
Action of Platelet-Rich Plasma on In Vitro Cellular Bioactivity: More than Platelets

 ,
,
Abstract
1. Introduction
2. Results
2.1. Platelet-Rich Plasma and Platelet-Poor Plasma Characterization
2.2. Comparison between Platelet-Rich Plasma and Platelet-Poor Plasma
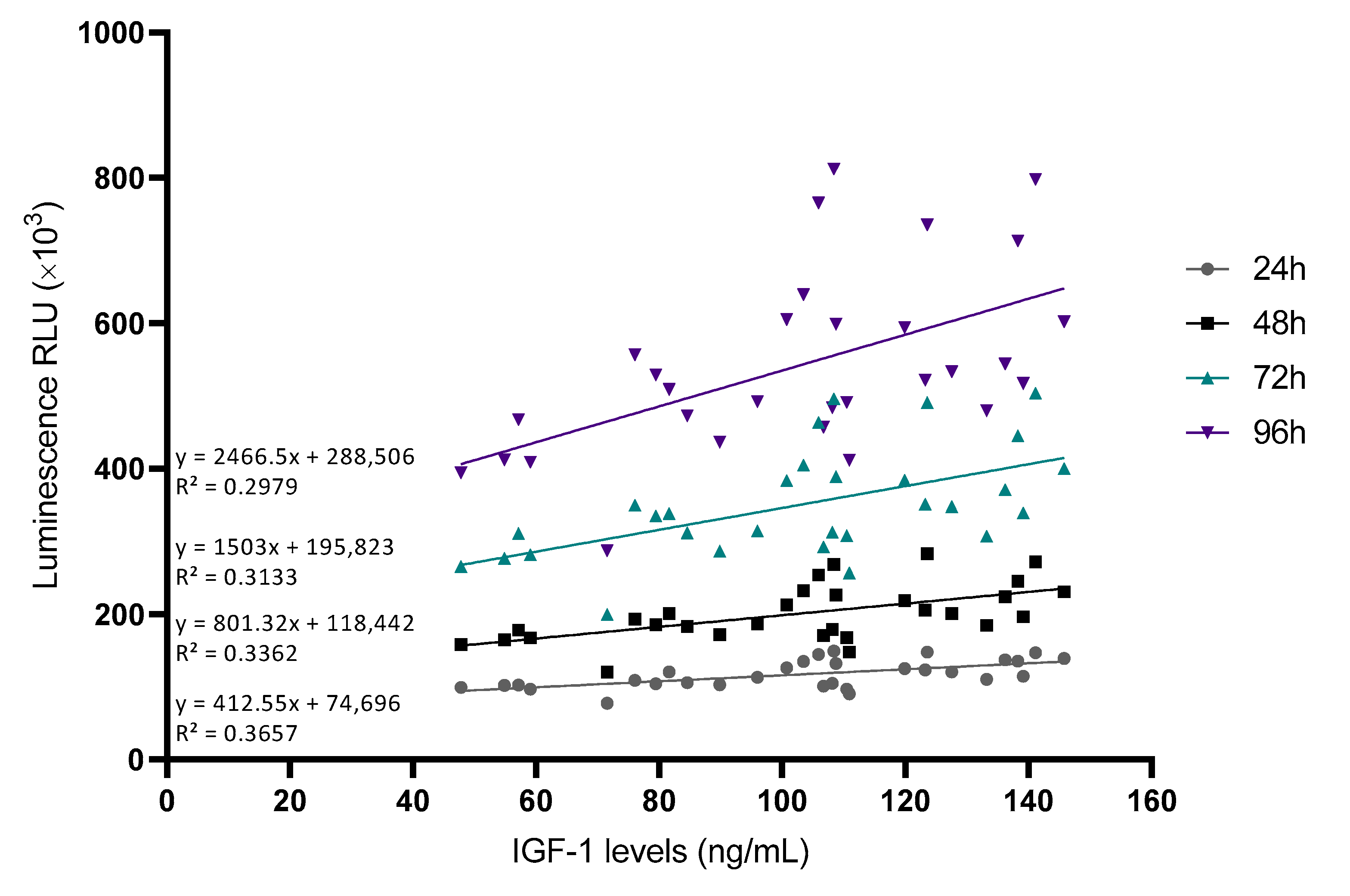
2.3. Analysis of the Effect of Platelet-Rich Plasma Growth Factors on Cell Proliferation
3. Discussion
4. Materials and Methods
4.1. Sample Collection
4.2. Platelet-Rich Plasma and Platelet-Poor Plasma Preparation
4.3. Platelet-Rich Plasma and Platelet-Poor Plasma Characterization
4.4. Enzyme-Linked Immunosorbent Assay (ELISA)
4.5. Cell Cultures
4.6. Cell Viability Assay
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anitua, E.; Prado, R.; Sánchez, M.; Orive, G. Platelet-Rich Plasma: Preparation and Formulation. Oper. Tech. Orthop. 2012, 22, 25–32. [Google Scholar] [CrossRef]
- Cui, Y.; Lin, L.; Wang, Z.; Wang, K.; Xiao, L.; Lin, W.; Zhang, Y. Research Trends of Platelet-Rich Plasma Therapy on Knee Osteoarthritis from 2011 to 2021: A Review. Medicine 2023, 102, e32434. [Google Scholar] [CrossRef]
- Anitua, E.; Muruzabal, F.; de la Fuente, M.; Merayo, J.; Durán, J.; Orive, G. Plasma Rich in Growth Factors for the Treatment of Ocular Surface Diseases. Curr. Eye Res. 2016, 41, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Meznerics, F.A.; Fehérvári, P.; Dembrovszky, F.; Kovács, K.D.; Kemény, L.V.; Csupor, D.; Hegyi, P.; Bánvölgyi, A. Platelet-Rich Plasma in Chronic Wound Management: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Clin. Med. 2022, 11, 7532. [Google Scholar] [CrossRef] [PubMed]
- Kia, C.; Baldino, J.; Bell, R.; Ramji, A.; Uyeki, C.; Mazzocca, A. Platelet-Rich Plasma: Review of Current Literature on Its Use for Tendon and Ligament Pathology. Curr. Rev. Musculoskelet. Med. 2018, 11, 566–572. [Google Scholar] [CrossRef]
- Sánchez, M.; Beitia, M.; Pompei, O.; Jorquera, C.; Sánchez, P.; Knörr, J.; Soldado, F.; López, L.; Oraa, J.; Bilbao, A.M.; et al. Isolation, Activation, and Mechanism of Action of Platelet-Rich Plasma and Its Applications for Joint Repair. In Regenerative Medicine; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef]
- Fice, M.P.; Miller, J.C.; Christian, R.; Hannon, C.P.; Smyth, N.; Murawski, C.D.; Cole, B.J.; Kennedy, J.G. The Role of Platelet-Rich Plasma in Cartilage Pathology: An Updated Systematic Review of the Basic Science Evidence. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 961.e3–976.e3. [Google Scholar] [CrossRef]
- Liu, X.; Li, Y.; Shen, L.; Yan, M. Leukocyte and Platelet-Rich Plasma (L-PRP) in Tendon Models: A Systematic Review and Meta-Analysis of in Vivo/in Vitro Studies. Evid.-Based Complement. Altern. Med. 2022, 2022, 5289145. [Google Scholar] [CrossRef]
- Miroshnychenko, O.; Chang, W.-T.; Dragoo, J.L. The Use of Platelet-Rich and Platelet-Poor Plasma to Enhance Differentiation of Skeletal Myoblasts: Implications for the Use of Autologous Blood Products for Muscle Regeneration. Am. J. Sport. Med. 2017, 45, 945–953. [Google Scholar] [CrossRef]
- Berndt, S.; Turzi, A.; Modarressi, A. Production of Autologous Platelet-Rich Plasma for Boosting In Vitro Human Fibroblast Expansion. J. Vis. Exp. JoVE 2021, 168, e60816. [Google Scholar] [CrossRef]
- Wang, Y.; Teichtahl, A.J.; Pelletier, J.-P.; Abram, F.; Wluka, A.E.; Hussain, S.M.; Martel-Pelletier, J.; Cicuttini, F.M. Knee Effusion Volume Assessed by Magnetic Resonance Imaging and Progression of Knee Osteoarthritis: Data from the Osteoarthritis Initiative. Rheumatology 2019, 58, 246–253. [Google Scholar] [CrossRef]
- Anitua, E.; de la Fuente, M.; Muruzabal, F.; Riestra, A.; Merayo-Lloves, J.; Orive, G. Plasma Rich in Growth Factors (PRGF) Eye Drops Stimulates Scarless Regeneration Compared to Autologous Serum in the Ocular Surface Stromal Fibroblasts. Exp. Eye Res. 2015, 135, 118–126. [Google Scholar] [CrossRef]
- Becerra-Bayona, S.M.; Solarte, V.A.; Alviar Rueda, J.D.; Sossa, C.L.; Arango-Rodríguez, M.L. Effect of Biomolecules Derived from Human Platelet-Rich Plasma on the Ex Vivo Expansion of Human Adipose-Derived Mesenchymal Stem Cells for Clinical Applications. Biol. J. Int. Assoc. Biol. Stand. 2022, 75, 37–48. [Google Scholar] [CrossRef]
- Borghese, C.; Agostini, F.; Durante, C.; Colombatti, A.; Mazzucato, M.; Aldinucci, D. Clinical-Grade Quality Platelet-Rich Plasma Releasate (PRP-R/SRGF) from CaCl2 -Activated Platelet Concentrates Promoted Expansion of Mesenchymal Stromal Cells. Vox Sang. 2016, 111, 197–205. [Google Scholar] [CrossRef]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef]
- Kon, E.; Di Matteo, B.; Delgado, D.; Cole, B.J.; Dorotei, A.; Dragoo, J.L.; Filardo, G.; Fortier, L.A.; Giuffrida, A.; Jo, C.H.; et al. Platelet-Rich Plasma for the Treatment of Knee Osteoarthritis: An Expert Opinion and Proposal for a Novel Classification and Coding System. Expert Opin. Biol. Ther. 2020, 20, 1–14. [Google Scholar] [CrossRef]
- Hahn, O.; Kieb, M.; Jonitz-Heincke, A.; Bader, R.; Peters, K.; Tischer, T. Dose-Dependent Effects of Platelet-Rich Plasma Powder on Chondrocytes In Vitro. Am. J. Sport. Med. 2020, 48, 1727–1734. [Google Scholar] [CrossRef]
- Mishra, A.; Tummala, P.; King, A.; Lee, B.; Kraus, M.; Tse, V.; Jacobs, C.R. Buffered Platelet-Rich Plasma Enhances Mesenchymal Stem Cell Proliferation and Chondrogenic Differentiation. Tissue Eng. Part C. Methods 2009, 15, 431. [Google Scholar] [CrossRef]
- Gruber, R.; Karreth, F.; Kandler, B.; Fuerst, G.; Rot, A.; Fischer, M.B.; Watzek, G. Platelet-Released Supernatants Increase Migration and Proliferation, and Decrease Osteogenic Differentiation of Bone Marrow-Derived Mesenchymal Progenitor Cells under in Vitro Conditions. Platelets 2004, 15, 29–35. [Google Scholar] [CrossRef]
- Mariani, E.; Pulsatelli, L.; Cattini, L.; Dolzani, P.; Assirelli, E.; Cenacchi, A.; Di Martino, A.; Arciola, C.R.; Filardo, G. Pure Platelet and Leukocyte-Platelet-Rich Plasma for Regenerative Medicine in Orthopedics-Time- and Preparation-Dependent Release of Growth Factors and Effects on Synovial Fibroblasts: A Comparative Analysis. Int. J. Mol. Sci. 2023, 24, 1512. [Google Scholar] [CrossRef]
- Ogino, Y.; Ayukawa, Y.; Kukita, T.; Koyano, K. The Contribution of Platelet-Derived Growth Factor, Transforming Growth Factor-Beta1, and Insulin-like Growth Factor-I in Platelet-Rich Plasma to the Proliferation of Osteoblast-like Cells. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 724–729. [Google Scholar] [CrossRef]
- Louis, M.L.; Magalon, J.; Jouve, E.; Bornet, C.E.; Mattei, J.C.; Chagnaud, C.; Rochwerger, A.; Veran, J.; Sabatier, F. Growth Factors Levels Determine Efficacy of Platelets Rich Plasma Injection in Knee Osteoarthritis: A Randomized Double Blind Noninferiority Trial Compared With Viscosupplementation. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2018, 34, 1530.e2–1540.e2. [Google Scholar] [CrossRef] [PubMed]
- De Figueiredo, C.S.; Raony, Í.; Medina, S.V.; de Mello Silva, E.; Dos Santos, A.A.; Giestal-de-Araujo, E. Insulin-like Growth Factor-1 Stimulates Retinal Cell Proliferation via Activation of Multiple Signaling Pathways. Curr. Res. Neurobiol. 2023, 4, 100068. [Google Scholar] [CrossRef]
- Zhang, B.; Hu, L.; Zhang, J.; Wu, H.; Li, W.; Gou, L.; Liu, H. Insulin Growth Factor-1 Enhances Proliferation and Inhibits Apoptosis of Neural Progenitor Cells by Phosphorylation of Akt/MTOR/P70S6K Molecules and Triggering Intrinsic Apoptosis Signaling Pathway. Cell Tissue Banking 2022, 23, 459–472. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Zhang, J.; Zhou, Z.; Pan, D.; Zhao, D.; Dong, H.; Yao, B. Novel Insights into the Effect of Deer IGF-1 on Chondrocyte Viability and IL-1β-Induced Inflammation Response. J. Biochem. Mol. Toxicol. 2023, 37, e23227. [Google Scholar] [CrossRef] [PubMed]
- Disser, N.P.; Sugg, K.B.; Talarek, J.R.; Sarver, D.C.; Rourke, B.J.; Mendias, C.L. Insulin-like Growth Factor 1 Signaling in Tenocytes Is Required for Adult Tendon Growth. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2019, 33, 12680–12695. [Google Scholar] [CrossRef]
- Yi, X.; Li, X.; Zhou, Y.; Ren, S.; Wan, W.; Feng, G.; Jiang, X. Hepatocyte growth factor regulates the TGF-β1-induced proliferation, differentiation and secretory function of cardiac fibroblasts. Int. J. Mol. Med. 2014, 34, 381–390. [Google Scholar] [CrossRef]
- Yamada, M.; Tatsumi, R.; Yamanouchi, K.; Hosoyama, T.; Shiratsuchi, S.; Sato, A.; Mizunoya, W.; Ikeuchi, Y.; Furuse, M.; Allen, R.E. High concentrations of HGF inhibit skeletal muscle satellite cell proliferation in vitro by inducing expression of myostatin: A possible mechanism for reestablishing satellite cell quiescence in vivo. Am. J. Physiol. Cell Physiol. 2010, 298, C465–C476. [Google Scholar] [CrossRef]
- Schievenbusch, S.; Strack, I.; Scheffler, M.; Wennhold, K.; Maurer, J.; Nischt, R.; Dienes, H.P.; Odenthal, M. Profiling of anti-fibrotic signaling by hepatocyte growth factor in renal fibroblasts. Biochem. Biophys. Res. Commun. 2009, 385, 55–61. [Google Scholar] [CrossRef]
- Zhang, J.; Middleton, K.K.; Fu, F.H.; Im, H.J.; Wang, J.H. HGF mediates the anti-inflammatory effects of PRP on injured tendons. PLoS One 2013, 8, e67303. [Google Scholar] [CrossRef]
- Van der Bijl, I.; Vlig, M.; Middelkoop, E.; de Korte, D. Allogeneic Platelet-Rich Plasma (PRP) Is Superior to Platelets or Plasma Alone in Stimulating Fibroblast Proliferation and Migration, Angiogenesis, and Chemotaxis as Relevant Processes for Wound Healing. Transfusion 2019, 59, 3492–3500. [Google Scholar] [CrossRef]
- Anitua, E.; Sanchez, M.; Nurden, A.T.; Zalduendo, M.; de la Fuente, M.; Azofra, J.; Andia, I. Reciprocal Actions of Platelet-Secreted TGF-Beta1 on the Production of VEGF and HGF by Human Tendon Cells. Plast. Reconstr. Surg. 2007, 119, 950–959. [Google Scholar] [CrossRef]
- Li, H.; Hicks, J.J.; Wang, L.; Oyster, N.; Philippon, M.J.; Hurwitz, S.; Hogan, M.V.; Huard, J. Customized Platelet-Rich Plasma with Transforming Growth Factor Β1 Neutralization Antibody to Reduce Fibrosis in Skeletal Muscle. Biomaterials 2016, 87, 147–156. [Google Scholar] [CrossRef]
- Anitua, E.; Pascual, C.; Pérez-Gonzalez, R.; Antequera, D.; Padilla, S.; Orive, G.; Carro, E. Intranasal Delivery of Plasma and Platelet Growth Factors Using PRGF-Endoret System Enhances Neurogenesis in a Mouse Model of Alzheimer’s Disease. PLoS One 2013, 8, e73118. [Google Scholar] [CrossRef]
- Delgado, D.; Bilbao, A.M.; Beitia, M.; Garate, A.; Sánchez, P.; González-Burguera, I.; Isasti, A.; López De Jesús, M.; Zuazo-Ibarra, J.; Montilla, A.; et al. Effects of Platelet-Rich Plasma on Cellular Populations of the Central Nervous System: The Influence of Donor Age. Int. J. Mol. Sci. 2021, 22, 1725. [Google Scholar] [CrossRef]
- Giusti, I.; D’Ascenzo, S.; Mancò, A.; Di Stefano, G.; Di Francesco, M.; Rughetti, A.; Dal Mas, A.; Properzi, G.; Calvisi, V.; Dolo, V. Platelet Concentration in Platelet-Rich Plasma Affects Tenocyte Behavior in Vitro. BioMed Res. Int. 2014, 2014, 630870. [Google Scholar] [CrossRef]
- Felthaus, O.; Prantl, L.; Skaff-Schwarze, M.; Klein, S.; Anker, A.; Ranieri, M.; Kuehlmann, B. Effects of Different Concentrations of Platelet-Rich Plasma and Platelet-Poor Plasma on Vitality and Differentiation of Autologous Adipose Tissue-Derived Stem Cells. Clin. Hemorheol. Microcirc. 2017, 66, 47–55. [Google Scholar] [CrossRef]
- Cho, H.S.; Song, I.H.; Park, S.-Y.; Sung, M.C.; Ahn, M.-W.; Song, K.E. Individual Variation in Growth Factor Concentrations in Platelet-Rich Plasma and Its Influence on Human Mesenchymal Stem Cells. Korean J. Lab. Med. 2011, 31, 212–218. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PRP Preparation | |
|---|---|
| Blood volume taken | 8 mL |
| Anticoagulant | Sodium citrate 3.8% (w/v) |
| System | Close |
| Centrifugation | Once, 580× g/8 min |
| Final PRP volume | 2 mL |
| PRP Characteristics | |
| PRP Type | 14-00-11 |
| MPV | 10.4 fL (CI: 9.40–11.60) |
| Red Blood Cells | <0.01 × 106/μL |
| White Blood Cells | <0.05 × 106/μL |
| Activation | CaCl2 10% (w/v) |
| Application Characteristics | |
| Dose | 10% |
| Direct/Indirect | Direct |
| Cell line | Normal human dermal fibroblasts |
| Other Remarkable PRP and Study Features | |
| The product added to the cell cultures was the platelet lysate obtained after activation of PRP using calcium chloride (10%) | |
| PRP: platelet-rich plasma; IA: intraarticular; IO: intraosseous; MPV: mean platelet volume | |
| IGF-1 Levels | HGF Levels | PDGF Levels | TGF-β Levels | VEGF Levels | Platelet Levels | ||
|---|---|---|---|---|---|---|---|
| RLU at 24 h | Pearson correlation | 0.605 | −0.115 | −0.065 | 0.018 | −0.076 | −0.057 |
| Sig. (bilateral) | 0.000 **** | 0.544 | 0.732 | 0.924 | 0.689 | 0.766 | |
| RLU at 48 h | Pearson correlation | 0.58 | −0.177 | −0.071 | −0.023 | −0.049 | −0.069 |
| Sig. (bilateral) | 0.001 *** | 0.35 | 0.71 | 0.903 | 0.798 | 0.715 | |
| RLU at 72 h | Pearson correlation | 0.56 | −0.216 | −0.067 | −0.015 | −0.042 | −0.07 |
| Sig. (bilateral) | 0.001 *** | 0.253 | 0.725 | 0.936 | 0.826 | 0.714 | |
| RLU at 96 h | Pearson correlation | 0.546 | −0.285 | −0.094 | −0.03 | −0.041 | −0.114 |
| Sig. (bilateral) | 0.002 ** | 0.127 | 0.622 | 0.873 | 0.831 | 0.549 |
| IGF-1 Levels | HGF Levels | PDGF Levels | TGF-β Levels | VEGF Levels | ||
|---|---|---|---|---|---|---|
| Platelet levels | Pearson correlation | 0.02 | 0.782 | 0.685 | 0.666 | 0.396 |
| Sig. (bilateral) | 0.915 | 0.000 **** | 0.000 **** | 0.000 **** | 0.030 * |
| B | Beta | p Value | 95% CI | ||
|---|---|---|---|---|---|
| IGF-1 | 2745.017 | 0.607 | 0.001 *** | 1206.009 | 4284,024 |
| HGF | −146.809 | −0.564 | 0.047 * | −291.848 | −1.769 |
| PDGF | −8.033 | −0.297 | 0.232 | −21.558 | 5.493 |
| TGF-β | −0.692 | −0.044 | 0.851 | −8.237 | 6.853 |
| VEGF | −225,451 | −0.205 | 0.313 | −677.801 | 226.898 |
| Platelets | 539.127 | 0.629 | 0.092 | −94.322 | 1172.575 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beitia, M.; Delgado, D.; Mercader, J.; Sánchez, P.; López de Dicastillo, L.; Sánchez, M. Action of Platelet-Rich Plasma on In Vitro Cellular Bioactivity: More than Platelets. Int. J. Mol. Sci. 2023, 24, 5367. https://doi.org/10.3390/ijms24065367
Beitia M, Delgado D, Mercader J, Sánchez P, López de Dicastillo L, Sánchez M. Action of Platelet-Rich Plasma on In Vitro Cellular Bioactivity: More than Platelets. International Journal of Molecular Sciences. 2023; 24(6):5367. https://doi.org/10.3390/ijms24065367
Chicago/Turabian StyleBeitia, Maider, Diego Delgado, Jon Mercader, Pello Sánchez, Leonor López de Dicastillo, and Mikel Sánchez. 2023. "Action of Platelet-Rich Plasma on In Vitro Cellular Bioactivity: More than Platelets" International Journal of Molecular Sciences 24, no. 6: 5367. https://doi.org/10.3390/ijms24065367
APA StyleBeitia, M., Delgado, D., Mercader, J., Sánchez, P., López de Dicastillo, L., & Sánchez, M. (2023). Action of Platelet-Rich Plasma on In Vitro Cellular Bioactivity: More than Platelets. International Journal of Molecular Sciences, 24(6), 5367. https://doi.org/10.3390/ijms24065367