
Diagnosis of Alzheimer’s Disease with Ensemble Learning Classifier and 3D Convolutional Neural Network

Abstract
:1. Introduction
- 1
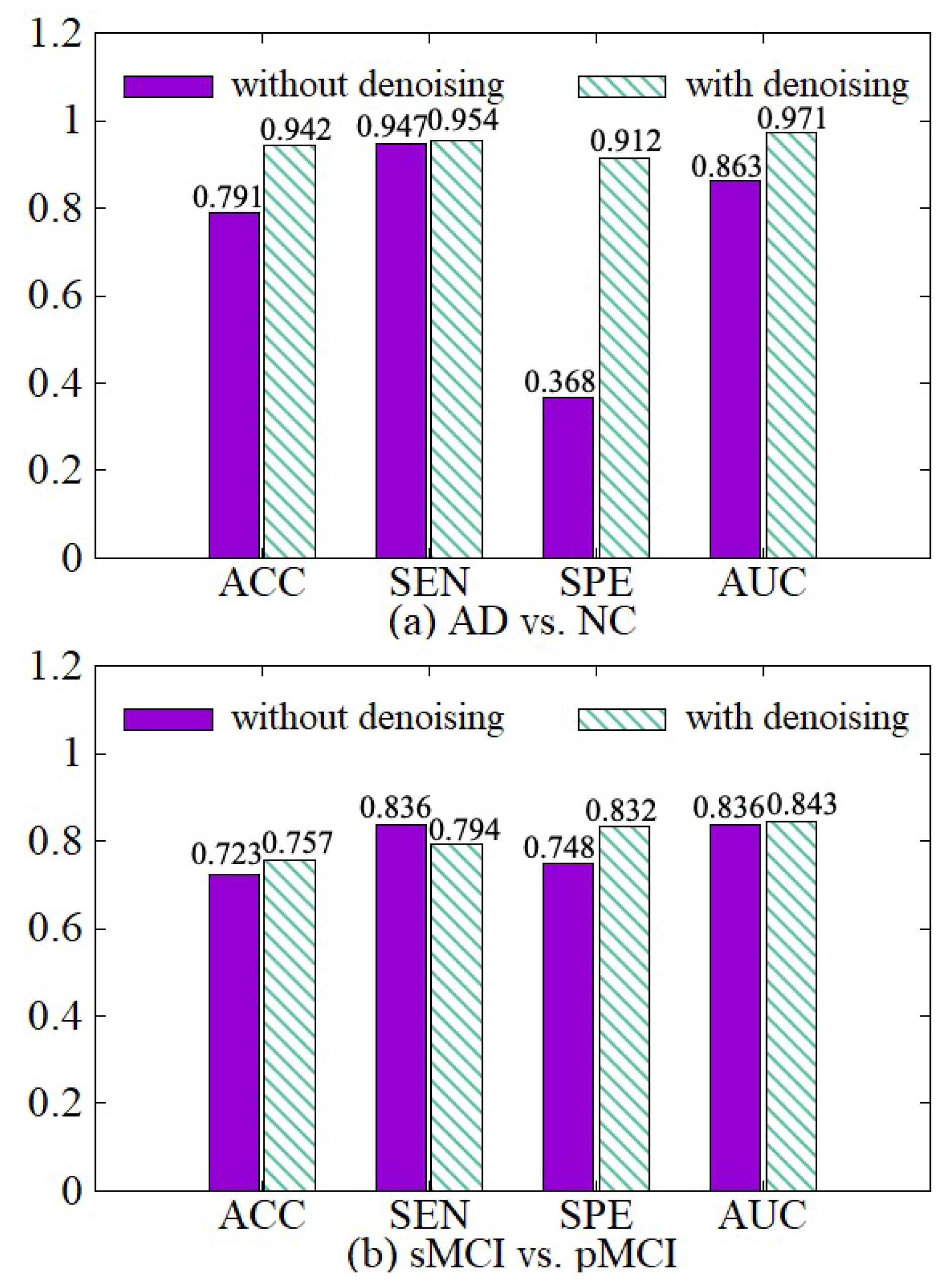
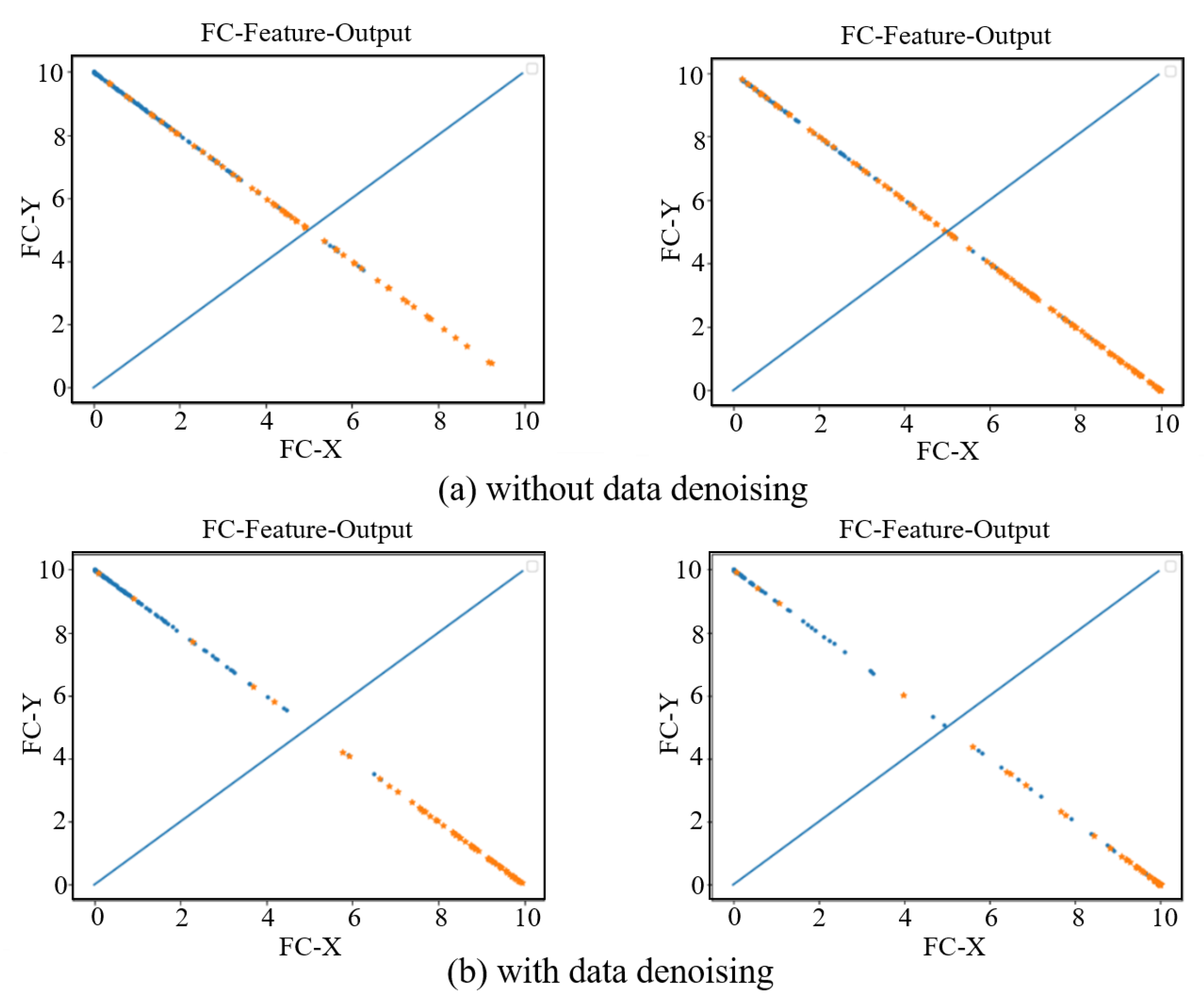
- To process the noise regions to increase training speed while improving diagnostic accuracy, we propose a data denoising method that reduces the noises at the boundaries of the 3D MRI images through the designed clipping algorithm. By analyzing the differences between the images of different label groups, the difference image is obtained, and the image boundary is cropped according to the normalized mask threshold to reduce noises. The data denoising method can remove about 47% of useless information from the data for AD diagnosis, which not only speeds up the training process but also improves the accuracy of diagnosis.
- 2
- Considering the limitation of a single classifier, the problem of hard sample learning and the issue of insufficient sample utilization, we propose a diagnosis network with multiple classifiers and serialization learning, where samples are repeatedly used in various classifiers with different weights according to their prediction errors in the previous classifier. Hard samples are assigned larger weights due to their larger prediction errors so that we can focus on them. The diagnosis network is trained based on the ensemble learning method with an improved loss function and adaptive fusion.
- 3
- The experimental results demonstrate that our proposed method outperforms the state-of-the-art methods regarding both accuracy and efficiency. Specifically, our proposed method has achieved a high accuracy 95.2% (AD vs. NC) and 77.8% (sMCI vs. pMCI).
2. Related Work
3. Our Diagnosis Model
3.1. Model Architecture
3.2. Data Denoising Module
| Algorithm 1: Data denoising process |
| Input: AD-Image group , NC-Image group , the threshold Output: The set R of the positions where the voxel values will be preserved in denoising |
|
3.3. Diagnosis Network Module
3.3.1. The Structure of Diagnosis Network
3.3.2. The Training of the Diagnosis Network
3.3.3. Loss Function
3.4. Fusion Diagnosis
4. Experiments
4.1. Dataset
4.2. Experiment Setting
4.2.1. Implement Details
4.2.2. Performance Evaluation
4.3. Experimental Results
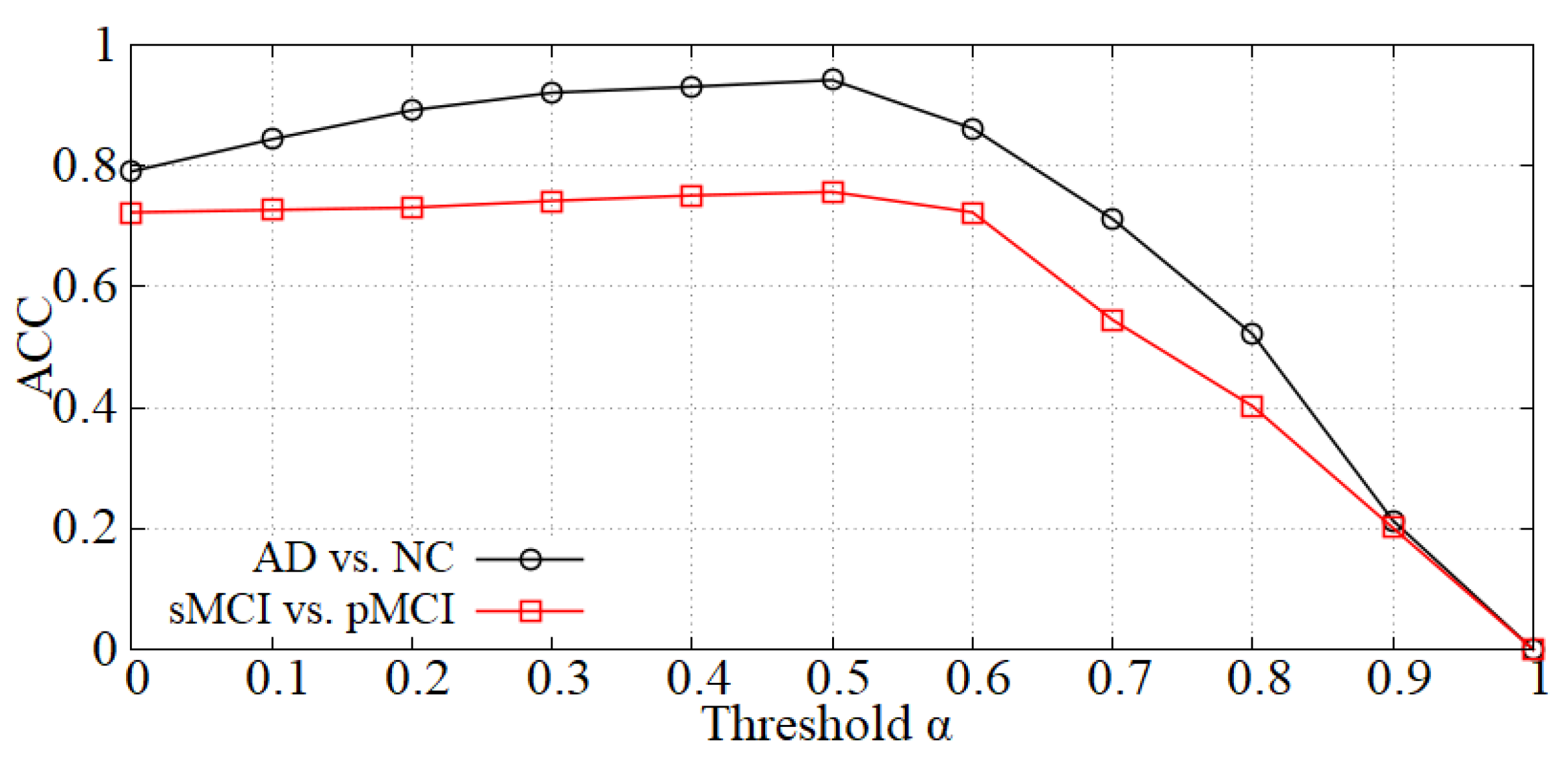
4.3.1. Parameter Analysis
4.3.2. Effectiveness of Data Denoising Module
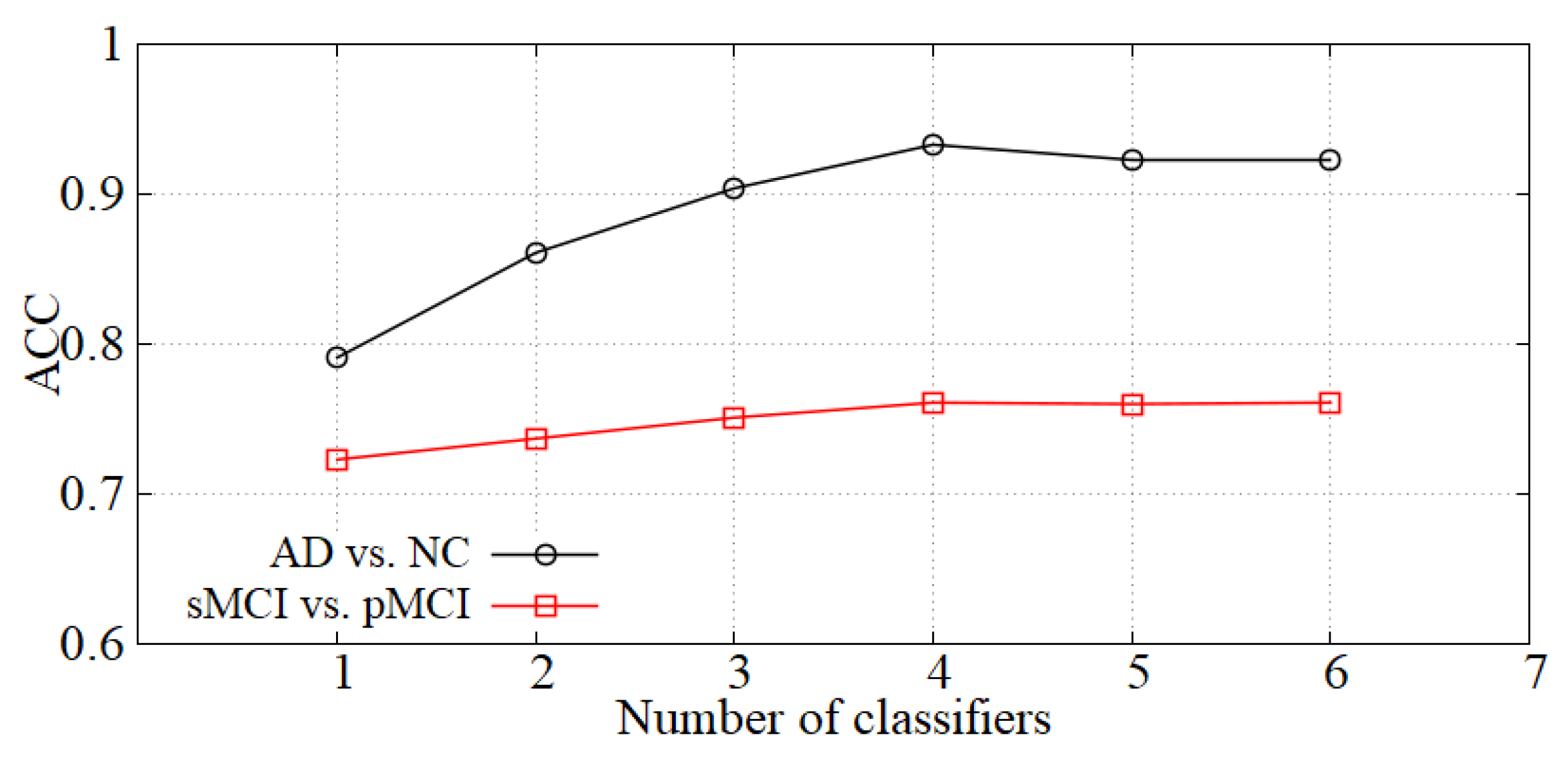
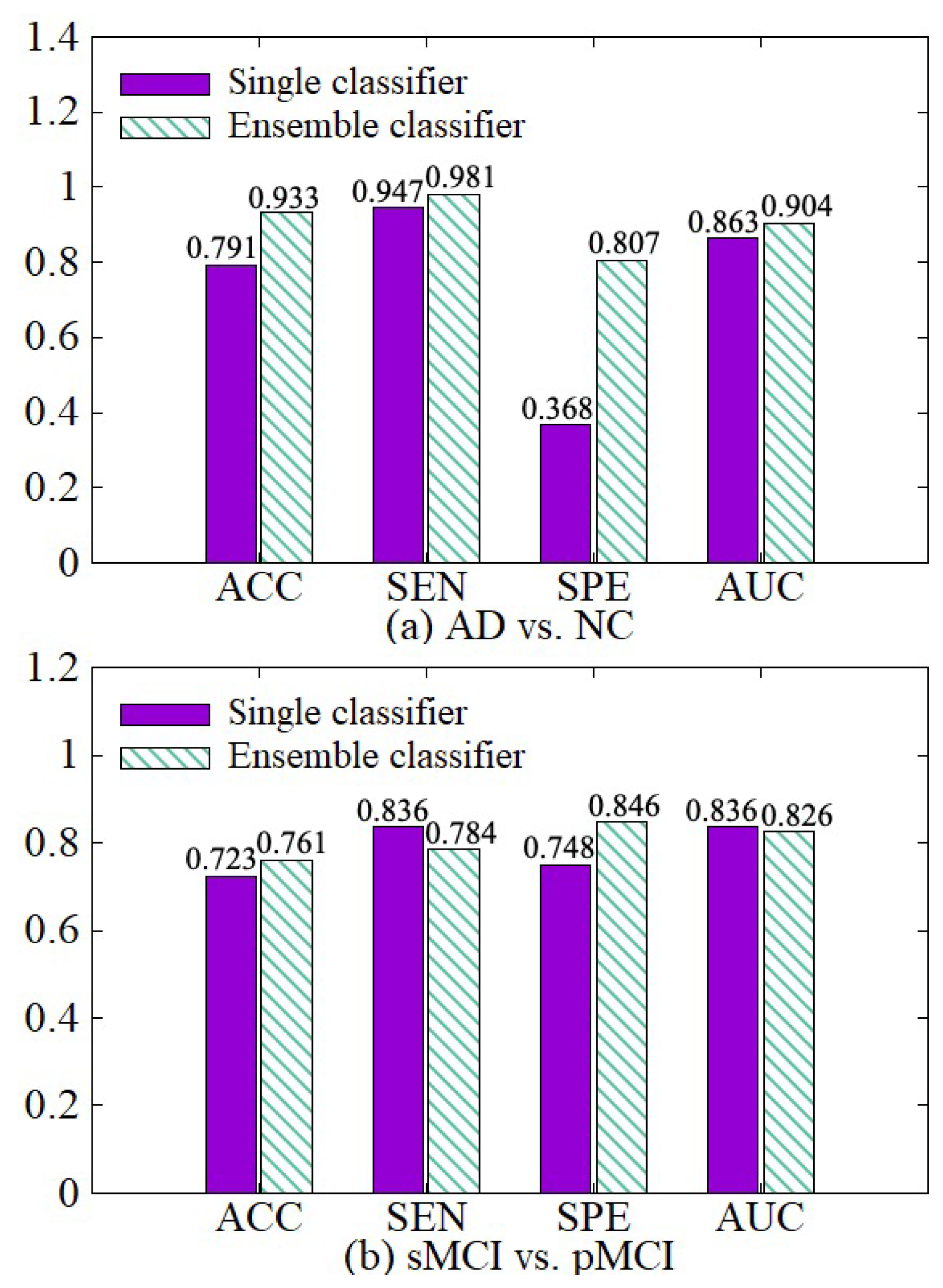
4.3.3. Effectiveness of Diagnosis Network Module
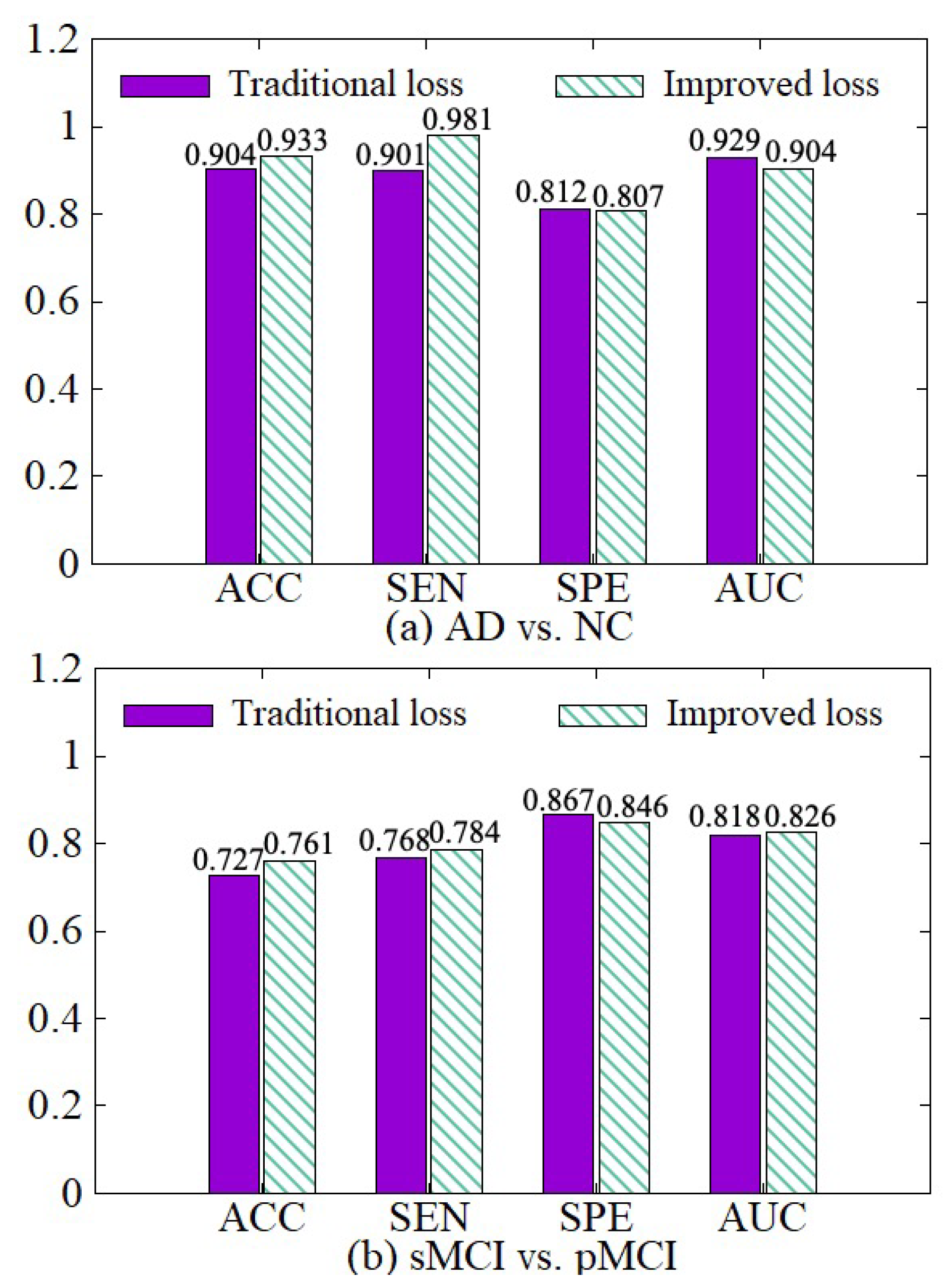
4.3.4. Effectiveness of the Improved Loss
4.3.5. Effectiveness of the Model including Data Denoising and Diagnosis Network
4.3.6. Comparisons with Other Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- LeCun, Y.; Boser, B.; Denker, J.S.; Henderson, D.; Howard, R.E.; Hubbard, W.; Jackel, L.D. Backpropagation Applied to Handwritten Zip Code Recognition. Neural Comput. 1989, 1, 541–551. [Google Scholar] [CrossRef]
- Alinsaif, S.; Lang, J. 3D Shearlet-Based Descriptors Combined with Deep Features for the Classification of Alzheimer’s Disease Based on MRI Data. Comput. Biol. Med. 2021, 138, 104879. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.C.; Chételat, G.; Desgranges, B.; Perchey, G.; Eustache, F. In vivo mapping of gray matter loss with voxel-based morphometry in mild Alzheimer’s disease. Neuroimage 2001, 14, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Yuan, X.; Pu, F.; Li, D.; Fan, Y.; Wu, L.; Chao, W.; Chen, N.; He, Y.; Han, Y. Abnormal changes of multidimensional surface features using multivariate pattern classification in amnestic mild cognitive impairment patients. J. Neurosci. 2014, 34, 10541–10553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Gao, Y.; Gao, Y.; Munsell, B.C.; Shen, D. Detecting anatomical landmarks for fast Alzheimer’s disease diagnosis. IEEE Trans. Med. Imaging 2016, 35, 2524–2533. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Cheng, D.; Wang, K.; Wang, Y. Multi-modality cascaded convolutional neural networks for Alzheimer’s disease diagnosis. Neuroinformatics 2018, 16, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Qiu, H.; Wang, Z.; Liu, W.; Zhang, H.; Li, Y. A new switching-delayed-PSO-based optimized SVM algorithm for diagnosis of Alzheimer’s disease. Neurocomputing 2018, 320, 195–202. [Google Scholar] [CrossRef]
- Wang, S.H.; Phillips, P.; Sui, Y.; Liu, B.; Yang, M.; Cheng, H. Classification of Alzheimer’s disease based on eight-layer convolutional neural network with leaky rectified linear unit and max pooling. J. Med. Syst. 2018, 42, 1–11. [Google Scholar] [CrossRef]
- Cui, R.; Liu, M.; Alzheimer’s Disease Neuroimaging Initiative. RNN-based longitudinal analysis for diagnosis of Alzheimer’s disease. Comput. Med. Imaging Graph. 2019, 73, 1–10. [Google Scholar] [CrossRef]
- Ju, R.; Hu, C.; Li, Q. Early diagnosis of Alzheimer’s disease based on resting-state brain networks and deep learning. IEEE/ACM Trans. Comput. Biol. Bioinform. 2017, 16, 244–257. [Google Scholar] [CrossRef]
- Cui, R.; Liu, M. Hippocampus Analysis by Combination of 3-D DenseNet and Shapes for Alzheimer’s Disease Diagnosis. IEEE J. Biomed. Health Inform. 2018, 23, 2099–2107. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Shen, Y.; Wang, S.; Xiao, T.; Deng, L.; Wang, X.; Zhao, X. Ensemble of 3D densely connected convolutional network for diagnosis of mild cognitive impairment and Alzheimer’s disease. Neurocomputing 2019, 333, 145–156. [Google Scholar] [CrossRef]
- Ashburner, J.; Friston, K.J. Voxel-based morphometry–the methods. Neuroimage 2000, 11, 805–821. [Google Scholar] [CrossRef] [Green Version]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Tong, T.; Wolz, R.; Gao, Q.; Hajnal, J.V.; Rueckert, D. Multiple Instance Learning for Classification of Dementia in Brain MRI. Med. Image Anal. 2013, 16, 599–606. [Google Scholar]
- Liu, M.; Zhang, J.; Adeli, E.; Shen, D. Landmark-based deep multi-instance learning for brain disease diagnosis. Med. Image Anal. 2018, 43, 157–168. [Google Scholar] [CrossRef]
- Pan, Y.; Liu, M.; Lian, C.; Zhou, T.; Xia, Y.; Shen, D. Synthesizing missing PET from MRI with cycle-consistent generative adversarial networks for Alzheimer’s disease diagnosis. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Granada, Spain, 16–20 September 2018; pp. 455–463. [Google Scholar]
- Suk, H.I.; Lee, S.W.; Shen, D.; Initiative, A.D.N. Hierarchical feature representation and multimodal fusion with deep learning for AD/MCI diagnosis. NeuroImage 2014, 101, 569–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lian, C.; Liu, M.; Zhang, J.; Shen, D. Hierarchical fully convolutional network for joint atrophy localization and Alzheimer’s disease diagnosis using structural MRI. IEEE Trans. Pattern Anal. Mach. Intell. 2020, 42, 880–893. [Google Scholar] [CrossRef]
- Ortiz, A.; Munilla, J.; Gorriz, J.M.; Ramirez, J. Ensembles of deep learning architectures for the early diagnosis of the Alzheimer’s disease. Int. J. Neural Syst. 2016, 26, 1650025. [Google Scholar] [CrossRef]
- Maguire, E.A.; Gadian, D.G.; Johnsrude, I.S.; Good, C.D.; Ashburner, J.; Frackowiak, R.; Frith, C.D.; Cadian, D.C.; Johnsrudet, I.S.; Goodt, C.D. Navigation-re ated structura change in the hippocampl ot taxi drivers. Proc. Natl. Acad. Sci. USA 2000, 97, 4398–4403. [Google Scholar] [CrossRef] [Green Version]
- Wolz, R.; Aljabar, P.; Hajnal, J.V.; Lötjönen, J.; Rueckert, D. Nonlinear dimensionality reduction combining MR imaging with non-imaging information. Med. Image Anal. 2012, 16, 819–830. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Cheng, D.; Yan, W.; Alzheimer’s Disease Neuroimaging Initiative. Classification of Alzheimer’s disease by combination of convolutional and recurrent neural networks using FDG-PET images. Front. Neuroinform. 2018, 12, 35. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Islam, J.; Zhang, Y. Early diagnosis of Alzheimer’s disease: A neuroimaging study with deep learning architectures. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops, Salt Lake City, UT, USA, 19–21 June 2018; pp. 1881–1883. [Google Scholar]
- Maqsood, M.; Nazir, F.; Khan, U.; Aadil, F.; Jamal, H.; Mehmood, I.; Song, O.Y. Transfer learning assisted classification and detection of Alzheimer’s disease stages using 3D MRI scans. Sensors 2019, 19, 2645. [Google Scholar] [CrossRef] [Green Version]
- Karasawa, H.; Liu, C.L.; Ohwada, H. Deep 3d convolutional neural network architectures for alzheimer’s disease diagnosis. In Proceedings of the Asian Conference on Intelligent Information and Database Systems, Dong Hoi City, Vietnam, 19–21 March 2018; pp. 287–296. [Google Scholar]
- Basaia, S.; Agosta, F.; Wagner, L.; Canu, E.; Magnani, G.; Santangelo, R.; Filippi, M.; Initiative, A.D.N. Automated classification of Alzheimer’s disease and mild cognitive impairment using a single MRI and deep neural networks. NeuroImage Clin. 2019, 21, 101645. [Google Scholar] [CrossRef] [PubMed]
- Duc, N.T.; Ryu, S.; Qureshi, M.N.I.; Choi, M.; Lee, K.H.; Lee, B. 3D-deep learning based automatic diagnosis of Alzheimer’s disease with joint MMSE prediction using resting-state fMRI. Neuroinformatics 2020, 18, 71–86. [Google Scholar] [CrossRef] [PubMed]
- Feng, C.; Elazab, A.; Yang, P.; Wang, T.; Zhou, F.; Hu, H.; Xiao, X.; Lei, B. Deep learning framework for Alzheimer’s disease diagnosis via 3D-CNN and FSBi-LSTM. IEEE Access 2019, 7, 63605–63618. [Google Scholar] [CrossRef]
- Freund, Y.; Schapire, R.; Abe, N. A short introduction to boosting. J. Jpn. Soc. Artif. Intell. 1999, 14, 1612. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Nair, V.; Hinton, G.E. Rectified Linear Units Improve Restricted Boltzmann Machines Vinod Nair. In Proceedings of the 27th International Conference on Machine Learning (ICML-10), Haifa, Israel, 21–24 June 2010; pp. 807–814. [Google Scholar]
- Ioffe, S.; Szegedy, C. Batch normalization: Accelerating deep network training by reducing internal covariate shift. In Proceedings of the International Conference on Machine Learning, Lille, France, 6–11 July 2015; pp. 448–456. [Google Scholar]
- Zhou, Y.T.; Chellappa, R. Computation of optical flow using a neural network. In Proceedings of the IEEE 1988 International Conference on Neural Networks, San Diego, CA, USA, 24–27 July 1988; pp. 71–78. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A Simple Way to Prevent Neural Networks from Overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Jack, C.R., Jr.; Bernstein, M.A.; Fox, N.C.; Thompson, P.; Alexander, G.; Harvey, D.; Borowski, B.; Britson, P.J.; Whitwell, J.L.; Ward, C.; et al. The Alzheimer’s disease neuroimaging initiative (ADNI): MRI methods. J. Magn. Reson. Imaging Off. J. Int. Soc. Magn. Reson. Med. 2008, 27, 685–691. [Google Scholar] [CrossRef] [Green Version]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer | Operation | Size | Input | Output |
|---|---|---|---|---|
| 0 | conv(bn) | 3 × 3 × 3 × 8 | 192 × 192 × 160 × 1 | 192 × 192 × 160 × 8 |
| 1 | maxpooling | 2 × 2 × 2 | 192 × 192 × 160 × 8 | 96 × 96 × 80 × 8 |
| 2 | conv(bn) | 3 × 3 × 3 × 16 | 96 × 96 × 80 × 8 | 96 × 96 × 80 × 16 |
| 3 | maxpooling | 2 × 2 × 2 | 96 × 96 × 80 × 16 | 48 × 48 × 40 × 16 |
| 4 | conv(bn) | 3 × 3 × 3 × 32 | 48 × 48 × 40 × 16 | 48 × 48 × 40 × 32 |
| 5 | conv(bn) | 3 × 3 × 3 × 32 | 48 × 48 × 40 × 32 | 48 × 48 × 40 × 32 |
| 6 | maxpooling | 2 × 2 × 2 | 48 × 48 × 40 × 32 | 24 × 24 × 20 × 32 |
| 7 | conv(bn) | 3 × 3 × 3 × 64 | 24 × 24 × 20 × 32 | 24 × 24 × 20 × 64 |
| 8 | conv(bn) | 3 × 3 × 3 × 64 | 24 × 24 × 20 × 64 | 24 × 24 × 20 × 64 |
| 9 | maxpooling | 2 × 2 × 2 | 24 × 24 × 20 × 64 | 12 × 12 × 10 × 64 |
| 10 | conv(bn) | 3 × 3 × 3 × 64 | 12 × 12 × 10 × 64 | 12 × 12 × 10 × 64 |
| 11 | conv(bn) | 3 × 3 × 3 × 64 | 12 × 12 × 10 × 64 | 12 × 12 × 10 × 64 |
| 12 | maxpooling | 2 × 2 × 2 | 12 × 12 × 10 × 64 | 6 × 6 × 5 × 64 |
| 13 | fc | 2048 | 6 × 6 × 5 × 64 | 2048 |
| 14 | fc | 2048 | 2048 | 2048 |
| 15 | fc | 2 | 2048 | 2 |
| Protocol Parameter | Value |
|---|---|
| Acquisition Plane | Sagittal |
| Acquisition Type | 3D |
| Field Strength | 1.5 tesla |
| Slice Thickness | 1.2 mm |
| TE | 3.5–3.7 ms |
| TI | 1000.0 ms |
| TR | 3000.0 ms |
| Weighting | T1 |
| Training Time(s) | AD vs. NC | sMCI vs. pMCI |
|---|---|---|
| Without denoising | 12,093 | 13,784 |
| With denoising | 6399 | 7273 |
| Methods | AD vs. NC | sMCI vs. pMCI | ||||||
|---|---|---|---|---|---|---|---|---|
| ACC | SEN | SPE | AUC | ACC | SEN | SPE | AUC | |
| Suk et al. [18] | 0.92 | 0.92 | 0.95 | 0.97 | 0.72 | 0.37 | 0.91 | 0.73 |
| Ortiz et al. [20] | 0.90 | - | - | 0.95 | - | - | - | - |
| Liu et al. [16] | 0.91 | 0.88 | 0.94 | 0.96 | 0.77 | 0.42 | 0.82 | 0.78 |
| Karasawa et al. [27] | 0.94 | - | - | - | - | - | - | - |
| Cui et al. [11] | 0.92 | 0.91 | 0.94 | 0.97 | 0.75 | 0.73 | 0.76 | 0.80 |
| Feng et al. [30] | 0.95 | 0.98 | 0.93 | 0.97 | - | - | - | - |
| Lian et al. [19] | 0.90 | 0.82 | 0.97 | 0.95 | 0.81 | 0.53 | 0.85 | 0.78 |
| Alinsaif et al. [2] | - | - | - | - | 0.70 | 0.60 | 0.80 | - |
| Ours | 0.95 | 0.96 | 0.93 | 0.97 | 0.78 | 0.79 | 0.87 | 0.84 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, P.; Lin, S.; Qiao, J.; Tu, Y. Diagnosis of Alzheimer’s Disease with Ensemble Learning Classifier and 3D Convolutional Neural Network. Sensors 2021, 21, 7634. https://doi.org/10.3390/s21227634
Zhang P, Lin S, Qiao J, Tu Y. Diagnosis of Alzheimer’s Disease with Ensemble Learning Classifier and 3D Convolutional Neural Network. Sensors. 2021; 21(22):7634. https://doi.org/10.3390/s21227634
Chicago/Turabian StyleZhang, Peng, Shukuan Lin, Jianzhong Qiao, and Yue Tu. 2021. "Diagnosis of Alzheimer’s Disease with Ensemble Learning Classifier and 3D Convolutional Neural Network" Sensors 21, no. 22: 7634. https://doi.org/10.3390/s21227634
APA StyleZhang, P., Lin, S., Qiao, J., & Tu, Y. (2021). Diagnosis of Alzheimer’s Disease with Ensemble Learning Classifier and 3D Convolutional Neural Network. Sensors, 21(22), 7634. https://doi.org/10.3390/s21227634