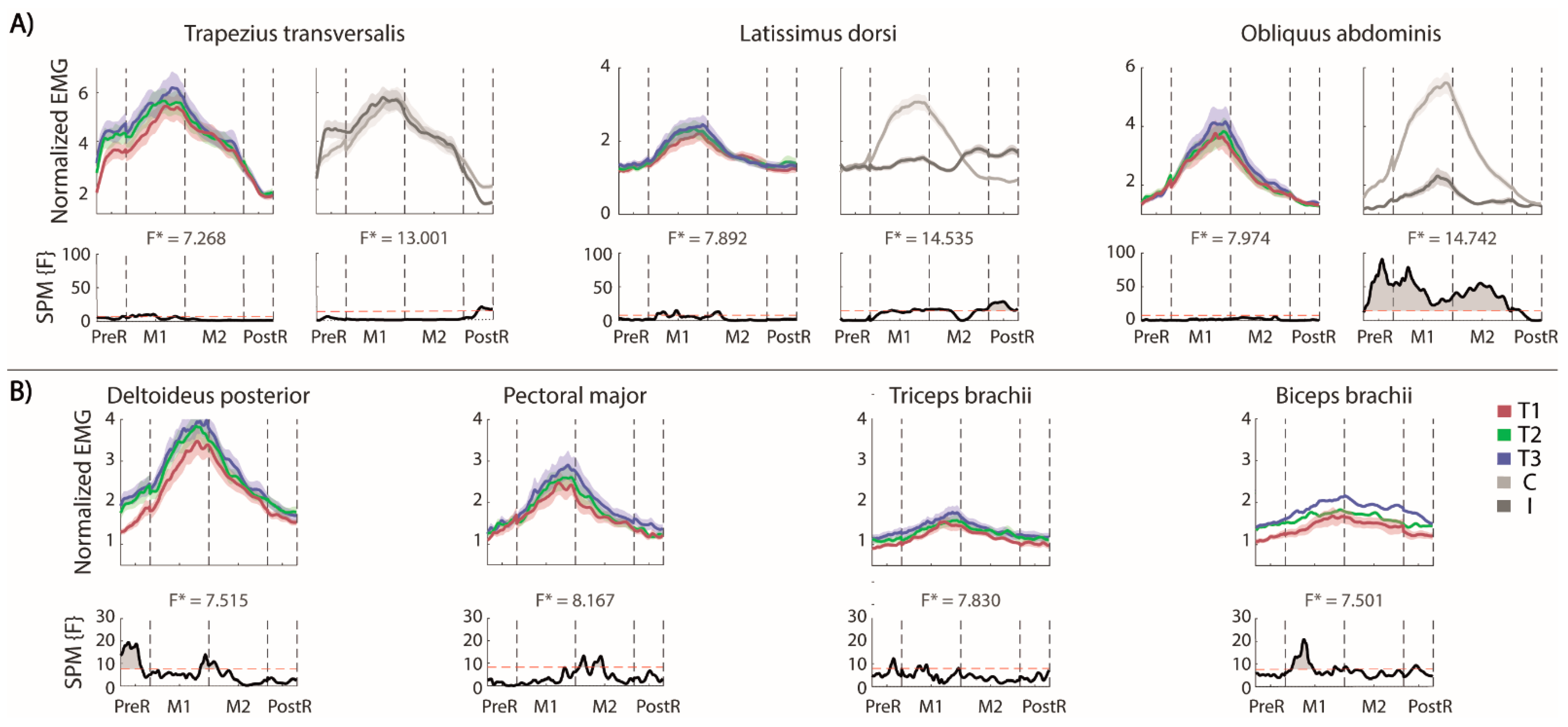
3.2. Lateral Reaching
Muscle Activity
4. Discussion
4.1. Trunk Muscles Activity
4.2. Muscles’ Activations in the Contralesional Arm, Not Actively Engaged in the Movement
4.3. Repetitions of Reaching Movement
4.4. Correlation between Clinical Test and Distance Reached in Frontal and Lateral MFRT
4.5. Limitations and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karthikbabu, S.; Chakrapani, M.; Ganeshan, S.; Rakshith, K.C.; Nafeez, S.; Prem, V. A review on assessment and treatment of the trunk in stroke: A need or luxury. Neural Regen. Res. 2012, 7, 1974. [Google Scholar]
- Dean, C.; Shepherd, R.; Adams, R. Sitting balance I: Trunk–arm coordination and the contribution of the lower limbs during self-paced reaching in sitting. Gait Posture 1999, 10, 135–146. [Google Scholar] [CrossRef]
- Segal, M. Muscle overactivity in the upper motor neuron syndrome: Pathophysiology. Phys. Med. Rehabil. Clin. N. Am. 2018, 29, 427–436. [Google Scholar] [CrossRef]
- McGill, S.M.; Grenier, S.; Kavcic, N.; Cholewicki, J. Coordination of muscle activity to assure stability of the lumbar spine. J. Electromyogr. Kinesiol. 2003, 13, 353–359. [Google Scholar] [CrossRef]
- Meyer, S.; Karttunen, A.H.; Thijs, V.; Feys, H.; Verheyden, G. How do somatosensory deficits in the arm and hand relate to upper limb impairment, activity, and participation problems after stroke? A systematic review. Phys. Ther. 2014, 94, 1220–1231. [Google Scholar] [CrossRef] [PubMed]
- Campbell, F.M.; Ashburn, A.M.; Pickering, R.M.; Burnett, M. Head and pelvic movements during a dynamic reaching task in sitting: Implications for physical therapists. Arch. Phys. Med. Rehabil. 2001, 82, 1655–1660. [Google Scholar] [CrossRef] [PubMed]
- Geiger, R.A.; Allen, J.B.; O’Keefe, J.; Hicks, R.R. Balance and mobility following stroke: Effects of physical therapy interventions with and without biofeedback/forceplate training. Phys. Ther. 2001, 81, 995–1005. [Google Scholar] [CrossRef] [PubMed]
- Cabanas-Valdés, R.; Cuchi, G.U.; Bagur-Calafat, C. Trunk training exercises approaches for improving trunk performance and functional sitting balance in patients with stroke: A systematic review. NeuroRehabilitation 2013, 33, 575–592. [Google Scholar] [CrossRef]
- Tessem, S.; Hagstrøm, N.; Fallang, B. Weight distribution in standing and sitting positions, and weight transfer during reaching tasks, in seated stroke subjects and healthy subjects. Physiother. Res. Int. 2007, 12, 82–94. [Google Scholar] [CrossRef]
- Wiskerke, E.; van Dijk, M.; Thuwis, R.; Vandekerckhove, C.; Myny, C.; Kool, J.; Dejaeger, E.; Beyens, H.; Verheyden, G. Maximum weight-shifts in sitting in non-ambulatory people with stroke are related to trunk control and balance: A cross-sectional study. Gait Posture 2021, 83, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Feigin, L.; Sharon, B.; Czaczkes, B.; Rosin, A.J. Sitting equilibrium 2 weeks after a stroke can predict the walking ability after 6 months. Gerontology 1996, 42, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Lee, D.; Hong, S.; Shin, D.; Jeong, S.; Shin, H.; Choi, W.; An, S.; Lee, G. The relationship between sitting balance, trunk control and mobility with predictive for current mobility level in survivors of sub-acute stroke. PLoS ONE 2021, 16, e0251977. [Google Scholar] [CrossRef]
- Duarte, E.; Marco, E.; Muniesa, J.M.; Belmonte, R.; Diaz, P.; Tejero, M.; Escalada, F. Trunk control test as a functional predictor in stroke patients. J. Rehabil. Med. 2002, 34, 267–272. [Google Scholar] [PubMed]
- Verheyden, G.; Nieuwboer, A.; De Wit, L.; Feys, H.; Schuback, B.; Baert, I.; Jenni, W.; Schupp, W.; Thijs, V.; De Weerdt, W. Trunk performance after stroke: An eye catching predictor of functional outcome. J. Neurol. Neurosurg. Psychiatry 2007, 78, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.-L.; Sheu, C.-F.; Hsueh, I.-P.; Wang, C.-H. Trunk control as an early predictor of comprehensive activities of daily living function in stroke patients. Stroke 2002, 33, 2626–2630. [Google Scholar] [CrossRef] [PubMed]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in stroke rehabilitation: A systematic review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Dukelow, S.P.; Herter, T.M.; Moore, K.D.; Demers, M.J.; Glasgow, J.I.; Bagg, S.D.; Norman, K.E.; Scott, S.H. Quantitative assessment of limb postion sense following stroke. Neurorehabil. Neural Repair 2010, 24, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Reaz, M.B.I.; Hussain, M.S.; Mohd-Yasin, F. Techniques of EMG signal analysis: Detection, processing, classification and applications. Biol. Proced. Online 2006, 8, 11–35. [Google Scholar] [CrossRef]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- Katz-Leurer, M.; Fisher, I.; Neeb, M.; Schwartz, I.; Carmeli, E. Reliability and validity of the modified functional reach test at the sub-acute stage post-stroke. Disabil. Rehabil. 2009, 31, 243–248. [Google Scholar] [CrossRef]
- Hill, K.; Ellis, P.; Bernhardt, J.; Maggs, P.; Hull, S. Balance and mobility outcomes for stroke patients: A comprehensive audit. Aust. J. Physiother. 1997, 43, 173–180. [Google Scholar] [CrossRef]
- Frzovic, D.; Morris, M.E.; Vowels, L. Clinical tests of standing balance: Performance of persons with multiple sclerosis. Arch. Phys. Med. Rehabil. 2000, 81, 215–221. [Google Scholar] [CrossRef]
- Holbein-Jenny, M.A.; Billek-Sawhney, B.; Beckman, E.; Smith, T. Balance in personal care home residents: A comparison of the Berg Balance Scale, the Multi-Directional Reach Test, and the Activities-specific Balance Confidence Scale. J. Geriatr. Phys. Ther. 2005, 28, 48–53. [Google Scholar] [CrossRef]
- Duncan, P.W.; Studenski, S.; Chandler, J.; Prescott, B. Functional reach: Predictive validity in a sample of elderly male veterans. J. Gerontol. 1992, 47, M93–M98. [Google Scholar] [CrossRef]
- Fishman, M.N.; Colby, L.A.; Sachs, L.A.; Nichols, D.S. Comparison of upper-extremity balance tasks and force platform testing in persons with hemiparesis. Phys. Ther. 1997, 77, 1052–1062. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Daubney, M.E.; Culham, E.G. Lower-extremity muscle force and balance performance in adults aged 65 years and older. Phys. Ther. 1999, 79, 1177–1185. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Ishida, K.; Yamamoto, H.; Takata, J.; Nishinaga, M.; Doi, Y.; Yamamoto, H. Modification of the functional reach test: Analysis of lateral and anterior functional reach in community-dwelling older people. Arch. Gerontol. Geriatr. 2006, 42, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Newton, R.A. Validity of the multi-directional reach test: A practical measure for limits of stability in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M248–M252. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jaasko, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar]
- Verheyden, G.; Nieuwboer, A.; Mertin, J.; Preger, R.; Kiekens, C.; De Weerdt, W. The Trunk Impairment Scale: A new tool to measure motor impairment of the trunk after stroke. Clin. Rehabil. 2004, 18, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; Catlin, P.A.; Ellis, M.; Archer, A.L.; Morgan, B.; Piacentino, A. Assessing Wolf Motor Function Test as outcome measure for research in patients after stroke. Stroke 2001, 32, 1635–1639. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The Timed Up and Go: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Pataky, T.C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar] [CrossRef]
- Anderson, T.W.; Darling, D.A. A test of goodness of fit. J. Am. Stat. Assoc. 1954, 49, 765–769. [Google Scholar] [CrossRef]
- Sakia, R.M. The Box-Cox transformation technique: A review. J. R. Stat. Soc. Ser. D 1992, 41, 169–178. [Google Scholar] [CrossRef]
- Mauchly, J.W. Significance test for sphericity of a normal n-variate distribution. Ann. Math. Stat. 1940, 11, 204–209. [Google Scholar] [CrossRef]
- Rea, L.M.; Parker, R.A. Designing and Conducting Survey Research: A Comprehensive Guide; John Wiley & Sons: San Francisco, CA, USA, 2014; ISBN 1118767039. [Google Scholar]
- Kapandji, I.A. The Physiology of the Joints: The Spinal Column, Pelvic Girdle and Head, 6th Revised Edition; Churchill Livingstone: Edinburgh, UK, 2007; Volume 3, ISBN 0702029599. [Google Scholar]
- Rabuffetti, M.; Carpinella, I.; Ferrarin, M.; Cattaneo, D.; Bonora, G.; Nardone, A.; Bowman, T. Counteracting Postural Perturbations Through Body Weight Shift: A Pilot Study Using a Robotic Platform in Subjects With Parkinson’s Disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1794–1802. [Google Scholar] [CrossRef]
- Morris, J.M.; Lucas, D.B.; Bresler, B. Role of the trunk in stability of the spine. JBJS 1961, 43, 327–351. [Google Scholar] [CrossRef]
- Anderson, K.G.; Behm, D.G. Maintenance of EMG activity and loss of force output with instability. J. Strength Cond. Res. 2004, 18, 637–640. [Google Scholar] [PubMed]
- Phadke, V.; Camargo, P.R.; Ludewig, P.M. Scapular and rotator cuff muscle activity during arm elevation: A review of normal function and alterations with shoulder impingement. Braz. J. Phys. Ther. 2009, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, L.; Coscia, M.; Pierella, C.; Giannoni, P.; Cherif, A.; Mugnosso, M.; Marinelli, L.; Casadio, M. Effects of hemispheric stroke localization on the reorganization of arm movements within different mechanical environments. Life 2021, 11, 383. [Google Scholar] [CrossRef]
- Sakamoto, K.; Nakamura, T.; Uenishi, H.; Umemoto, Y.; Arakawa, H.; Abo, M.; Saura, R.; Fujiwara, H.; Kubo, T.; Tajima, F. Immediate effects of unaffected arm exercise in poststroke patients with spastic upper limb hemiparesis. Cerebrovasc. Dis. 2014, 37, 123–127. [Google Scholar] [CrossRef]
- Pandian, S.; Arya, K.N.; Kumar, D. Effect of motor training involving the less-affected side (MTLA) in post-stroke subjects: A pilot randomized controlled trial. Top. Stroke Rehabil. 2015, 22, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Pandian, S.; Arya, K.N.; Kumar, D. Does motor training of the nonparetic side influences balance and function in chronic stroke? A pilot RCT. Sci. World J. 2014, 2014, 769726. [Google Scholar] [CrossRef] [PubMed]
- Cernacek, J. Contralateral motor irradiation-cerebral dominance: Its changes in hemiparesis. Arch. Neurol. 1961, 4, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Ehrensberger, M.; Simpson, D.; Broderick, P.; Monaghan, K. Cross-education of strength has a positive impact on post-stroke rehabilitation: A systematic literature review. Top. Stroke Rehabil. 2016, 23, 126–135. [Google Scholar] [CrossRef] [PubMed]
- van der Krogt, H.; Kouwijzer, I.; Klomp, A.; Meskers, C.G.M.; Arendzen, J.H.; de Groot, J.H. Loss of selective wrist muscle activation in post-stroke patients. Disabil. Rehabil. 2020, 42, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Billek-Sawhney, B.; Gay, J. The Functional Reach Test: Are 3 trials necessary? Top. Geriatr. Rehabil. 2005, 21, 144–148. [Google Scholar] [CrossRef]
- Bennie, S.; Bruner, K.; Dizon, A.; Fritz, H.; Goodman, B.; Peterson, S. Measurements of balance: Comparison of the Timed” Up and Go” test and Functional Reach test with the Berg Balance Scale. J. Phys. Ther. Sci. 2003, 15, 93–97. [Google Scholar] [CrossRef]
- Portnoy, S.; Reif, S.; Mendelboim, T.; Rand, D. Postural control of individuals with chronic stroke compared to healthy participants: Timed-Up-and-Go, Functional Reach Test and center of pressure movement. Eur. J. Phys. Rehabil. Med. 2017, 53, 685–693. [Google Scholar] [CrossRef]
- Monticone, M.; Ambrosini, E.; Verheyden, G.; Brivio, F.; Brunati, R.; Longoni, L.; Mauri, G.; Molteni, A.; Nava, C.; Rocca, B. Development of the Italian version of the trunk impairment scale in subjects with acute and chronic stroke. Cross-cultural adaptation, reliability, validity and responsiveness. Disabil. Rehabil. 2019, 41, 66–73. [Google Scholar] [CrossRef]
- Hwang, W.-J.; Kim, J.-H.; Jeon, S.-H.; Chung, Y. Maximal lateral reaching distance on the affected side using the multi-directional reach test in persons with stroke. J. Phys. Ther. Sci. 2015, 27, 2713–2715. [Google Scholar] [CrossRef] [PubMed]
- Verheyden, G.; Vereeck, L.; Truijen, S.; Troch, M.; Herregodts, I.; Lafosse, C.; Nieuwboer, A.; De Weerdt, W. Trunk performance after stroke and the relationship with balance, gait and functional ability. Clin. Rehabil. 2006, 20, 451–458. [Google Scholar] [CrossRef]
- Mier, C.M. Accuracy and feasibility of video analysis for assessing hamstring flexibility and validity of the sit-and-reach test. Res. Q. Exerc. Sport 2011, 82, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, Y.; Tran, D.T.; Yamazoe, H.; Lee, J.-H. Recent use of deep learning techniques in clinical applications based on gait: A survey. J. Comput. Des. Eng. 2021, 8, 1499–1532. [Google Scholar] [CrossRef]
- Capecci, M.; Ceravolo, M.G.; Ferracuti, F.; Grugnetti, M.; Iarlori, S.; Longhi, S.; Romeo, L.; Verdini, F. An instrumental approach for monitoring physical exercises in a visual markerless scenario: A proof of concept. J. Biomech. 2018, 69, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Kanko, R.M.; Laende, E.K.; Davis, E.M.; Selbie, W.S.; Deluzio, K.J. Concurrent assessment of gait kinematics using marker-based and markerless motion capture. J. Biomech. 2021, 127, 110665. [Google Scholar] [CrossRef]
- Moro, M.; Marchesi, G.; Odone, F.; Casadio, M. Markerless gait analysis in stroke survivors based on computer vision and deep learning: A pilot study. In Proceedings of the Proceedings of the 35th Annual ACM Symposium on Applied Computing, Brno, Czech Republic, 30 March–3 April 2020; Association for Computing Machinery: New York, NY, USA, 2020; pp. 2097–2104. [Google Scholar]
- Handelzalts, S.; Ballardini, G.; Avraham, C.; Pagano, M.; Casadio, M.; Nisky, I. Integrating Tactile Feedback Technologies into Home-Based Telerehabilitation: Opportunities and Challenges in Light of COVID-19 Pandemic. Front. Neurorobot. 2021, 15, 4. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (ys) | Gender | TSS (ys) | Etiology | PS | FMA-AD (0–66) | FMA-H (0–12) | TIS (0–23) | WMFT (0–85) | TUG (s) | |
|---|---|---|---|---|---|---|---|---|---|---|
| ID01 | 66 | F | 11 | I | R | 39 | 12 | 13 | 49 | 15.3 |
| ID02 | 48 | F | 6 | H | L | 23 | 10 | 14 | 32 | 11.3 |
| ID03 | 65 | F | 2 | H | R | 14 | 12 | 19 | 9 | 15.5 |
| ID04 | 52 | F | 5 | I | R | 37 | 0 | 16 | 44 | 15.4 |
| ID05 | 68 | M | 16 | I | R | 55 | 12 | 11 | 75 | 9.4 |
| ID06 | 68 | M | 1.5 | H | R | 33 | 12 | 12 | 57 | 16.7 |
| ID07 | 60 | F | 8 | I | R | 9 | 10 | 12 | 14 | 18.5 |
| ID08 | 62 | F | 4 | I | L | 56 | 11 | 16 | 78 | 36.2 |
| ID09 | 60 | M | 4 | I | R | 57 | 9 | 17 | 78 | 10.9 |
| ID10 | 69 | M | 4 | I | L | 50 | 12 | 16 | 74 | 13.3 |
| ID11 | 68 | F | 1 | I | L | 14 | 12 | 16 | 14 | 35.7 |
| ID12 | 70 | F | 7 | I | R | 44 | 3 | 12 | 62 | 26.8 |
| ID13 | 78 | M | 1 | I | L | 52 | 12 | 13 | 73 | 9.5 |
| ID14 | 72 | M | 12 | I | R | 11 | 3 | 13 | 1 | 25.3 |
| ID15 | 60 | M | 10 | I | R | 14 | 3 | 14 | 30 | 19.2 |
| All * | ||||||||||
| 64.4 ± 7.4 | 8 F 7 M | 6.2 ± 4.3 | 12 I 3 H | 10 R 5L | 33.9 ± 17.6 | 8.9 ± 4.2 | 14.2 ± 2.2 | 46.0 ± 26.7 | 18.60 ± 8.39 |
| Parameters | T1 | T2 | T3 |
|---|---|---|---|
| Normalized reaching distance ** | 0.58 ± 0.03 | 0.63 ± 0.03 | 0.67 ± 0.03 |
| Movement time (s) | 5.66 ± 0.49 | 5.17 ± 0.43 | 5.20 ± 0.44 |
| Δpelvis (cm) | 1.01 ± 0.10 | 1.02 ± 0.10 | 1.11 ± 0.12 |
| Parameters | T1 | T2 | T3 |
|---|---|---|---|
| Normalized reaching distance | 0.29 ± 0.02 | 0.34 ± 0.02 | 0.36 ± 0.03 |
| Movement time (s) | 4.81 ± 0.33 | 4.82 ± 0.33 | 5.06 ± 0.42 |
| Δpelvis (cm) * | 1.47 ± 0.30 | 2.89 ± 0.62 | 2.70 ± 0.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchesi, G.; Ballardini, G.; Barone, L.; Giannoni, P.; Lentino, C.; De Luca, A.; Casadio, M. Modified Functional Reach Test: Upper-Body Kinematics and Muscular Activity in Chronic Stroke Survivors. Sensors 2022, 22, 230. https://doi.org/10.3390/s22010230
Marchesi G, Ballardini G, Barone L, Giannoni P, Lentino C, De Luca A, Casadio M. Modified Functional Reach Test: Upper-Body Kinematics and Muscular Activity in Chronic Stroke Survivors. Sensors. 2022; 22(1):230. https://doi.org/10.3390/s22010230
Chicago/Turabian StyleMarchesi, Giorgia, Giulia Ballardini, Laura Barone, Psiche Giannoni, Carmelo Lentino, Alice De Luca, and Maura Casadio. 2022. "Modified Functional Reach Test: Upper-Body Kinematics and Muscular Activity in Chronic Stroke Survivors" Sensors 22, no. 1: 230. https://doi.org/10.3390/s22010230
APA StyleMarchesi, G., Ballardini, G., Barone, L., Giannoni, P., Lentino, C., De Luca, A., & Casadio, M. (2022). Modified Functional Reach Test: Upper-Body Kinematics and Muscular Activity in Chronic Stroke Survivors. Sensors, 22(1), 230. https://doi.org/10.3390/s22010230