4.2.1. Changing Body Position
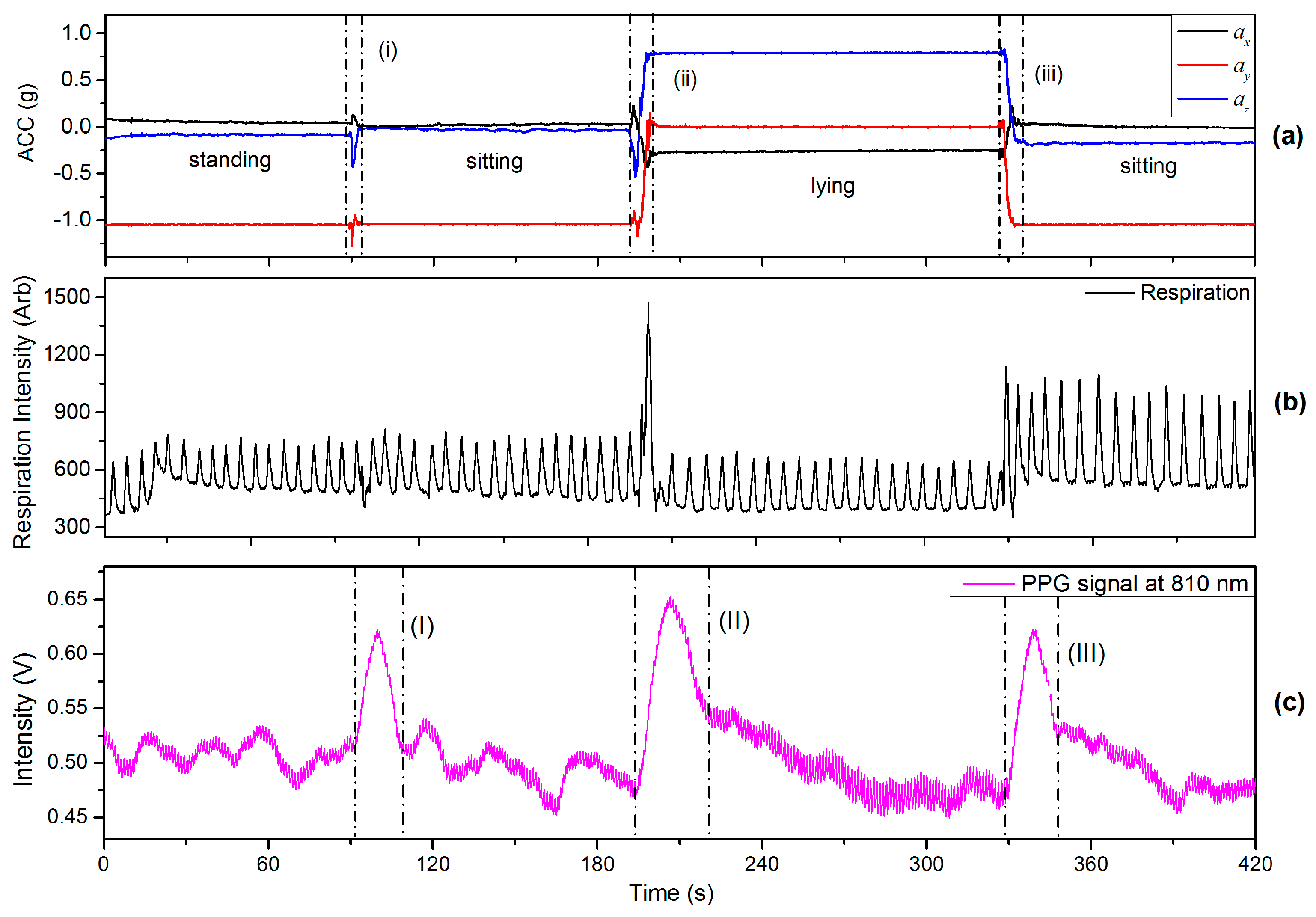
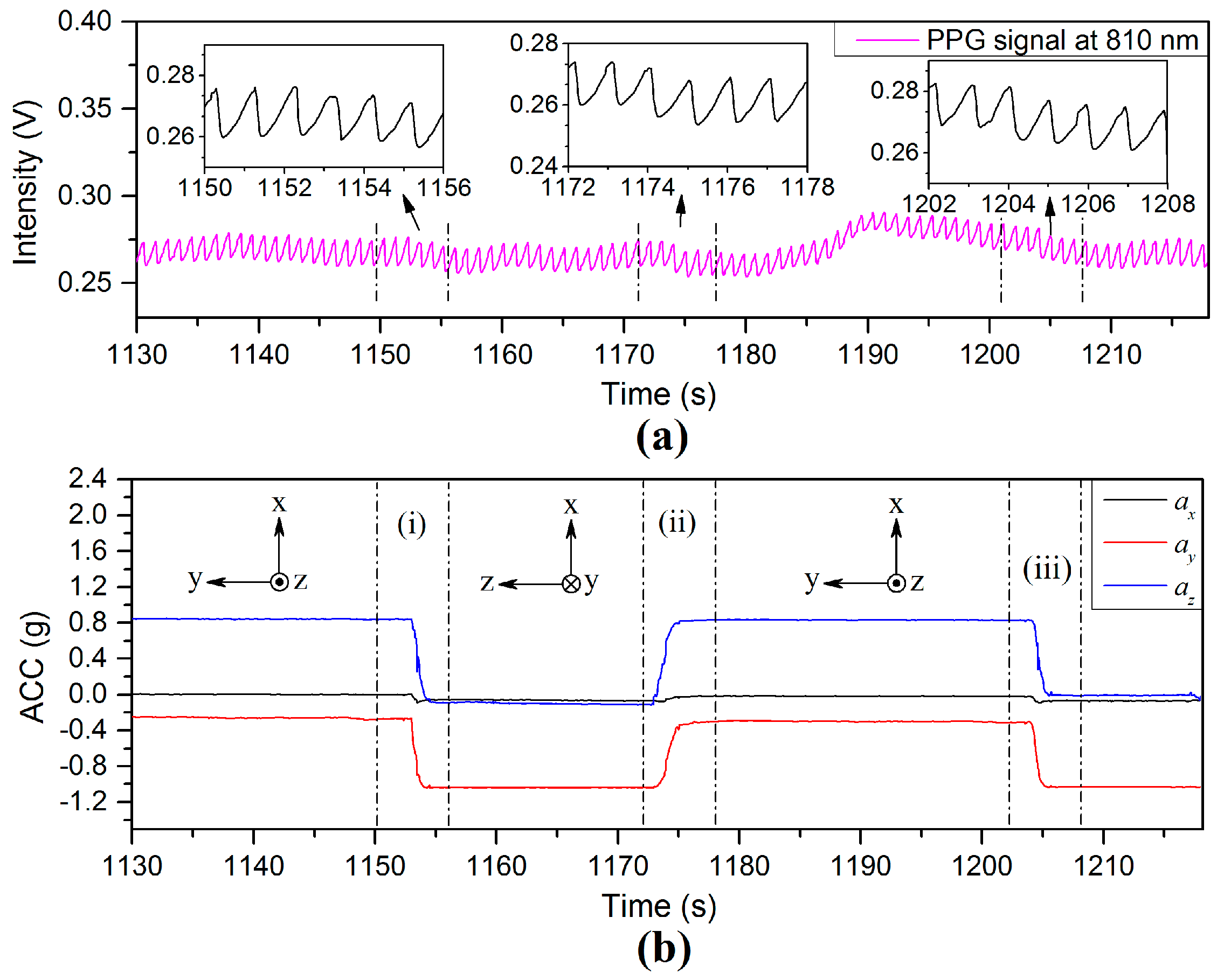
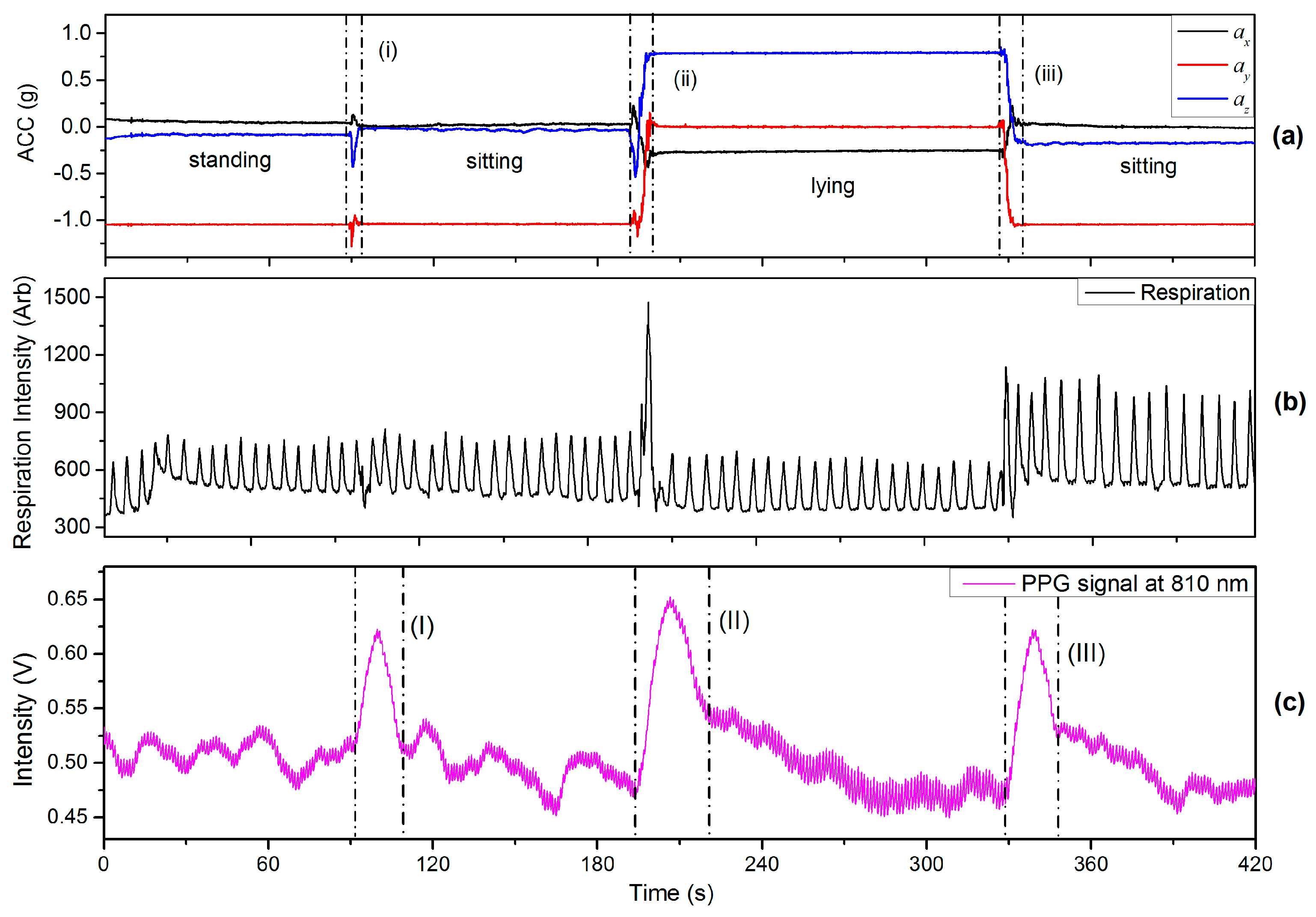
This section includes the results of an experiment in which the finger sensor probe was fixed at the same VHD whilst changing the body position. In one of the experiments the finger sensor probe was kept in front of chest at heart level whilst changing body positions between sitting, standing and lying positions. The subjects were requested to breathe evenly and smoothly without talking throughout the experiments. The recorded respiration data corresponding to the arbitrary analog output of the respiration monitor belt device is shown in
Figure 10b. The period from the rising edge of PPG signal to the start of a stable region (no significant signal change) is defined as a PPG-fluctuation, e.g., the regions (I–III) in
Figure 10c. Region (i) in
Figure 10a indicates a sitting down process (from standing to sitting). The reason for the PPG-fluctuation in
Figure 10c is believed to arise from ANS variations induced by the change in body position. Since there is no VHD, the observed values of BLs are almost the same before and after the PPG-fluctuation as was to be expected. Region (ii) represents the process of lying down for which the height of the finger sensor probe was unavoidably changed from heart level to a level about 6 cm above heart level since the finger sensor probe was kept in front of chest at all the times. The PPG fluctuation [region (II in
Figure 10c)] is believed to be caused by an ANS variation accompanied with BP changes resulting from hydrostatic changes caused by the body position variation. Similarly, region (iii) corresponds to the postural change from lying to sitting, and another PPG-fluctuation [region (III)] is associated with it. Rotating the wrist was also included in this experiment, indicated by region (ii) and (iii), in
Figure 10a. The effect of wrist rotation on PPG signals is discussed in detail in
Section 4.4 of this paper.
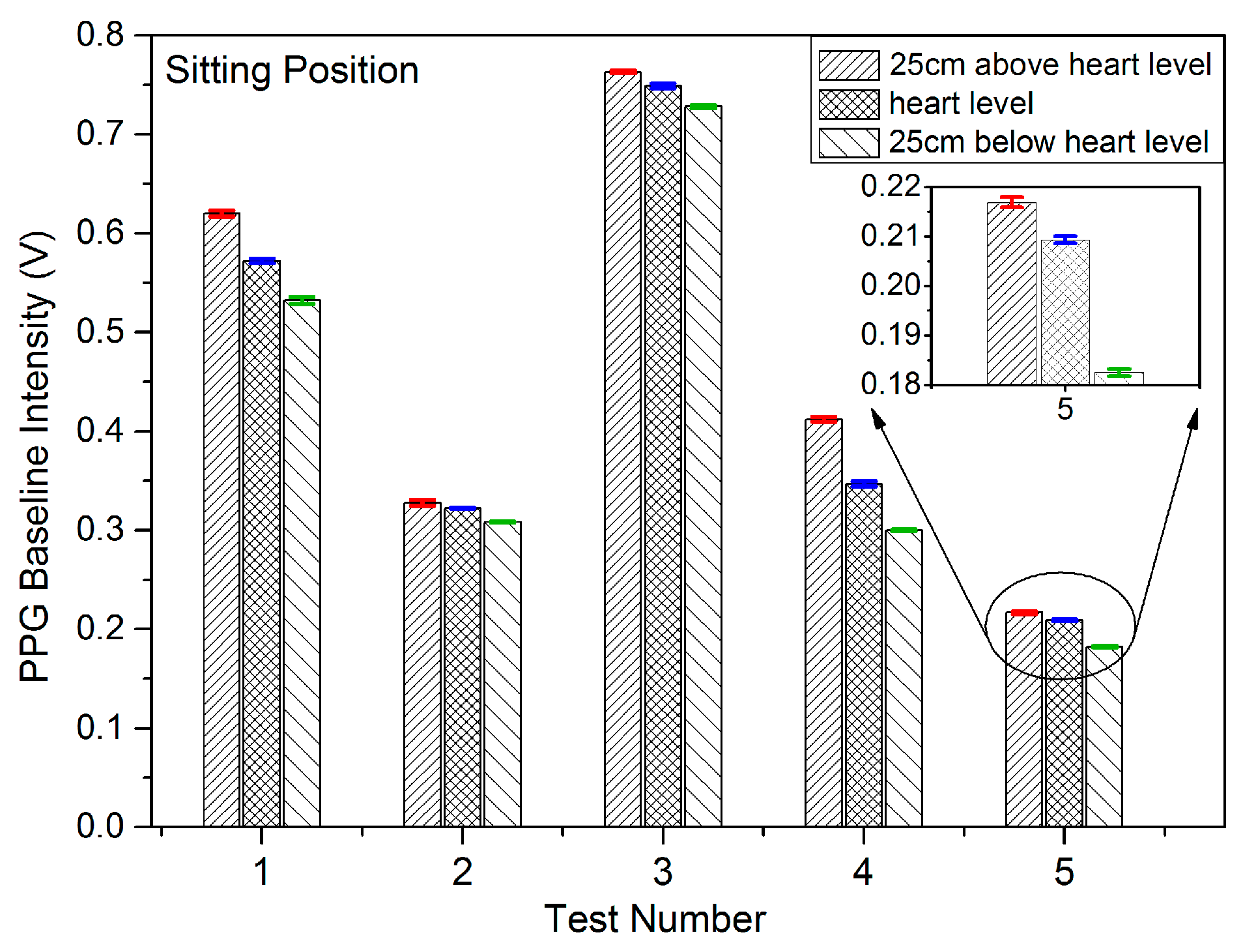
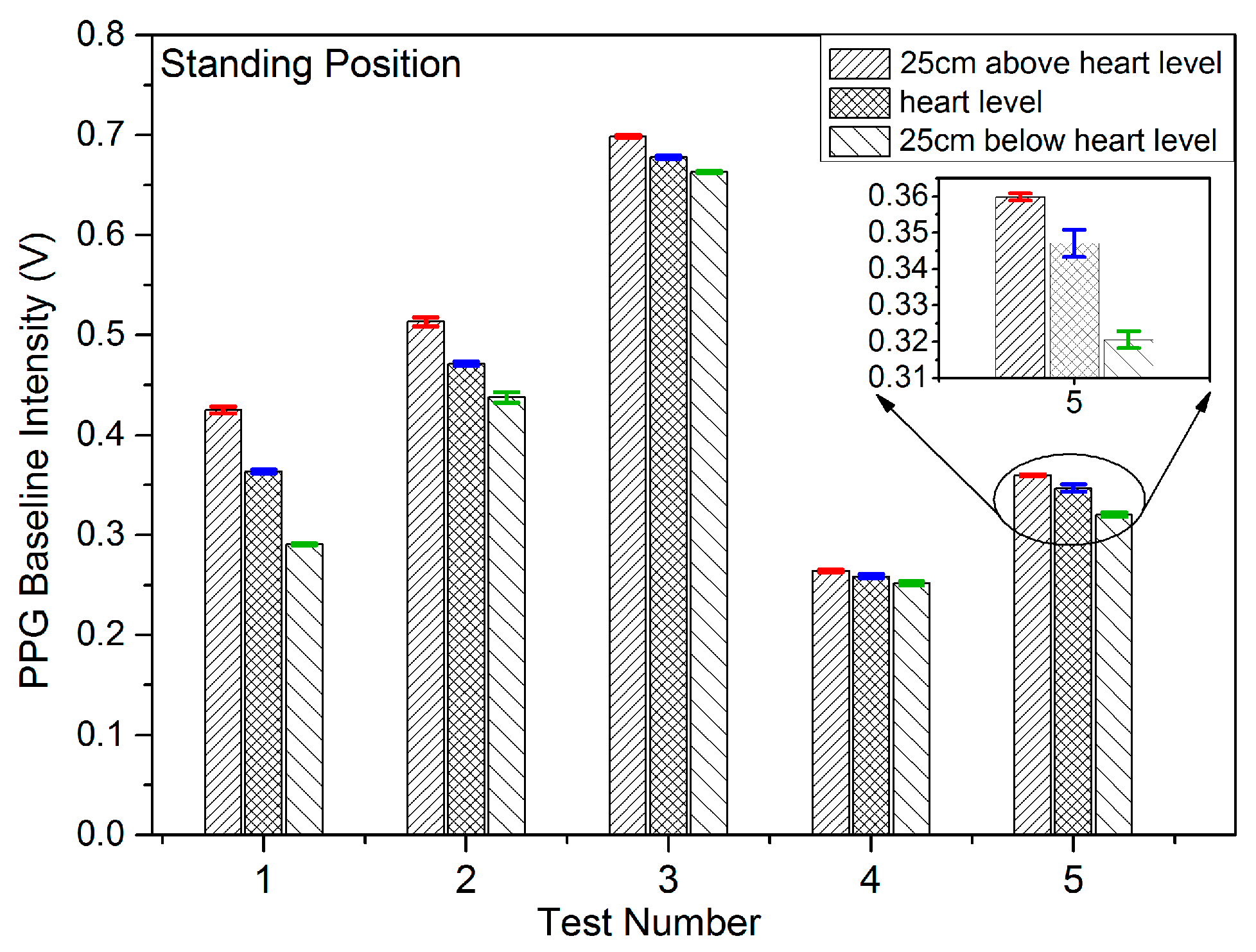
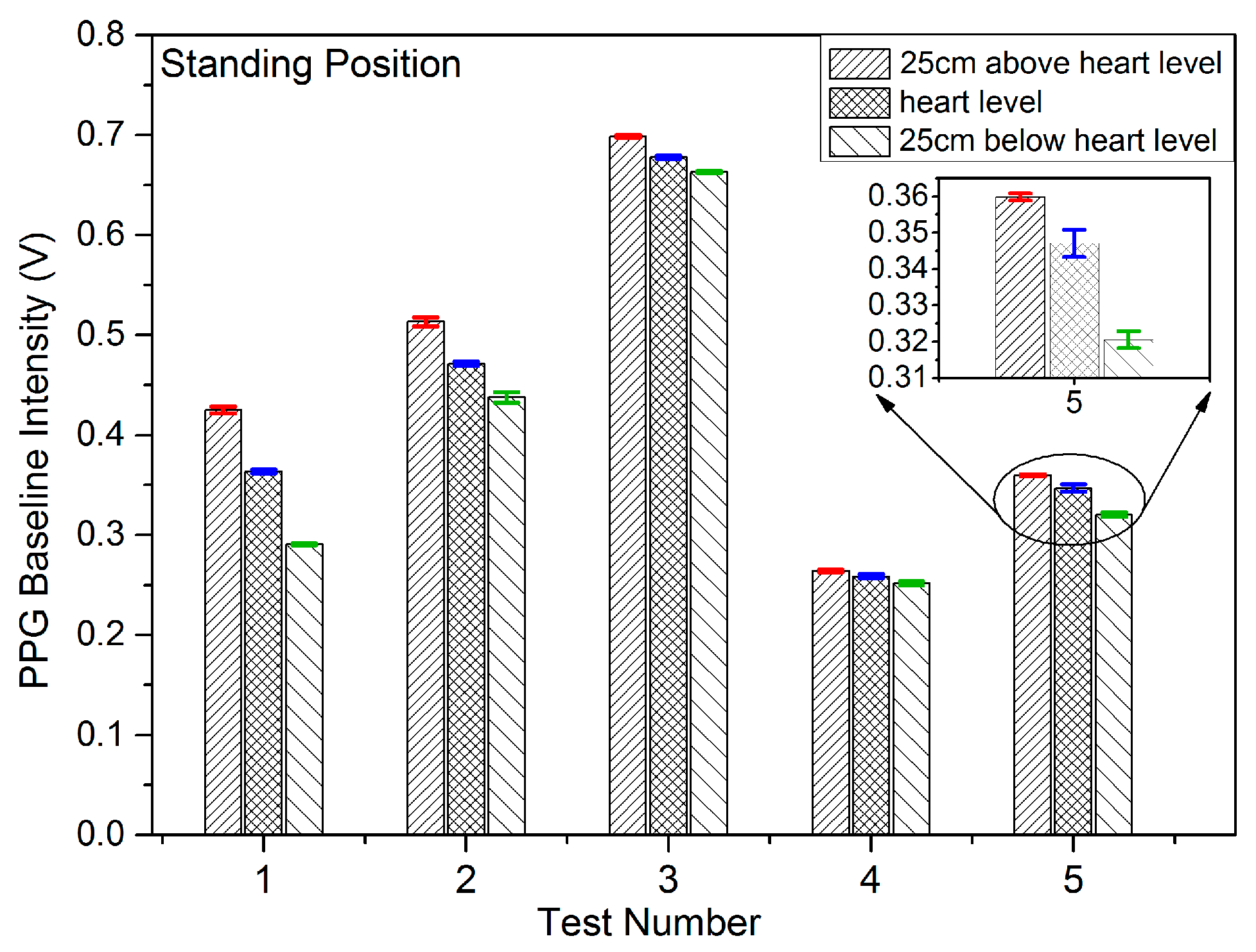
Results were initially gathered from five separate randomly selected subjects for which body position varied from a standing position to a sitting position corresponding to the tests outlined above. These are characterised using the parameters outlined in
Table 5. These parameters are defined as the period of body variation process as
t∆ACC (in seconds); the interval of the PPG fluctuation according to body position variation as
t∆BL (in seconds); respiration rate (RR) (in units of per min); and the difference between the peak value of BL in the fluctuation and average of BL before the fluctuation (a 60 s interval used in this case) as ∆BL (in Volts). The demonstration shows that the PPG signals at the point of measurement are affected by the ANS variations induced by change in body position.
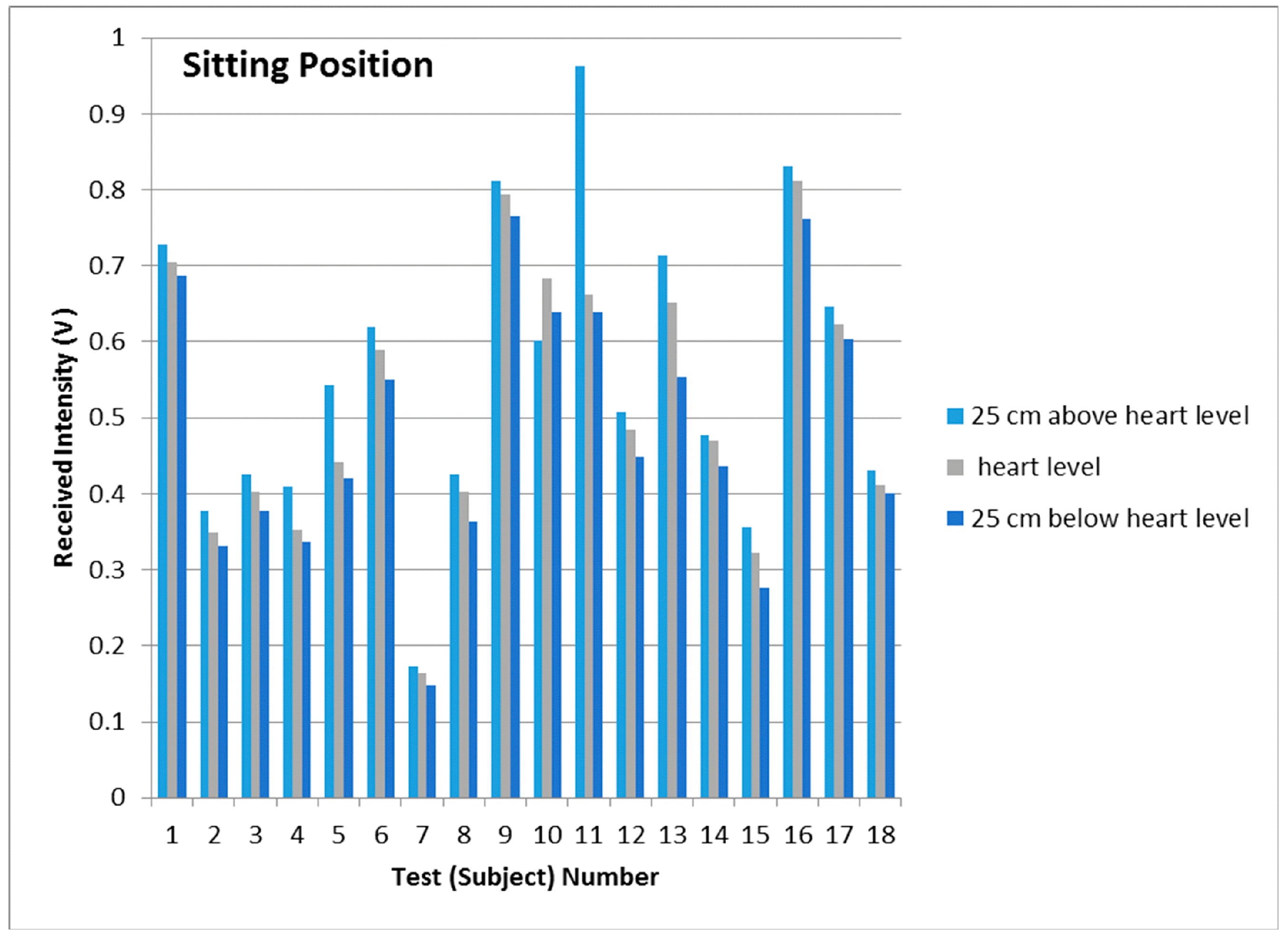
Further independent tests results were obtained from the other 18 subjects referred to in
Section 4.1. For which body position was varied from a sitting position to a standing position and these are listed in
Table 6, accompanied with a study of the preliminary statistical analysis including mean, median, standard deviation and interquartile range as shown in
Table 7. These results captured for a large group of subjects confirm the efficacy of the earlier results (
Table 5) and hence the validity of the measurement technique employed in this investigation.
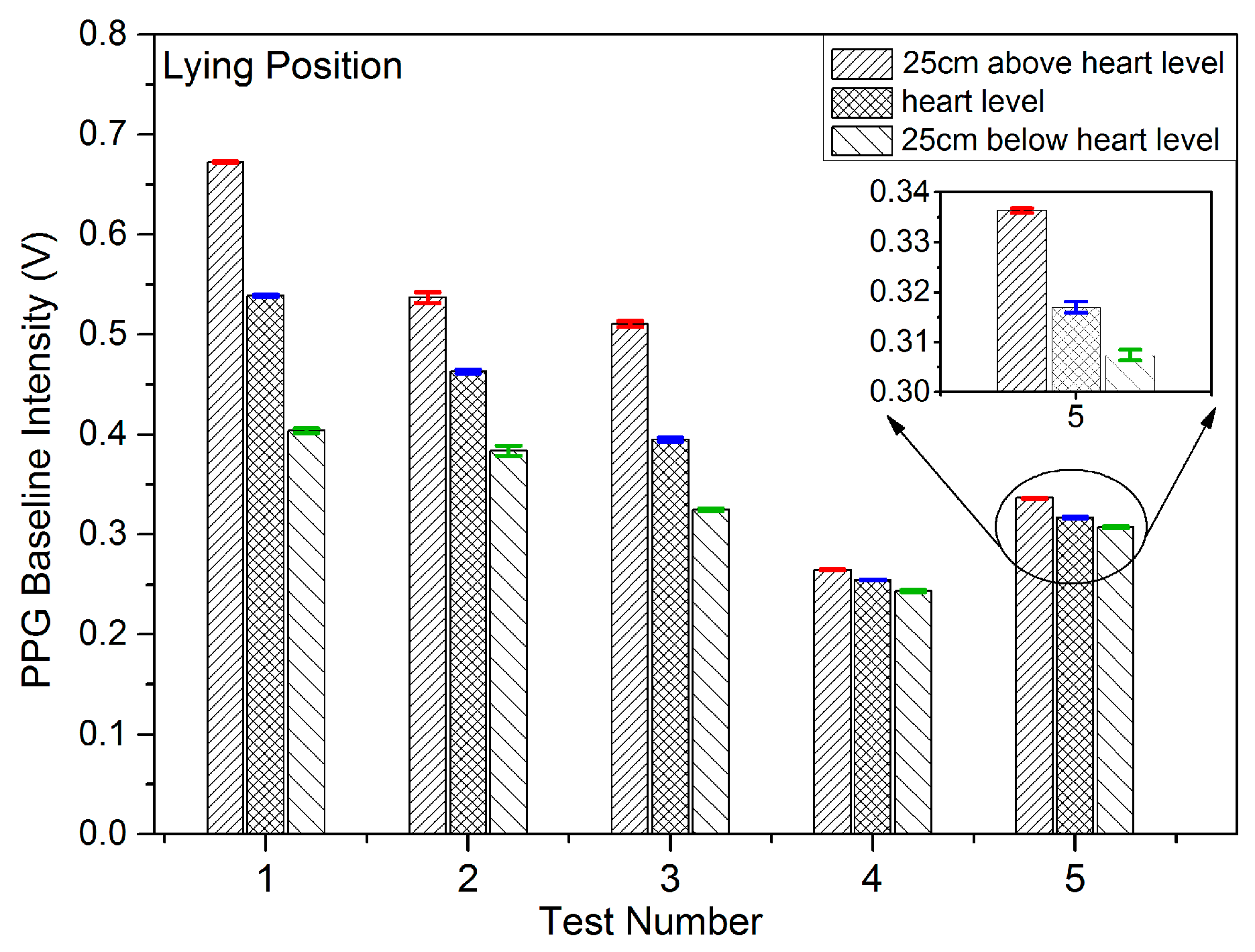
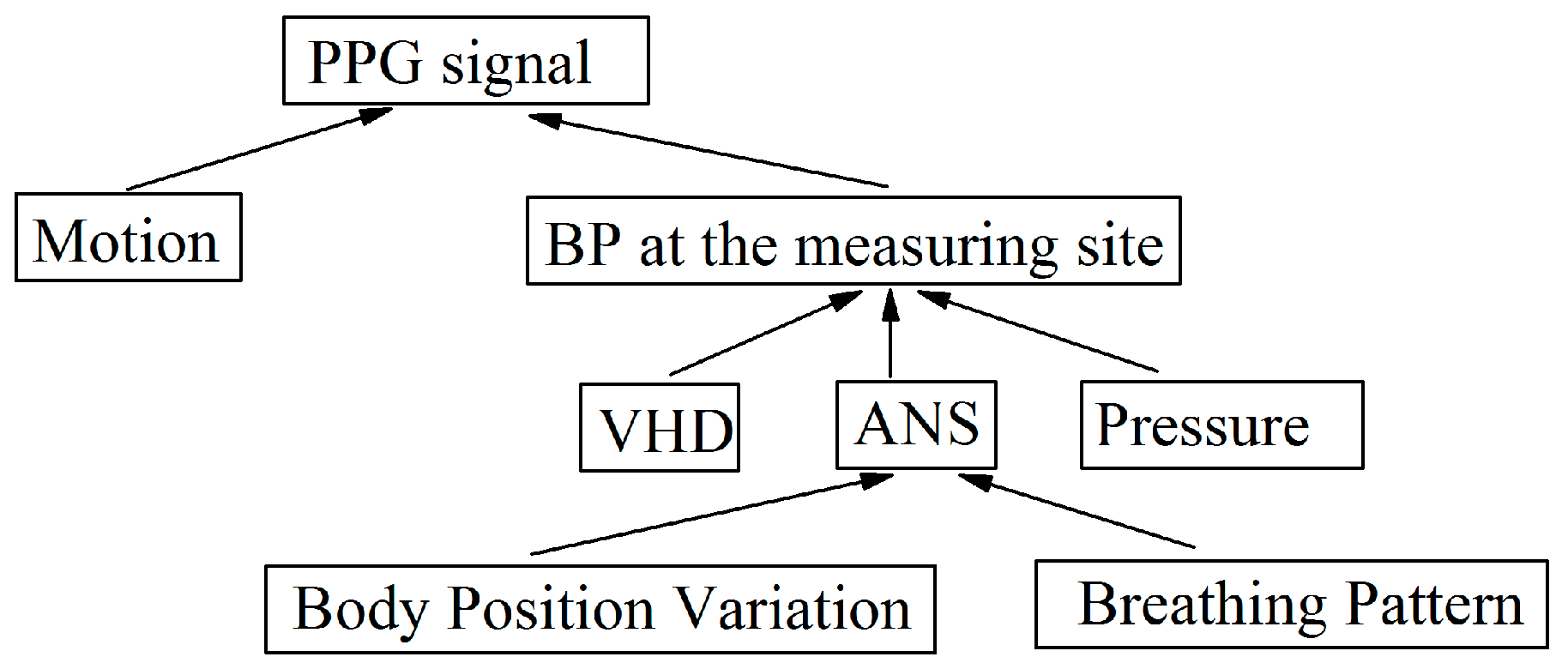
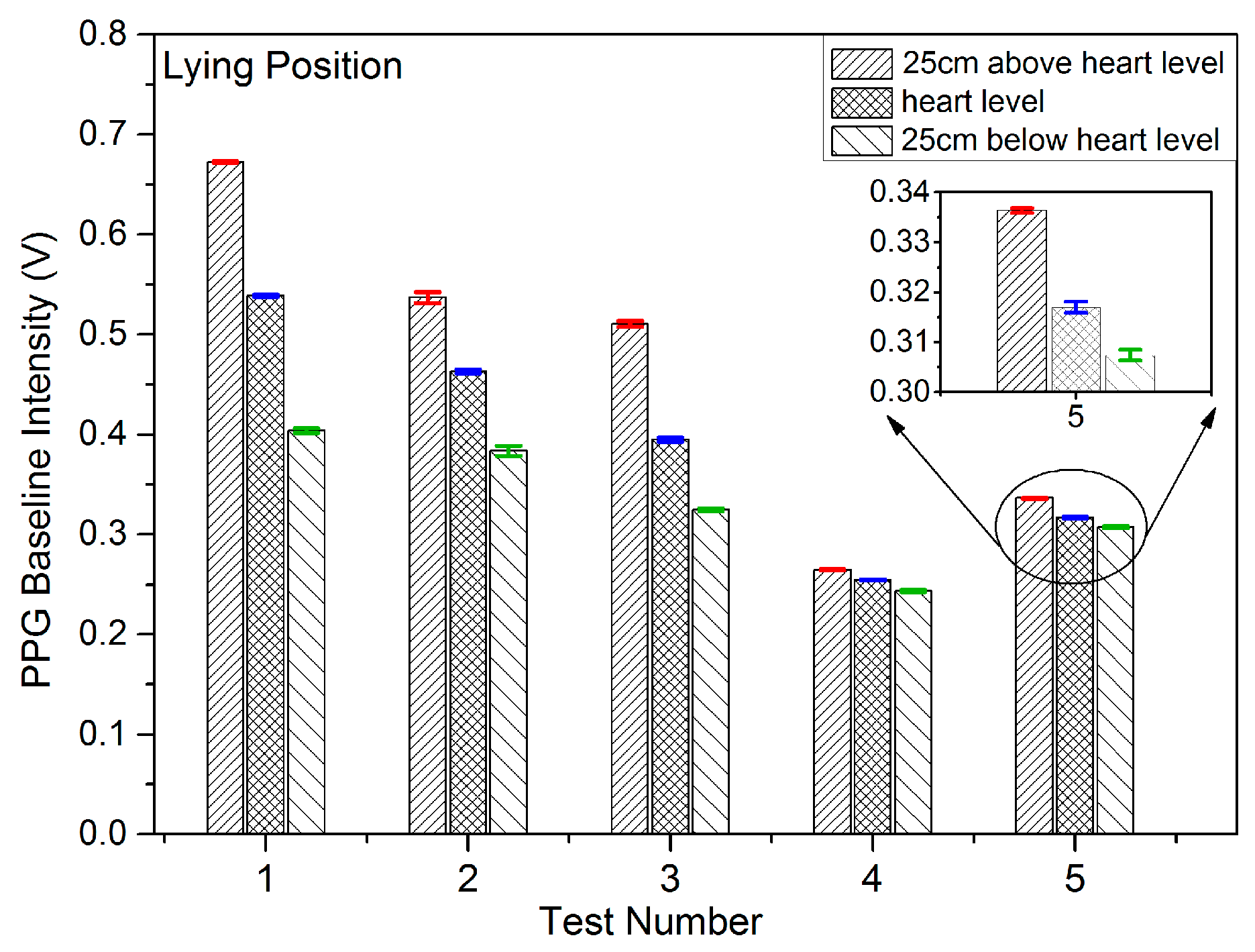
The experimental results of this section show the PPG fluctuation as a result of body positional changes. A position change involves a change in blood flow and BP, and homeostasis is recovered by means of the ANS. The PPG fluctuation is therefore most likely caused by hemodynamic changes and not solely by the ANS. Furthermore it is generally accepted that the parasympathetic system dominates whilst in the lying position, and therefore the effect of the ANS should be present throughout the duration of the lying position.
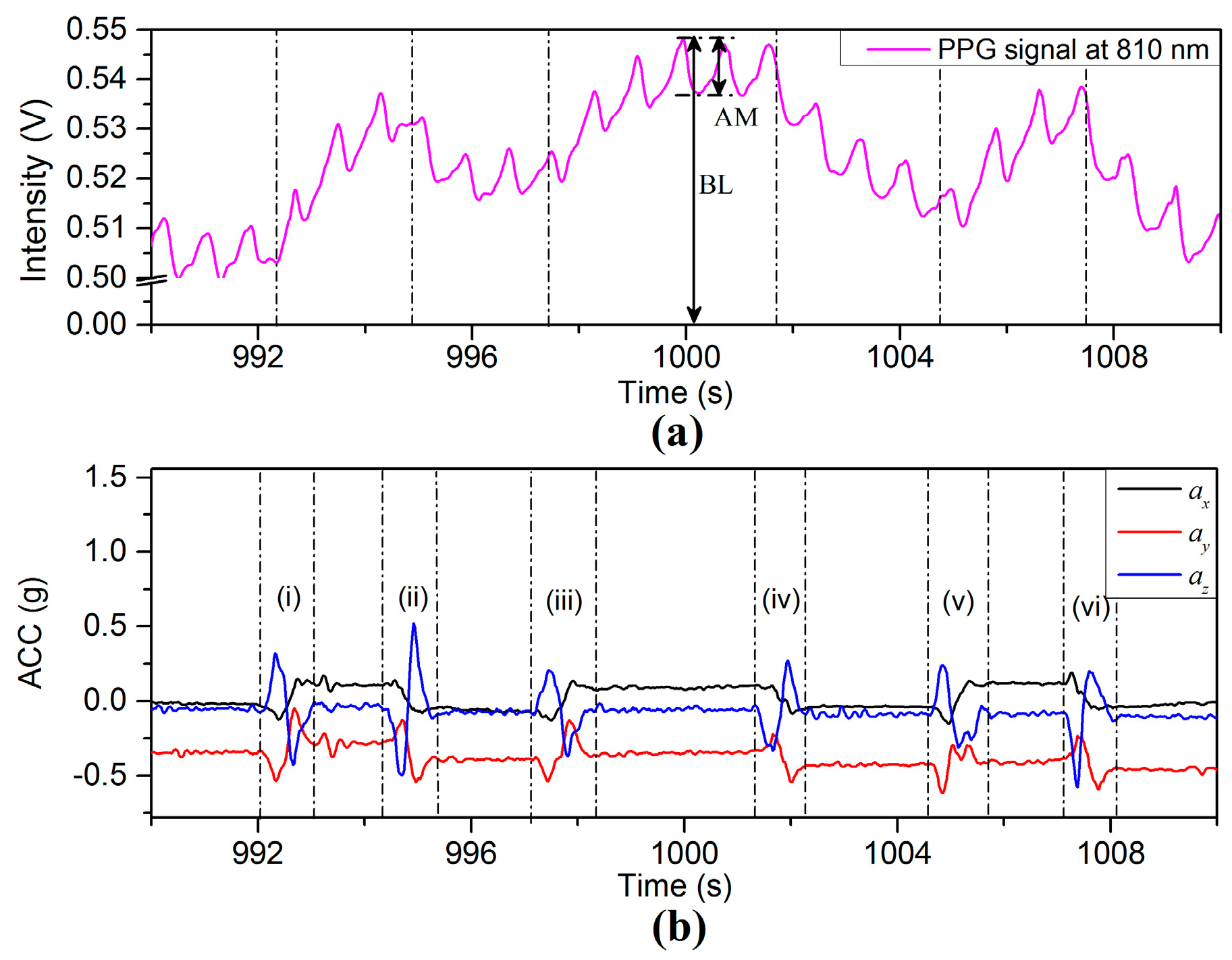
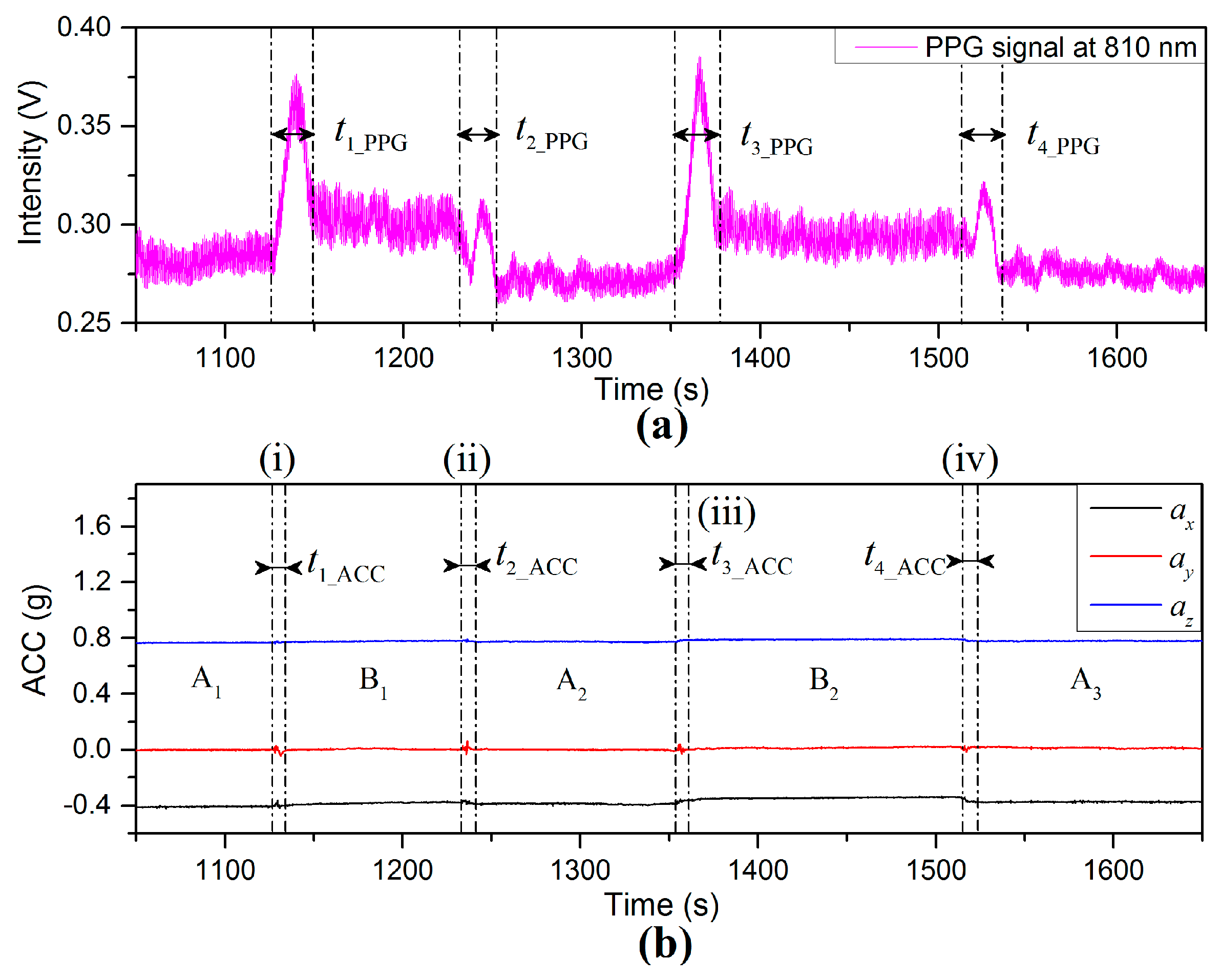
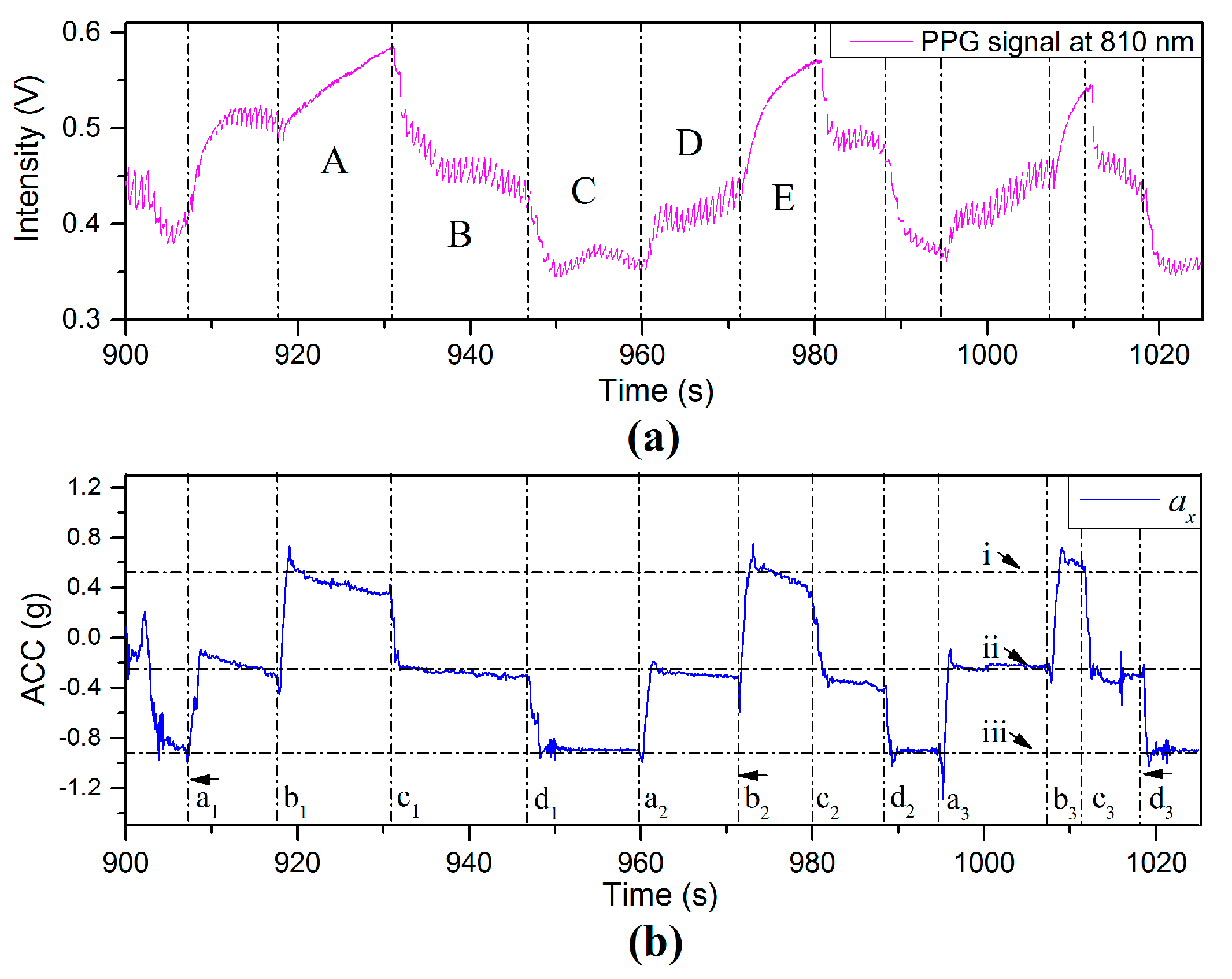
PPG and ACC time dependent signals are shown in
Figure 11 for which the subjects were required to maintain the finger sensor probe at the same height above the floor and the VHD was varied by changing body position. Time period
represents the subject standing still with the finger sensor probe at 25 cm below heart level. Region (i) represented by
in
Figure 11b shows the process of sitting down slowly and the VHD changing from 25 cm below heart level to a level close to heart level, where the amplitudes of accelerations are low and in the range of 0.05 g (0.49 ms
−2). Referring to
Figure 11a, it can be seen that there is an increase of BL in the PPG signal during the time period defined by
. The time duration difference between
and
is 15.1 s, however during
the BL fluctuates significantly whereas the accelerometer on the finger sensor probe detects only limited acceleration due to motion. Time period
corresponds to signals recorded for which the subject was sitting with the finger sensor probe at heart level. Region (ii) which is defined by
in
Figure 11b shows the accelerometer signal while the subject was standing up and the VHD changes from heart level to 25 cm below heart level. During the interval (ii), the BL of the PPG signal decreases, and the time interval for the PPG signal change is described by
. There is a 13.6 s difference between
and
. The transition intervals (iii) and (iv) thereafter display similar results to those of (i) and (ii), being 18.8 s and 18.0 s difference, respectively, between the accelerometer data settling and the PPG signal settling.
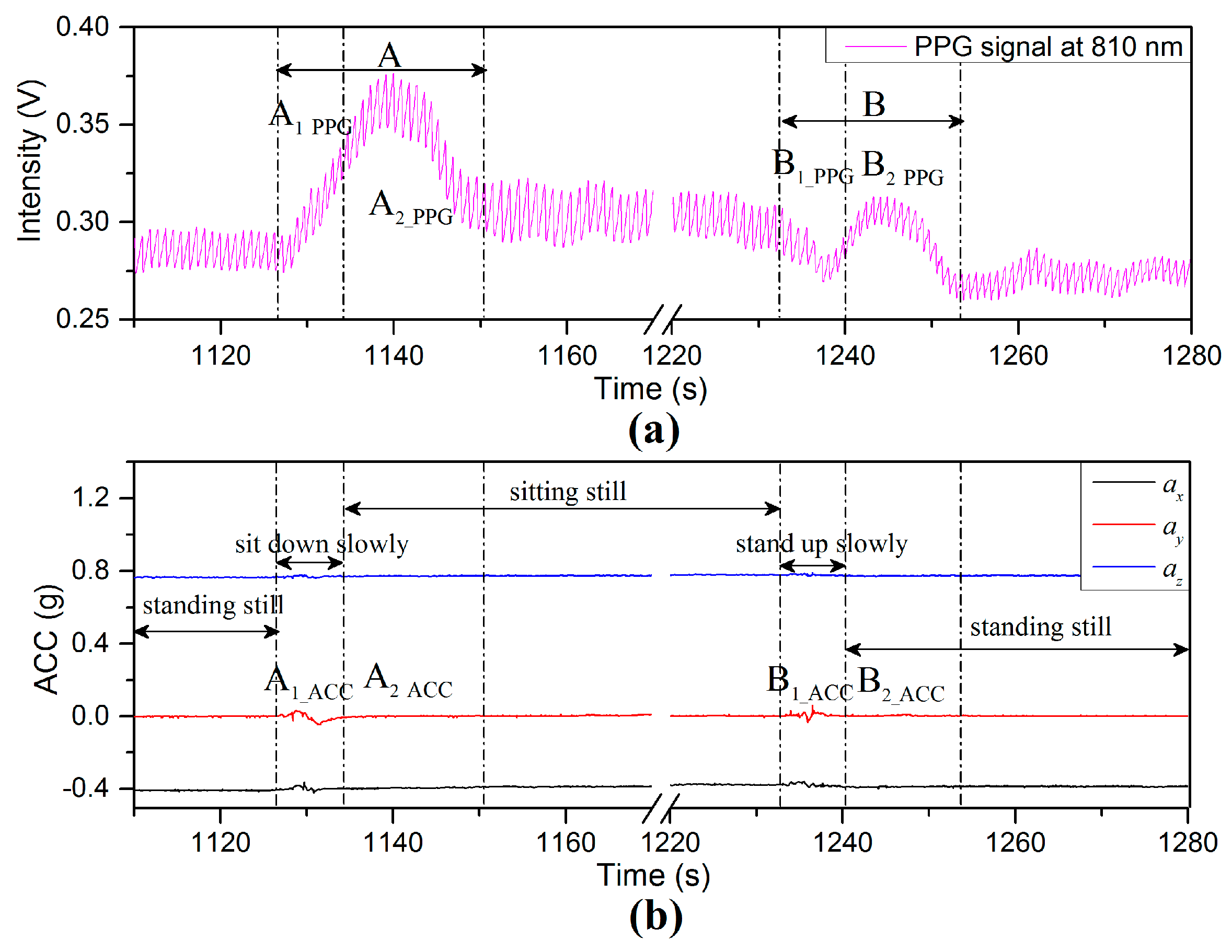
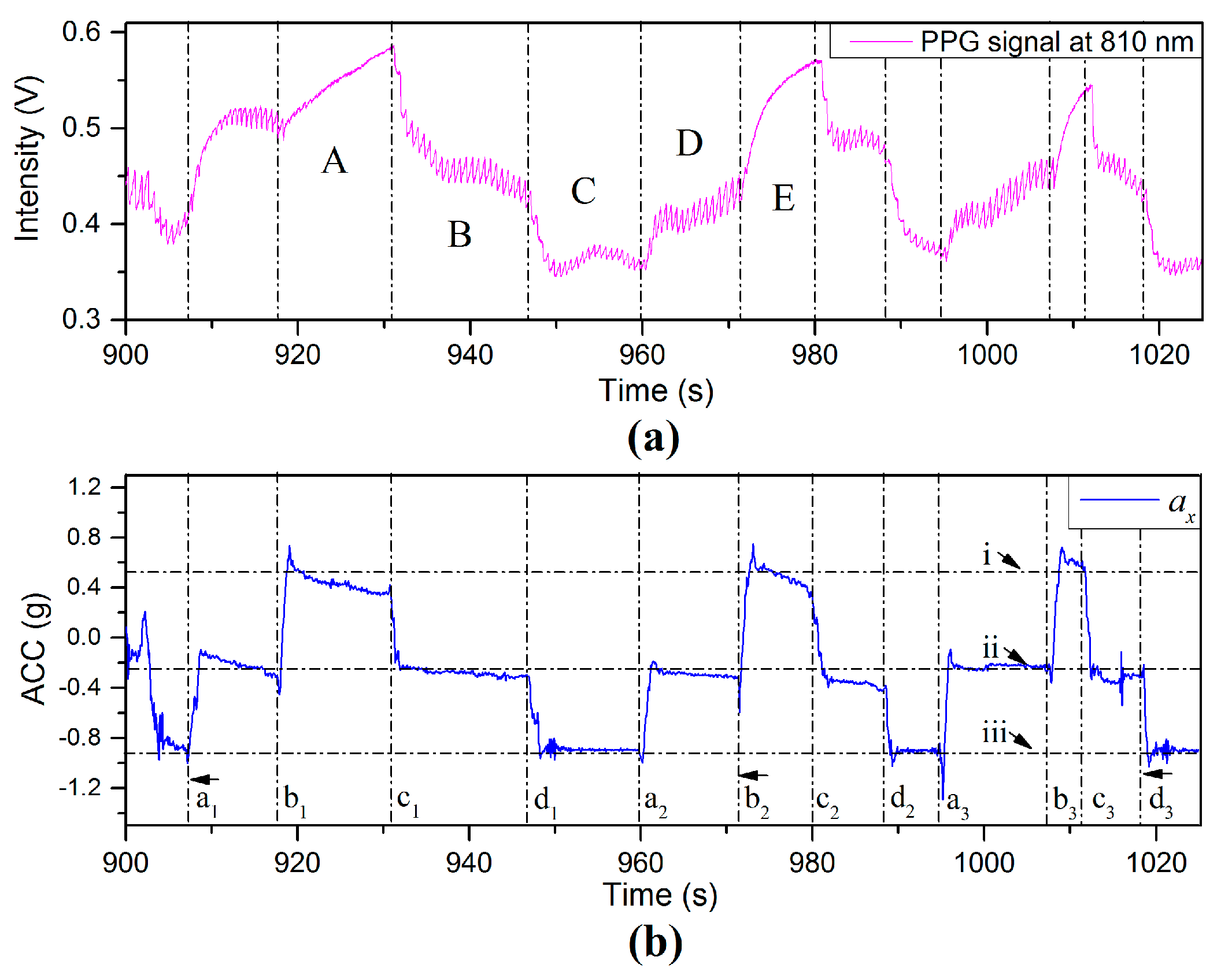
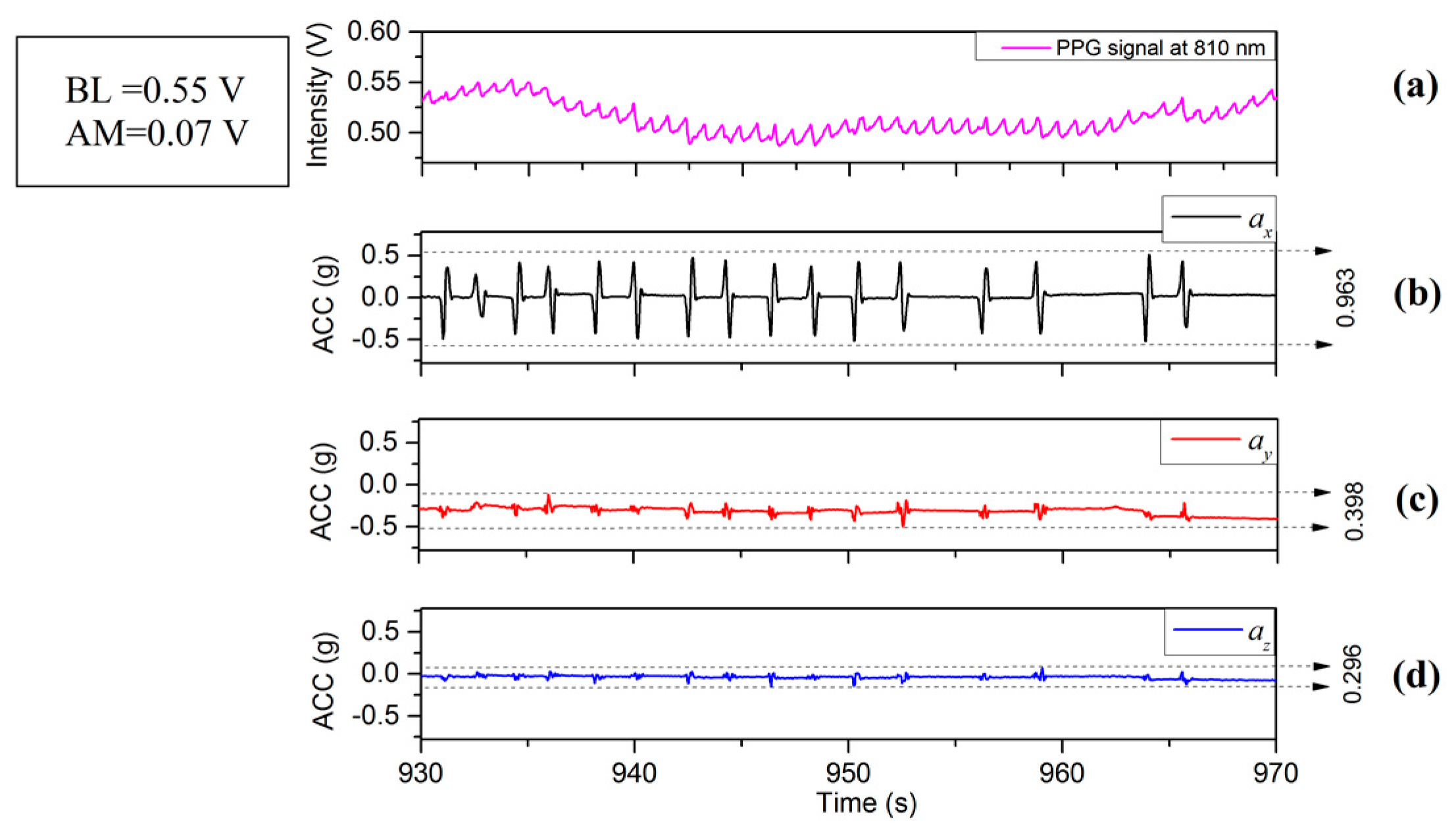
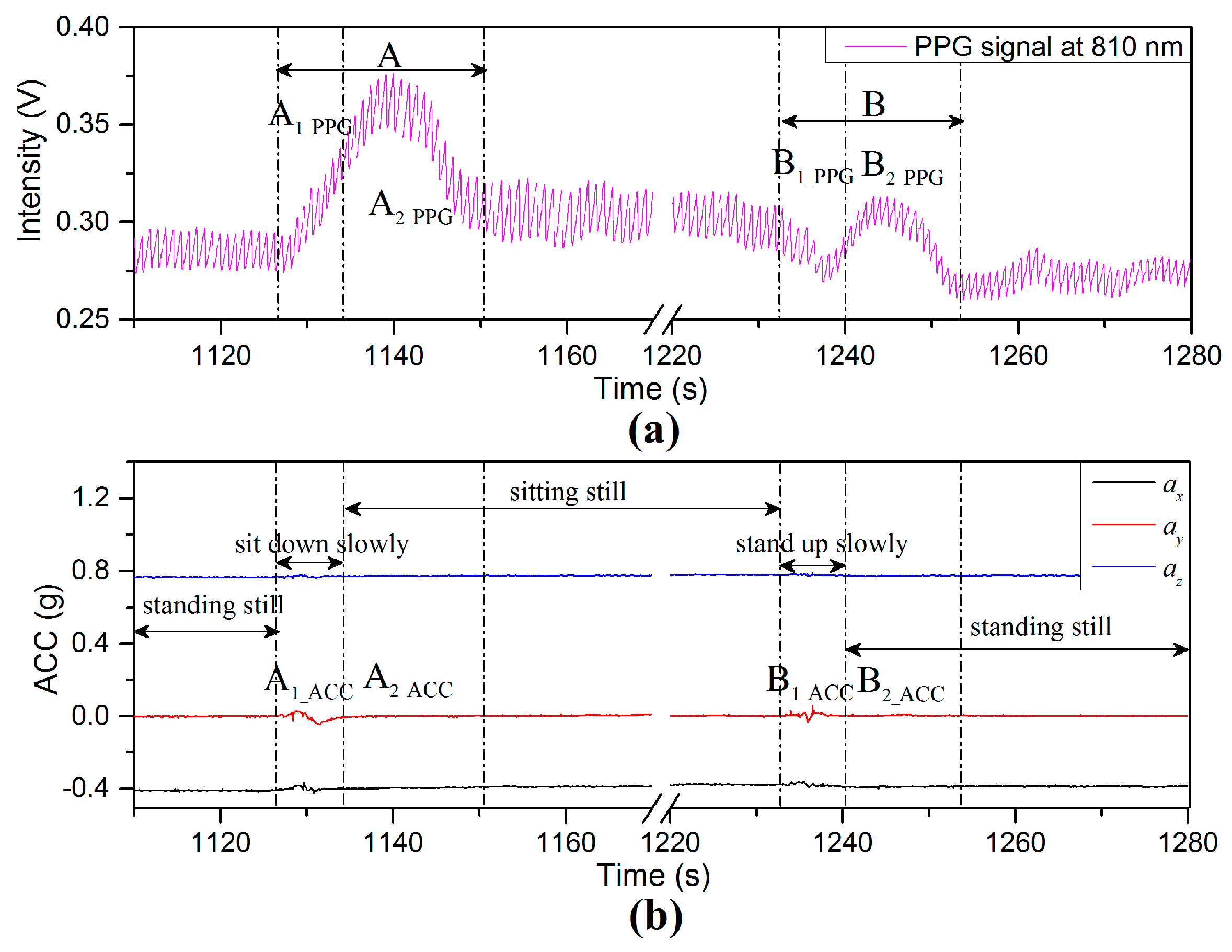
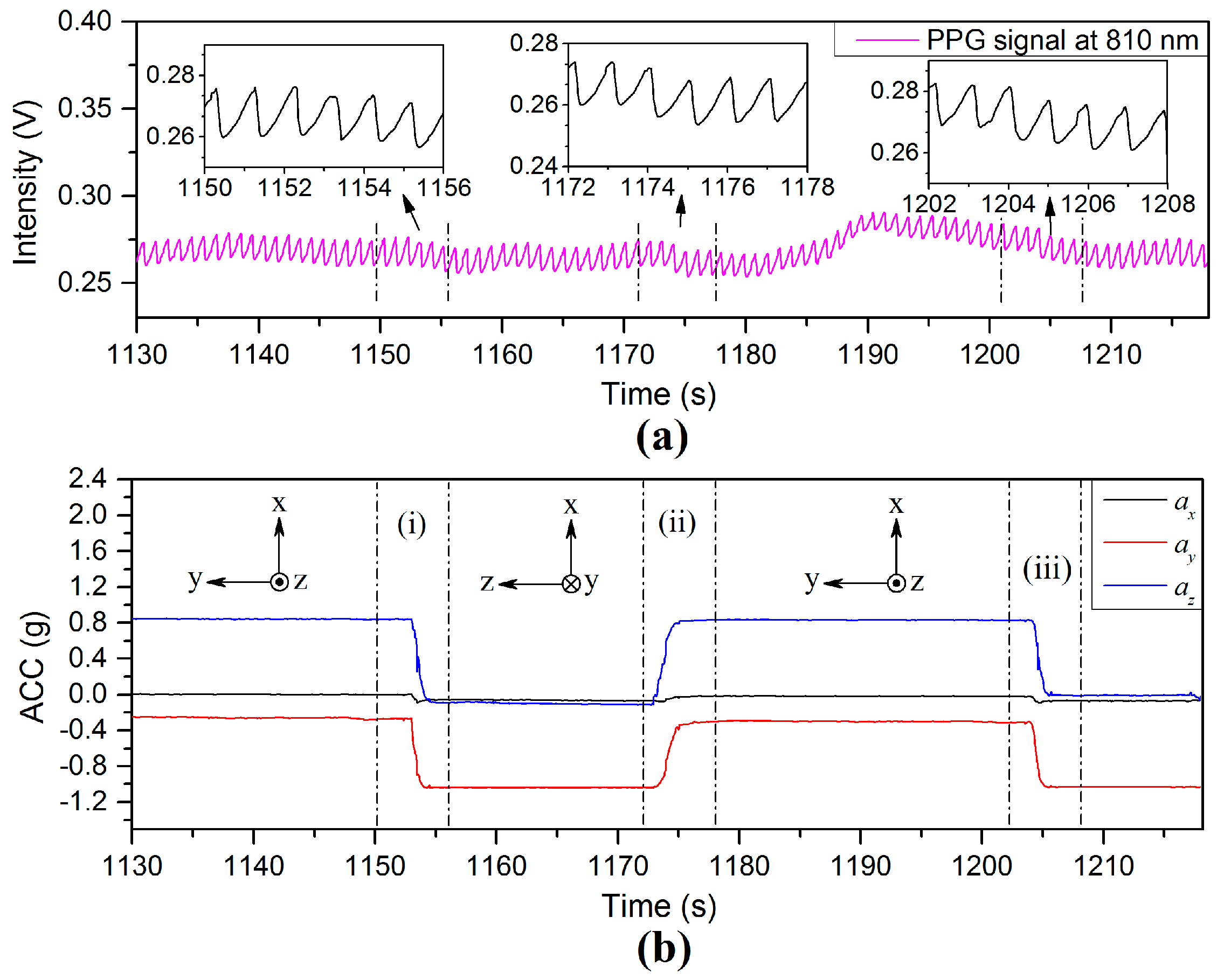
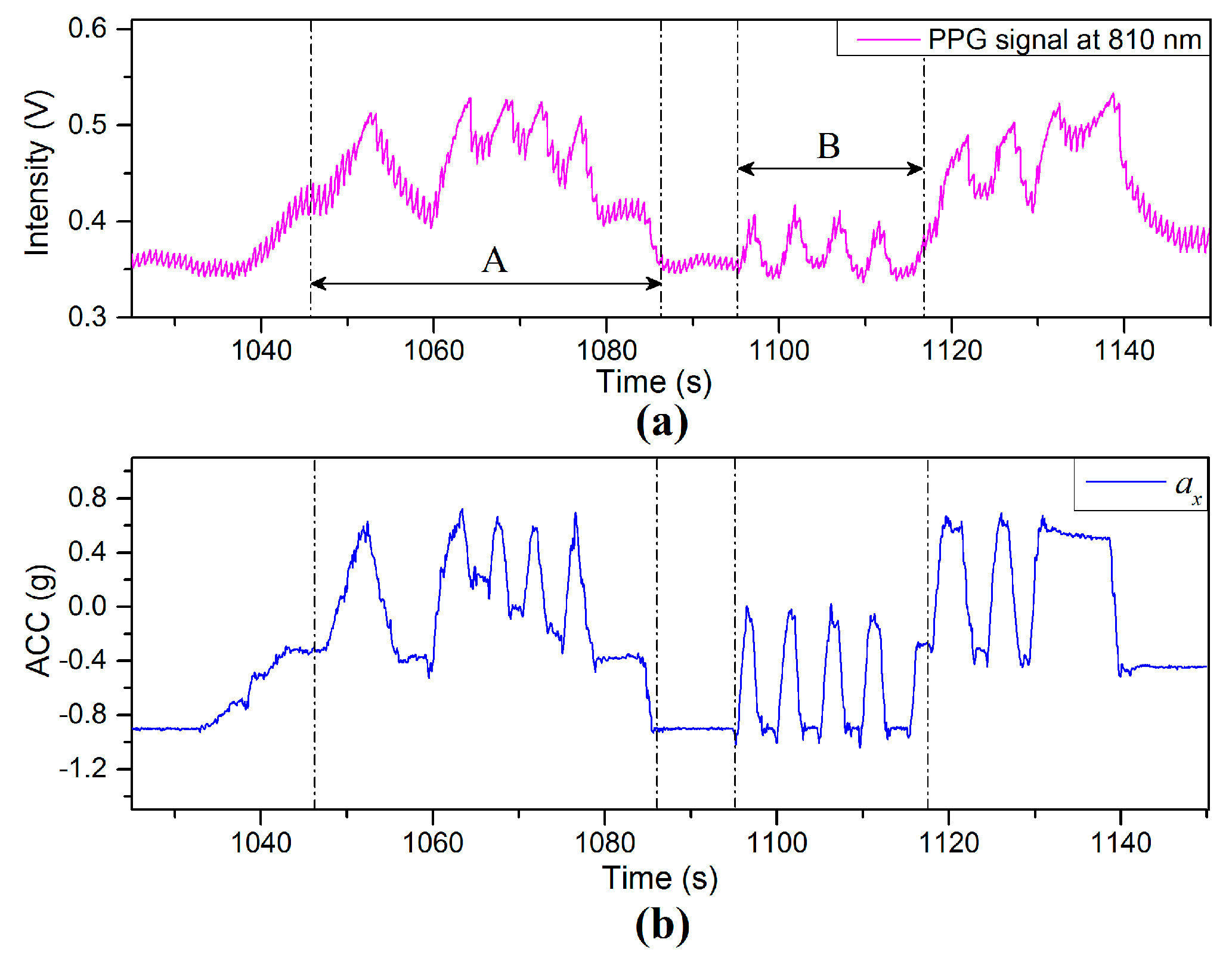
The details of the PPG and the ACC signals in the interval 1110–1280 s in
Figure 11 are represented in
Figure 12. The PPG fluctuation in Region (A) is the period from the rising edge of PPG signal to the start of a stable region. This interval can be divided into two regions for both signals:
and
for the ACC signals (
Figure 12b; and these are transposed to
and
for the PPG signal in the case of
Figure 12a. Region (
) defines the total interval during which the body position was changed from the standing to the sitting position. The decrease of VHD between the finger sensor probe and heart level is 25 cm due only to change of body position (while the finger sensor probe was kept still and stayed at the same height above the floor). The BP near the finger sensor probe decreases with decreasing negative VHD deviation according to the previous result in
Section 3.2 and the increase of BL according to the previous result in
Figure 9, as shown by the region
in
Figure 12a. Region
(
Figure 12b, is the interval where the accelerometer on the finger sensor probe detects only limited or no acceleration due to motion, while the BL of component
initially increases (dominated by the sympathetic part of the ANS) and then decreases (dominated by the parasympathetic part) during which time the homeostasis process is recovered via the ANS [
20,
24].
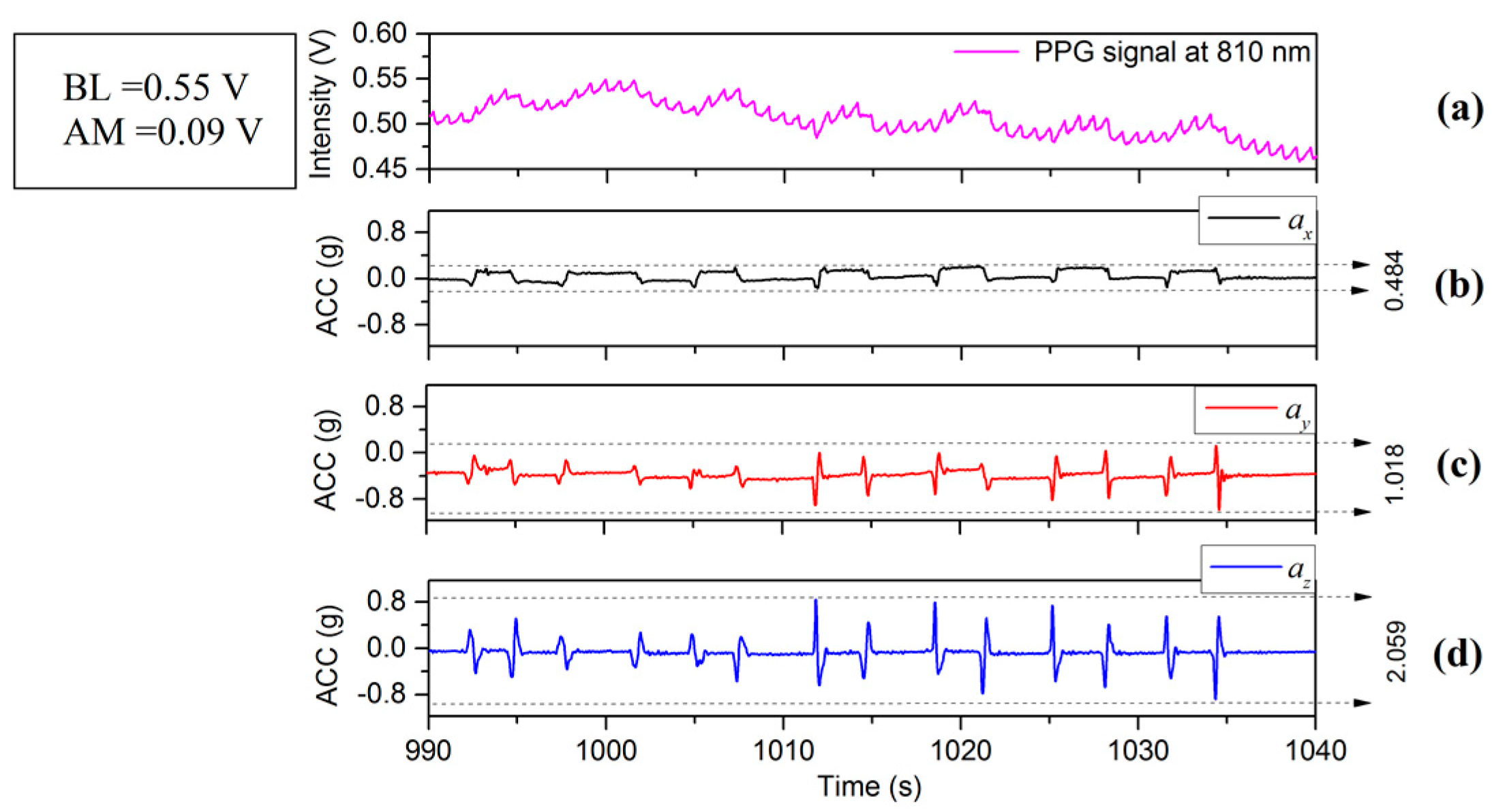
Region (B) in
Figure 12 is the interval from the decreasing edge of the PPG signal to where it stabilizes again. This interval can be divided into two regions for both signals:
and
for the ACC signals;
and
for the PPG signal. Region (
) is the interval during which the body position was changed from sitting to standing position. The increase of VHD is 25 cm (while the finger sensor probe was kept still and stayed at the same height above the floor). The BP falls with the decrease of VHD (consistent with the data of
Figure 9), leading to the decrease of BL, as shown by region (
). Region (
) defines the interval where the accelerometer on the finger sensor probe detects limited or no acceleration due to motion, while the BL of component
firstly increases (dominated by sympathetic part of the ANS) and then decreases (dominated by parasympathetic part) during which time the homeostasis process is recovered via the ANS. The PPG fluctuation observed in region (B) is dominant and is induced by body position variations (governed by BP changes from hydrostatic changes in the body position variation) compared with increase of negative VHD deviation accompanied with blood volume changes and hydrostatic changes (increase of BP near the finger sensor probe induced by the VHD variation). Clearly, BL variations of components
and
are not affected by motion but by the increase of the BP at the point of measurement. It is conjectured that changing the body position leads to a physiological variation with hydrostatic pressure changes, resulting in an increase of BP, which stimulates a response of the ANS [
2,
20].
4.2.2. Changes in the Breathing Pattern
PPG signals are sensitive to physiological variations; several examples are given in the literature [
2], such as changes in the breathing pattern, coughing or yawning. Similar experiments were conducted for the current investigation and detailed results include the PPG waveforms resulting from these tests.
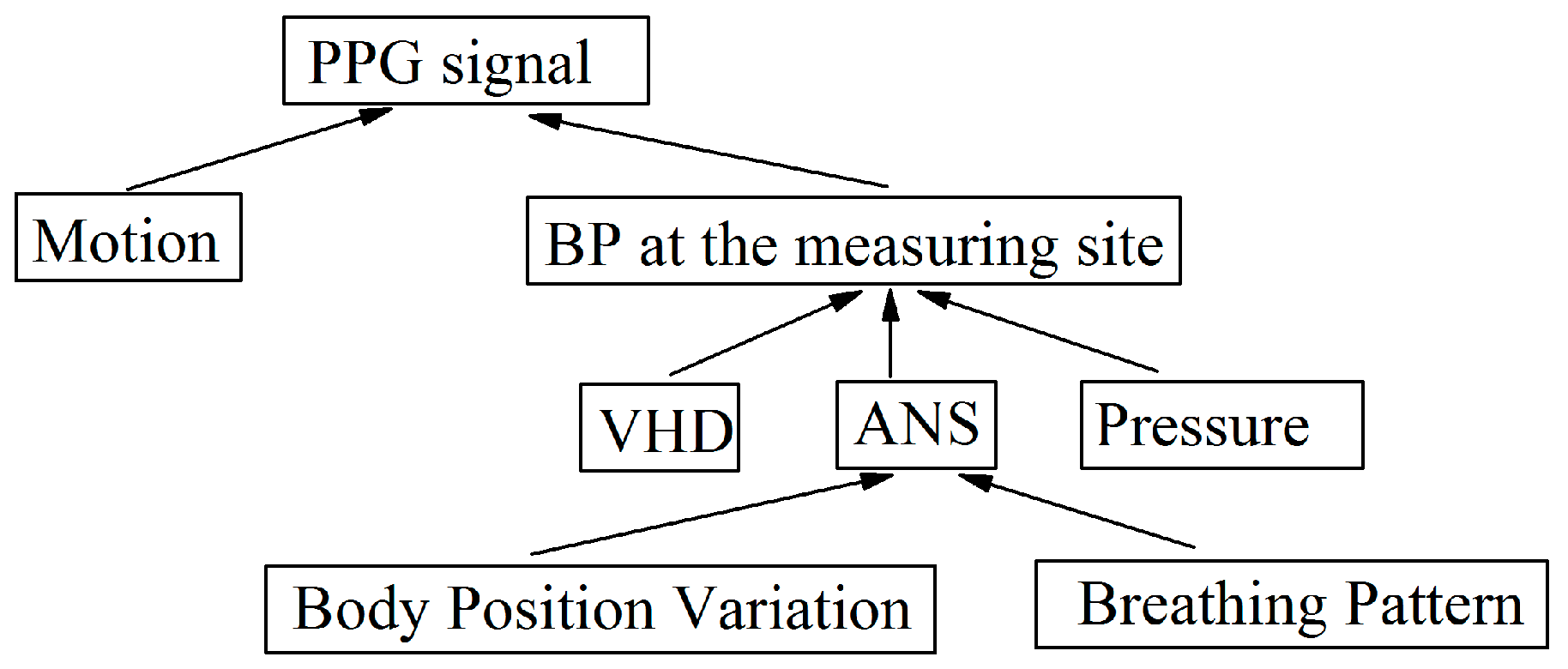
Many types of physiological influences can result in an increase, or decrease of the local BP at the measuring site, which affects the BL and the AM of the PPG signals.
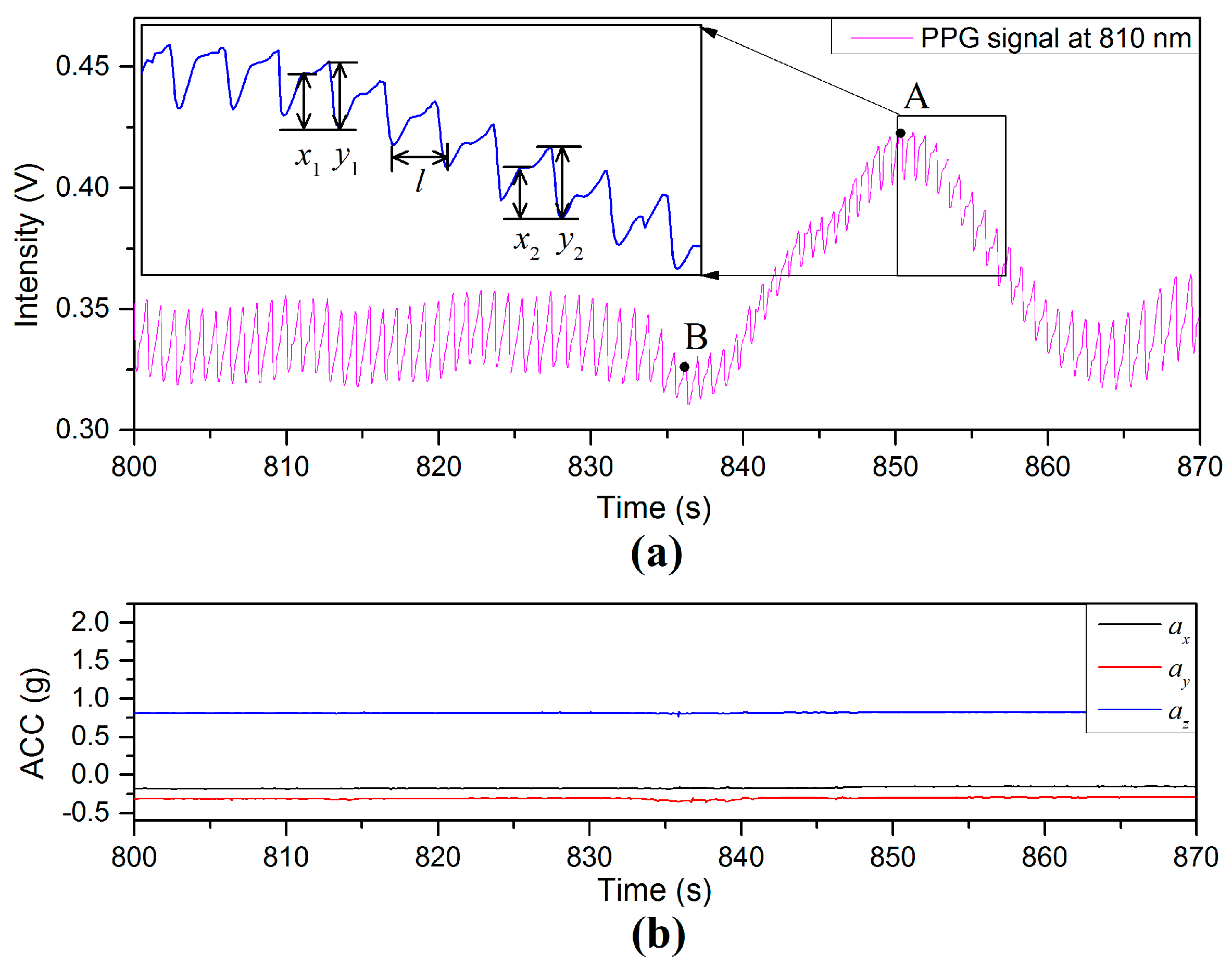
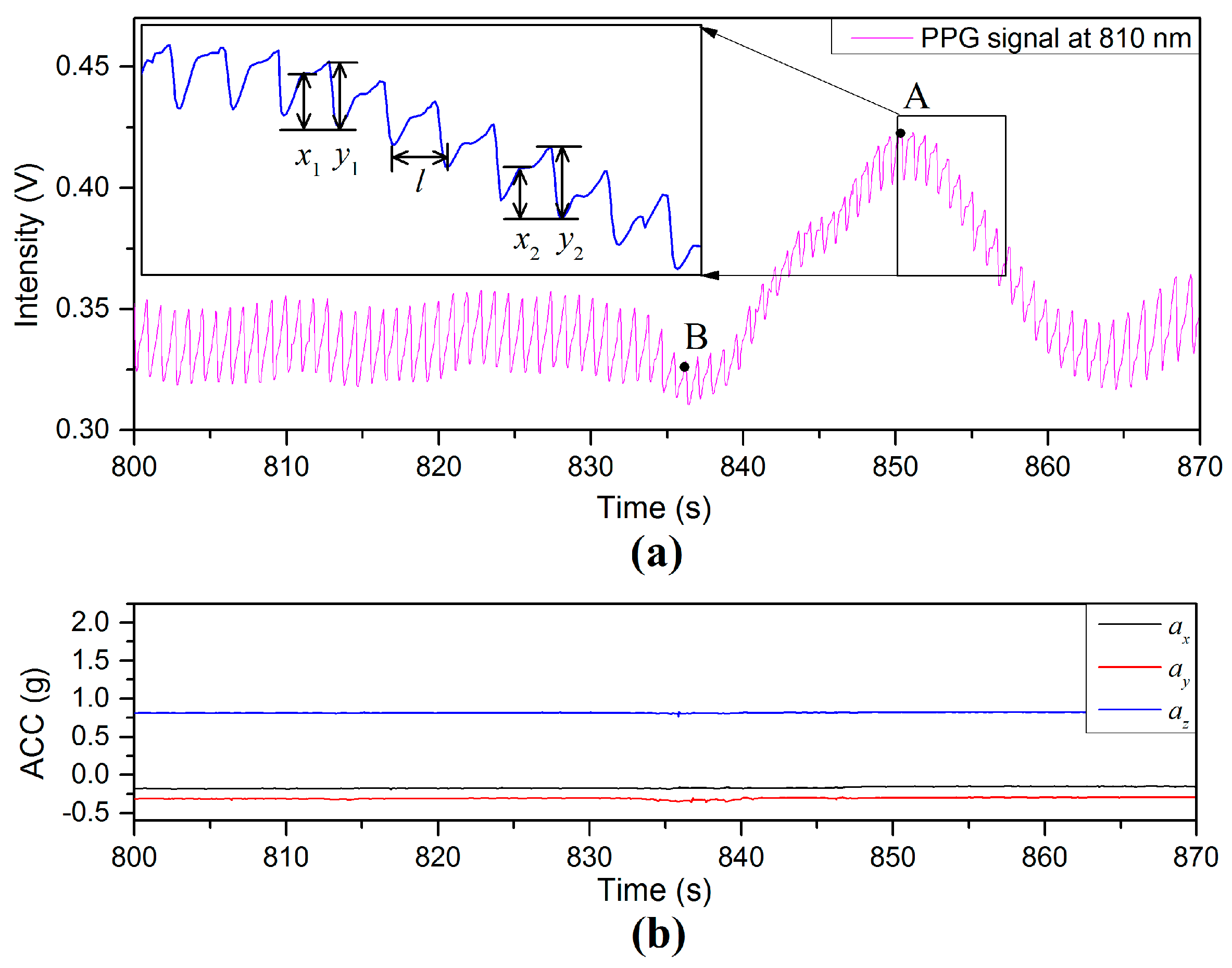
Figure 13 illustrates PPG and acceleration signals during a deep yawn event. As can been seen from the intensity of PPG signal in
Figure 13a, the average value of BL is 0.35 V before the deep yawn. The activity of a deep yawn started at the time of 835 s. The next 25 s shows a PPG-fluctuation triggered by the yawn event. Repeated experiments (40 times) show that: (1) the value of AM tends to be restricted and (2) the BL tends to continue without significant variation. A zoomed PPG signal in the time period of 852–857 s is included as an inset on the top left of
Figure 13a. The interval
is the instantaneous period of the PPG waveform, at a given point in time, and has been used to determine HR. Two examples of the AM of the diastolic peak are illustrated by
and
, whereas
and
are examples of the AM of the systolic peaks [
25]. The mean ratio of diastolic peak to systolic peak during the period 810–830 s is 0.403 (±0.023) in
Figure 13 prior to the yawning event. During the yawning event, the value of the ratio
(e.g., 0.83 at the peak point, A) is larger than that of
(e.g., 0.52 at the valley point, B), and the BL/AM ratio is also affected during the PPG fluctuation. Even though the PPG signal is highly affected by the yawn activity, the interval
can still be reliably used to calculate HR [
26,
27].
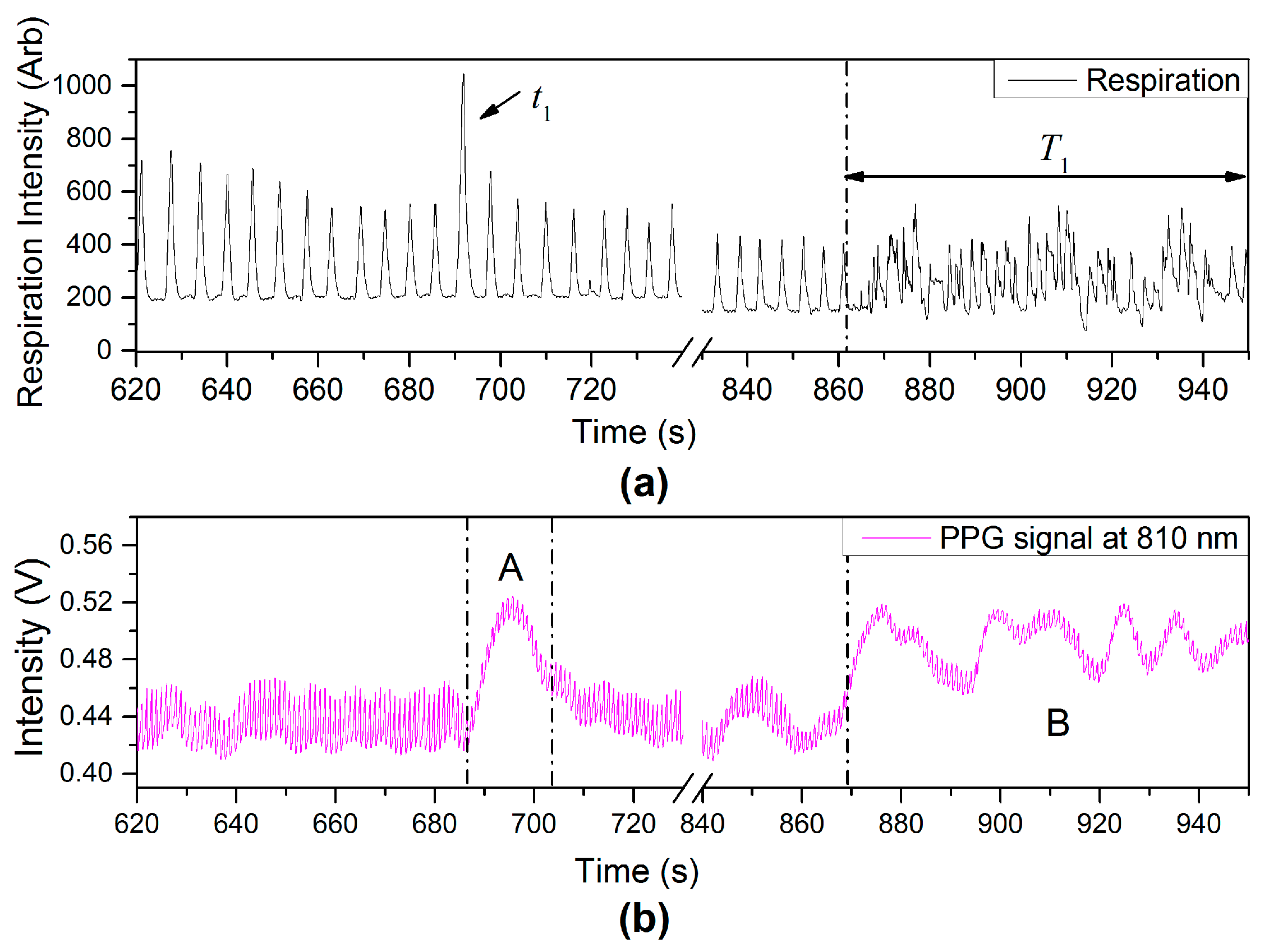
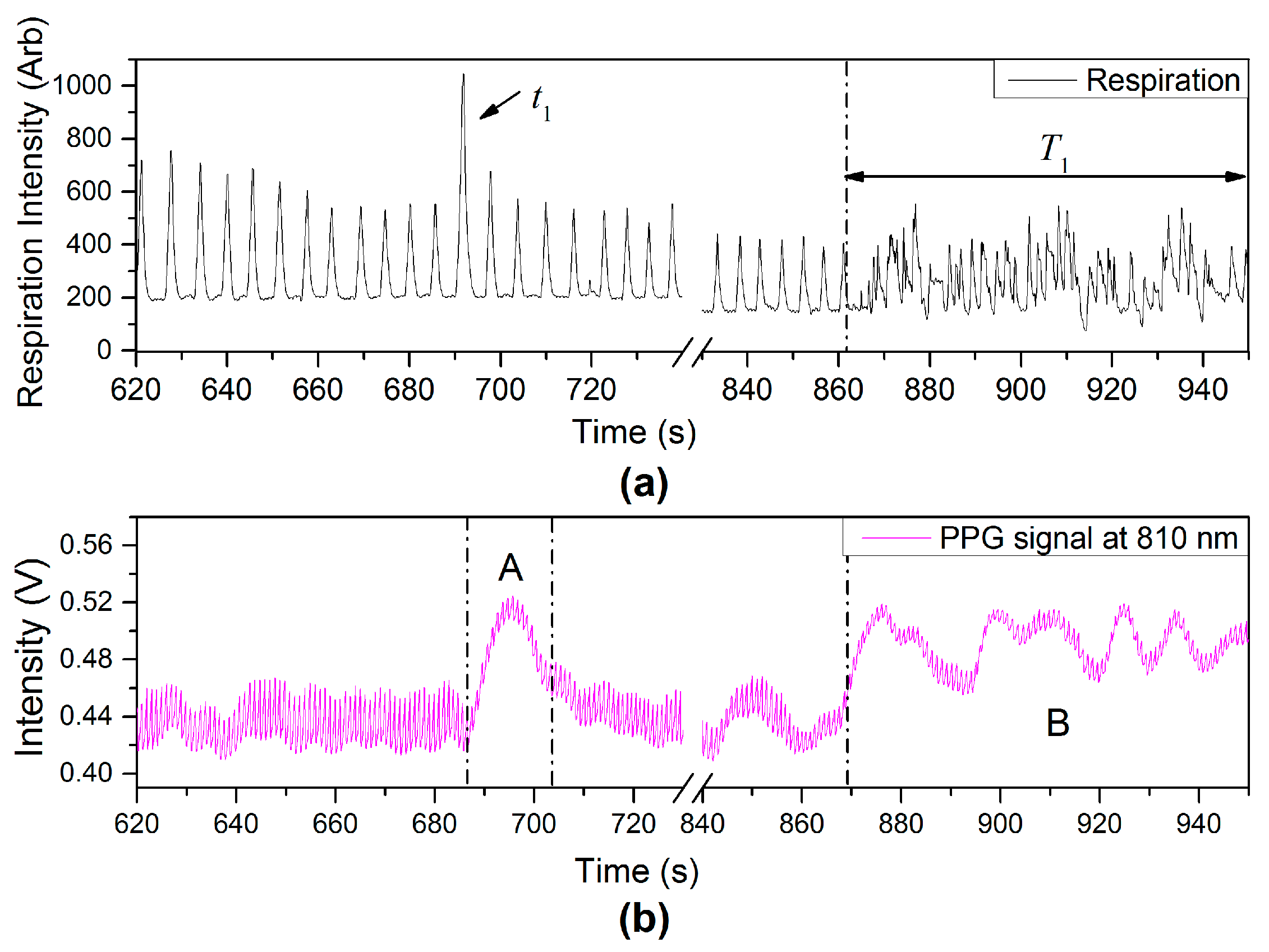
Another type of physiological variation from variation of breathing pattern, deep breathing (
) and talking (
) events, can also affect the PPG signals as observed in PPG-fluctuations [region (A) and (B)], shown in
Figure 14.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}