
Skeletal System Biology and Smoke Damage: From Basic Science to Medical Clinic


 , , ,
, , , 
Abstract
1. Introduction
2. Smoking and Bone Damage
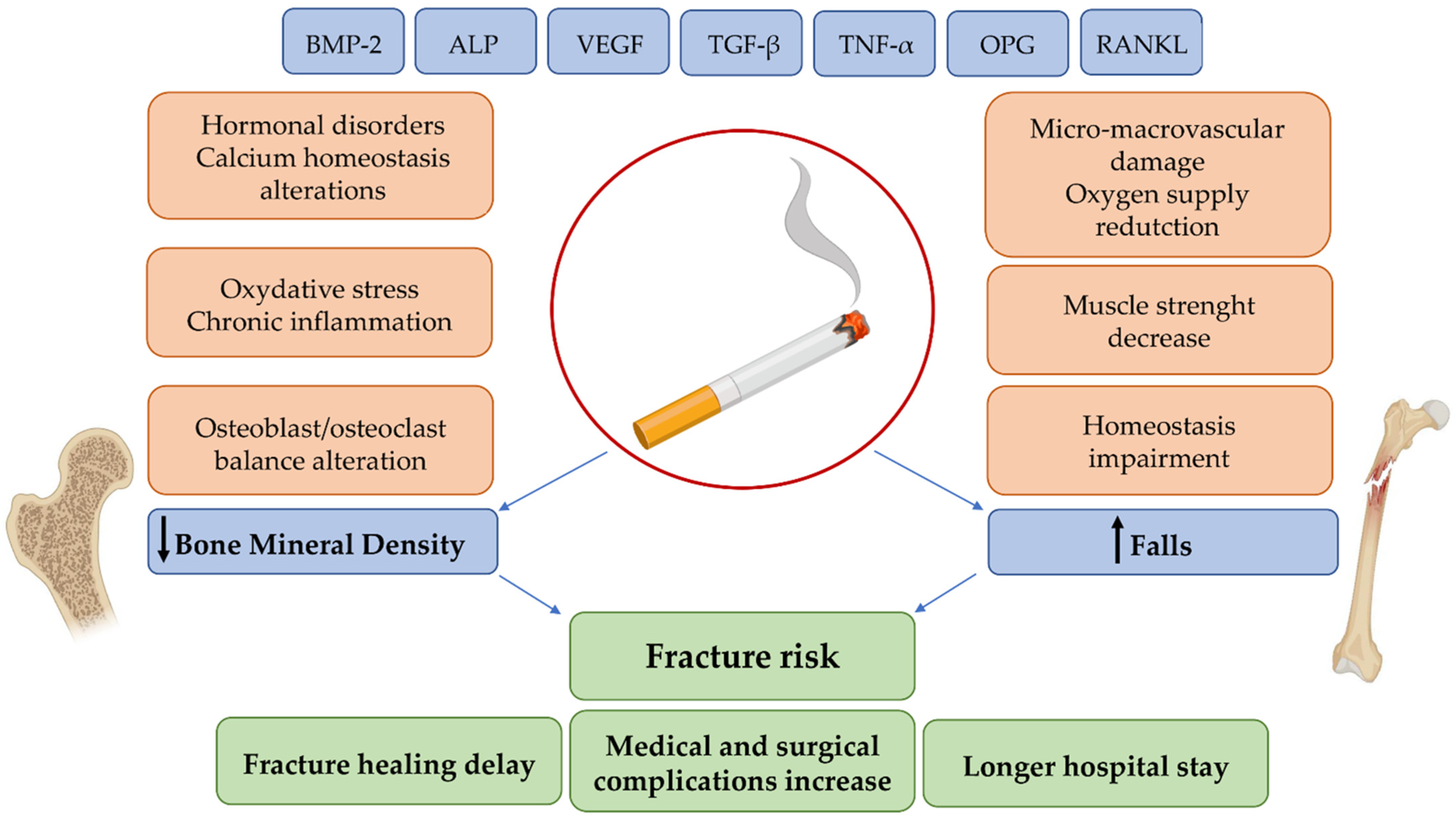
3. Pathophysiological Mechanisms of Smoking Effects on Bone Tissue
4. Medical and Surgical Complications of Fragility Fractures in Smokers
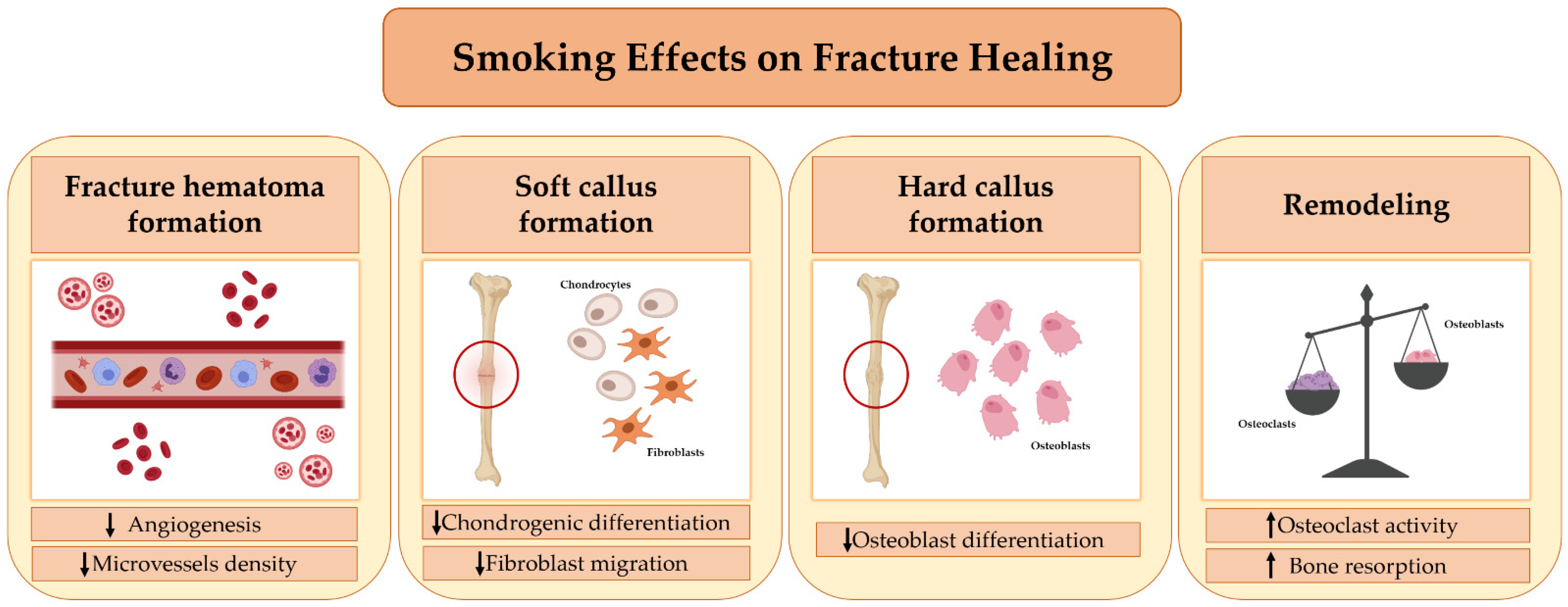
5. Smoking and Fracture Healing
6. Effects of Smoking Cessation on Bone Health
7. Discussion
8. Potential Intervention Strategies for the Prevention and Treatment of Smoking-Related Bone Damage
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathers, C.D.; Loncar, D. Projections of Global Mortality and Burden of Disease from 2002 to 2030. PLoS Med. 2006, 3, e442. [Google Scholar] [CrossRef] [PubMed]
- Collin, J. Global health, equity and the WHO Framework Convention on Tobacco Control. Glob. Health Promot. 2010, 17, 73–75. [Google Scholar] [CrossRef]
- Nturibi, E.M.; Kolawale, A.A.; McCurdy, S.A. Smoking Prevalence and Tobacco-Control Measures In Kenya, Uganda, The Gambia And Liberia: A Review. Int. J. Tuberc. Lung Dis. 2009, 13, 165–170. [Google Scholar]
- WHO. WHO Global Report on Trends in Prevalence of Tobacco Smoking; WHO: Geneva, Switzerland, 2015; pp. 1–359. [Google Scholar]
- Ng, M.; Freeman, M.K.; Fleming, T.D.; Robinson, M.; Dwyer-Lindgren, L.; Thomson, B.; Wollum, A.; Sanman, E.; Wulf, S.; Lopez, A.D.; et al. Smoking Prevalence and Cigarette Consumption in 187 Countries, 1980–2012. JAMA 2014, 311, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Al-Bashaireh, A.M.; Haddad, L.G.; Weaver, M.; Kelly, D.L.; Chengguo, X.; Yoon, S. The Effect of Tobacco Smoking on Musculoskeletal Health: A Systematic Review. J. Environ. Public Health 2018, 2018, 1–106. [Google Scholar] [CrossRef]
- Law, M.R.; Hackshaw, A.K. A meta-analysis of cigarette smoking, bone mineral density and risk of hip fracture: Recognition of a major effect. BMJ 1997, 315, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.D.; Klesges, R.C. A meta-analysis of the effects of cigarette smoking on bone mineral density. Calcif. Tissue Int. 2001, 68, 259–270. [Google Scholar] [CrossRef]
- Morse, C.I.; Wüst, R.C.I.; Jones, D.A.; de Haan, A.; Degens, H. Muscle fatigue resistance during stimulated contractions is reduced in young male smokers. Acta Physiol. 2007, 191, 123–129. [Google Scholar] [CrossRef]
- Lee, P.N.; Coombs, K.J.; Afolalu, E.F. Considerations related to vaping as a possible gateway into cigarette smoking: An analytical review. F1000Research 2018, 7, 1915. [Google Scholar] [CrossRef]
- Abate, M.; Vanni, D.; Pantalone, A.; Salini, V. Cigarette smoking and musculoskeletal disorders. Muscle Ligaments Tendons J. 2013, 3, 63–69. [Google Scholar] [CrossRef]
- Kanis, J.A.; Johnell, O.; Oden, A.; Johansson, H.; de Laet, C.; Eisman, J.A.; Fujiwara, S.; Kroger, H.; McCloskey, E.V.; Mellstrom, D.; et al. Smoking and fracture risk: A meta-analysis. Osteoporos. Int. 2005, 16, 155–162. [Google Scholar] [CrossRef]
- Aspera-Werz, R.H.; Ehnert, S.; Heid, D.; Zhu, S.; Chen, T.; Braun, B.; Sreekumar, V.; Arnscheidt, C.; Nussler, A.K. Nicotine and Cotinine Inhibit Catalase and Glutathione Reductase Activity Contributing to the Impaired Osteogenesis of SCP-1 Cells Exposed to Cigarette Smoke. Oxidative Med. Cell. Longev. 2018, 2018, 1–13. [Google Scholar] [CrossRef]
- Yoon, V.; Maalouf, N.M.; Sakhaee, K. The effects of smoking on bone metabolism. Osteoporos. Int. 2012, 23, 2081–2092. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.H.; Chan, R.L.Y.; Siu, W.S.; Shum, W.T.; Leung, P.C.; Zhang, L.; Cho, C.H. Deteriorating Effect on Bone Metabolism and Microstructure by Passive Cigarette Smoking Through Dual Actions on Osteoblast and Osteoclast. Calcif. Tissue Int. 2015, 96, 389–400. [Google Scholar] [CrossRef] [PubMed]
- Daniell, H.W. Osteoporosis of the slender smoker. Vertebral compression fractures and loss of metacarpal cortex in relation to postmenopausal cigarette smoking and lack of obesity. Arch. Intern. Med. 1976, 136, 298–304. [Google Scholar] [CrossRef]
- Rudäng, R.; Darelid, A.; Nilsson, M.; Nilsson, S.; Mellström, D.; Ohlsson, C.; Lorentzon, M. Smoking is associated with impaired bone mass development in young adult men: A 5-year longitudinal study. J. Bone Miner. Res. 2012, 27, 2189–2197. [Google Scholar] [CrossRef]
- Nuti, R.; Brandi, M.L.; Checchia, G.; Di Munno, O.; Dominguez, L.; Falaschi, P.; Fiore, C.E.; Iolascon, G.; Maggi, S.; Michieli, R.; et al. Guidelines for the management of osteoporosis and fragility fractures. Intern. Emerg. Med. 2019, 14, 85–102. [Google Scholar] [CrossRef]
- Bączyk, G.; Opala, T.; Kleka, P.; Chuchracki, M. Multifactorial analysis of risk factors for reduced bone mineral density among postmenopausal women. Arch. Med Sci. 2012, 8, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Noale, M.; Maggi, S.; Crepaldi, G. Osteoporosis among Italian women at risk: The OSTEOLAB study. J. Nutr. Health Aging 2012, 16, 529–533. [Google Scholar] [CrossRef]
- Al-Bashaireh, A.M.; Haddad, L.G.; Weaver, M.; Chengguo, X.; Kelly, D.L.; Yoon, S. The Effect of Tobacco Smoking on Bone Mass: An Overview of Pathophysiologic Mechanisms. J. Osteoporos. 2018, 2018, 1206235. [Google Scholar] [CrossRef]
- Oh, S.-W. Obesity, Sarcopenia, and Smoking: Landscape in the Mist. Korean J. Fam. Med. 2019, 40, 61–62. [Google Scholar] [CrossRef] [PubMed]
- Clair, C.; Chiolero, A.; Faeh, D.; Cornuz, J.; Marques-Vidal, P.; Paccaud, F.; Mooser, V.; Waeber, G.; Vollenweider, P. Dose-dependent positive association between cigarette smoking, abdominal obesity and body fat: Cross-sectional data from a population-based survey. BMC Public Health 2011, 11, 23. [Google Scholar] [CrossRef]
- Kim, Y.; Jeong, S.M.; Yoo, B.; Oh, B.; Kang, H.-C. Associations of smoking with overall obesity, and central obesity: A cross-sectional study from the Korea National Health and Nutrition Examination Survey (2010–2013). Epidemiol. Health 2016, 38, e2016020. [Google Scholar] [CrossRef]
- Chatkin, R.; Chatkin, J.M. Tabagismo e variação ponderal: A fisiopatologia e genética podem explicar esta associação? J. Bras. Pneumol. 2007, 33, 712–719. [Google Scholar] [CrossRef]
- Ferrara, C.; Kumar, M.; Nicklas, B.; McCrone, S.; Goldberg, A. Weight gain and adipose tissue metabolism after smoking cessation in women. Int. J. Obes. 2001, 25, 1322–1326. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wong, P.K.K.; Christie, J.J.; Wark, J.D. The effects of smoking on bone health. Clin. Sci. 2007, 113, 233–241. [Google Scholar] [CrossRef]
- Jo, Y.; Linton, J.A.; Choi, J.; Moon, J.; Kim, J.; Lee, J.; Oh, S. Association between Cigarette Smoking and Sarcopenia according to Obesity in the Middle-Aged and Elderly Korean Population: The Korea National Health and Nutrition Examination Survey (2008–2011). Korean J. Fam. Med. 2019, 40, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Rom, O.; Kaisari, S.; Aizenbud, D.; Reznick, A.Z. Sarcopenia and smoking: A possible cellular model of cigarette smoke effects on muscle protein breakdown. Ann. N. Y. Acad. Sci. 2012, 1259, 47–53. [Google Scholar] [CrossRef]
- Jorde, R.; Stunes, A.K.; Kubiak, J.; Grimnes, G.; Thorsby, P.M.; Syversen, U. Smoking and other determinants of bone turnover. PLoS ONE 2019, 14, e0225539. [Google Scholar] [CrossRef]
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef]
- Mousavi, S.E.; Amini, H.; Heydarpour, P.; Chermahini, F.A.; Godderis, L. Air pollution, environmental chemicals, and smoking may trigger vitamin D deficiency: Evidence and potential mechanisms. Environ. Int. 2019, 122, 67–90. [Google Scholar] [CrossRef]
- Kassi, E.N.; Stavropoulos, S.; Kokkoris, P.; Galanos, A.; Moutsatsou, P.; Dimas, C.; Papatheodorou, A.; Zafeiris, C.; Lyritis, G. Smoking is a significant determinant of low serum vitamin D in young and middle-aged healthy males. Hormones 2014, 14, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Lahmann, C.; Bergemann, J.; Harrison, G.; Young, A.R. Matrix metalloproteinase-1 and skin ageing in smokers. Lancet 2001, 357, 935–936. [Google Scholar] [CrossRef]
- Jandikova, H.; Duskova, M.; Simunkova, K.; Racz, B.; Hill, M.; Kralikova, E.; Vondra, K.; Stárka, L. The Steroid Spectrum During and After Quitting Smoking. Physiol. Res. 2015, 64, S211–S218. [Google Scholar] [CrossRef]
- Michnovicz, J.J.; Hershcopf, R.J.; Naganuma, H.; Bradlow, H.L.; Fishman, J. Increased 2-Hydroxylation of Estradiol as a Possible Mechanism for the Anti-Estrogenic Effect of Cigarette Smoking. N. Engl. J. Med. 1986, 315, 1305–1309. [Google Scholar] [CrossRef]
- Jandíková, H.; Dušková, M.; Stárka, L. The Influence of Smoking and Cessation on the Human Reproductive Hormonal Balance. Physiol. Res. 2017, 66, S323–S331. [Google Scholar] [CrossRef] [PubMed]
- Ruan, X.; Mueck, A.O. Impact of smoking on estrogenic efficacy. Climacteric 2014, 18, 38–46. [Google Scholar] [CrossRef]
- Meek, M.D.; Finch, G.L. Diluted Mainstream Cigarette Smoke Condensates Activate Estrogen Receptor and Aryl Hydrocarbon Receptor-Mediated Gene Transcription. Environ. Res. 1999, 80, 9–17. [Google Scholar] [CrossRef]
- Kapoor, D.; Malkin, C.J.; Channer, K.S.; Jones, T.H. Androgens, insulin resistance and vascular disease in men. Clin. Endocrinol. 2005, 63, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Badrick, E.; Kirschbaum, C.; Kumari, M. The Relationship between Smoking Status and Cortisol Secretion. J. Clin. Endocrinol. Metab. 2007, 92, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Stalke, J.; Hader, O.; Bähr, V.; Hensen, J.; Scherer, G.; Oelkers, W. The role of vasopressin in the nicotine-induced stimulation of ACTH and cortisol in men. Clin. Investig. 1992, 70, 218–223. [Google Scholar] [CrossRef]
- Kim, B.S.; Kim, S.-J.; Kim, H.-J.; Lee, S.-J.; Park, Y.-J.; Lee, J.; You, H.-K. Effects of nicotine on proliferation and osteoblast differentiation in human alveolar bone marrow-derived mesenchymal stem cells. Life Sci. 2012, 90, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.; Branco, J.C. Rank/Rankl/opg: Literature review. Acta Reum. Port. 2011, 36, 209–218. [Google Scholar]
- Al-Bashaireh, A.M.; Alqudah, O. Comparison of Bone Turnover Markers between Young Adult Male Smokers and Nonsmokers. Cureus 2020, 12, e6782. [Google Scholar] [CrossRef]
- Ribeiro, L.N.S.; Monteiro, P.M.; Barretto, G.D.; Luiz, K.G.; Alves, S.Y.F.; Stuani, M.B.S. The Effect of Cigarette Smoking and Low-Level Laser Irradiation in RANK/RANKL/OPG Expression. Braz. Dent. J. 2020, 31, 57–62. [Google Scholar] [CrossRef]
- Wheater, G.; Elshahaly, M.; Tuck, S.P.; Datta, H.K.; van Laar, J.M. The clinical utility of bone marker measurements in osteoporosis. J. Transl. Med. 2013, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Huttunen, R.; Heikkinen, T.; Syrjänen, J. Smoking and the outcome of infection. J. Intern. Med. 2010, 269, 258–269. [Google Scholar] [CrossRef]
- Arcavi, L.; Benowitz, N.L. Cigarette Smoking and Infection. Arch. Intern. Med. 2004, 164, 2206–2216. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, J.; Schuind, F. Tobacco and bone fractures: A review of the facts and issues that every orthopaedic surgeon should know. Bone Jt. Res. 2019, 8, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Krueger, J.K.; Rohrich, R.J. Clearing the smoke: The scientific rationale for tobacco abstention with plastic surgery. Plast. Reconstr. Surg. 2001, 108, 1063–1067. [Google Scholar] [CrossRef]
- Pearson, R.G.; Clement, R.; Edwards, K.; Scammell, B.E. Do smokers have greater risk of delayed and non-union after fracture, osteotomy and arthrodesis? A systematic review with meta-analysis. BMJ Open 2016, 6, e010303. [Google Scholar] [CrossRef]
- Matson, A.P.; Hamid, K.S.; Adams, S.B. Predictors of Time to Union After Operative Fixation of Closed Ankle Fractures. Foot Ankle Spec. 2017, 10, 308–314. [Google Scholar] [CrossRef]
- Hernigou, J.; Schuind, F. Smoking as a predictor of negative outcome in diaphyseal fracture healing. Int. Orthop. 2013, 37, 883–887. [Google Scholar] [CrossRef] [PubMed]
- Adams, C.; Keating, J.; Court-Brown, C. Cigarette smoking and open tibial fractures. Injury 2001, 32, 61–65. [Google Scholar] [CrossRef]
- Baron, J.A.; Farahmand, B.Y.; Weiderpass, E.; Michaëlsson, K.; Alberts, A.; Persson, I.; Ljunghall, S. Cigarette Smoking, Alcohol Consumption, and Risk of Hip Fracture in Women. Arch. Intern. Med. 2001, 161, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Scolaro, J.A.; Schenker, M.L.; Yannascoli, S.M.; Baldwin, K.; Mehta, S.; Ahn, J. Cigarette Smoking Increases Complications Following Fracture: A systematic review. JBJS 2014, 96, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-J.; Jou, I.-M.; Wu, T.-T.; Su, F.-C.; Tai, T.-W. Cigarette smoke inhalation impairs angiogenesis in early bone healing processes and delays fracture union. Bone Jt. Res. 2020, 9, 99–107. [Google Scholar] [CrossRef]
- Wong, L.S.; Martins-Green, M. Firsthand cigarette smoke alters fibroblast migration and survival: Implications for impaired healing. Wound Repair Regen. 2004, 12, 471–484. [Google Scholar] [CrossRef]
- Shabestari, M.; Kise, N.J.; Landin, M.A.; Sesseng, S.; Hellund, J.C.; Reseland, J.E.; Eriksen, E.F.; Haugen, I.K. Enhanced angiogenesis and increased bone turnover characterize bone marrow lesions in osteoarthritis at the base of the thumb. Bone Jt. Res. 2018, 7, 406–413. [Google Scholar] [CrossRef]
- Aspera-Werz, R.H.; Chen, T.; Ehnert, S.; Zhu, S.; Fröhlich, T.; Nussler, A.K. Cigarette Smoke Induces the Risk of Metabolic Bone Diseases: Transforming Growth Factor Beta Signaling Impairment via Dysfunctional Primary Cilia Affects Migration, Proliferation, and Differentiation of Human Mesenchymal Stem Cells. Int. J. Mol. Sci. 2019, 20, 2915. [Google Scholar] [CrossRef]
- Giorgetti, A.P.O.; Neto, J.B.C.; Ruiz, K.G.S.; Casati, M.Z.; Sallum, E.A.; Nociti, F.H. Cigarette smoke inhalation modulates gene expression in sites of bone healing: A study in rats. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2010, 110, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Gaston, M.S.; Simpson, A.H.R.W. Inhibition of fracture healing. J. Bone Jt. Surg. 2007, 89, 1553–1560. [Google Scholar] [CrossRef] [PubMed]
- Effeney, D.J. Prostacyclin production by the heart: Effect of nicotine and carbon monoxide. J. Vasc. Surg. 1987, 5, 237–247. [Google Scholar] [CrossRef]
- Chen, Y.; Guo, Q.; Pan, X.; Qin, L.; Zhang, P. Smoking and impaired bone healing: Will activation of cholinergic anti-inflammatory pathway be the bridge? Int. Orthop. 2011, 35, 1267–1270. [Google Scholar] [CrossRef] [PubMed]
- Cornuz, J.; Feskanich, D.; Willett, W.C.; Colditz, G. Smoking, smoking cessation, and risk of hip fracture in women. Am. J. Med. 1999, 106, 311–314. [Google Scholar] [CrossRef]
- Gerdhem, P.; Obrant, K.J. Effects of Cigarette-Smoking on Bone Mass as Assessed by Dual-Energy X-ray Absorptiometry and Ultrasound. Osteoporos. Int. 2002, 13, 932–936. [Google Scholar] [CrossRef]
- Oncken, C.; Prestwood, K.M.; Cooney, J.L.; Unson, C.; Fall, P.; Kulldorff, M.; Raisz, L.G. Effects of smoking cessation or reduction on hormone profiles and bone turnover in postmenopausal women. Nicotine Tob. Res. 2002, 4, 451–458. [Google Scholar] [CrossRef]
- Oncken, C.; Prestwood, K.; Kleppinger, A.; Wang, Y.; Cooney, J.; Raisz, L. Impact of Smoking Cessation on Bone Mineral Density in Postmenopausal Women. J. Women Health 2006, 15, 1141–1150. [Google Scholar] [CrossRef]
- Doll, R.; Peto, R.; Boreham, J.; Sutherland, I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ 2004, 328, 1519. [Google Scholar] [CrossRef]
- Ru, J.-Y.; Chen, L.-X.; Hu, F.-Y.; Shi, D.; Xu, R.; Du, J.-W.; Niu, Y.-F. Factors associated with development of re-nonunion after primary revision in femoral shaft nonunion subsequent to failed intramedullary nailing. J. Orthop. Surg. Res. 2018, 13, 180. [Google Scholar] [CrossRef]
- Taormina, D.P.; Shulman, B.S.; Karia, R.; Spitzer, A.B.; Konda, S.R.; Egol, K.A. Older Age Does Not Affect Healing Time and Functional Outcomes After Fracture Nonunion Surgery. Geriatr. Orthop. Surg. Rehabil. 2014, 5, 116–121. [Google Scholar] [CrossRef]
- Mills, E.; Eyawo, O.; Lockhart, I.; Kelly, S.; Wu, P.; Ebbert, J.O. Smoking Cessation Reduces Postoperative Complications: A Systematic Review and Meta-analysis. Am. J. Med. 2011, 124, 144–154.e8. [Google Scholar] [CrossRef]
- Cusano, N.E. Skeletal Effects of Smoking. Curr. Osteoporos. Rep. 2015, 13, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Leibson, C.L.; Tosteson, A.N.A.; Gabriel, S.E.; Ransom, J.E.; Melton, L.J., III. Mortality, Disability, and Nursing Home Use for Persons with and without Hip Fracture: A Population-Based Study. J. Am. Geriatr. Soc. 2002, 50, 1644–1650. [Google Scholar] [CrossRef] [PubMed]
- Vega, D.; Maalouf, N.M.; Sakhaee, K. The Role of Receptor Activator of Nuclear Factor-κB (RANK)/RANK Ligand/Osteoprotegerin: Clinical Implications. J. Clin. Endocrinol. Metab. 2007, 92, 4514–4521. [Google Scholar] [CrossRef] [PubMed]
- Leibbrandt, A.; Penninger, J.M. RANK/RANKL: Regulators of immune responses and bone physiology. Ann. N. Y. Acad. Sci. 2008, 1143, 123–150. [Google Scholar] [CrossRef]
- Lindström, D.; Azodi, O.S.; Wladis, A.; Tønnesen, H.; Linder, S.; Nåsell, H.; Ponzer, S.; Adami, J. Effects of a Perioperative Smoking Cessation Intervention on Postoperative Complications: A randomized trial. Ann. Surg. 2008, 248, 739–745. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| INDIRECT EFFECTS | Pathophysiological Mechanism | Methods | Bone Effects | References |
| Nicotine causes an alteration in body weight, suppressing appetite and increasing dopamine and serotonin levels |
| Weight loss causes a decrease in the mechanical load on the skeletal system, leading to a decrease in BMD | [23] | |
| [24] | |||
| [28] | |||
| [26] | |||
| Tobacco suppresses PTH, cholecalciferol, and calcitriol production Nicotine increases skin aging, causing it to lose its capacity to synthesize cholecalciferol |
| The reduction in serum levels of PTH and consequent vitamin D activation causes a decrease in BMD | [33] | |
| [34] | |||
| [30] | |||
| Smoking causes a decrease in testosterone levels Some alkaloids derived from tobacco inhibit the activity of the aromatic enzyme, exerting an antiestrogenic effects |
| The decrease in gonadal hormone levels causes a reduction in the activity and proliferation of osteoblasts and an increase in the resorption activity of osteoclasts | [35] | |
| [36] | |||
| Smoking causes an increase in levels of adrenocorticotrophin, causing a consequent increase in circulating cortisol levels |
| Cortisol causes a reduction in collagen and bone matrix synthesis | [41] | |
| DIRECT EFFECTS | Smoking causes an increase in the RANKL/OPG ratio |
| Increase in osteoclastogenesis and bone resorption | [45] |
| [46] | |||
| Smoking causes an increase in DKK1 (bone formation inhibitor) levels and a decrease in P1NP (bone formation marker) levels |
| Alteration of bone formation | [30] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarantino, U.; Cariati, I.; Greggi, C.; Gasbarra, E.; Belluati, A.; Ciolli, L.; Maccauro, G.; Momoli, A.; Ripanti, S.; Falez, F.; et al. Skeletal System Biology and Smoke Damage: From Basic Science to Medical Clinic. Int. J. Mol. Sci. 2021, 22, 6629. https://doi.org/10.3390/ijms22126629
Tarantino U, Cariati I, Greggi C, Gasbarra E, Belluati A, Ciolli L, Maccauro G, Momoli A, Ripanti S, Falez F, et al. Skeletal System Biology and Smoke Damage: From Basic Science to Medical Clinic. International Journal of Molecular Sciences. 2021; 22(12):6629. https://doi.org/10.3390/ijms22126629
Chicago/Turabian StyleTarantino, Umberto, Ida Cariati, Chiara Greggi, Elena Gasbarra, Alberto Belluati, Luigi Ciolli, Giulio Maccauro, Alberto Momoli, Simone Ripanti, Francesco Falez, and et al. 2021. "Skeletal System Biology and Smoke Damage: From Basic Science to Medical Clinic" International Journal of Molecular Sciences 22, no. 12: 6629. https://doi.org/10.3390/ijms22126629
APA StyleTarantino, U., Cariati, I., Greggi, C., Gasbarra, E., Belluati, A., Ciolli, L., Maccauro, G., Momoli, A., Ripanti, S., Falez, F., & Brandi, M. L. (2021). Skeletal System Biology and Smoke Damage: From Basic Science to Medical Clinic. International Journal of Molecular Sciences, 22(12), 6629. https://doi.org/10.3390/ijms22126629