
Chemokine Profile in Psoriasis Patients in Correlation with Disease Severity and Pruritus

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. PsO Group
4.2. Control Group
4.3. Classification into Early and Late-Onset PsO
4.4. Assessment of PsO Severity
4.5. Assessment of Pruritus
4.6. Evaluation of Serum Chemokine Levels
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campanati, A.; Marani, A.; Martina, E.; Diotallevi, F.; Radi, G.; Offidani, A. Psoriasis as an Immune-Mediated and Inflammatory Systemic Disease: From Pathophysiology to Novel Therapeutic Approaches. Biomedicines 2021, 9, 1511. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, F. Psoriasis: Comorbidities. J. Dermatol. 2021, 48, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Jaworecka, K.; Muda-Urban, J.; Rzepko, M.; Reich, A. Molecular Aspects of Pruritus Pathogenesis in Psoriasis. Int. J. Mol. Sci. 2021, 22, 858. [Google Scholar] [CrossRef]
- Szepietowski, J.C.; Reich, A. Pruritus in psoriasis: An update. Eur. J. Pain 2016, 20, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Hugh, J.M.; Weinberg, J.M. Update on the pathophysiology of psoriasis. Cutis 2018, 102, 6–12. [Google Scholar] [PubMed]
- Baliwag, J.; Barnes, D.H.; Johnston, A. Cytokines in psoriasis. Cytokine 2015, 73, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Kakarala, C.L.; Hassan, M.; Belavadi, R.; Gudigopuram, S.; Raguthu, C.C.; Gajjela, H.; Kela, I.; Sange, I. Beyond the Skin Plaques: Psoriasis and Its Cardiovascular Comorbidities. Cureus 2021, 13, e19679. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.H.; Schön, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Mohd Noor, A.A.; Azlan, M.; Mohd Redzwan, N. Orchestrated Cytokines Mediated by Biologics in Psoriasis and Its Mechanisms of Action. Biomedicines 2022, 10, 498. [Google Scholar] [CrossRef]
- Hughes, C.E.; Nibbs, R.J.B. A guide to chemokines and their receptors. FEBS J. 2018, 285, 2944–2971. [Google Scholar] [CrossRef] [PubMed]
- Nedoszytko, B.; Sokołowska-Wojdyło, M.; Ruckemann-Dziurdzińska, K.; Roszkiewicz, J.; Nowicki, R.J. Chemokines and cytokines network in the pathogenesis of the inflammatory skin diseases: Atopic dermatitis, psoriasis and skin mastocytosis. Postepy Dermatol. Alergol. 2014, 31, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Chu, D.; Kalantar-Zadeh, K.; George, J.; Young, H.A.; Liu, G. Cytokines: From Clinical Significance to Quantification. Adv. Sci. 2021, 8, e2004433. [Google Scholar] [CrossRef] [PubMed]
- Zdanowska, N.; Kasprowicz-Furmańczyk, M.; Placek, W.; Owczarczyk-Saczonek, A. The Role of Chemokines in Psoriasis-An Overview. Medicina 2021, 57, 754. [Google Scholar] [CrossRef] [PubMed]
- Joshi, N.; Narang, T.; Dogra, S.; Chhabra, S. Circulating levels of chemokines in patients with psoriasis vulgaris and their association with disease severity: A case-control study from North India. Indian J. Dermatol. Venereol. Leprol. 2019, 85, 567. [Google Scholar]
- Du, L.X.; Zhu, J.Y.; Mi, W.L. Cytokines and Chemokines Modulation of Itch. Neuroscience 2022, 495, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.; Wang, M.; Gao, H.; Zheng, A.; Li, J.; Mu, D.; Tong, J. The Role of Helper T Cells in Psoriasis. Front. Immunol. 2021, 12, 788940. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Vattepu, R.; Zhang, S. Chemokines and Innate Lymphoid Cells in Skin Inflammation. Cells 2021, 10, 3074. [Google Scholar] [CrossRef]
- Chovatiya, R.; Silverberg, J.I. Pathophysiology of Atopic Dermatitis and Psoriasis: Implications for Management in Children. Children 2019, 6, 108. [Google Scholar] [CrossRef]
- Furue, M.; Kadono, T. “Inflammatory skin march” in atopic dermatitis and psoriasis. Inflamm. Res. 2017, 66, 833–842. [Google Scholar] [CrossRef]
- Kaburagi, Y.; Shimada, Y.; Nagaoka, T.; Hasegawa, M.; Takehara, K.; Sato, S. Enhanced production of CC-chemokines (RANTES, MCP-1, MIP-1alpha, MIP-1beta, and eotaxin) in patients with atopic dermatitis. Arch. Dermatol. Res. 2001, 293, 350–355. [Google Scholar] [CrossRef]
- Dai, Y.J.; Li, Y.Y.; Zeng, H.M.; Liang, X.A.; Xie, Z.J.; Zheng, Z.A.; Pan, Q.H.; Xing, Y.X. Effect of pharmacological intervention on MIP-1α, MIP-1β and MCP-1 expression in patients with psoriasis vulgaris. Asian Pac. J. Trop. Med. 2014, 7, 582–584. [Google Scholar] [CrossRef]
- Lembo, S.; Capasso, R.; Balato, A.; Cirillo, T.; Flora, F.; Zappia, V.; Balato, N.; Ingrosso, D.; Ayala, F. MCP-1 in psoriatic patients: Effect of biological therapy. J. Dermatolog. Treat. 2014, 25, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Schuster, C.; Huard, A.; Sirait-Fischerm, E.; Dillmann, C.; Brünem, B.; Weigert, A. S1PR4-dependent CCL2 production promotes macrophage recruitment in a murine psoriasis model. Eur. J. Immunol. 2020, 50, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Zablotna, M.; Sobjanek, M.; Purzycka-Bohdan, D.; Szczerkowska-Dobosz, A.; Nedoszytko, B.; Nowicki, R. The -2518 A/G MCP-1 and -403 G/A RANTES promoter gene polymorphisms are associated with psoriasis vulgaris. Clin. Exp. Dermatol. 2016, 41, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Zhang, J.; Liu, B.; Tang, Y.; Wang, L.; Wang, G.; Wu, H.; Yang, C.; Li, X.; Li, B. Causal Effects of Circulating Cytokines on the Risk of Psoriasis Vulgaris: A Mendelian Randomization Study. Front. Genet. 2022, 13, 941961. [Google Scholar] [CrossRef] [PubMed]
- Rateb, A.A.; Fawzi, M.M.; Abdel Hay, R.M.; Mohammed, F.N.; Amr, K.S. Reduction of RANTES expression in lesional psoriatic skin after narrow band ultraviolet therapy: A possible marker of therapeutic efficacy. Eur. J. Dermatol. 2012, 22, 481–487. [Google Scholar] [CrossRef]
- de Groot, M.; Teunissen, M.B.; Ortonne, J.P.; Lambert, J.R.; Naeyaert, J.M.; Picavet, D.I.; Arreaza, M.G.; Simon, J.S.; Kraan, M.; Bos, J.D.; et al. Expression of the chemokine receptor CCR5 in psoriasis and results of a randomized placebo controlled trial with a CCR5 inhibitor. Arch. Dermatol. Res. 2007, 299, 305–313. [Google Scholar] [CrossRef]
- Saeki, H.; Tamaki, K. Thymus and activation regulated chemokine (TARC)/CCL17 and skin diseases. J. Dermatol. Sci. 2006, 43, 75–84. [Google Scholar] [CrossRef]
- Kakinuma, T.; Sugaya, M.; Nakamura, K.; Kaneko, F.; Wakugawa, M.; Matsushima, K.; Tamaki, K. Thymus and activation-regulated chemokine (TARC/CCL17) in mycosis fungoides: Serum TARC levels reflect the disease activity of mycosis fungoides. J. Am. Acad. Dermatol. 2003, 48, 23–30. [Google Scholar] [CrossRef]
- Renert-Yuval, Y.; Thyssen, J.P.; Bissonnette, R.; Bieber, T.; Kabashima, K.; Hijnen, D.; Guttman-Yassky, E. Biomarkers in atopic dermatitis-a review on behalf of the International Eczema Council. J. Allergy Clin. Immunol. 2021, 147, 1174–1190.e1. [Google Scholar] [CrossRef]
- Kataoka, Y. Thymus and activation-regulated chemokine as a clinical biomarker in atopic dermatitis. J. Dermatol. 2014, 41, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Kimura, T.; Sugaya, M.; Suga, H.; Morimura, S.; Miyamoto, A.; Kai, H.; Kagami, S.; Yanaba, K.; Fujita, H.; Asano, Y.; et al. Variations in serum TARC and I-TAC levels reflect minor changes in disease activity and pruritus in atopic dermatitis. Acta Derm. Venereol. 2014, 94, 331–332. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, Y.; Kamata, M.; Shimizu, T.; Nagata, M.; Fukaya, S.; Hayashi, K.; Fukuyasu, A.; Tanaka, T.; Ishikawa, T.; Ohnishi, T.; et al. Thymus and activation-regulated chemokine (TARC) in patients with psoriasis: Increased serum TARC levels in patients with generalized pustular psoriasis. J. Dermatol. 2020, 47, 1149–1156. [Google Scholar] [CrossRef] [PubMed]
- Borges, T.J.; Abarzua, P.; Gassen, R.B.; Kollar, B.; Lima-Filho, M.; Aoyama, B.T.; Gluhova, D.; Clark, R.A.; Islam, S.A.; Pomahac, B.; et al. T cell-attracting CCL18 chemokine is a dominant rejection signal during limb transplantation. Cell Rep. Med. 2022, 3, 100559. [Google Scholar] [CrossRef]
- Kim, H.O.; Cho, S.I.; Chung, B.Y.; Ahn, H.K.; Park, C.W.; Lee, C.H. Expression of CCL1 and CCL18 in atopic dermatitis and psoriasis. Clin. Exp. Dermatol. 2012, 37, 521–526. [Google Scholar] [CrossRef]
- Kakinuma, T.; Nakamura, K.; Wakugawa, M.; Mitsui, H.; Tada, Y.; Saeki, H.; Torii, H.; Komine, M.; Asahina, A.; Tamaki, K. Serum macrophage-derived chemokine (MDC) levels are closely related with the disease activity of atopic dermatitis. Clin. Exp. Immunol. 2002, 127, 270–273. [Google Scholar] [CrossRef]
- Kusumoto, S.; Kajihara, I.; Nagamoto, E.; Makino, K.; Ichihara, A.; Aoi, J.; Johno, T.; Makino, T.; Fukushima, S.; Jinnin, M.; et al. Increased CCL22 expression in psoriatic skin predicts a good response to infliximab therapy. Br. J. Dermatol. 2014, 171, 1259–1261. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, S.; Oliveira, H.; Reis, F.; Belo, L.; Rocha, S.; Quintanilha, A.; Figueiredo, A.; Teixeira, F.; Castro, E.; Rocha-Pereira, P.; et al. Interleukin (IL)-22, IL-17, IL-23, IL-8, vascular endothelial growth factor and tumour necrosis factor-α levels in patients with psoriasis before, during and after psoralen-ultraviolet A and narrowband ultraviolet B therapy. Br. J. Dermatol. 2010, 163, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Ha, H.; Debnath, B.; Neamati, N. Role of the CXCL8-CXCR1/2 Axis in Cancer and Inflammatory Diseases. Theranostics 2017, 7, 1543–1588. [Google Scholar] [CrossRef]
- Matsushima, K.; Yang, D.; Oppenheim, J.J. Interleukin-8: An evolving chemokine. Cytokine 2022, 153, 155828. [Google Scholar] [CrossRef]
- Lemster, B.H.; Carroll, P.B.; Rilo, H.R.; Johnson, N.; Nikaein, A.; Thomson, A.W. IL-8/IL-8 receptor expression in psoriasis and the response to systemic tacrolimus (FK506) therapy. Clin. Exp. Immunol. 1995, 99, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Q.; Li, X.; Tang, R. Effects of Narrow Band Ultraviolet B on Serum Levels of Vascular Endothelial Growth Factor and Interleukin-8 in Patients with Psoriasis. Am. J. Ther. 2016, 23, e655–e662. [Google Scholar] [CrossRef] [PubMed]
- Sticherling, M.; Sautier, W.; Schröder, J.M.; Christophers, E. Interleukin-8 plays its role at local level in psoriasis vulgaris. Acta Derm. Venereol. 1999, 79, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Kurpet, K.; Chwatko, G. S100 Proteins as Novel Therapeutic Targets in Psoriasis and Other Autoimmune Diseases. Molecules 2022, 27, 6640. [Google Scholar] [CrossRef]
- Singh, P.; Ali, S.A. Multifunctional Role of S100 Protein Family in the Immune System: An Update. Cells 2022, 11, 2274. [Google Scholar] [CrossRef]
- Wilsmann-Theis, D.; Wagenpfeil, J.; Holzinger, D.; Roth, J.; Koch, S.; Schnautz, S.; Bieber, T.; Wenzel, J. Among the S100 proteins, S100A12 is the most significant marker for psoriasis disease activity. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1165–1170. [Google Scholar] [CrossRef]
- Xia, C.; Braunstein, Z.; Toomey, A.C.; Zhong, J.; Rao, X. S100 Proteins As an Important Regulator of Macrophage Inflammation. Front. Immunol. 2018, 8, 1908. [Google Scholar] [CrossRef]
- El Dein Mohamed, A.S.; Hagag, M.M.; Kassem, N.; Shehata, W.A. Valosin-containing Protein in Psoriasis: A Clinical and Immunohistochemical Study. Appl. Immunohistochem. Mol. Morphol. 2021, 29, e68–e72. [Google Scholar] [CrossRef]
- Krahel, J.A.; Baran, A.; Kamiński, T.W.; Flisiak, I. Proprotein Convertase Subtilisin/Kexin Type 9, Angiopoietin-Like Protein 8, Sortilin, and Cholesteryl Ester Transfer Protein-Friends of Foes for Psoriatic Patients at the Risk of Developing Cardiometabolic Syndrome? Int. J. Mol. Sci. 2020, 21, 3682. [Google Scholar] [CrossRef]
- Szepietowski, J.C.; Reich, A.; Wiśnicka, B. Itching in patients suffering from psoriasis. Acta Dermatovenerol. Croat. 2002, 10, 221–226. [Google Scholar]
- Damiani, G.; Cazzaniga, S.; Conic, R.R.; Naldi, L.; Psocare Registry Network. Pruritus Characteristics in a Large Italian Cohort of Psoriatic Patients. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1316–1324. [Google Scholar] [CrossRef] [PubMed]
- Bahali, A.G.; Onsun, N.; Su, O.; Ozkaya, D.B.; Dizman, D.; Topukcu, B.; Uysal, O. The relationship between pruritus and clinical variables in patients with psoriasis. Bras. Dermatol. 2017, 92, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Prignano, F.; Ricceri, F.; Pescitelli, L.; Lotti, T. Itch in psoriasis: Epidemiology, clinical aspects and treatment options. Clin. Cosmet. Investig. Dermatol. 2009, 2, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Yosipovitch, G.; Goon, A.; Wee, J.; Chan, Y.H.; Goh, C.L. The prevalence and clinical characteristics of pruritus among patients with extensive psoriasis. Br. J. Dermatol. 2000, 143, 969–973. [Google Scholar] [CrossRef]
- Roblin, D.; Wickramasinghe, R.; Yosipovitch, G. Pruritus severity in patients with psoriasis is not correlated with psoriasis disease severity. J. Am. Acad. Dermatol. 2014, 70, 390–391. [Google Scholar] [CrossRef]
- Fatema, F.; Ghoshal, L.; Saha, A.; Agarwal, S.; Bandyopadhyay, D. Early-Onset versus Late-Onset Psoriasis: A Comparative Study of Clinical Variables, Comorbidities, and Association with HLA CW6 in a Tertiary Care Center. Indian J. Dermatol. 2021, 66, 705. [Google Scholar]
- Reich, A.; Riepe, C.; Anastasiadou, Z.; Mędrek, K.; Augustin, M.; Szepietowski, J.C.; Ständer, S. Itch Assessment with Visual Analogue Scale and Numerical Rating Scale: Determination of Minimal Clinically Important Difference in Chronic Itch. Acta Derm. Venereol. 2016, 96, 978–980. [Google Scholar] [CrossRef]


{kind=link}
| Chemokines | Controls n = 40 Mean ± SD Median [Range] (pg/mL) | PsO n = 60 Mean ± SD Median [Range] (pg/mL) | PsO vs. Controls p-Value | PsO Correlation between Chemokine Serum Level and PASI R * p-Value | PsO Correlation between Chemokine Serum Level and Pruritus Assessed by VAS R * p-Value |
|---|---|---|---|---|---|
| CCL2 (MCP-1) | 301.21 ± 88.40 303.00 [130.4–544.4] | 415.71 ± 138.06 409.95 [205.4–934.5] | <0.0001 | NS | NS |
| CCL3 (MIP-1α) | 13.31 ± 7.98 10.60 [2.9–32.2] | 31.15 ± 23.19 24.47 [6.1–136.8] | <0.0001 | NS | NS |
| CCL4 (MIP-1β) | 74.47 ± 31.72 73.75 [13.9–148.3] | 95.29 ± 70.55 75.10 [21.3–426.3] | 0.32 | NS | NS |
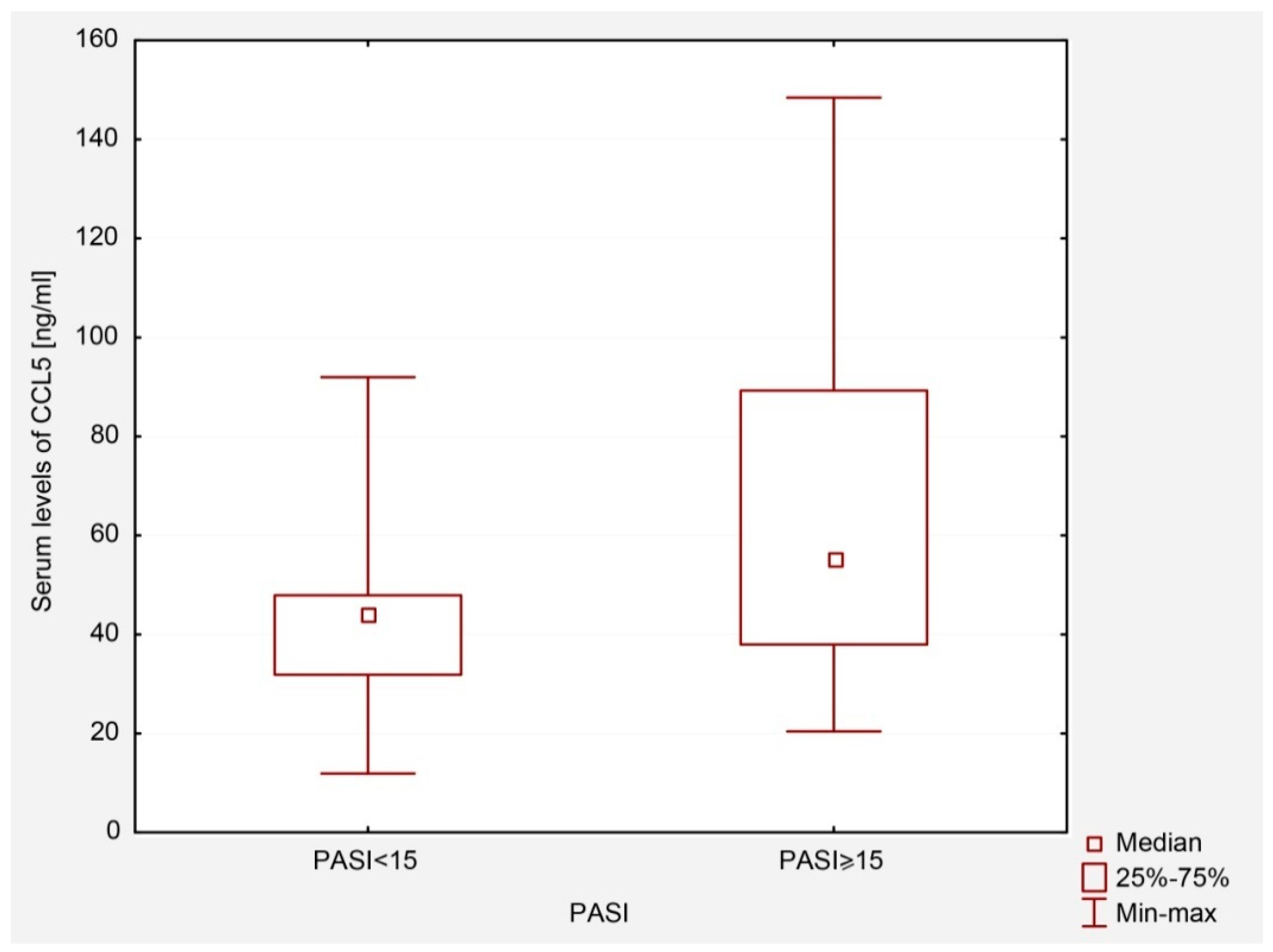
| CCL5 (RANTES) | 44,471 ± 24,786.8 42,804.00 [1877–94,522] | 68,695.78 ± 91,785 47,144.00 [11,914–148,425] | 0.037 | NS | NS |
| CCL17 (TARC) | 401.48 ± 182.40 408.59 [66.1–950.6] | 665.96 ± 463.24 510.20 [70.9–2300] | 0.002 | NS | R = 0.47 p = 0.05 |
| CCL18 (PARC) | 12.80 ± 6.72 11.85 [3.3–39.8] | 49.76 ± 26.56 42.48 [8.2–125] | <0.0001 | NS | NS |
| CCL22 (MDC) | 835.55 ± 336.96 770.46 [238.1–2262.9] | 1463.62 ± 816.39 1279.26 [254.4–3770.7] | <0.0001 | NS | NS |
| CXCL8 (IL-8) | 12.36 ± 7.41 9.44 [2.6–38.1] | 13.85 ± 14.80 9.62 [2.3–76] | 0.62 | NS | NS |
| Parameter | PsO | Early-Onset PsO | Late-Onset PsO | Controls |
|---|---|---|---|---|
| Total number of subjects, n (%) | 60 | 45 (75.0) | 15 (25.0) | 40 |
| Males, n (%) | 30 (50.0) | 26 (57.8) | 4 (26.7) | 29 (72.5) |
| Females, n (%) | 30 (50.0) | 19 (42.2) | 11 (73.3) | 11 (27.5) |
| Age at enrolment (years) Mean ± SD | 48.5 ± 14.6 | 45.3 ± 14.9 | 58.1 ± 7.8 | 39.75 ± 15.03 |
| Positive family history of PsO, n (%) | 29 (48.3) | 22 (75.9) | 7 (24.1) | 0 |
| PASI (points) Mean ± SD | 16.3 ± 9.2 | 16.9 ± 9.3 | 14.6 ± 9.0 | - |
| Pruritus according to VAS Mean ± SD | 5.5 ± 1.8 | 5.4 ± 1.9 | 6.0 ± 1.7 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Purzycka-Bohdan, D.; Nedoszytko, B.; Zabłotna, M.; Gleń, J.; Szczerkowska-Dobosz, A.; Nowicki, R.J. Chemokine Profile in Psoriasis Patients in Correlation with Disease Severity and Pruritus. Int. J. Mol. Sci. 2022, 23, 13330. https://doi.org/10.3390/ijms232113330
Purzycka-Bohdan D, Nedoszytko B, Zabłotna M, Gleń J, Szczerkowska-Dobosz A, Nowicki RJ. Chemokine Profile in Psoriasis Patients in Correlation with Disease Severity and Pruritus. International Journal of Molecular Sciences. 2022; 23(21):13330. https://doi.org/10.3390/ijms232113330
Chicago/Turabian StylePurzycka-Bohdan, Dorota, Bogusław Nedoszytko, Monika Zabłotna, Jolanta Gleń, Aneta Szczerkowska-Dobosz, and Roman J. Nowicki. 2022. "Chemokine Profile in Psoriasis Patients in Correlation with Disease Severity and Pruritus" International Journal of Molecular Sciences 23, no. 21: 13330. https://doi.org/10.3390/ijms232113330
APA StylePurzycka-Bohdan, D., Nedoszytko, B., Zabłotna, M., Gleń, J., Szczerkowska-Dobosz, A., & Nowicki, R. J. (2022). Chemokine Profile in Psoriasis Patients in Correlation with Disease Severity and Pruritus. International Journal of Molecular Sciences, 23(21), 13330. https://doi.org/10.3390/ijms232113330