1. Introduction
Arachnoid granulations (AG), also commonly known as Pacchionian bodies, are present along the meningeal surface of the mammalian brain and are primarily localized in parasagittal brain regions in the vicinity of dural venous sinuses (DVS) [
1]. In humans, AGs typically measure only a few millimeters in diameter [
1], but on occasion, they enlarge to form giant arachnoid granulations, or giant Pacchionian bodies (GAGs). When enlarged, these structures may be associated with clinical symptomatology [
2,
3,
4,
5,
6,
7]. GAGs have increasingly been reported in recent years, primarily in radiological literature [
4,
5,
6,
7], though their composition remains poorly established [
1,
2]. In our diagnostic practice, we prospectively encountered five new GAGs in middle-aged individuals who presented with scalp or calvarial masses and/or complaints of intermittent or chronic headache. The rarity of biopsy assessment of this tissue [
1,
2,
3] as well as unexpected and symptomatic reactive changes in one patient prompted this report. Here, we document neuroimaging findings in five new GAGs that were diagnosed in three symptomatic adults and provide histopathological characterization that, for the first time, depicts prominent internal vascular components and reactive perivascular and immunological changes. These findings may aid diagnostic physicians who encounter symptomatic AGs or GAGs in live patients. Evidence provided here also suggests that these structures are dynamic tissues at brain borders and are susceptible to pathologies.
3. Case 2
3.1. Clinical Presentation
A patient was admitted for workup after presenting with a complaint of chronic headache. The patient described the headaches as migraines that had been intermittent over several years. Pain episodes began in the occipital region but often radiated toward the forehead. More recently, the patient began experiencing neck pain that radiated into the right shoulder, arm, and first three digits of the right hand. The patient also reported numbness and discomfort in these three digits as well as the radial aspect of the right hand, exacerbated by movement. Additionally, the patient described difficulty with right-sided head movement but denied noticing any masses or tenderness in the suboccipital region. Prior to presentation, the patient had undergone physical therapy, which led to minimal relief of symptoms. The family history was unremarkable, though the patient’s past medical history and review of systems were significant for balance disturbance, sinus headaches, hypertension, and mild memory problems. Physical examination of the head revealed a firm, non-tender, palpable mass in the suboccipital region. A neck exam revealed discomfort and reduced range of motion to the right side. Motor examination revealed minimal weakness in the right brachioradialis and right upper digits, upon digital extension. A sensory exam revealed diminished sensation in the right C6 distribution. Neurological examination was otherwise unremarkable.
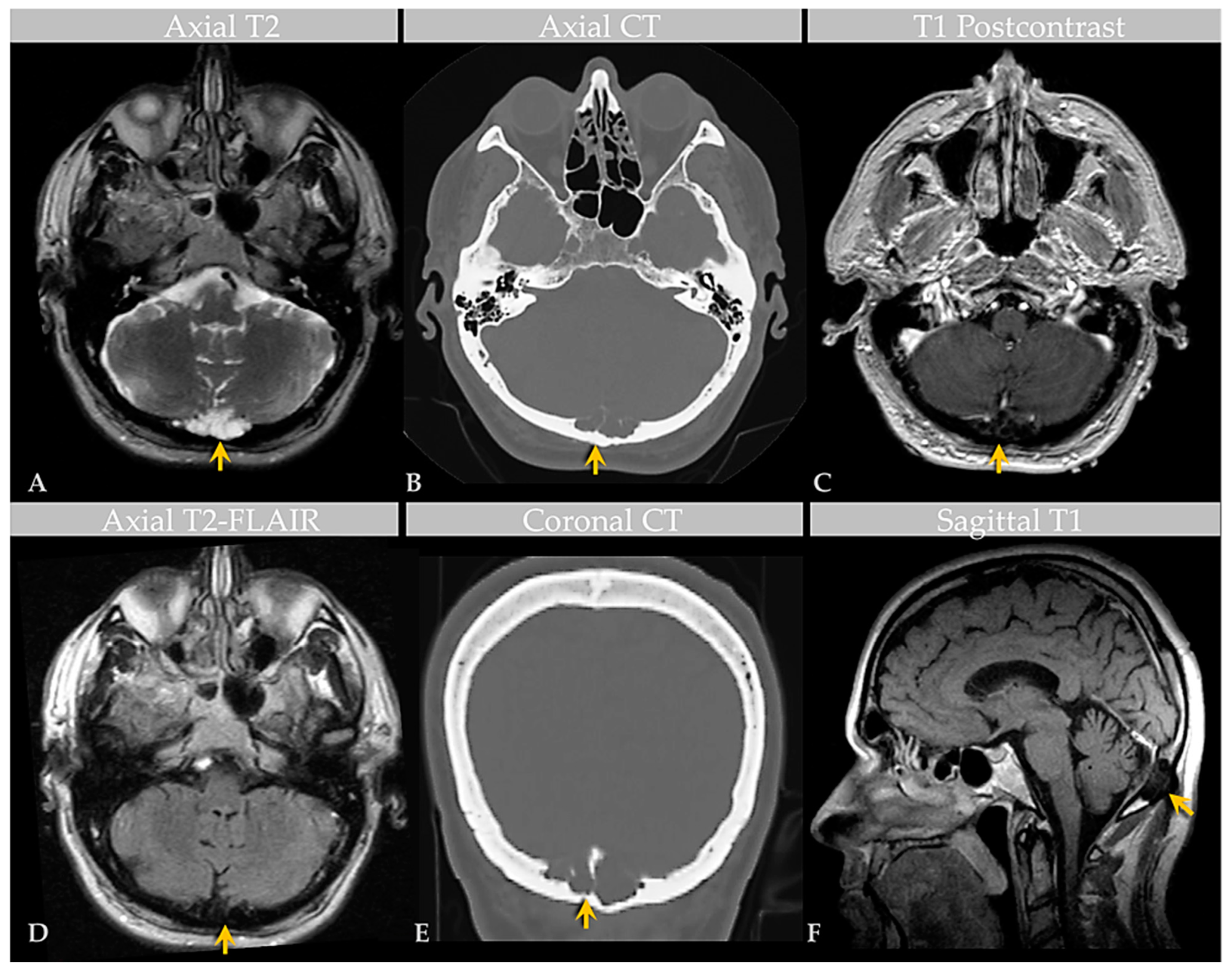
3.2. Imaging Features
Brain MRI with and without contrast and noncontrast CT of the head (
Figure 2) revealed a non-enhancing 3.6 × 1.3 × 1.8 cm abnormality that eroded the inner table of the occipital bone, causing lytic marrow expansion, extension through the dura and to the inion and the level of the torcula. Heterogeneous internal cystic-appearing MRI signal characteristics raised the possibility of an epidermoid cyst. There was no enhancing mass. MRI of the cervical spine did not reveal any abnormality to explain the patient’s symptomatology, though diffuse degenerative disease was appreciated. No definite cause for the radiculopathy was identified. A prior CT study documented the absence of the observed cranial lesion seven years prior to admission. To further evaluate the spinal cord, subarachnoid space, and associated structures, a CT myelogram was also performed (
Figure 3) and revealed partial penetration of iopamidol (Isovue-M
® 300) contrast tracer into the GAG interior, which demonstrated prominent internal soft tissue elements.
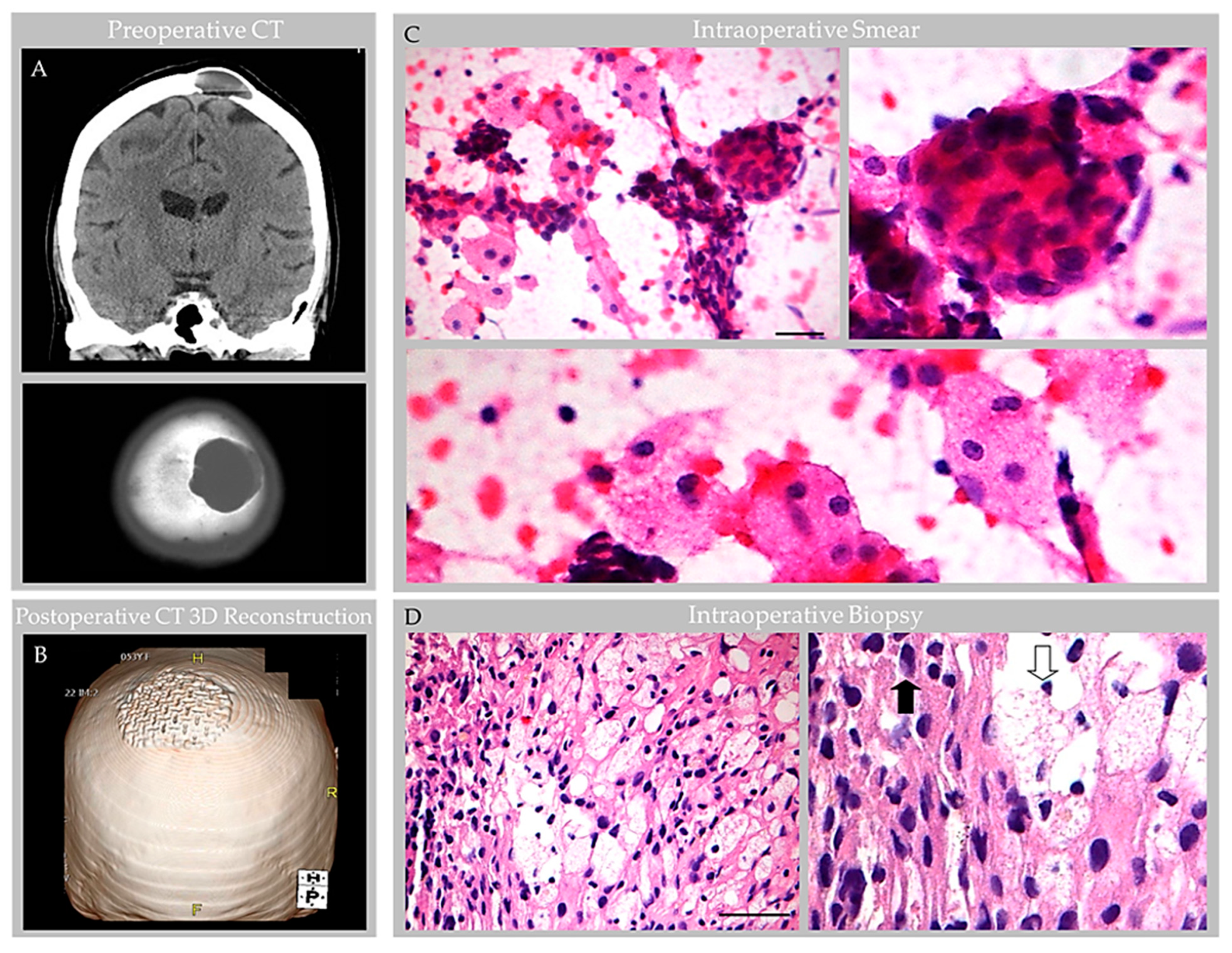
3.3. Surgical Course
Due to the persistent symptoms and unusual imaging findings, suboccipital craniectomy and surgical excision of the mass were performed and sent for biopsy workup. An intraoperative biopsy of 0.6 to 0.8 cm fragments of fresh tissue returned a diagnosis of benign bone. Titanium mesh cranioplasty was performed. The patient reported significant improvement in the headaches immediately following surgery.
3.4. General Histology Features
A larger resected mass measuring 3.2 × 3.0 × 1.0 cm was received in the pathology lab for permanent section analysis. The specimen was decalcified and then underwent routine processing. On histology, the biopsy material revealed fragments of benign bone and collagen tissue with a proliferation of small blood vessels. The mass was initially interpreted as a cavernous hemangioma, but on subsequent evaluation and radiological–pathological correlation, it was reinterpreted as a GAG. The associated bone fragments exhibited evidence of remodeling and reactive change without evidence of malignancy or other pathological changes. The patient reported complete resolution of the headaches following GAG resection.
5. Discussion
GAGs are well documented in radiological literature [
4,
5,
6,
7] and have been reported in various locations across human brain surfaces [
2,
3,
4,
5,
6,
7]. However, their prevalence and etiologies are minimally investigated and evidence concerning GAG internal microstructure is limited. Despite scant anatomical evidence, the potential for GAGs to cause clinical symptomatology is well known [
3,
4,
5,
6,
7]. Moreover, a recent investigation of non-giant AG anatomy [
1] revises concepts on the AG structure and function in humans [
8,
9,
10]. This recently published work systematically analyzed AG histology in persons across age and documented the presence of vessels and various immune cells within AG interiors, highlighting neuroimmune roles of these meningeal bodies that likely surveil CNS interfaces [
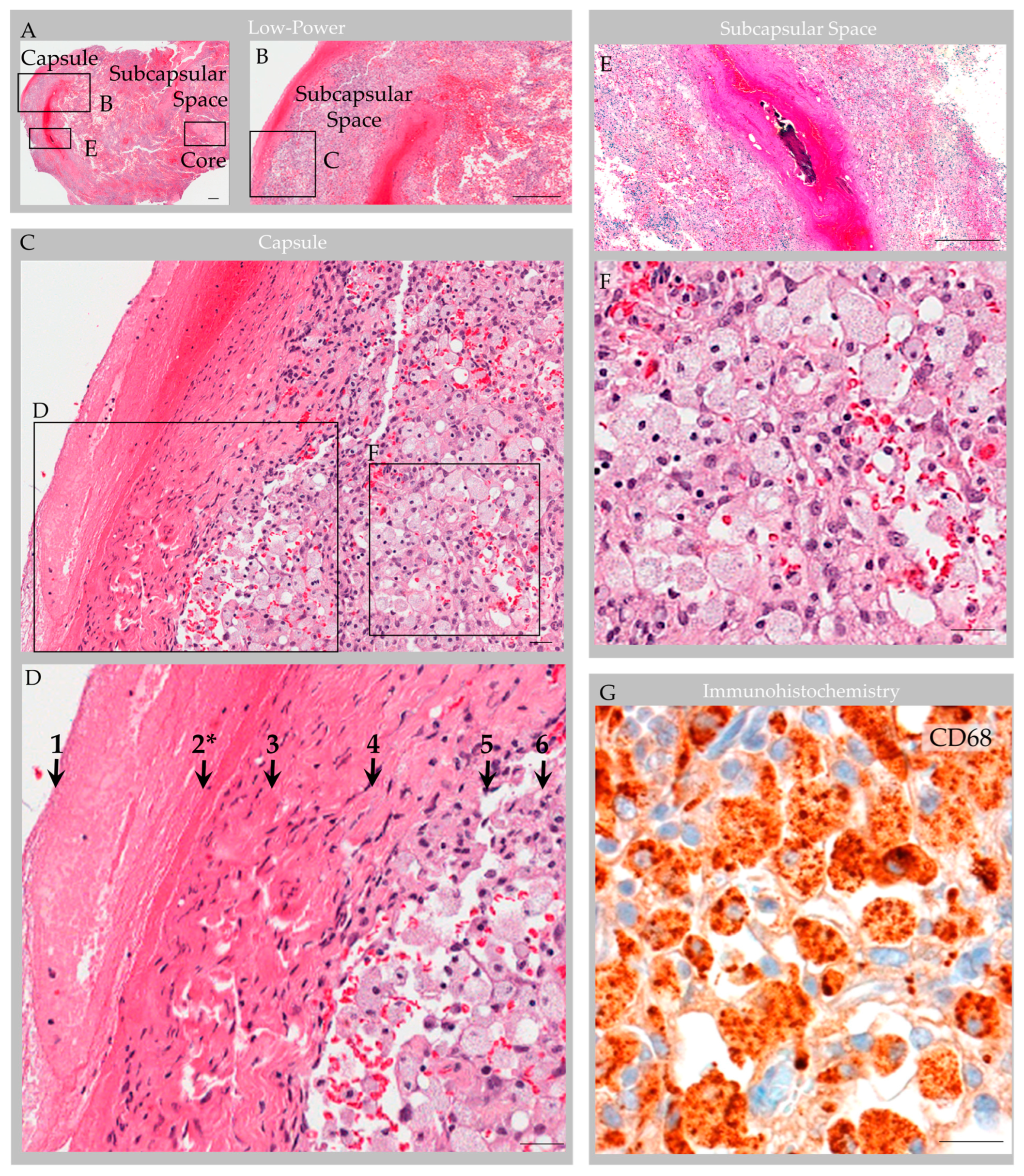
1]. However, this prior work incorporated postmortem tissues from non-diseased brains, only. Here, we studied available anatomical data associated with five GAGs from three individuals who presented with neurological symptoms to better understand the GAG structure based on in vivo and ex vivo features. On imaging examinations, GAGs indented bone and/or DVS and varied in size from 1.1 cm to 3.6 cm (mean, 2.2 cm). We also discovered that two of two (100%) GAGs with available H&E-labeled biopsy evidence showed florid internal vascular proliferation. One of the two biopsied GAGs (50%) also showed evidence of heterogeneous elements with exuberant inflammation. Additional internal reactive changes, including venous thrombosis and hemorrhage with early thrombus organization and calcification, were present in this latter GAG specimen that was sampled from an individual who sustained recent head trauma. The immune cell infiltrate in this patient displayed mixed constituents but was primarily comprised of foam cells that permeated and obliterated the subcapsular and central sinusoidal spaces. Meningothelial hyperplasia and associated nuclear PR expression was also focally present in this specimen and was most prominent in perivascular locations, suggesting important perivascular molecular exchange and signaling in AG and GAG tissues.
Given the prominent and heterogenous nature of the reactive changes identified within this latter specimen (i.e., Case 3), the resection material was further characterized with a comprehensive immunohistochemistry panel. Importantly, labeling with anti-CD31, CD34 and D2-40 antibodies and counterstain revealed that internal vessels within the structure consisted of erythrocyte-containing and erythrocyte-devoid blood and lymphatic vascular channels. D2-40-labeled lymphatic vascular elements within the GAGs consisted of well-formed tubularized lymphatic vessels as well as loosely formed lymphatic channels and singly scattered LECs that haphazardly extended into spaces of the central collagen core [
1], appearing to have a proliferative edge. The lymphatic vessels and LEC encircled and engulfed extravasated erythrocytes in the subcapsular space. To our knowledge, the presence of lymphatic vessels, lymphatic elements and LECs within central GAG tissue has not previously been reported in the literature and this feature was not identified in non-giant AGs that were recently thoroughly investigated from frontal brain regions of asymptomatic persons of variable age [
1]. Given this novel finding in a reactive GAG from an otherwise healthy middle-aged adult, in combination with the observation that the patient’s headaches resolved following partial GAG dome resection and drainage, we suspect that the obstructive hemorrhage, immune cell infiltrate, and associated flow stasis within the GAG structure were causative of the patient’s headaches [
7].
In light of historical literature and generally accepted knowledge regarding human AG structure [
8,
9,
10], the diagnosis of GAGs may be challenging in some patients. Detailed radiologic–pathologic data pertaining to GAGs are not available in published literature, although internal vascular components are well described in radiological reports [
4,
5,
6,
7]. Diagnostic challenges are exemplified by the differential diagnoses and initial diagnostic impressions rendered in the cases presented here. The first case was originally interpreted on imaging studies as bilateral transverse sinus thrombosis, which delayed proper diagnostic workup and management in this patient who experienced persistent headaches over the course of decades and was ultimately determined to have multiple GAGs involving three distinct brain regions. Likewise, the second case was interpreted on imaging studies as a possible GAG versus epidermoid cyst, and on biopsy was interpreted initially as a cavernous hemangioma, but consultation and radiologic–pathologic evaluation ultimately confirmed the diagnosis of GAGs in this patient. The third case was suspected to be a GAG based on characteristic imaging features and surgical inspection, and the diagnosis was confirmed by radiological–pathological correlation following biopsy. However, imaging features also raised the possibility of a benign bone cyst while the histology features in some areas closely mimicked a meningioma, cavernous hemangioma, and/or infection given the focal arrangement and hyperplasia of meningothelium, collagen and vessels in combination with the accumulation of immune cells. Follow-up in two patients (i.e., case two and case three), performed 2 months to 4 years after surgery, was notable for the absence of headache and MRI recurrence.
As with asymptomatic non-giant AG, investigation of GAG tissue is challenging in live humans [
1]. A recent study demonstrated that internal collagen forms a stromal meshwork within AGs and depicted, for the first time, the presence of cytokine and immune cell enrichment within AG cores [
1], which has revised concepts pertaining to AG biology as these findings suggested that AGs have underrecognized implications in neurophysiology. This prior study also demonstrated that AGs increase in size and have altered composition across the lifespan, raising the hypothesis that chronic flow stasis and uncharacterized degenerative changes may be involved in their reorganization and/or enlargement. While GAGs are rarely biopsied from live persons, the present report provides new data regarding their possible internal composite. Here, we show the potential for prominent reactive vascular and immune changes within enlarged AGs. These features within a prominently enlarged specimen further support that AGs and GAGs likely have important roles in vascular and immune homeostatic mechanisms. Importantly, the ingrowth of lymphatic vascular elements shown here for the first time supports the role of AGs in neurofluid, antigen and macromolecular processing. Additional preclinical and clinical studies are warranted to further elucidate GAG structure and function in health and aging as well as across various disease states.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







