

Association Between Tissue Accumulation of Skin Autofluorescence, Disease, and Exercise Capacity in Older Adults


Abstract
1. Introduction
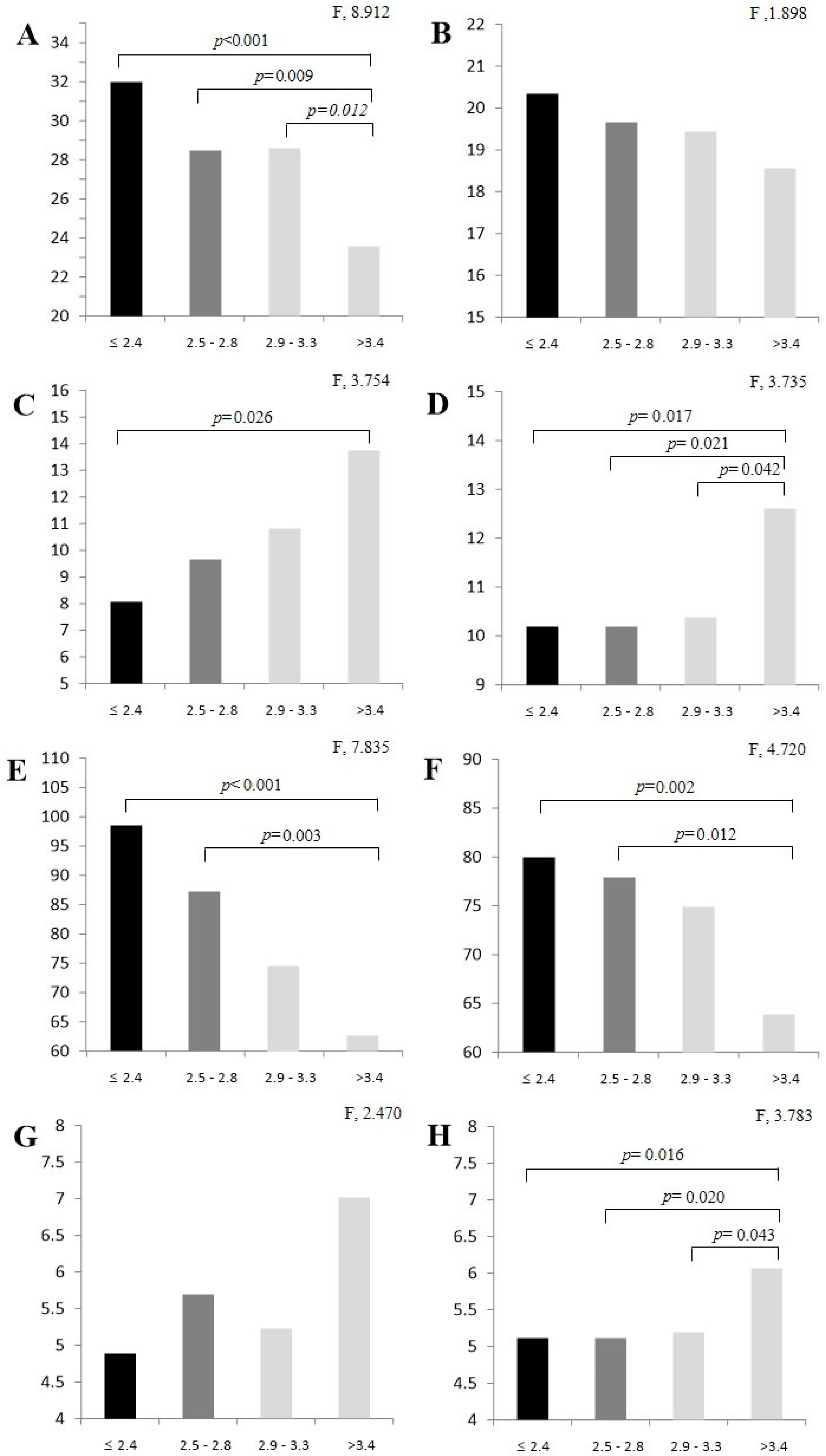
2. Results
3. Discussion
4. Materials and Methods
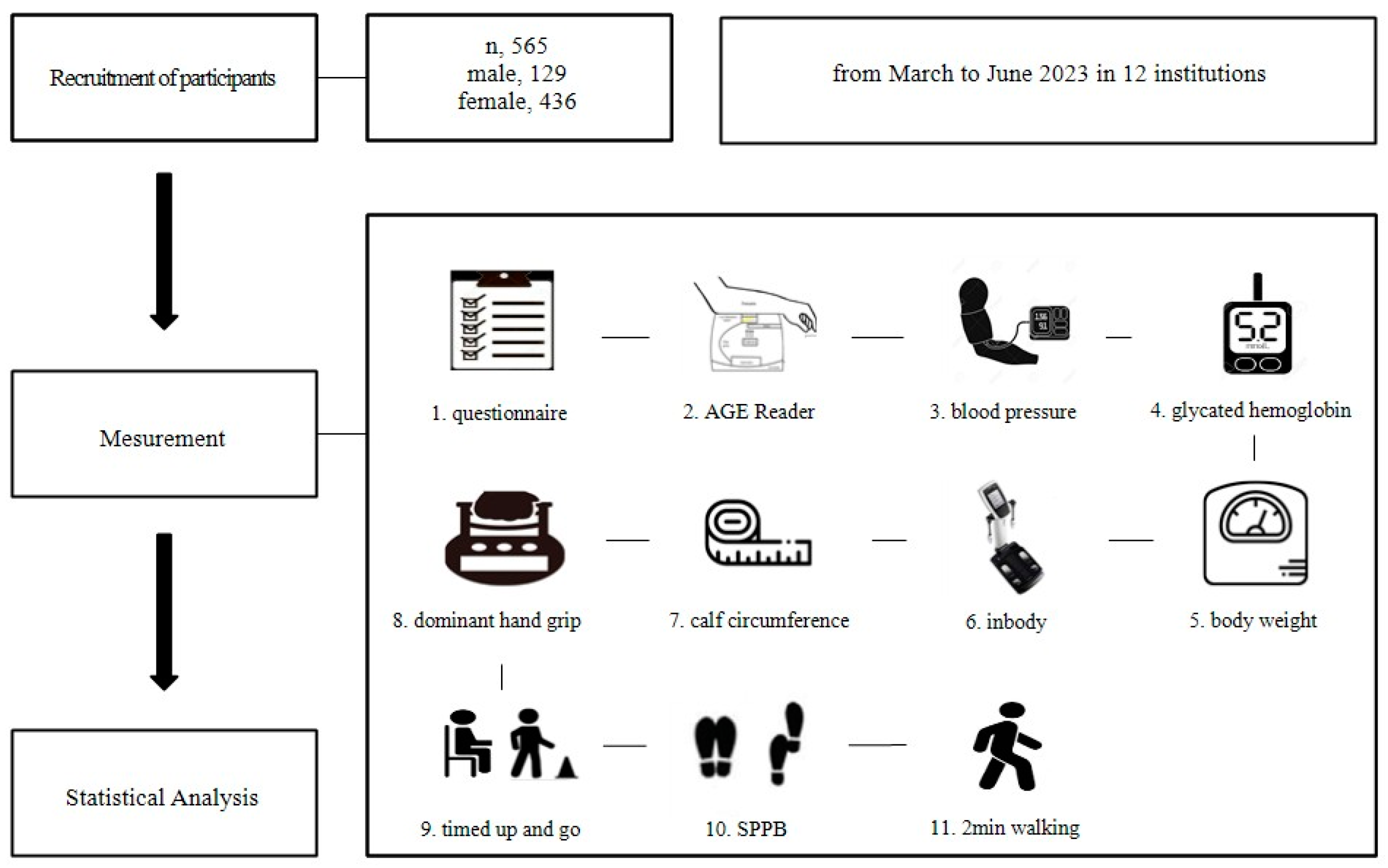
4.1. Participants
4.2. Study Design
4.3. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AGE | Advanced glycation end product |
| ANOVA | Analysis of variance |
| AMPK | Activated protein kinase |
| ASM | Appendicular skeletal muscle |
| AU | Arbitrary units |
| BMI | Body mass index |
| CC | Calf circumference |
| DHG | Dominant hand grip |
| DM | Diabetes mellitus |
| HbA1c | Glycated hemoglobin |
| GLUT-4 | Glucose transporter-4 |
| IL-6 | Interleukin 6 |
| NFκB | Nuclear factor kappa B |
| MuRF1 | Muscle RING-finger protein-1 |
| PI-3 | Phosphoinositide-3 |
| SAF | Skin autofluorescence |
| SPPB | Short physical performance battery |
| TNF-α | Tumor necrosis factor-α |
| TUG | Timed up-and-go |
References
- Twarda-Clapa, A.; Olczak, A.; Białkowska, A.M.; Koziołkiewicz, M. Advanced glycation end-products (AGEs): Formation, chemistry, classification, receptors, and diseases related to AGEs. Cells 2022, 11, 1312. [Google Scholar] [CrossRef] [PubMed]
- Mulder, D.J.; Water, T.V.; Lutgers, H.L.; Graaff, R.; Gans, R.O.; Zijlstra, F.; Smit, A.J. Skin autofluorescence, a novel marker for glycemic and oxidative stress-derived advanced glycation endproducts: An overview of current clinical studies, evidence, and limitations. Diabetes Technol. Ther. 2006, 8, 523–535. [Google Scholar] [PubMed]
- Calviño, J.; Cigarran, S.; Gonzalez-Tabares, L.; Menendez, N.; Latorre, J.; Cillero, S.; Millan, B.; Cobelo, C.; Sanjurjo-Amado, A.; Quispe, J.; et al. Advanced glycation end products (AGEs) estimated by skin autofluorescence are related with cardiovascular risk in renal transplant. PLoS ONE 2018, 13, e0201118. [Google Scholar]
- Vlassara, H.; Uribarri, J. Advanced glycation end products (AGE) and diabetes: Cause, effect, or both? Curr. Diabetes Rep. 2014, 14, 453. [Google Scholar]
- Nabi, R.; Alvi, S.S.; Khan, R.H.; Ahmad, S.; Ahmad, S.; Khan, M.S. Antiglycation study of HMG-R inhibitors and tocotrienol against glycated BSA and LDL: A comparative study. Int. J. Biol. Macromol. 2018, 116, 983–992. [Google Scholar]
- Peker, T.; Boyraz, B. The Relationship between Resistant Hypertension and Advanced Glycation End-Product Levels Measured Using the Skin Autofluorescence Method: A Case-Control Study. J. Clin. Med. 2023, 12, 6606. [Google Scholar]
- Kunimoto, M.; Yokoyama, M.; Shimada, K.; Matsubara, T.; Aikawa, T.; Ouchi, S.; Fukao, K.; Miyazaki, T.; Fujiwara, K.; Abulimiti, A.; et al. Relationship between skin autofluorescence levels and clinical events in patients with heart failure undergoing cardiac rehabilitation. Cardiovasc. Diabetol. 2021, 20, 208. [Google Scholar]
- Kunimoto, M.; Shimada, K.; Yokoyama, M.; Matsubara, T.; Aikawa, T.; Ouchi, S.; Shimizu, M.; Fukao, K.; Miyazaki, T.; Kadoguchi, T.; et al. Association between the tissue accumulation of advanced glycation end products and exercise capacity in cardiac rehabilitation patients. BMC Cardiovasc. Disord. 2020, 20, 195. [Google Scholar]
- Dalal, M.; Ferrucci, L.; Sun, K.; Beck, J.; Fried, L.P.; Semba, R.D. Elevated serum advanced glycation end products and poor grip strength in older community-dwelling women. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 132–137. [Google Scholar]
- Semba, R.D.; Bandinelli, S.; Sun, K.; Guralnik, J.M.; Ferrucci, L. Relationship of an advanced glycation end product, plasma carboxymethyl-lysine, with slow walking speed in older adults: The InCHIANTI study. Eur. J. Appl. Physiol. 2010, 108, 191–195. [Google Scholar]
- Atzeni, I.M.; van de Zande, S.C.; Westra, J.; Zwerver, J.; Smit, A.J.; Mulder, D.J. The AGE Reader: A non-invasive method to assess long-term tissue damage. Methods 2022, 203, 533–541. [Google Scholar] [PubMed]
- Cleary, P.A.; Braffett, B.H.; Orchard, T.; Lyons, T.J.; Maynard, J.; Cowie, C.; Gubitosi-Klug, R.A.; Way, J.; Anderson, K.; Barnie, A.; et al. Clinical and technical factors associated with skin intrinsic fluorescence in subjects with type 1 diabetes from the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study. Diabetes Technol. Ther. 2013, 15, 466–474. [Google Scholar] [PubMed]
- Januszewski, A.S.; Xu, D.; Cho, Y.H.; Benitez-Aguirre, P.Z.; O’Neal, D.N.; Craig, M.E.; Donaghue, K.C.; Jenkins, A.J. Skin autofluorescence in people with type 1 diabetes and people without diabetes: An eight-decade cross-sectional study with evidence of accelerated aging and associations with complications. Diabet. Med. 2021, 38, e14432. [Google Scholar] [PubMed]
- Yozgatli, K.; Lefrandt, J.D.; Noordzij, M.J.; Oomen, P.H.N.; Brouwer, T.; Jager, J.; Castro Cabezas, M.; Smit, A.J. Accumulation of advanced glycation end products is associated with macrovascular events and glycaemic control with microvascular complications in type 2 diabetes mellitus. Diabet. Med. 2018, 35, 1242–1248. [Google Scholar]
- Mesinovic, J.; Zengin, A.; De Courten, B.; Ebeling, P.R.; Scott, D. Sarcopenia and type 2 diabetes mellitus: A bidirectional relationship. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1057–1072. [Google Scholar]
- Haddad, F.; Zaldivar, F.; Cooper, D.M.; Adams, G.R. IL-6-induced skeletal muscle atrophy. J. Appl. Physiol. 2005, 98, 911–917. [Google Scholar]
- Lee, M.J.; Sung, J.-Y.; Kim, J. Effect of Low-Intensity High-Repetition Versus High-Intensity Low-Repetition Elastic Band Resistance Training on Functional Physical Fitness and Myokine Levels in Older Adults. Appl. Sci. 2025, 15, 757. [Google Scholar] [CrossRef]
- Sung, J.-Y.; Lee, M.J.; Kim, J. Relationship Between Lifestyle and Physical Fitness Among Older Women with Sarcopenia. Int. J. Mol. Sci. 2025, 26, 2205. [Google Scholar] [CrossRef]
- Purnamasari, D.; Tetrasiwi, E.N.; Kartiko, G.J.; Astrella, C.; Husam, K.; Laksmi, P.W. Sarcopenia and chronic complications of type 2 diabetes mellitus. Rev. Diabet. Stud. 2022, 18, 157–165. [Google Scholar]
- Russell, S.T.; Rajani, S.; Dhadda, R.S.; Tisdale, M.J. Mechanism of induction of muscle protein loss by hyperglycaemia. Exp. Cell Res. 2009, 315, 16–25. [Google Scholar]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [PubMed]
- Yang, M.; Lu, J.; Jiang, J.; Zeng, Y.; Tang, H. Comparison of four sarcopenia screening tools in nursing home residents. Aging Clin. Exp. Res. 2019, 31, 1481–1489. [Google Scholar]
- Pingitore, A.; Lima, G.P.P.; Mastorci, F.; Quinones, A.; Iervasi, G.; Vassalle, C. Exercise and oxidative stress: Potential effects of antioxidant dietary strategies in sports. Nutrition 2015, 31, 916–922. [Google Scholar] [PubMed]
- Chen, C.Y.; Tseng, W.C.; Yang, Y.H.; Chen, C.L.; Lin, L.L.; Chen, F.P.; Wong, A.M.K. Calf circumference as an optimal choice of four screening tools for sarcopenia among ethnic Chinese older adults in assisted living. Clin. Interv. Aging 2020, 15, 2415–2422. [Google Scholar] [PubMed]
- Hjerrild, J.N.; Wobbe, A.; Stausholm, M.B.; Larsen, A.E.; Josefsen, C.O.; Malmgaard-Clausen, N.M.; Dela, F.; Kjaer, M.; Magnusson, S.P.; Hansen, M.; et al. Effects of long-term physical activity and diet on skin glycation and Achilles tendon structure. Nutrients 2019, 11, 1409. [Google Scholar] [CrossRef]
- Duda-Sobczak, A.; Falkowski, B.; Araszkiewicz, A.; Zozulinska-Ziolkiewicz, D. Association between self-reported physical activity and skin autofluorescence, a marker of tissue accumulation of advanced glycation end products in adults with Type 1 diabetes: A cross-sectional study. Clin. Ther. 2018, 40, 872–880. [Google Scholar]
- Atzeni, I.M.; Boersema, J.; Pas, H.H.; Diercks, G.F.H.; Scheijen, J.L.J.M.; Schalkwijk, C.G.; Mulder, D.J.; van der Zee, P.; Smit, A.J. Is skin autofluorescence (SAF) representative of dermal advanced glycation endproducts (AGEs) in dark skin? A pilot study. Heliyon 2020, 6, e05364. [Google Scholar]

{kind=link}
{kind=link}
| Variables | Male | % | Female | % | |
|---|---|---|---|---|---|
| Age (years) | 60–69 | 24 | 18.6 | 101 | 23.2 |
| 70–79 | 43 | 33.3 | 167 | 38.3 | |
| 80–89 | 55 | 42.6 | 149 | 34.2 | |
| <90 | 7 | 5.5 | 19 | 4.3 | |
| Height (cm) | ~155.9 | 26 | 20.2 | 412 | 94.5 |
| 160–164.9 | 45 | 34.9 | 20 | 4.7 | |
| 165–169.9 | 30 | 23.2 | 3 | 0.6 | |
| <170 | 28 | 21.7 | 1 | 0.2 | |
| Weight (kg) | ~44.9 | 3 | 2.3 | 40 | 9.2 |
| 45–54.9 | 13 | 10.1 | 153 | 35.1 | |
| 55–64.9 | 49 | 38.0 | 165 | 37.8 | |
| 65–74.9 | 42 | 32.5 | 52 | 11.9 | |
| <75 | 22 | 17.1 | 26 | 6.0 | |
| Body fat mass (%) | ~19.9 | 4 | 3.1 | 24 | 5.5 |
| 20–29.9 | 32 | 24.8 | 99 | 22.7 | |
| 30–39.9 | 51 | 39.6 | 217 | 49.8 | |
| <40 | 42 | 32.5 | 96 | 22.0 | |
| BMI (kg/m2) | ~18.5 | 3 | 2.3 | 17 | 3.9 |
| 18.6–24.9 | 81 | 62.9 | 231 | 53.0 | |
| 25–29.9 | 42 | 32.5 | 152 | 34.8 | |
| <30 | 3 | 2.3 | 36 | 8.3 | |
| ASM (kg) | ~5.9 | 5 | 3.9 | 239 | 54.8 |
| 6–8.9 | 120 | 93.0 | 195 | 44.7 | |
| <9 | 4 | 3.1 | 2 | 0.5 | |
| Diabetes | Yes | 43 | 33.3 | 131 | 30.1 |
| No | 86 | 66.7 | 305 | 69.9 | |
| Hypertension | Yes | 62 | 48.1 | 240 | 55.0 |
| No | 67 | 51.9 | 196 | 45.0 | |
| Hyperlipidemia | Yes | 38 | 29.5 | 173 | 39.7 |
| No | 91 | 70.5 | 263 | 60.3 | |
| total | 129 | 100 | 436 | 100 | |
| Variable Category | Male = 129 | Female = 436 | |||
|---|---|---|---|---|---|
| OR (95% CI) and p | |||||
| HbA1c (mg/dL) | ≤2.4 | Reference | |||
| 2.5–2.8 | 0.920 (0.457~1.854) | 0.056 | 0.968 (0.710~1.320) | 0.839 | |
| 2.9–3.3 | 1.094 (0.564~2.124) | 0.079 | 1.111 (0.824~1.498) | 0.491 | |
| >3.4 | 0.807 (0.393~1.657) | 0.598 | 1.878 (1.411~2.501) *** | <0.001 | |
| ASM (kg) | ≤2.4 | Reference | |||
| 2.5–2.8 | 1.671 (0.456~6.128) | 0.439 | 1.129 (0.735~1.735) | 0.580 | |
| 2.9–3.3 | 2.759 (0.731~10.419) | 0.134 | 1.021 (0.661~1.579) | 0.924 | |
| >3.4 | 1.982 (0.551~7.121) | 0.295 | 0.637 (0.378~1.076) | 0.092 | |
| CC (cm) | ≤2.4 | Reference | |||
| 2.5–2.8 | 0.706 (0.492~1.013) | 0.059 | 0.978 (0.848~1.127) | 0.755 | |
| 2.9–3.3 | 0.680 (0.468~0.987) * | 0.043 | 0.913 (0.791~1.055) | 0.217 | |
| >3.4 | 0.647 (0.451~0.926) * | 0.017 | 1.088 (0.918~1.288) | 0.331 | |
| DHG (rep) | ≤2.4 | Reference | |||
| 2.5–2.8 | 0.893 (0.788~1.013) | 0.079 | 0.933 (0.876~0.994) * | 0.032 | |
| 2.9–3.3 | 0.949 (0.828~1.087) | 0.451 | 0.956 (0.898~1.019) | 0.164 | |
| >3.4 | 0.842 (0.740~0.958) ** | 0.009 | 0.965 (0.899~1.036) | 0.325 | |
| SPPB (rep and sec) | ≤2.4 | Reference | |||
| 2.5–2.8 | 2.179 (1.177~4.033) * | 0.013 | 1.549 (1.291~1.858) *** | <0.001 | |
| 2.9–3.3 | 1.758 (0.951~3.250) | 0.072 | 1.496 (1.250~1.789) *** | <0.001 | |
| >3.4 | 2.110 (1.159~3.839) * | 0.015 | 1.541 (1.266~1.875) *** | <0.001 | |
| TUG (rep) | ≤2.4 | Reference | |||
| 2.5–2.8 | 1.355 (0.878~2.090) * | 0.017 | 1.161 (0.971~1.193) | 0.161 | |
| 2.9–3.3 | 1.683 (1.064~2.660) * | 0.026 | 1.053 (0.950~1.167) | 0.327 | |
| >3.4 | 1.433 (0.936~2.194) | 0.098 | 1.073 (0.966~1.191) | 0.188 | |
| 2 min walking test (rep) | ≤2.4 | Reference | |||
| 2.5–2.8 | 0.984 (0.951~1.018) | 0.343 | 0.989 (0.977~1.001) | 0.065 | |
| 2.9–3.3 | 0.968 (0.936~1.002) | 0.065 | 0.987 (0.976~0.999) * | 0.035 | |
| >3.4 | 0.962 (0.931~0.995) * | 0.022 | 0.979 (0.966~0.992) ** | 0.002 | |
| Gait speed (sec) | ≤2.4 | Reference | |||
| 2.5–2.8 | 1.025 (0.523~2.009) | 0.942 | 1.071 (0.837~1.370) | 0.585 | |
| 2.9–3.3 | 0.503 (0.228~1.107) | 0.088 | 1.103 (0.863~1.410) | 0.433 | |
| >3.4 | 0.837 (0.434~1.614) | 0.595 | 1.118 (0.869~1.439) | 0.387 | |
| Variable Category | (a) Model 1 | (b) Model 2 | (c) Model 3 | ||||
|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||
| SAF | ≤2.4 | Reference | |||||
| 2.5–2.8 | 1.008 (0.999~1.017) | 0.073 | 1.346 (0.522~3.471) | 0.239 | 1.002 (0.998~1.005) | 0.539 | |
| 2.9–3.3 | 1.006 (0.996~1.015) | 0.239 | 2.154 (0.879~5.294) | 0.239 | 1.001 (0.997~1.005) | 0.669 | |
| >3.4 | 1.018 (1.009~1.027) | <0.001 *** | 2.639 (1.054~6.608) | 0.038 * | 1.004 (1.000~1.007) | 0.035 * | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, J.-Y.; Kim, J. Association Between Tissue Accumulation of Skin Autofluorescence, Disease, and Exercise Capacity in Older Adults. Int. J. Mol. Sci. 2025, 26, 2913. https://doi.org/10.3390/ijms26072913
Sung J-Y, Kim J. Association Between Tissue Accumulation of Skin Autofluorescence, Disease, and Exercise Capacity in Older Adults. International Journal of Molecular Sciences. 2025; 26(7):2913. https://doi.org/10.3390/ijms26072913
Chicago/Turabian StyleSung, Jun-Young, and Jiyoun Kim. 2025. "Association Between Tissue Accumulation of Skin Autofluorescence, Disease, and Exercise Capacity in Older Adults" International Journal of Molecular Sciences 26, no. 7: 2913. https://doi.org/10.3390/ijms26072913
APA StyleSung, J.-Y., & Kim, J. (2025). Association Between Tissue Accumulation of Skin Autofluorescence, Disease, and Exercise Capacity in Older Adults. International Journal of Molecular Sciences, 26(7), 2913. https://doi.org/10.3390/ijms26072913