
The Association between Apolipoprotein B, Cardiovascular Risk Factors and Subclinical Atherosclerosis—Findings from the SEPHAR National Registry on Hypertension in Romania

 ,
,  , ,
, , 
Abstract
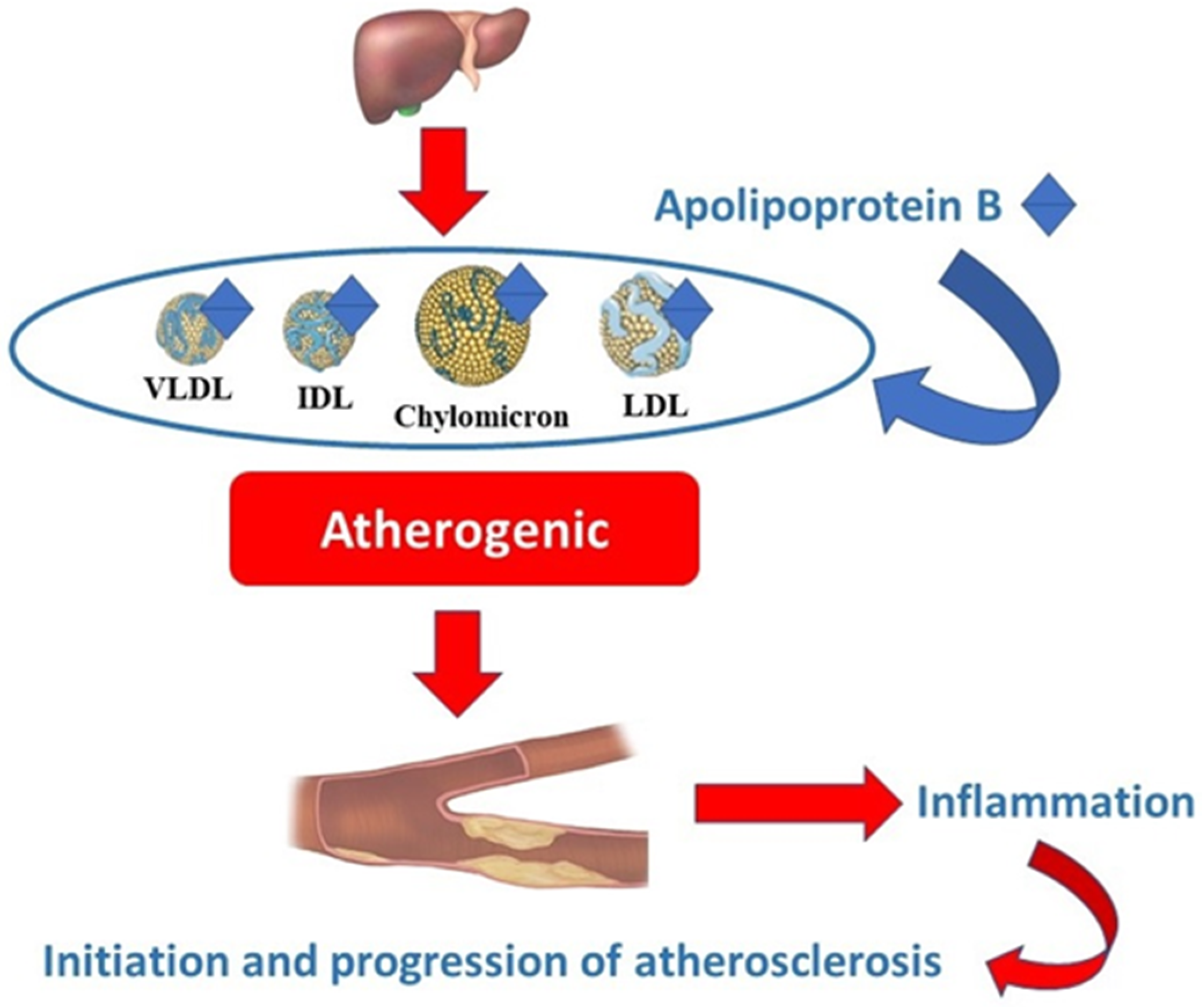
1. Introduction
2. Results
2.1. General Characteristics of the Study Populations in the Low versus High Apo B Groups
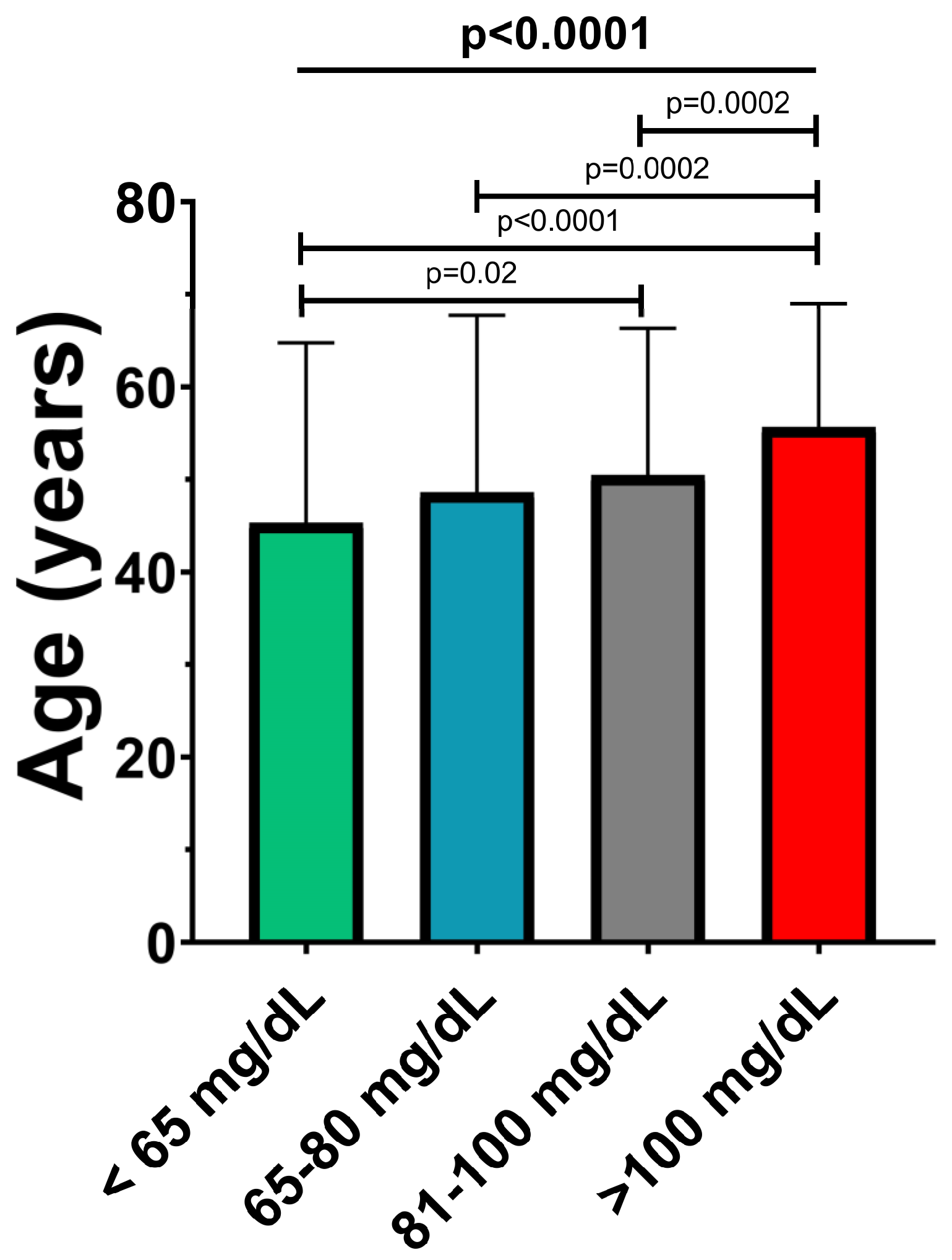
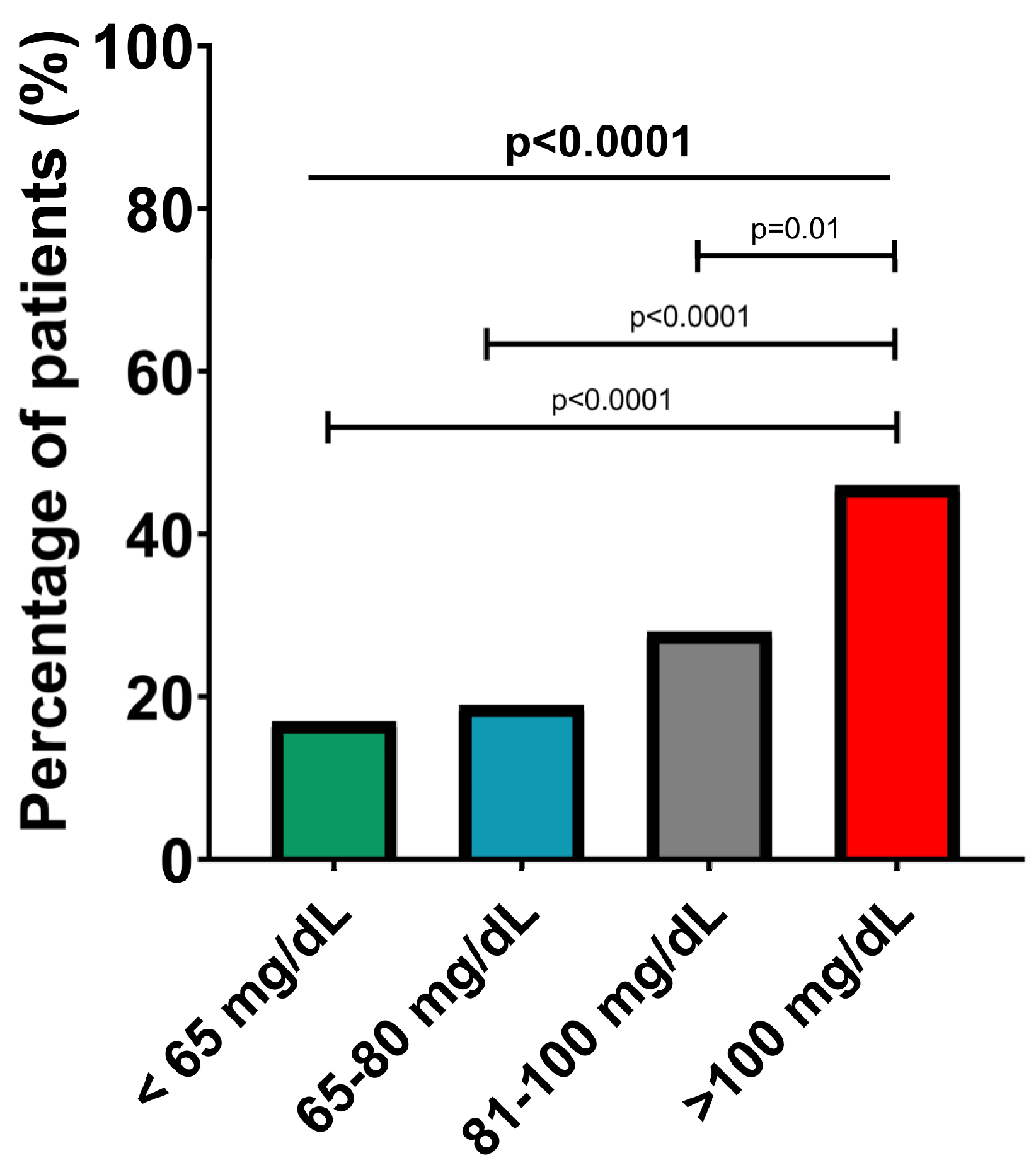
2.2. Characteristics of the Study Populations in the Four Subgroups According to Apo B Level
2.3. Apolipoprotein B, Uric Acid and Serum Lipids
3. Discussion
3.1. Apolipoprotein B and Lipid Profile
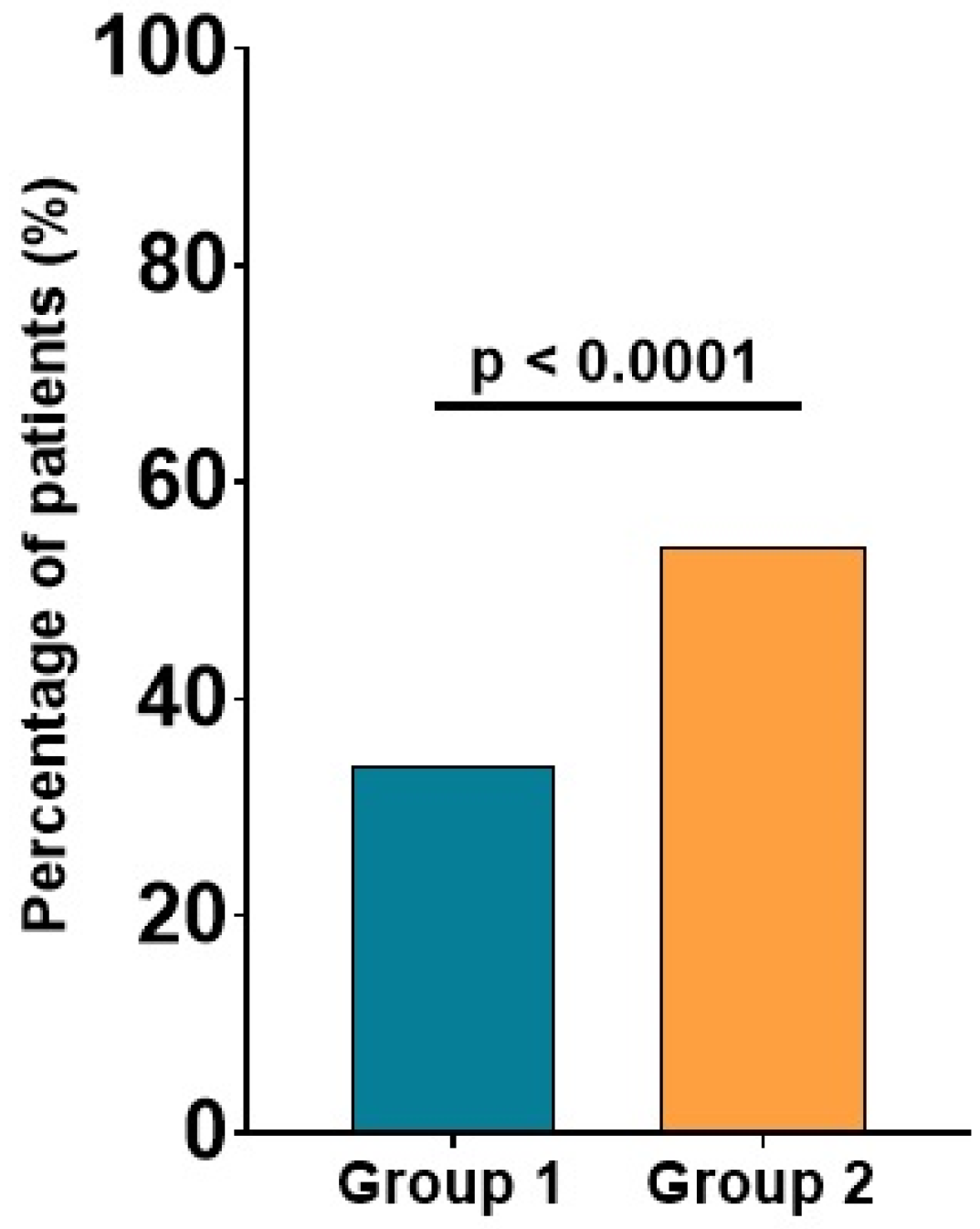
3.2. Apolipoprotein B and Carotid Plaques
3.3. Apolipoprotein B and Serum Levels of Uric Acid
3.4. Apolipoprotein B, Fasting Glucose Level and Diabetes Mellitus
4. Materials and Methods
4.1. Study Population
4.2. Study Groups
4.3. Collected Data
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, P.; Fang, Z.; Wang, H.; Cai, Y.; Rahimi, K.; Zhu, Y.; Fowkes, F.G.R.; Fowkes, F.J.; Rudan, I. Global and regional prevalence, burden, and risk factors for carotid atherosclerosis: A systematic review, meta-analysis, and modelling study. Lancet Glob. Health 2020, 8, e721–e729. [Google Scholar] [CrossRef] [PubMed]
- Amini, M.; Zayeri, F.; Salehi, M. Trend analysis of cardiovascular disease mortality, incidence, and mortality-to-incidence ratio: Results from global burden of disease study 2017. BMC Public Health 2021, 21, 401. [Google Scholar] [CrossRef] [PubMed]
- Dorobanţu, M.; Darabont, R.; Ghiorghe, S.; Georgescu, C.A.; Macarie, C.; Mitu, F.; Lighezan, D.; Musetescu, R.; Pop, C.; Ardeleanu, E.; et al. Hypertension prevalence and control in Romania at a seven-year interval. Comparison of SEPHAR I and II surveys. J. Hypertens. 2014, 32, 39–47. [Google Scholar] [CrossRef]
- Chen, G.; Farris, M.S.; Cowling, T.; Pinto, L.; Rogoza, R.M.; MacKinnon, E.; Champsi, S.; Anderson, T.J. Prevalence of atherosclerotic cardiovascular disease and subsequent major adverse cardiovascular events in Alberta, Canada: A real-world evidence study. Clin. Cardiol. 2021, 44, 1613–1620. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.M. Atherosclerotic cardiovascular disease beginning in childhood. Korean Circ. J. 2010, 40, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, F.D.R.; Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar]
- Kong, P.; Cui, Z.Y.; Huang, X.F.; Zhang, D.D.; Guo, R.J.; Han, M. Inflammation and atherosclerosis: Signaling pathways and therapeutic intervention. Signal Transduct. Target Ther. 2022, 7, 131. [Google Scholar] [CrossRef]
- Rodean, I.P.; Lazăr, L.; Halațiu, V.B.; Biriș, C.; Benedek, I.; Benedek, T. Periodontal disease is associated with increased vulnerability of coronary atheromatous plaques in patients undergoing coronary computed tomography angiography—Results from the atherodent study. J. Clin. Med. 2021, 10, 1290. [Google Scholar] [CrossRef]
- Rodean, I.P.; Biriș, C.I.; Halațiu, V.B.; Modiga, A.; Lazăr, L.; Benedek, I.; Benedek, T. Is there a link between COVID-19 infection, periodontal disease and acute myocardial infarction? Life 2021, 11, 1050. [Google Scholar] [CrossRef]
- Lee, C.K.; Liao, C.W.; Meng, S.W.; Wu, W.K.; Chiang, J.Y.; Wu, M.S. Lipids and lipoproteins in health and disease: Focus on targeting atherosclerosis. Biomedicines 2021, 9, 985. [Google Scholar] [CrossRef]
- Mehta, A.; Shapiro, M.D. Apolipoproteins in vascular biology and atherosclerotic disease. Nat. Rev. Cardiol. 2022, 19, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Behbodikhah, J.; Ahmed, S.; Elyasi, A.; Kasselman, L.J.; De Leon, J.; Glass, A.D.; Reiss, A.B. Apolipoprotein b and cardiovascular disease: Biomarker and potential therapeutic target. Metabolites 2021, 11, 690. [Google Scholar] [CrossRef] [PubMed]
- Sniderman, A.D.; Thanassoulis, G.; Glavinovic, T.; Navar, A.M.; Pencina, M.; Catapano, A.; Ference, B.A. Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review. JAMA Cardiol. 2019, 4, 1287–1295. [Google Scholar] [CrossRef]
- Lawler, P.R.; Akinkuolie, A.O.; Ridker, P.M.; Sniderman, A.D.; Buring, J.E.; Glynn, R.J.; Chasman, D.I.; Mora, S. Discordance between Circulating Atherogenic Cholesterol Mass and Lipoprotein Particle Concentration in Relation to Future Coronary Events in Women. Clin. Chem. 2017, 63, 870–879. [Google Scholar] [CrossRef] [PubMed]
- Welsh, C.; Celis-Morales, C.A.; Brown, R.; Mackay, D.F.; Lewsey, J.; Mark, P.B.; Gray, S.R.; Ferguson, L.D.; Anderson, J.J.; Lyall, D.M.; et al. Comparison of conventional lipoprotein tests and apolipoproteins in the prediction of cardiovascular disease data from UK biobank. Circulation 2019, 140, 542–552. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Malekmohammad, K.; Bezsonov, E.E.; Rafieian-Kopaei, M. Role of Lipid Accumulation and Inflammation in Atherosclerosis: Focus on Molecular and Cellular Mechanisms. Front. Cardiovasc. Med. 2021, 8, 707529. [Google Scholar] [CrossRef]
- Cho, D.S.; Woo, S.; Kim, S.; Byrne, C.D.; Kong, J.H.; Sung, K.C. Estimation of plasma apolipoprotein B concentration using routinely measured lipid biochemical tests in apparently healthy Asian adults. Cardiovasc. Diabetol. 2012, 11, 55. [Google Scholar] [CrossRef]
- Kim, B.J.; Hwang, S.T.; Sung, K.C.; Kim, B.S.; Kang, J.H.; Lee, M.H.; Park, J.R. Comparison of the relationships between serum apolipoprotein B and serum lipid distributions. Clin. Chem. 2005, 51, 2257–2263. [Google Scholar] [CrossRef]
- Hagström, E.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Danchin, N.; Diaz, R.; Goodman, S.G.; Harrington, R.A.; Jukema, J.W.; et al. Apolipoprotein B, Residual Cardiovascular Risk After Acute Coronary Syndrome, and Effects of Alirocumab. Circulation 2022, 146, 657–672. [Google Scholar] [CrossRef]
- Roșca, A.; Ion, B.; Mihăilă, T. Elevated Lipoprotein(a) Linked to Recurrent Cardiovascular Events—A Case Report. JIM 2022, 7, 78–80. [Google Scholar] [CrossRef]
- Steffen, B.T.; Guan, W.; Remaley, A.T.; Stein, J.H.; Tattersall, M.C.; Kaufman, J.; Tsai, M.Y. Apolipoprotein B is associated with carotid atherosclerosis progression independent of individual cholesterol measures in a 9-year prospective study of Multi-Ethnic Study of Atherosclerosis participants. J. Clin. Lipidol. 2017, 11, 1181–1191.e1. [Google Scholar] [CrossRef]
- Huang, F.; Yang, Z.; Xu, B.; Bi, Y.; Xu, M.; Xu, Y.; Lu, J.; Liu, Y.; Dai, M.; Zhou, W.; et al. Both Serum Apolipoprotein B and the Apolipoprotein B/Apolipoprotein A-I Ratio Are Associated with Carotid Intima-Media Thickness. PLoS ONE 2013, 8, e54628. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Shang, D.; Shao, J.; Dai, S.; Ge, X.; Hao, C.; Zhu, T. Prognostic significance of carotid plaque presence in peritoneal dialysis patients and its association with the apolipoprotein B/apolipoprotein A1 ratio. Nephrology 2020, 15, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Czeck, M.A.; Northrop, E.F.; Evanoff, N.G.; Dengel, D.R.; Rudser, K.D.; Kelly, A.S.; Ryder, J.R. Relationship of Apolipoproteins with Subclinical Cardiovascular Risk in Youth. J. Pediatr. 2020, 227, 199–203.e1. [Google Scholar] [CrossRef]
- Fahmy, E.M.; El Awady, M.A.E.S.; Sharaf, S.A.A.; Selim, N.M.; Abdo, H.E.S.; Mohammed, S.S. Apolipoproteins A1 and B and their ratio in acute ischemic stroke patients with intracranial and extracranial arterial stenosis: An Egyptian study. Egypt J. Neurol. Psychiatry Neurosurg. 2020, 56, 115. [Google Scholar] [CrossRef]
- Huddam, B.; Alp, A.; Genek, D.; Azak, A.; Karakus, V. Increased QT Dispersion and High Risk of Ventricular Arrhythmias is Associated with Hyperuricemia in Individuals with Normal Renal Function. J. Cardiovasc. Emerg. 2021, 7, 77–83. [Google Scholar] [CrossRef]
- Yu, W.; Cheng, J.D. Uric Acid and Cardiovascular Disease: An Update From Molecular Mechanism to Clinical Perspective. Front. Pharmacol. 2020, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Wang, L.; Huang, W.; Zhong, X.; Li, L.; Wang, H.; Peng, B.; Mao, M. Meta-analysis of the correlation between serum uric acid level and carotid intima-media thickness. PLoS ONE 2021, 16, e0246416. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Giovannini, M.; Grandi, E.; Rosticci, M.; D’Addato, S.; Borghi, C. Serum uric acid predicts incident metabolic syndrome in the elderly in an analysis of the Brisighella Heart Study. Sci. Rep. 2018, 8, 4–9. [Google Scholar] [CrossRef]
- Peng, T.-C.; Wang, C.-C.; Kao, T.-W.; Chan, J.Y.-H.; Yang, Y.-H.; Chang, Y.-W.; Chen, W.-L. Relationship between hyperuricemia and lipid profiles in us adults. Biomed. Res. Int. 2015, 2015, 127596. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, H.; Hsu, A.; Dalbeth, N.; Stamp, L.K.; McCormick, S.; Merriman, T.R. The relationship of apolipoprotein B and very low density lipoprotein triglyceride with hyperuricemia and gout. Arthritis Res. Ther. 2014, 16, 495. [Google Scholar] [CrossRef] [PubMed]
- Mester, A.; Cernica, D.; Opincariu, D.; Rat, N.; Hodas, R.; Kovacs, I.; Benedek, T.; Benedek, I. Magnitude of ST-segment Elevation Is Associated with Increased Acute Inflammatory Response and Myocardial Scar in Patients with Acute Myocardial Infarction Undergoing pPCI. J. Cardiovasc. Emerg. 2021, 7, 100–106. [Google Scholar] [CrossRef]
- Lee, K.W.; Shin, D. Concurrent presence of high serum uric acid and inflammation is associated with increased incidence of type 2 diabetes mellitus in Korean adult population. Sci. Rep. 2022, 12, 11000. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Katsuyama, H. Molecular Biological and Clinical Understanding of the Pathophysiology and Treatments of Hyperuricemia and Its Association with Metabolic Syndrome, Cardiovascular Diseases and Chronic Kidney Disease. Int. J. Mol. Sci. 2021, 22, 9221. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Wang, Y.; Li, Z.P.; Baiseitova, A.; Ban, Y.J.; Park, K.H. Xanthine Oxidase Inhibition and Anti-LDL Oxidation by Prenylated Isoflavones from Flemingia philippinensis Root. Molecules 2020, 25, 3074. [Google Scholar] [CrossRef]
- Jang, S.; Park, W.; Kim, H.; Yoo, S.; Lee, J.; Oh, M. Association of Apolipoprotein B with HbA1c in Nondiabetic Adults. Korean J. Fam. Pract. 2017, 7, 844–850. [Google Scholar] [CrossRef]
- Dong, H.; Ni, W.; Bai, Y.; Yuan, X.; Zhang, Y.; Zhang, H.; Sun, Y.; Xu, J. Cross-sectional and longitudinal associations of apolipoprotein A1 and B with glycosylated hemoglobin in Chinese adults. Sci. Rep. 2022, 12, 2751. [Google Scholar] [CrossRef]
- Gao, L.; Zhang, Y.; Wang, X.; Dong, H. Association of apolipoproteins A1 and B with type 2 diabetes and fasting blood glucose: A cross-sectional study. BMC Endocr. Disord. 2021, 21, 59. [Google Scholar] [CrossRef]
- Chou, Y.C.; You, S.L.; Bai, C.H.; Liao, Y.C.; Wei, C.Y.; Sun, C.A. Utility of apolipoprotein measurements in predicting incident type 2 diabetes: A Chinese cohort study. J. Formos. Med. Assoc. 2020, 119, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Richardson, T.G.; Wang, Q.; Sanderson, E.; Mahajan, A.; McCarthy, M.I.; Frayling, T.M.; Ala-Korpela, M.; Sniderman, A.; Smith, G.D.; Holmes, M.V. Effects of apolipoprotein B on lifespan and risks of major diseases including type 2 diabetes: A mendelian randomisation analysis using outcomes in first-degree relatives. Lancet Healthy Longev. 2021, 2, e317–e326. [Google Scholar] [CrossRef] [PubMed]
- Cojocaru, C.; Vîjîiac, A.-E.; Gheorghe-Fronea, O.; Mohaiu, T.; Itu, L.; Dorobanțu, M. Nine-Year Trends in Atrial Fibrillation Prevalence among Romanian Adult Hypertensives: A Post-Hoc Analysis of SEPHAR II-IV Surveys. Int. J. Environ. Res. Public Health 2022, 19, 9250. [Google Scholar] [CrossRef] [PubMed]
- Dorobantu, M.; Vijiiac, A.E.; Gheroghe-Fronea, O. The SEPHAR-FUp 2020 Project (Study for the Evaluation of Prevalence of Hypertension and Cardiovascular Risk in Romania—Follow-up 2020). J. Hypertens. Res. 2021, 7, 29–33. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 (<130 mg/dL) | Group 2 (>130 mg/dL) | p-Value | |
|---|---|---|---|
| Active smoking | 614 (86%) | 75 (77%) | 0.01 |
| Obesity | 313 (44%) | 53 (54%) | 0.06 |
| Hypertension | 259 (36%) | 43 (44%) | 0.1 |
| Diabetes mellitus | 71 (10%) | 12 (12%) | 0.4 |
| HF | 45 (6%) | 2 (2%) | 0.1 |
| MI | 16 (2%) | 5 (5%) | 0.4 |
| Angina pectoris | 64 (9%) | 13 (13%) | 0.1 |
| PCI or CABG | 28 (3%) | 1 (1%) | 0.2 |
| Atrial fibrillation | 52 (7%) | 5 (5%) | 0.5 |
| Stroke | 27 (4%) | 7 (7%) | 0.1 |
| Peripheral arterial disease | 15 (2%) | 4 (4%) | 0.2 |
| CKD | 10 (1%) | 3 (3%) | 0.2 |
| Parameter | Group 1 (<130 mg/dL) | Group 2 (>130 mg/dL) | p-Value |
|---|---|---|---|
| Total cholesterol (mg/dL) | 192.0 ± 36.3 [189.6–194.5] | 289.0 ± 48.7 [270.3–289.8] | <0.0001 |
| Triglycerides (mg/dL) | 111.4 ± 67.1 [106.6–116.2] | 201.9 ± 120.1 [176.4–227.4] | <0.0001 |
| HDL-cholesterol (mg/dL) | 53.9 ± 13.7 [53.0–54.9] | 50.2 ± 12.5 [47.7–52.7] | 0.005 |
| LDL-cholesterol (mg/dL) | 123.4 ± 35.0 [121.0–125.8] | 201.5 ± 43.4 [192.8–210.2] | <0.0001 |
| Parameter | Apo B < 65 mg/dL n = 102 | Apo B 65–80 mg/dL n = 180 | Apo B 81–100 mg/dL n = 221 | Apo B > 100 mg/dL n = 308 | p-Value ANOVA | p-Value of CV |
|---|---|---|---|---|---|---|
| Total cholesterol (mg/dL) | 144.0 ± 20.3 (14%) [140.1–147.8] | 171.1 ± 21.0 (12%) [167.6–174.5] | 195.3 ± 23.2 (12%) [192.5–198.1] | 239.8 ± 42.0 (18%) [235.4–244.1] | <0.0001 | <0.0001 |
| Triglycerides (mg/dL) | 71.8 ± 42.2 (59%) [63.3–80.4] | 95.1 ± 56.6 (60%) [86.8–103.5] | 106.2 ± 58.6 (55%) [98.8–149.8] | 159.9 ± 93.3 (58%) [149.8–170.0] | <0.0001 | 0.85 |
| HDL-cholesterol (mg/dL) | 57.9 ± 13.9 (24%) [55.3-60.5] | 56.5 ± 14.4 (25%) [54.4–58.5] | 53.7 ± 14.2 (26%) [52.0–55.4] | 50.5 ± 12.0 (24%) [49.3–51.8] | <0.0001 | 0.38 |
| LDL-cholesterol (mg/dL) | 73.4 ± 15.5 (21%) [70.5–76.3] | 101.7 ± 21.8 (21%) [98.6–104.8] | 127.5 ± 19.6 (15%) [125.1–129.8] | 168 ± 36.4 (22%) [164.9–172.5] | <0.0001 | <0.0001 |
| Parameter | Apo B < 65 mg/dL n = 102 | Apo B 65–80 mg/dL n = 180 | Apo B 81–100 mg/dL n = 221 | Apo B > 100 mg/dL n = 308 | p-Value | p-Value of CV |
|---|---|---|---|---|---|---|
| Uric acid (mg/dL) | 4.8 ± 1.3 (27%) [4.4–1.3] | 5.0 ± 1.6 (32%) [4.6–5.3] | 5.1 ± 1.5 (29%) [4.8–5.4] | 5.8 ± 1.6 (28%) [5.5–6.1] | <0.0001 | 0.15 |
| Fasting glucose (mg/dl) | 96.9 ± 24.8 (26%) [91.8–102.0] | 98.6 ± 24.4 (25%) [95.1–102.2] | 96.8 ± 16.6 (17%) [94.7–98.8] | 104.4 ± 25.8 (25%) [101.7–107.2] | <0.0001 | <0.0001 |
| HbA1c% | 5.5 ± 0.9 (16%) [5.3–5.6] | 5.5 ± 0.7 (13%) [5.4–5.6] | 5.5 ± 0.5 (9%) [5.4–5.6] | 5.8 ± 0.9 (16%) [5.7–5.9] | <0.0001 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dorobanțu, M.; Halațiu, V.-B.; Gheorghe-Fronea, O.; Bala, C.-G.; Moldovan, H.; Irinel-Parepa, R.; Rodean, I.-P.; Benedek, I.; Benedek, T. The Association between Apolipoprotein B, Cardiovascular Risk Factors and Subclinical Atherosclerosis—Findings from the SEPHAR National Registry on Hypertension in Romania. Int. J. Mol. Sci. 2023, 24, 2813. https://doi.org/10.3390/ijms24032813
Dorobanțu M, Halațiu V-B, Gheorghe-Fronea O, Bala C-G, Moldovan H, Irinel-Parepa R, Rodean I-P, Benedek I, Benedek T. The Association between Apolipoprotein B, Cardiovascular Risk Factors and Subclinical Atherosclerosis—Findings from the SEPHAR National Registry on Hypertension in Romania. International Journal of Molecular Sciences. 2023; 24(3):2813. https://doi.org/10.3390/ijms24032813
Chicago/Turabian StyleDorobanțu, Maria, Vasile-Bogdan Halațiu, Oana Gheorghe-Fronea, Cornelia-Gabriela Bala, Horațiu Moldovan, Raluca Irinel-Parepa, Ioana-Patricia Rodean, Imre Benedek, and Theodora Benedek. 2023. "The Association between Apolipoprotein B, Cardiovascular Risk Factors and Subclinical Atherosclerosis—Findings from the SEPHAR National Registry on Hypertension in Romania" International Journal of Molecular Sciences 24, no. 3: 2813. https://doi.org/10.3390/ijms24032813
APA StyleDorobanțu, M., Halațiu, V.-B., Gheorghe-Fronea, O., Bala, C.-G., Moldovan, H., Irinel-Parepa, R., Rodean, I.-P., Benedek, I., & Benedek, T. (2023). The Association between Apolipoprotein B, Cardiovascular Risk Factors and Subclinical Atherosclerosis—Findings from the SEPHAR National Registry on Hypertension in Romania. International Journal of Molecular Sciences, 24(3), 2813. https://doi.org/10.3390/ijms24032813