
A Real-Time Wearable Physiological Monitoring System for Home-Based Healthcare Applications



Abstract
:1. Introduction
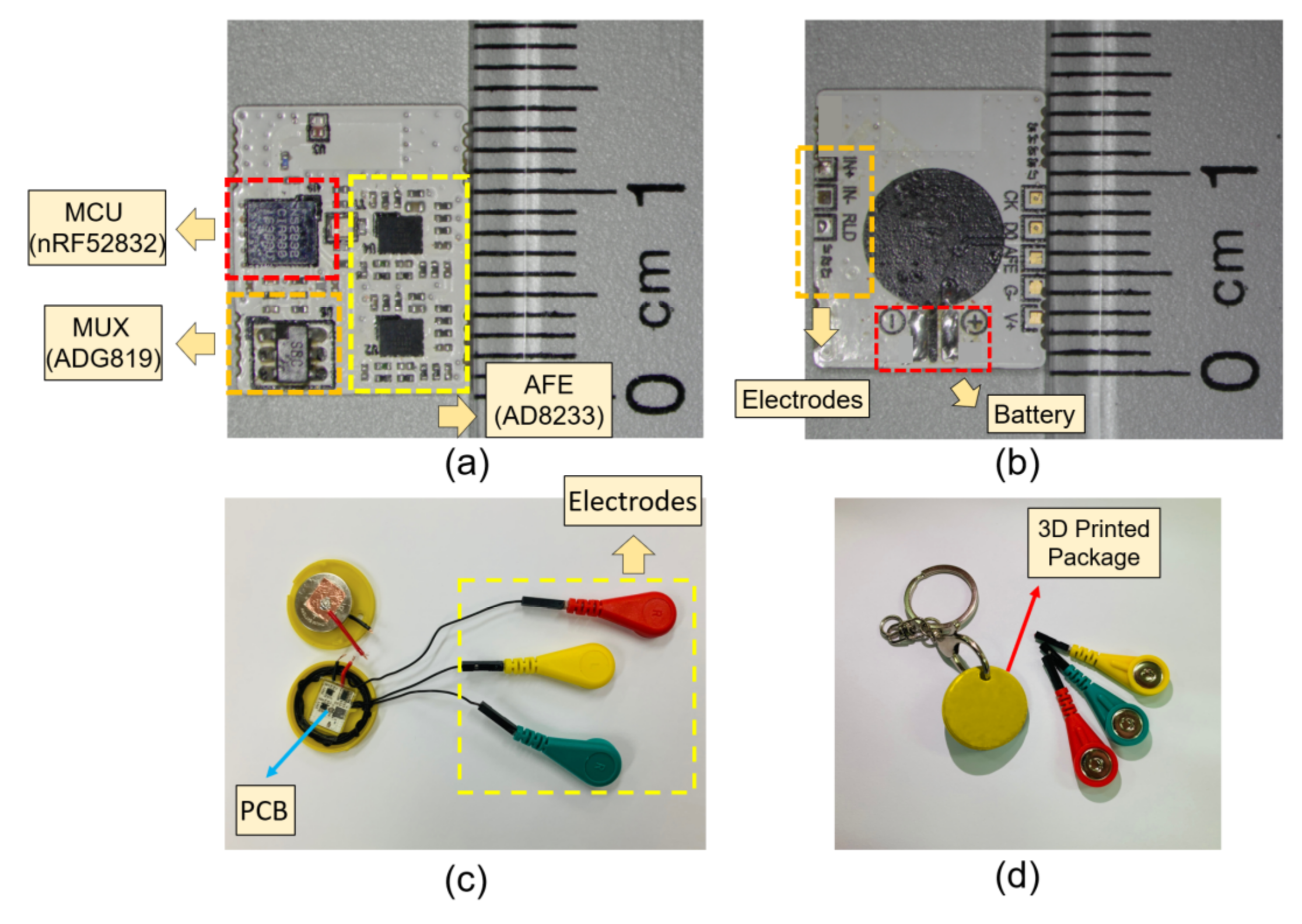
- The proposed surface bio-potential acquisition system is compactly devised for an everyday wearable application with supporting long-term stability validation. The total area of the monitoring device is just about the size of a button-shape battery (CR2032). The overall system implementation is cost effective compared to existing systems with a dedicated host device.
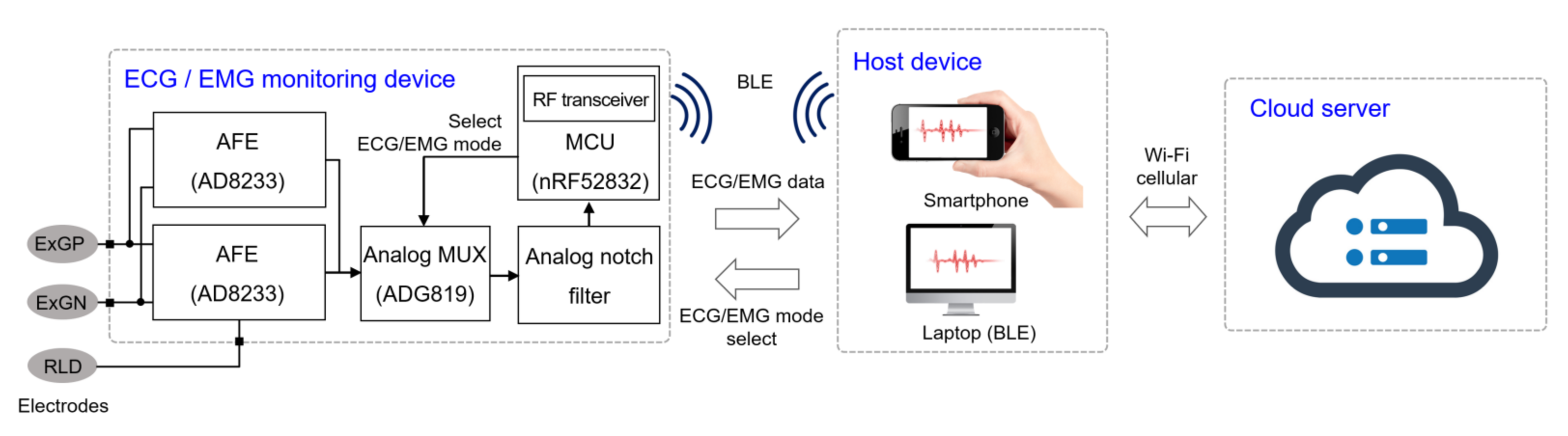
- A host node manages the role of the monitoring device and displays the signals in a real-time plot. Furthermore, a healthcare network is established between the host node and a cloud server where an intelligent analysis is performed, and remote clinical support can be provided by the physicians.
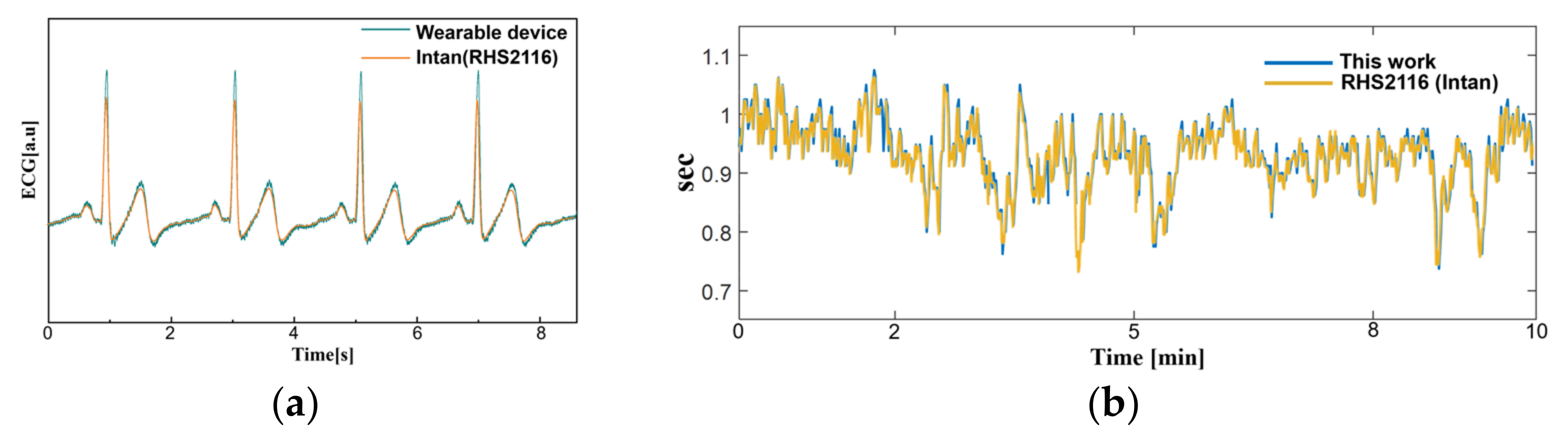
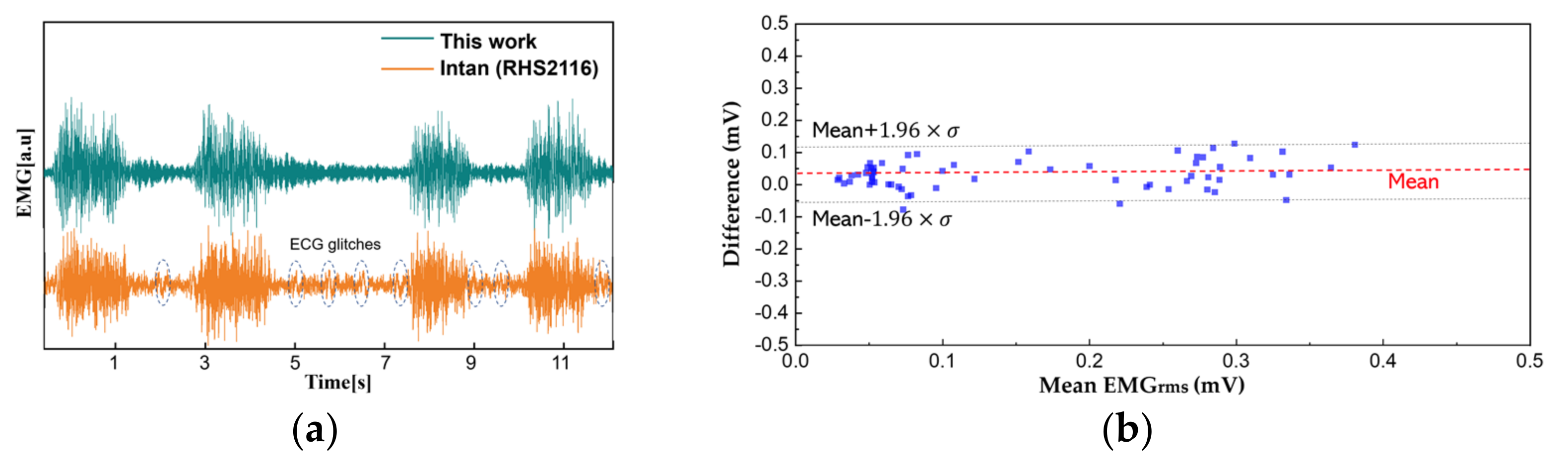
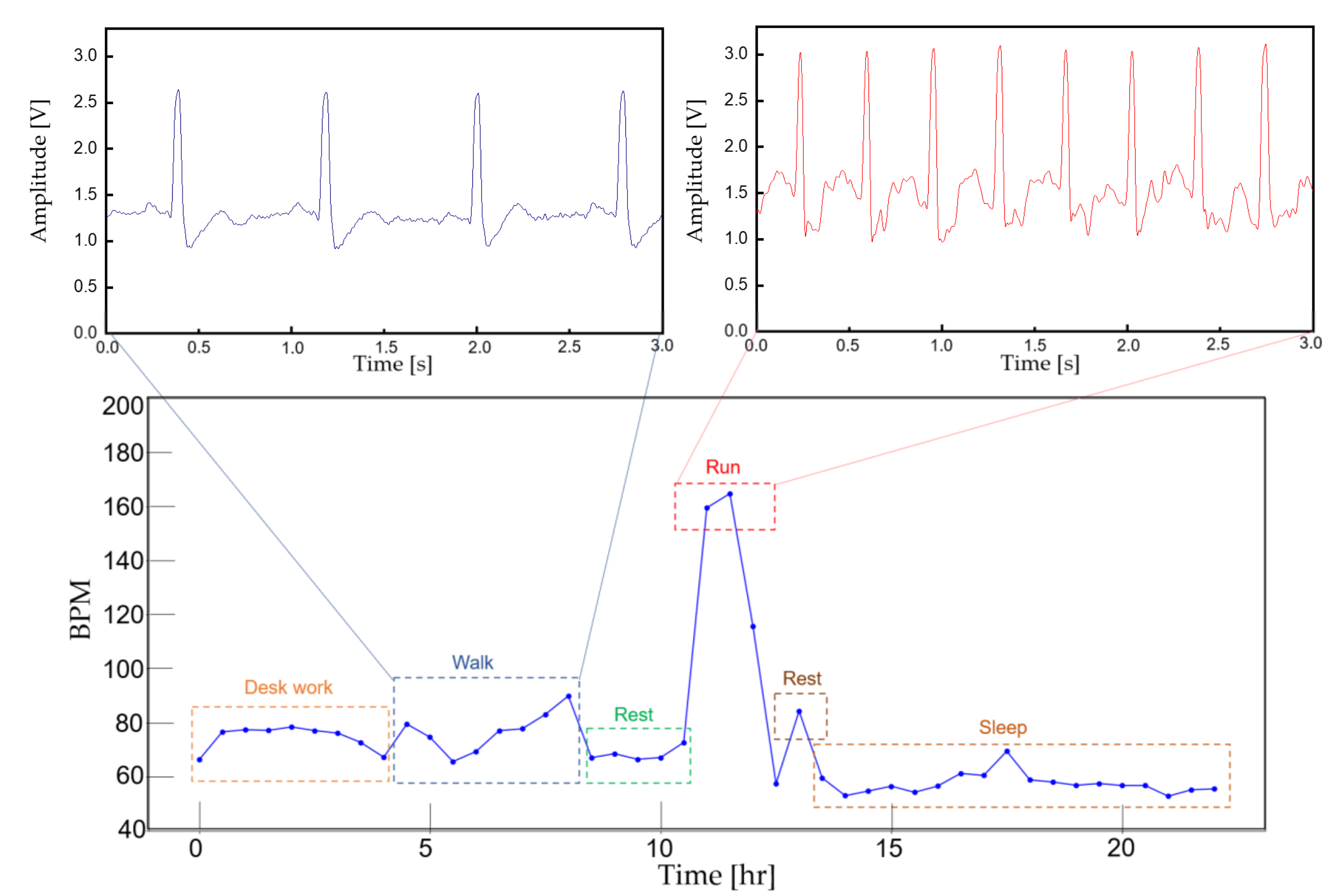
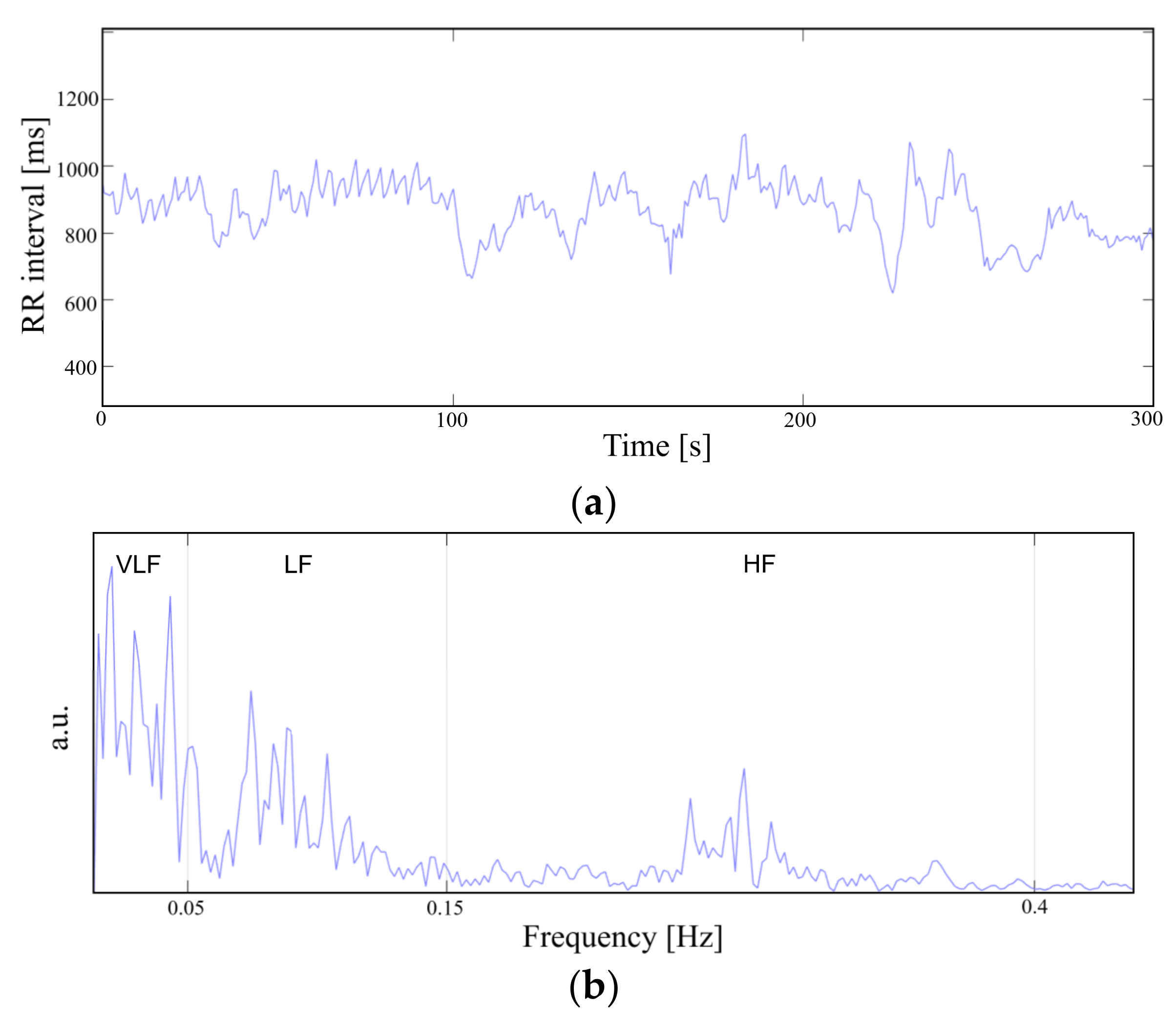
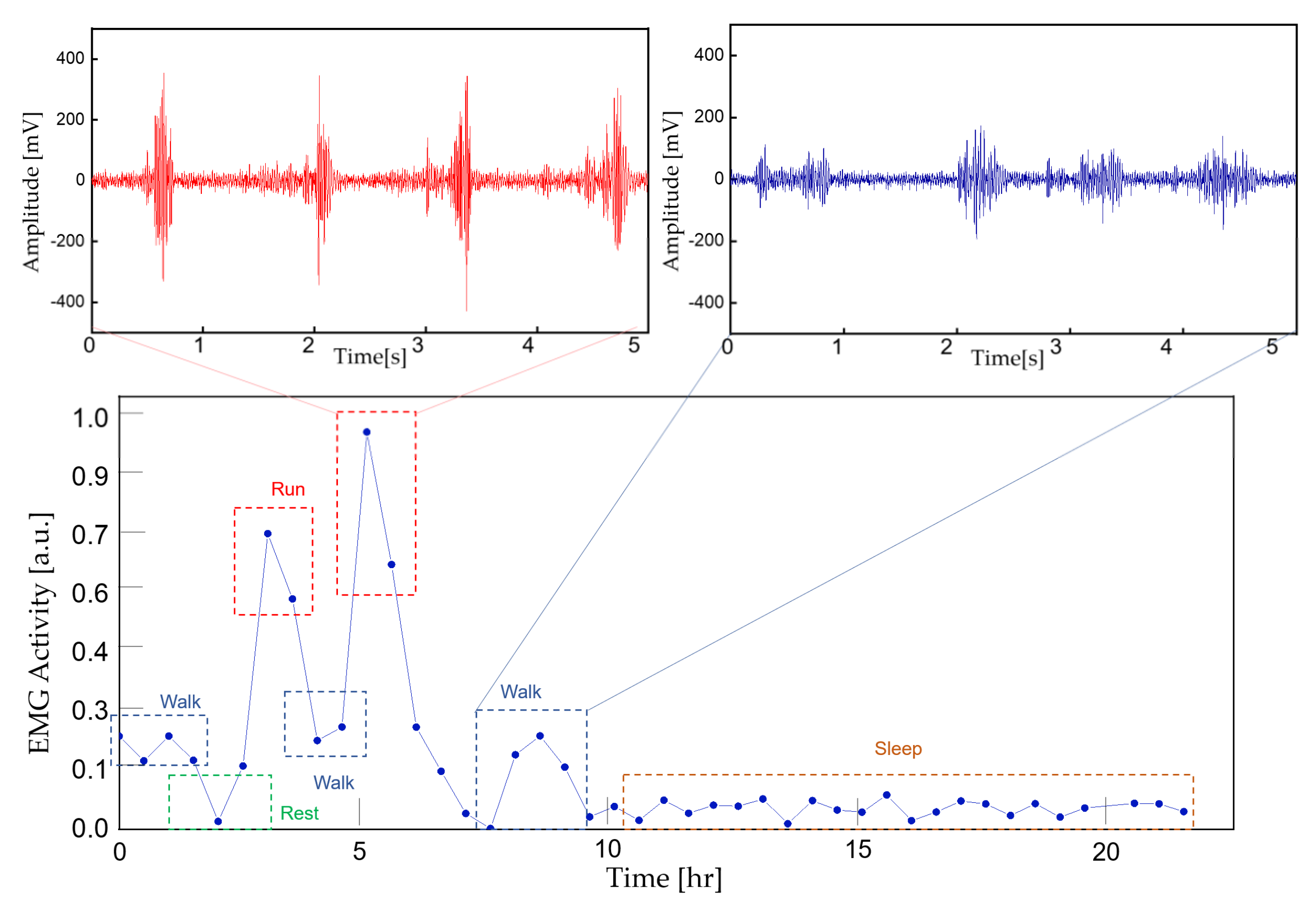
- A short-term physiological signal acquisition session with a reference instrument and series of analyses concludes that the signal quality of this work is precise. A practical long-term ECG and EMG acquisition session verifies the feasibility and wearability of the proposed device under a regular daily activity, including aggressive exercise.
2. Design of the Proposed System
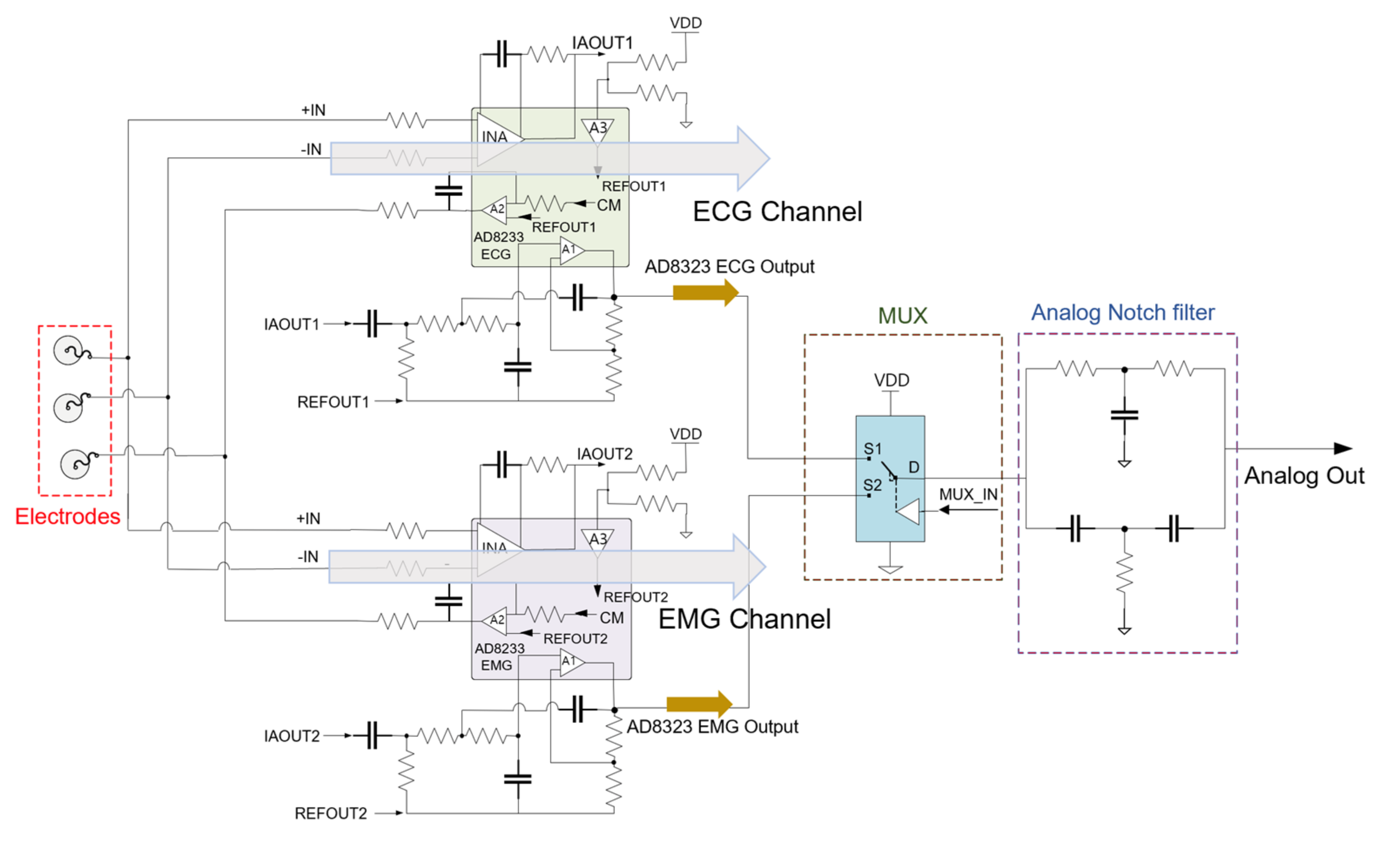
2.1. Monitoring Device Design and Fabrication
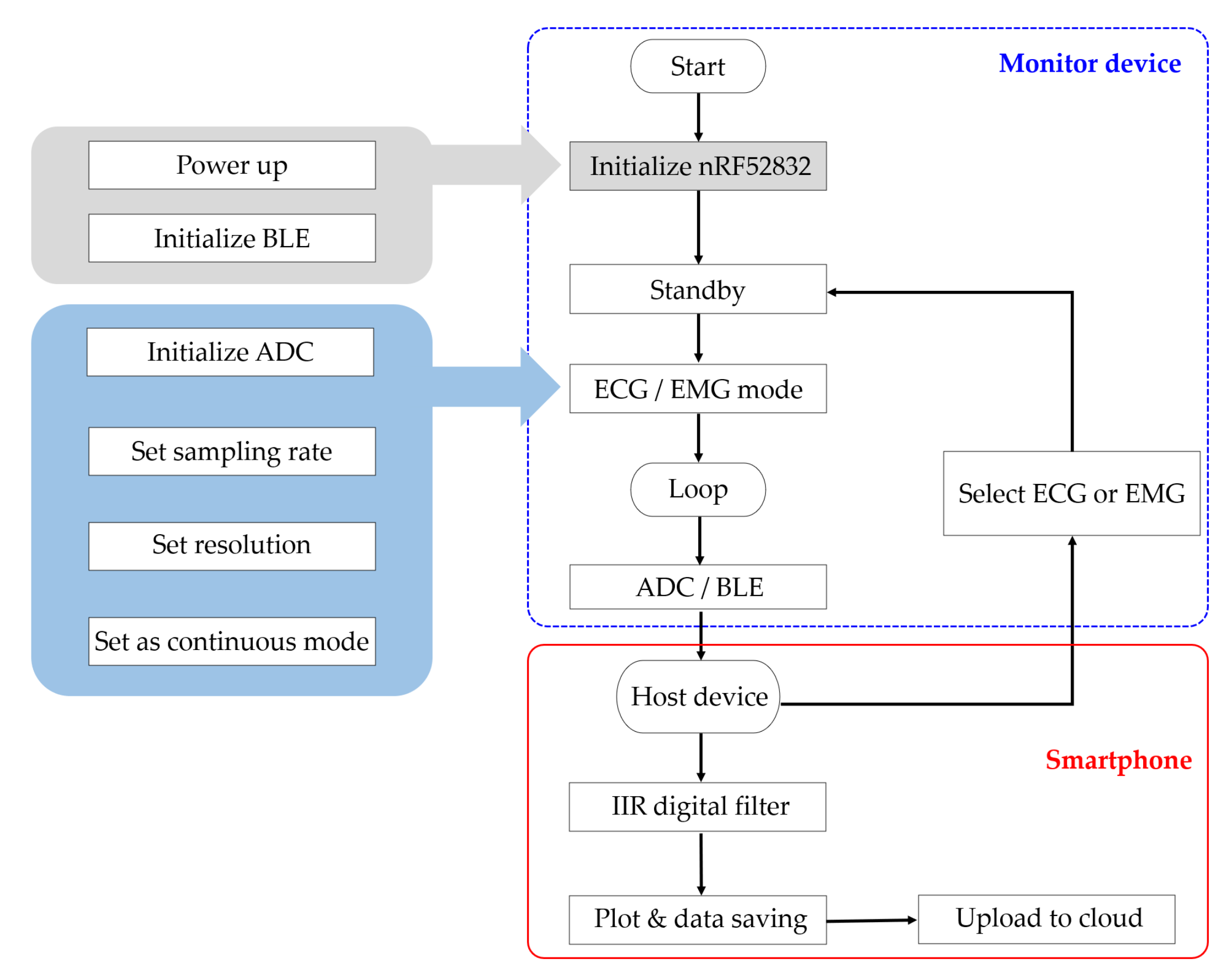
2.2. Host Node Software Implementation
2.3. Data Analysis on Remote Server
3. Experimental Results
3.1. Continuous ECG and EMG Monitoring
3.2. Accuracy of the Acquired Signal
3.3. Long-Term Monitoring and Data Analysis
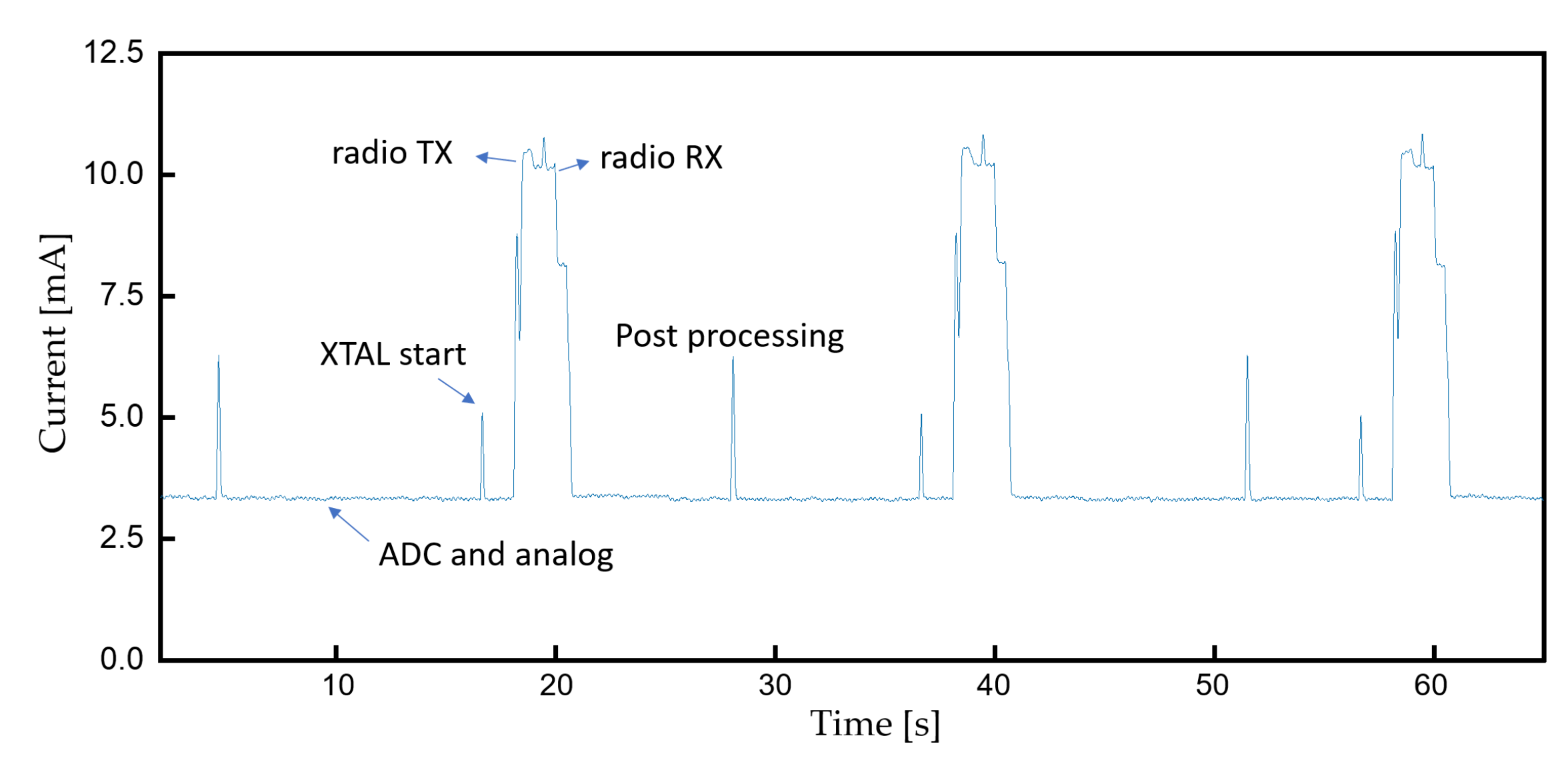
3.4. Device Lifetime
4. Conclusions
5. Discussion and Future Work
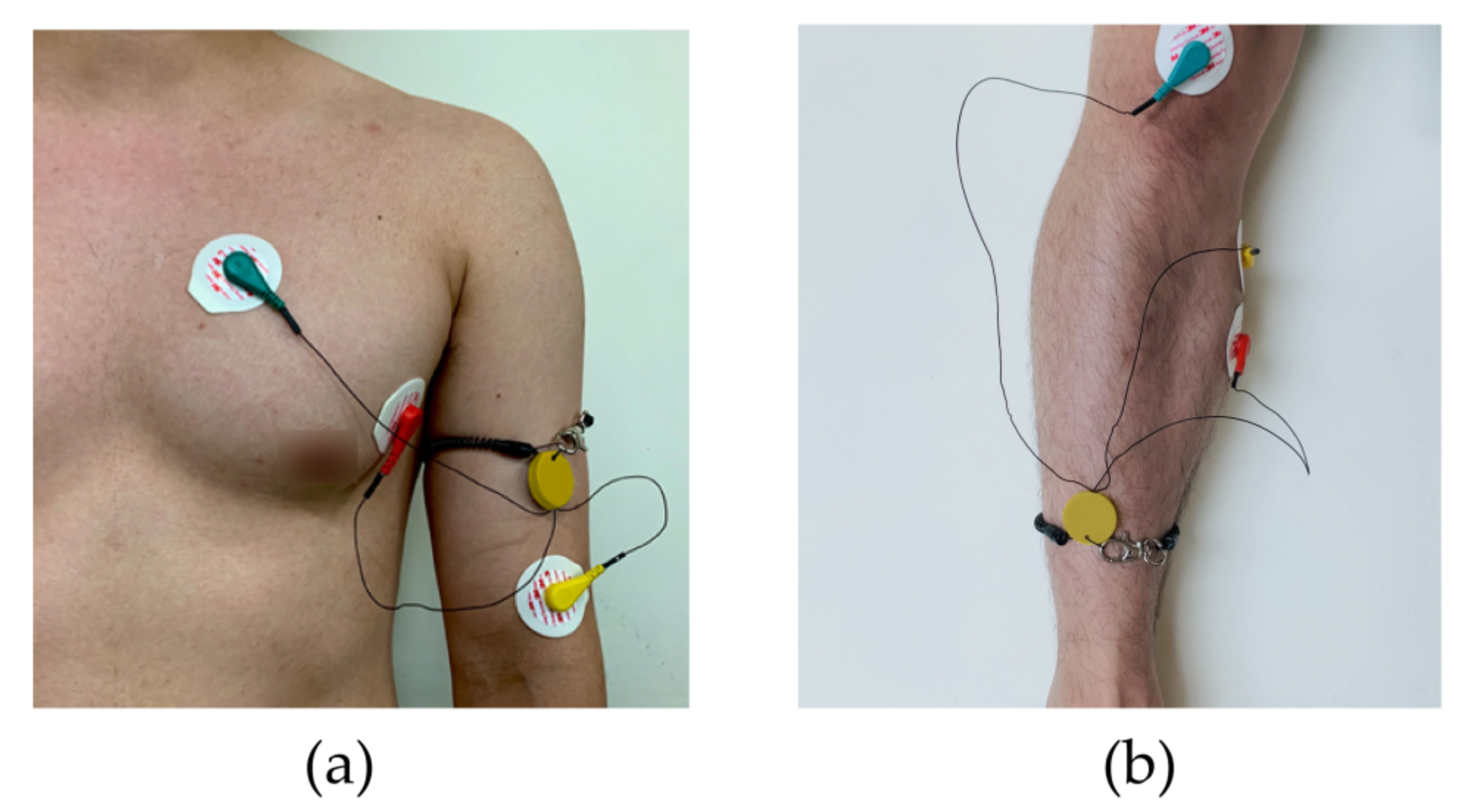
- The current monitoring device has a ring hole and an adjustable band that the patient can tie onto their limb or neck. Although the rigid structure offers protection for the monitoring device, it can sometimes be uncomfortable to the patient. A flexible patch-type miniature monitoring device that be attached to the skin could be a solution.
- Feature extraction in the host device (smartphone) is necessary since it can sometimes be very difficult to spot a past event and the file size can be large in a prolonged recording session.
- Without a classification algorithm based on machine learning that can alert the patient or the physician, abnormal activity can easily go undetected unless a specialist monitors the data all the time. Hence, there is a need to integrate the current system with an algorithm that can effectively detect specific features, make accurate predictions, and alarm the patient or the physician [25,26].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; Howard, V.J. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Raedt, S.; De Vos, A.; De Keyser, J. Autonomic dysfunction in acute ischemic stroke: An underexplored therapeutic area? J. Neurol. Sci. 2015, 348, 24–34. [Google Scholar] [CrossRef]
- Steinhubl, S.R.; Waalen, J.; Edwards, A.M.; Ariniello, L.M.; Mehta, R.R.; Ebner, G.S.; Carter, C.; Baca-Motes, K.; Felicione, E.; Sarich, T. Effect of a home-based wearable continuous ECG monitoring patch on detection of undiagnosed atrial fibrillation: The mSToPS randomized clinical trial. JAMA 2018, 320, 146–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobkin, B.H.; Dorsch, A. New evidence for therapies in stroke rehabilitation. Curr. Atheroscler. Rep. 2013, 15, 331. [Google Scholar] [CrossRef]
- Hong, S.; Kim, D.; Park, H.; Seo, Y.; Hussain, I.; Park, S.J. Gait Feature Vectors for Post-stroke Prediction using Wearable Sensor. Sci. Emot. Sensib. 2019, 22, 55–64. [Google Scholar] [CrossRef]
- Sawacha, Z.; Spolaor, F.; Piątkowska, W.J.; Cibin, F.; Ciniglio, A.; Guiotto, A.; Ricca, M.; Polli, R.; Murgia, A. Feasibility and Reliability Assessment of Video-Based Motion Analysis and Surface Electromyography in Children with Fragile X during Gait. Sensors 2021, 21, 4746. [Google Scholar] [CrossRef] [PubMed]
- Dimyan, M.A.; Cohen, L.G.J.N.R.N. Neuroplasticity in the context of motor rehabilitation after stroke. Nat. Rev. Neurol. 2011, 7, 76–85. [Google Scholar] [CrossRef]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Qian, Q.; Hu, X.; Lai, Q.; Ng, S.C.; Zheng, Y.; Poon, W. Early stroke rehabilitation of the upper limb assisted with an electromyography-driven neuromuscular electrical stimulation-robotic arm. Front. Neurol. 2017, 8, 447. [Google Scholar] [CrossRef] [PubMed]
- Marin-Pardo, O.; Laine, C.M.; Rennie, M.; Ito, K.L.; Finley, J.; Liew, S.-L. A Virtual Reality Muscle–Computer Interface for Neurorehabilitation in Chronic Stroke: A Pilot Study. Sensors 2020, 20, 3754. [Google Scholar] [CrossRef]
- Hu, X.L.; Tong, K.Y.; Wei, X.J.; Rong, W.; Susanto, E.A.; Ho, S.K. The effects of post-stroke upper-limb training with an electromyography (EMG)-driven hand robot. J. Electromyogr. Kinesiol. 2013, 23, 1065–1074. [Google Scholar] [CrossRef]
- Jabaudon, D.; Sztajzel, J.; Sievert, K.; Landis, T.; Sztajzel, R. Usefulness of ambulatory 7-day ECG monitoring for the detection of atrial fibrillation and flutter after acute stroke and transient ischemic attack. Stroke 2004, 35, 1647–1651. [Google Scholar] [CrossRef] [Green Version]
- Murphy, T.H.; Corbett, D. Plasticity during stroke recovery: From synapse to behaviour. Nat. Rev. Neurosci. 2009, 10, 861–872. [Google Scholar] [CrossRef]
- Zeiler, S.R.; Krakauer, J.W. The interaction between training and plasticity in the post-stroke brain. Curr. Opin. Neurol. 2013, 26, 609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, H.; Naing, H.H.; Yaqub, R. An IoT assisted real-time high CMRR wireless ambulatory ECG monitoring system with arrhythmia detection. Electronics 2021, 10, 1871. [Google Scholar] [CrossRef]
- Chen, Q.; Kastratovic, S.; Eid, M.; Ha, S. A Non-Contact Compact Portable ECG Monitoring System. Electronics 2021, 10, 2279. [Google Scholar] [CrossRef]
- Zhu, L.; Mao, G.; Su, H.; Zhou, Z.; Li, W.; Lu, X.; Wang, Z. A Wearable, High-Resolution, and Wireless System for Multichannel Surface Electromyography Detection. IEEE Sens. J. 2021, 21, 9937–9948. [Google Scholar] [CrossRef]
- Spanò, E.; Di Pascoli, S.; Iannaccone, G. Low-power wearable ECG monitoring system for multiple-patient remote monitoring. IEEE Sens. J. 2016, 16, 5452–5462. [Google Scholar] [CrossRef]
- Satti, A.T.; Park, J.; Park, J.; Kim, H.; Cho, S. Fabrication of Parylene-Coated Microneedle Array Electrode for Wearable ECG Device. Sensors 2020, 20, 5183. [Google Scholar] [CrossRef] [PubMed]
- Satti, A.T.; Kim, J.; Yi, E.; Cho, H.-y.; Cho, S. Microneedle Array Electrode-Based Wearable EMG System for Detection of Driver Drowsiness through Steering Wheel Grip. Sensors 2021, 21, 5091. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Park, C.-K.; Kim, K.G. An EMG-based variable impedance control for elbow exercise: Preliminary study. Adv. Robot. 2017, 31, 809–820. [Google Scholar] [CrossRef]
- Bravo-Zanoguera, M.; Cuevas-González, D.; Reyna, M.A.; García-Vázquez, J.P.; Avitia, R.L. Fabricating a Portable ECG Device Using AD823X Analog Front-End Microchips and Open-Source Development Validation. Sensors 2020, 20, 5962. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, C.; Philippon, F.; Sanchez, M.; Fortier-Poisson, P.; O’Hara, G.; Molin, F.; Sarrazin, J.-F.; Nault, I.; Blier, L.; Roy, K. A novel wearable device for continuous ambulatory ECG recording: Proof of concept and assessment of signal quality. Biosensors 2019, 9, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masihi, S.; Panahi, M.; Maddipatla, D.; Hanson, A.J.; Fenech, S.; Bonek, L.; Sapoznik, N.; Fleming, P.D.; Bazuin, B.J.; Atashbar, M.Z. Development of a Flexible Wireless ECG Monitoring Device with Dry Fabric Electrodes for Wearable Applications. IEEE Sens. J. 2021. ahead of print. [Google Scholar] [CrossRef]
- Ali, F.; El-Sappagh, S.; Islam, S.M.R.; Ali, A.; Attique, M.; Imran, M.; Kwak, K.-S. An intelligent healthcare monitoring framework using wearable sensors and social networking data. Future Gener. Comput. Syst. 2021, 114, 23–43. [Google Scholar] [CrossRef]
- Ali, F.; El-Sappagh, S.; Islam, S.M.R.; Kwak, D.; Ali, A.; Imran, M.; Kwak, K.-S. A smart healthcare monitoring system for heart disease prediction based on ensemble deep learning and feature fusion. Inf. Fusion 2020, 63, 208–222. [Google Scholar] [CrossRef]
- Lakhan, A.; Dootio, M.A.; Alqahtani, F.; Alzahrani, R.I.; Baothman, F.; Shah, S.Y.; Shah, S.A.; Anjum, N.; Abbasi, Q.H.; Khokhar, M.S. Hybrid workload enabled and secure healthcare monitoring sensing framework in distributed fog-cloud network. Electronics 2021, 10, 1974. [Google Scholar] [CrossRef]
- Piskorowski, J. Digital Q-varying notch IIR filter with transient suppression. IEEE Trans. Instrum. Meas. 2009, 59, 866–872. [Google Scholar] [CrossRef]
- Levkov, C.; Mihov, G.; Ivanov, R.; Daskalov, I.; Christov, I.; Dotsinsky, I. Removal of power-line interference from the ECG: A review of the subtraction procedure. BioMed. Eng. Online 2005, 4, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Pei, S.-C.; Tseng, C.-C. Elimination of AC interference in electrocardiogram using IIR notch filter with transient suppression. IEEE Trans. Biomed. Eng. 1995, 42, 1128–1132. [Google Scholar]
- Li, J.; Deng, G.; Wei, W.; Wang, H.; Ming, Z. Design of a real-time ECG filter for portable mobile medical systems. IEEE Access 2016, 5, 696–704. [Google Scholar] [CrossRef]
- Parente, F.R.; Santonico, M.; Zompanti, A.; Benassai, M.; Ferri, G.; D’Amico, A.; Pennazza, G. An electronic system for the contactless reading of ECG signals. Sensors 2017, 17, 2474. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symbol | Parameter | Value |
|---|---|---|
| Sampling Frequency | Sample per second | 104 |
| A/D Resolution | Bit | 8~12 (this work: 8) |
| VDD | V | 1.8~3.3 |
| Bandwidth (ECG) | Hz | 0.34~41 |
| Bandwidth (EMG) | Hz | 40.17~727 |
| Gain | V/V | 1100 |
| Communication Type | - | BLE |
| PCB Dimension | mm3 | 15 × 10 × 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, J.-W.; Lee, W.; Kim, Y.-J. A Real-Time Wearable Physiological Monitoring System for Home-Based Healthcare Applications. Sensors 2022, 22, 104. https://doi.org/10.3390/s22010104
Jeong J-W, Lee W, Kim Y-J. A Real-Time Wearable Physiological Monitoring System for Home-Based Healthcare Applications. Sensors. 2022; 22(1):104. https://doi.org/10.3390/s22010104
Chicago/Turabian StyleJeong, Jin-Woo, Woochan Lee, and Young-Joon Kim. 2022. "A Real-Time Wearable Physiological Monitoring System for Home-Based Healthcare Applications" Sensors 22, no. 1: 104. https://doi.org/10.3390/s22010104
APA StyleJeong, J.-W., Lee, W., & Kim, Y.-J. (2022). A Real-Time Wearable Physiological Monitoring System for Home-Based Healthcare Applications. Sensors, 22(1), 104. https://doi.org/10.3390/s22010104