
Effectiveness of COVID-19 Vaccines in the General Population of an Italian Region before and during the Omicron Wave

 ,
,  ,
, 
Abstract
:1. Introduction
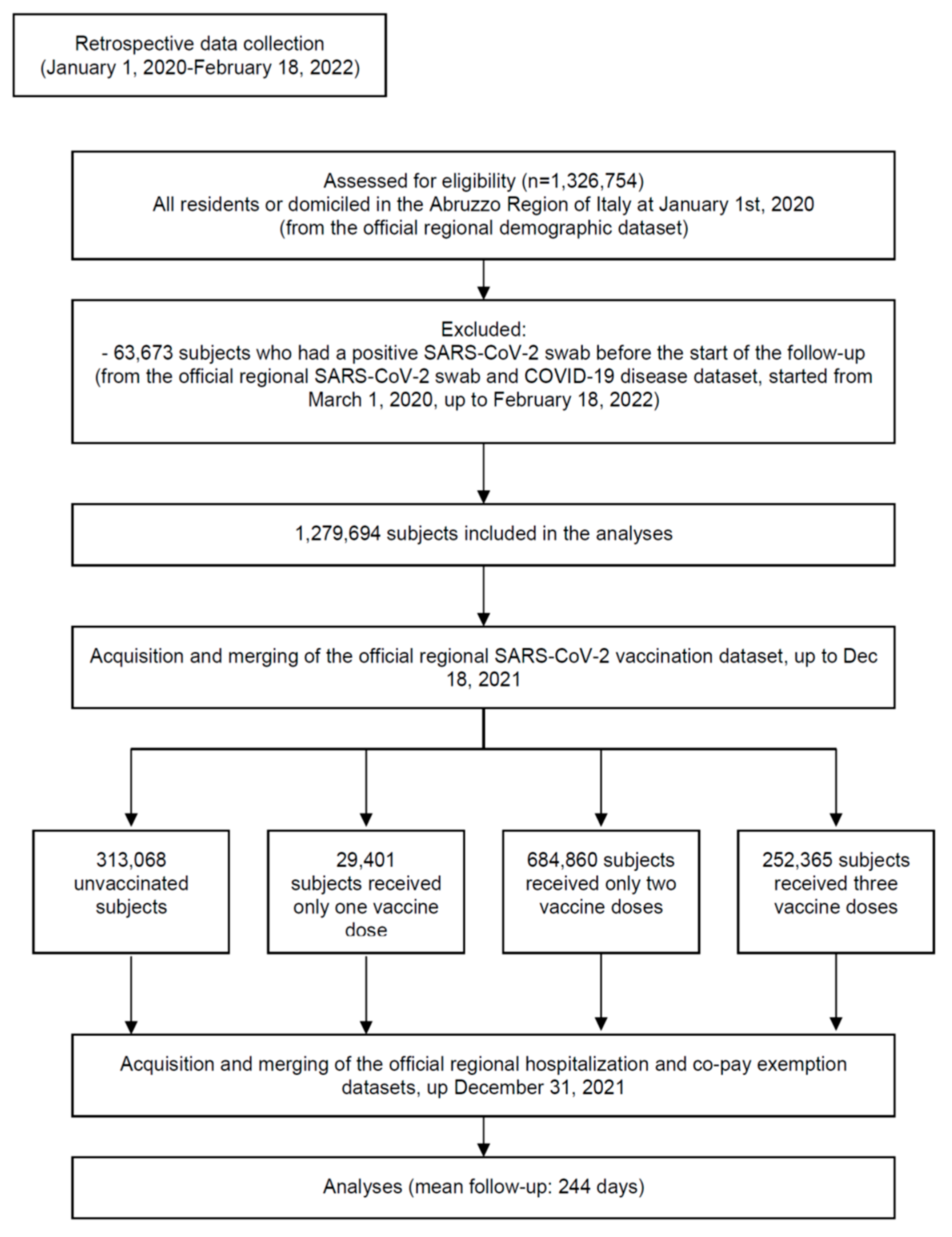
2. Materials and Methods
- The subjects who received only one dose of BNT162b2, mRNA-1273 or ChAdOx1 nCoV-19 vaccines, were included in the group “1 dose”;
- The subjects who received only one dose of JNJ-78436735 vaccine, or only two doses of BNT162b2, mRNA-1273 or ChAdOx1 nCoV-19 vaccines, were included in the group “2 doses”;
- The subjects who received two doses of JNJ-78436735 vaccine, or three doses of BNT162b2, mRNA-1273 or ChAdOx1 nCoV-19 vaccines, were included in the group “3 doses”.
- For the analyses comparing unvaccinated versus those receiving only one vaccine dose (set of analyses “1 dose”), the start of follow-up was set 14 days after the single vaccine dose (to account for the time required for seroconversion) [27] for vaccinated subjects and 14 days after the first administration of the first vaccine dose (16 January 2021) for the group “unvaccinated”.
- For the analyses comparing unvaccinated versus those receiving two vaccine doses only (set of analyses “2 doses”), the start of follow-up was set 14 days after the second vaccine dose for vaccinated subjects and 14 days after the first administration of the second vaccine dose (31 January 2021) for the group “unvaccinated”.
- For the analyses comparing unvaccinated versus those receiving three vaccine doses (set of analyses “3 doses”), the start of follow-up was set 14 days after the third vaccine dose for vaccinated subjects and 14 days after the start of the mass administration of the third vaccine dose (17 September 2021) for the group “unvaccinated”.
- −
- On 18 February 2022 for those who had no positive swabs during the follow-up;
- −
- On the day of the first positive swab for those who were not infected before the start of the follow-up (“uninfected” cohort).
2.1. Data Collection
2.2. Statistical Analyses
3. Results
3.1. Risk of Primary Infection
3.2. Risk of COVID-19 Hospitalization
3.3. Risk of COVID-19-Related Death
3.4. Vaccine Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- USA Department of Health & Human Services. Secretarial Directive of Eligibility to Receive COVID-19 Vaccines—17 March 2021; USA Department of Health & Human Services: Washington, DC, USA, 2021.
- European Commission. Communication from the Commission to the European Parliament, the European Council and the Council—A United Front to Beat COVID-19; European Commission: Brussels, Belgium, 2021; Volume 19.1.2021, COM (2021) 35 final.
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Sobieszczyk, M.E.; Hirsch, I.; Sproule, S.; Robb, M.L.; Corey, L.; Neuzil, K.M.; Hahn, W.; Hunt, J.; Mulligan, M.J.; et al. Phase 3 Safety and Efficacy of AZD1222 (ChAdOx1 nCoV-19) COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 2348–2360. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef]
- Tanriover, M.D.; Doğanay, H.L.; Akova, M.; Güner, H.R.; Azap, A.; Akhan, S.; Köse, Ş.; Erdinç, F.Ş.; Akalın, E.H.; Tabak, Ö.F.; et al. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): Interim results of a double-blind, randomised, placebo-controlled, phase 3 trial in Turkey. Lancet 2021, 398, 213–222. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Soldato, G.; Acuti Martellucci, C.; Carota, R.; Di Luzio, R.; Caponetti, A.; Manzoli, L. Interim Estimates of COVID-19 Vaccine Effectiveness in a Mass Vaccination Setting: Data from an Italian Province. Vaccines 2021, 9, 628. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet Lond. Engl. 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Thompson, M.G.; Burgess, J.L.; Naleway, A.L.; Tyner, H.; Yoon, S.K.; Meece, J.; Olsho, L.E.W.; Caban-Martinez, A.J.; Fowlkes, A.L.; Lutrick, K.; et al. Prevention and Attenuation of COVID-19 with the BNT162b2 and mRNA-1273 Vaccines. N. Engl. J. Med. 2021, 385, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Tenforde, M.W.; Rhoads, J.P.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; et al. Comparative Effectiveness of Moderna, Pfizer-BioNTech, and Janssen (Johnson & Johnson) Vaccines in Preventing COVID-19 Hospitalizations Among Adults Without Immunocompromising Conditions—United States, March–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of Protection against Mild and Severe Disease by COVID-19 Vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef]
- Fabiani, M.; Puopolo, M.; Morciano, C.; Spuri, M.; Spila Alegiani, S.; Filia, A.; D’Ancona, F.; Del Manso, M.; Riccardo, F.; Tallon, M.; et al. Effectiveness of mRNA vaccines and waning of protection against SARS-CoV-2 infection and severe COVID-19 during predominant circulation of the delta variant in Italy: Retrospective cohort study. BMJ 2022, 376, e069052. [Google Scholar] [CrossRef]
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 10 January 2022).
- Collie, S.; Champion, J.; Moultrie, H.; Bekker, L.-G.; Gray, G. Effectiveness of BNT162b2 Vaccine against Omicron Variant in South Africa. N. Engl. J. Med. 2021, 386, 494–496. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Dorabawila, V.; Easton, D.; Bauer, U.E.; Kumar, J.; Hoen, R.; Hoefer, D.; Wu, M.; Lutterloh, E.; Conroy, M.B.; et al. COVID-19 Vaccine Effectiveness in New York State. N. Engl. J. Med. 2021, 386, 116–127. [Google Scholar] [CrossRef]
- Fast, H.E.; Zell, E.; Murthy, B.P.; Murthy, N.; Meng, L.; Gibbs Scharf, L.; Black, C.L.; Shaw, L.; Chorba, T.; Harris, L.Q. Booster and Additional Primary Dose COVID-19 Vaccinations Among Adults Aged ≥65 Years—United States, August 13, 2021–November 19, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1735–1739. [Google Scholar] [CrossRef]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to COVID-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef]
- Acuti Martellucci, C.; Flacco, M.E.; Cappadona, R.; Bravi, F.; Mantovani, L.; Manzoli, L. SARS-CoV-2 pandemic: An overview. Adv. Biol. Regul. 2020, 77, 100736. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Health. Piano Vaccini Anti COVID-19 [Italian Mational Immunization Plan against COVID-19]; Italian Ministry of Health: Roma, Italy, 2020.
- Italian Government. Decreto Legge: Misure urgenti per fronteggiare l’emergenza COVID-19. In Particolare Nei Luoghi Di Lavoro, Nelle Scuole E Negli Istituti Della Formazione Superiore; Government, I., Ed.; Gazzetta Ufficiale S.G. n. 4: Roma, Italy, 2022; Volume Decreto Legge n. 1. [Google Scholar]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Coyle, P.; Al Kanaani, Z.; et al. Association of Prior SARS-CoV-2 Infection With Risk of Breakthrough Infection Following mRNA Vaccination in Qatar. JAMA 2021, 326, 1930–1939. [Google Scholar] [CrossRef] [PubMed]
- Bravi, F.; Flacco, M.E.; Carradori, T.; Volta, C.A.; Cosenza, G.; De Togni, A.; Acuti Martellucci, C.; Parruti, G.; Mantovani, L.; Manzoli, L. Predictors of severe or lethal COVID-19, including Angiotensin Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers, in a sample of infected Italian citizens. PLoS ONE 2020, 15, e0235248. [Google Scholar] [CrossRef] [PubMed]
- Riccardo, F.; Andrianou, X.; Bella, A.; Del Manso, M.; Urdiales, A.M.; Fabiani, M.; Bellino, S.; Boros, S.; D’Ancona, F.; Rota, M.C.; et al. COVID-19 Integrated Surveillance System. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-sorveglianza (accessed on 7 January 2022).
- Italian Government. Proroga Dello Stato Di Emergenza Nazionale E Ulteriori Misure per Il Contenimento Della Diffusione Dell’epidemia da COVID-19; Italian Government, Ed.; Serie Generale, n. 305; Gazzetta Ufficiale: Roma, Italy, 2021.
- Italian Institute of Health. Characteristics of COVID-19 Patients Dying in Italy Report Based on Available Data on 10 January 2022; Italian Institute of Health: Rome, Italy, 2022.
- Italian Government. Raccomandazioni Ad Interim Sui Gruppi Target Della Vaccinazione Anti SARS-CoV-2/COVID-19; Italian Government, Ed.; Serie Generale, n. 72; Gazzetta Ufficiale: Rome, Italy, 2021.
- Pouwels, K.B.; Pritchard, E.; Matthews, P.C.; Stoesser, N.; Eyre, D.W.; Vihta, K.D.; House, T.; Hay, J.; Bell, J.I.; Newton, J.N.; et al. Effect of Delta variant on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK. Nat. Med. 2021, 27, 2127–2135. [Google Scholar] [CrossRef]
- Pizzi, C.; Costa, G.M.; Santarella, L.; Flacco, M.E.; Capasso, L.; Bert, F.; Manzoli, L. Depression symptoms and the progression of carotid intima-media thickness: A 5-year follow-up study. Atherosclerosis 2014, 233, 530–536. [Google Scholar] [CrossRef] [Green Version]
- Italian National Institute of Health. Stima Della Prevalenza Delle Varianti VOC (Variants of Concern) in Italia: Beta, Gamma, Delta, Omicron E Altre Varianti Di SARS-CoV-2; Italian National Institute of Health: Roma, Italy, 2021.
- Agenzia Italiana del Farmaco (AIFA). Rapporto Annuale Sulla Sicurezza Dei Vaccini Anti-COVID-19; AIFA: Rome, Italy, 2022.
- Abu-Raddad, L.J.; Chemaitelly, H.; Butt, A.A. Effectiveness of the BNT162b2 COVID-19 vaccine against the B.1.1.7 and B.1.351 variants. N. Engl. J. Med. 2021, 385, 187–189. [Google Scholar] [CrossRef]
- Charmet, T.; Schaeffer, L.; Grant, R.; Galmiche, S.; Chény, O.; Von Platen, C.; Maurizot, A.; Rogoff, A.; Omar, F.; David, C.; et al. Impact of original, B.1.1.7, and B.1.351/P.1 SARS-CoV-2 lineages on vaccine effectiveness of two doses of COVID-19 mRNA vaccines: Results from a nationwide case-control study in France. Lancet Reg. Health—Eur. 2021, 8, 100171. [Google Scholar] [CrossRef]
- Nordström, P.; Ballin, M.; Nordström, A. Effectiveness of heterologous ChAdOx1 nCoV-19 and mRNA prime-boost vaccination against symptomatic COVID-19 infection in Sweden: A nationwide cohort study. Lancet Reg. Health—Eur. 2021, 11, 100249. [Google Scholar] [CrossRef]
- UK Health Security Agency. COVID-19 Vaccine Surveillance Report Week 4; UK Health Security Agency: London, UK, 2022.
- Thompson, M.G.; Natarajan, K.; Irving, S.A.; Rowley, E.A.; Griggs, E.P.; Gaglani, M.; Klein, N.P.; Grannis, S.J.; DeSilva, M.B.; Stenehjem, E.; et al. Effectiveness of a Third Dose of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 139–145. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Amir, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection by 4th dose of BNT162b2 against Omicron in Israel. N. Engl. J. Med. 2022. NEJMoa2201570. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.; Richterman, A.; Cevik, M. COVID-19 vaccination: Evidence of waning immunity is overstated. BMJ 2021, 374, n2320. [Google Scholar] [CrossRef] [PubMed]
- Italian Government. Decreto Legge: Misure Urgenti per La Graduale Ripresa Delle Attivita’ Economiche E Sociali Nel Rispetto Delle Esigenze Di Contenimento Della Diffusione Dell’epidemia Da COVID-19; Italian Government: Roma, Italy, 2021; Gazzetta Ufficiale S.G. 96, Volume D.L. n. 52.
- Bhopal, S.S.; Bagaria, J.; Olabi, B.; Bhopal, R. Children and young people remain at low risk of COVID-19 mortality. Lancet Child Adolesc Health 2021, 5, e12–e13. [Google Scholar] [CrossRef]
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Italian Agency of Drugs (AIFA). Annual Report on the Safety of Anti-COVID-19 Vaccines; Italian Agency of Drugs (AIFA): Rome, Italy, 2022.
- Doshi, P.; Godlee, F.; Abbasi, K. COVID-19 vaccines and treatments: We must have raw data, now. BMJ 2022, 376, o102. [Google Scholar] [CrossRef]
- Andersson, O.; Campos-Mercade, P.; Meier, A.N.; Wengström, E. Anticipation of COVID-19 vaccines reduces willingness to socially distance. J. Health Econ. 2021, 80, 102530. [Google Scholar] [CrossRef]
- Sullivan, S.G.; Tchetgen Tchetgen, E.J.; Cowling, B.J. Theoretical Basis of the Test-Negative Study Design for Assessment of Influenza Vaccine Effectiveness. Am. J. Epidemiol. 2016, 184, 345–353. [Google Scholar] [CrossRef]

{kind=link}
| Unvaccinated | 1 Dose A | 2 Doses B | 3 Doses C | Total Sample | |
|---|---|---|---|---|---|
| (n = 313,068) | (n = 29,401) | (n = 684,860) | (n = 252,365) | (n = 1,279,694) | |
| Gender | |||||
| Females | 23.9 | 2.3 | 52.8 | 21.0 | 50.9 (651,752) |
| Males | 25.1 | 2.3 | 54.2 | 18.4 | 49.1 (627,942) |
| Mean age in years (SD) | 35.3 (26.6) | 41.6 (21.6) | 47.6 (19.7) | 64.3 (16.9) | 47.8 (23.3) |
| Age category in years | |||||
| 0–29 | 45.6 | 3.3 | 48.4 | 2.7 | 25.3 (323,613) |
| 30–59 | 19.2 | 2.4 | 61.8 | 16.7 | 42.0 (537,148) |
| 60 or more | 15.0 | 1.4 | 46.8 | 36.8 | 32.7 (418,933) |
| Risk factors and comorbiditiesD | |||||
| No hypertension | 25.8 | 2.4 | 55.3 | 16.4 | 87.4 (1,117,986) |
| Hypertension | 14.9 | 1.4 | 41.1 | 42.6 | 12.6 (161,708) |
| No diabetes | 24.9 | 2.3 | 54.4 | 18.4 | 94.7 (1,212,278) |
| Diabetes | 16.8 | 1.4 | 38.4 | 43.3 | 5.3 (67,416) |
| No CVD | 24.8 | 2.3 | 54.7 | 18.2 | 93.6 (1,198,232) |
| CVD | 19.7 | 1.5 | 36.7 | 42.0 | 6.4 (81,462) |
| No COPD | 24.5 | 2.3 | 53.8 | 19.4 | 97.5 (1,247,276) |
| COPD | 25.1 | 2.0 | 42.2 | 30.7 | 2.5 (32,418) |
| No kidney disease | 24.4 | 2.3 | 53.9 | 19.5 | 98.5 (1,260,117) |
| Kidney disease | 30.3 | 1.6 | 31.7 | 36.4 | 1.5 (19,577) |
| No cancer | 24.7 | 2.3 | 54.3 | 18.7 | 95.4 (1,220,868) |
| Cancer | 20.6 | 1.2 | 36.7 | 41.5 | 4.6 (58,826) |
| Type of vaccineE | |||||
| BNT162b2 | -- | 64.6 | 65.4 | 59.7 | 63.9 (617,751) |
| mRNA-1273 | -- | 29.7 | 14.2 | 7.6 | 13.0 (125,551) |
| ChAdOx1 nCoV-19 | -- | 5.7 | 16.1 | 0.1 | 11.5 (111,658) |
| JNJ-78436735 | -- | -- | 1.7 | 0.0 | 1.2 (11,510) |
| Mixed F | -- | -- | 2.6 | 32.6 | 10.4 (100,156) |
| Mean follow-up in days (SD) G | 367 (58) | 130 (87) | 188 (51) | 71 (18) | 244 (99) |
| SARS-CoV-2-positive swab before the second dose H | 0.3 (877) | -- | 0.4 (2758) | 0.1 (236) | 0.3 (3871) |
| SARS-CoV-2-positive swab before the third dose H | 4.7 (14,835) | -- | -- | 0.7 (1745) | 1.3 (16,580) |
| Variables | Total Sample | Unvaccinated | 1 Dose A | 2 Doses B | 3 Doses C |
|---|---|---|---|---|---|
| (n = 1,279,694) | (n = 313,068) | (n = 29,401) | (n = 684,860) | (n = 252,365) | |
| Health status | |||||
| Whole period | |||||
| All subjects | n = 1,275,823 D | n = 312,191 | n = 29,401 | n = 682,102 | n = 250,620 |
| SARS-CoV-2-positive swab | 13.4 (170,761) | 19.1 (59,770) | 13.8 (4053) | 13.1 (89,236) | 6.5 (16,193) |
| COVID-19 hospitalization | 0.15 (1910) | 0.41 (1270) | 0.22 (66) | 0.06 (390) | 0.06 (162) |
| COVID-19-related death | 0.08 (1050) | 0.28 (872) | 0.13 (39) | 0.02 (105) | 0.01 (31) |
| Infected subjects only | n = 170,761 D | n = 59,770 | n = 4053 | n = 89,236 | n = 16,193 |
| COVID-19 among the infected | 1.12 (1910) | 2.12 (1270) | 1.63 (66) | 0.44 (390) | 1.00 (162) |
| Death among the infected | 0.61 (1050) | 1.46 (872) | 0.96 (39) | 0.12 (105) | 0.19 (31) |
| Pre-Omicron WavesE | |||||
| All subjects | n = 1,275,823 D | n = 312,191 | n = 29,401 | n = 682,102 | n = 250,620 |
| SARS-CoV-2-positive swab | 2.4 (30,726) | 5.9 (18,489) | 3.4 (1013) | 1.4 (9449) | 0.1 (266) |
| COVID-19 hospitalization | 0.09 (1152) | 0.31 (975) | 0.15 (44) | 0.02 (107) | 0.00 (4) |
| COVID-19-related death | 0.07 (933) | 0.27 (831) | 0.12 (35) | 0.01 (63) | 0.00 (1) |
| Infected subjects only | n = 30,726 D | n = 18,489 | n = 1013 | n = 9449 | n = 266 |
| COVID-19 among the infected | 3.75 (1152) | 5.27 (975) | 4.34 (44) | 1.13 (107) | 1.50 (4) |
| Death among the infected | 3.04 (933) | 4.49 (831) | 3.46 (35) | 0.67 (63) | 0.38 (1) |
| Omicron Wave F | |||||
| All subjects | n = 1,245,097 D | n = 293,702 | n = 28,388 | n = 672,653 | n = 250,354 |
| SARS-CoV-2-positive swab | 11.2 (140,035) | 14.1 (41,281) | 10.7 (3040) | 11.9 (79,787) | 6.4 (15,927) |
| COVID-19 hospitalization | 0.06 (758) | 0.10 (295) | 0.08 (22) | 0.04 (283) | 0.06 (158) |
| COVID-19-related death | 0.01 (117) | 0.01 (41) | 0.01 (4) | 0.01 (42) | 0.01 (30) |
| Infected subjects only | n = 140,035 D | n = 41,281 | n = 3040 | n = 79,787 | n = 15,927 |
| COVID-19 among the infected | 0.54 (758) | 0.71 (295) | 0.72 (22) | 0.35 (283) | 0.99 (158) |
| Death among the infected | 0.08 (117) | 0.10 (41) | 0.13 (4) | 0.05 (42) | 0.19 (30) |
| Age category | |||||
| 0–29 years | n = 322,643 D | n = 146,948 | n = 10,567 | n = 156,352 | n = 8658 |
| SARS-CoV-2-positive swab | 21.8 (70,345) | 26.2 (38,494) | 16.6 (1755) | 18.5 (28,895) | 12.9 (1113) |
| COVID-19 hospitalization | 0.01 (24) | 0.01 (19) | 0.00 (0) | 0.00 (4) | 0.01 (1) |
| COVID-19-related death | 0.00 (0) | 0.00 (0) | 0.00 (0) | 0.00 (0) | 0.00 (0) |
| 30–59 years | n = 535,525 D | n = 102,594 | n = 12,873 | n = 330,649 | n = 88,639 |
| SARS-CoV-2-positive swab | 13.8 (73,852) | 15.8 (16,177) | 14.1 (1820) | 14.1 (46,473) | 9.7 (8612) |
| COVID-19 hospitalization | 0.05 (253) | 0.18 (189) | 0.05 (6) | 0.01 (46) | 0.01 (8) |
| COVID-19-related death | 0.01 (78) | 0.07 (74) | 0.00 (0) | 0.00 (2) | 0.00 (2) |
| 60+ years | n = 417,655 D | n = 62,649 | n = 5961 | n = 195,101 | n = 153,323 |
| SARS-CoV-2-positive swab | 6.3 (26,534) | 8.1 (5099) | 8.0 (478) | 7.1 (13,868) | 4.2 (6468) |
| COVID-19 hospitalization | 0.39 (1633) | 1.70 (1062) | 1.01 (60) | 0.17 (340) | 0.10 (153) |
| COVID-19-related death | 0.23 (972) | 1.27 (798) | 0.65 (39) | 0.05 (103) | 0.02 (29) |
| Vaccine type | |||||
| BNT162b2 | n = 615,841 D | -- | n = 18,994 | n = 446,235 | n = 149,708 |
| SARS-CoV-2-positive swab | 12.2 (74,886) | -- | 14.3 (2709) | 13.8 (61,751) | 6.36 (9522) |
| COVID-19 hospitalization | 0.08 (477) | -- | 0.29 (56) | 0.06 (279) | 0.09 (130) |
| COVID-19-related death | 0.02 (148) | -- | 0.18 (34) | 0.02 (88) | 0.02 (25) |
| mRNA-1273 | n = 125,162 D | -- | n = 8727 | n = 97,237 | n = 19,098 |
| SARS-CoV-2-positive swab | 11.5 (14,458) | -- | 12.2 (1067) | 12.7 (12,369) | 4.8 (922) |
| COVID-19 hospitalization | 0.05 (61) | -- | 0.10 (9) | 0.04 (39) | 0.07 (13) |
| COVID-19-related death | 0.01 (16) | -- | 0.05 (4) | 0.01 (9) | 0.02 (3) |
| ChAdOx1 nCoV-19 | n = 111,570 D | -- | n = 1680 | n = 109,874 | n = 16 |
| SARS-CoV-2-positive swab | 10.5 (11,679) | -- | 16.5 (277) | 10.4 (11,401) | 6.25 (1) |
| COVID-19 hospitalization | 0.06 (65) | -- | 0.06 (1) | 0.06 (64) | 0.00 (0) |
| COVID-19-related death | 0.01 (8) | -- | 0.06 (1) | 0.01 (7) | 0.00 (0) |
| JNJ-78436735 | n = 11,510 D | -- | -- | n = 11,508 | n = 2 |
| SARS-CoV-2-positive swab | 13.1 (1508) | -- | -- | 13.1 (1508) | 0.00 (0) |
| COVID-19 hospitalization | 0.06 (7) | -- | -- | 0.06 (7) | 0.00 (0) |
| COVID-19-related death | 0.00 (0) | -- | -- | 0.00 (0) | 0.00 (0) |
| Mixed G | n = 99,549 D | -- | -- | n = 17,248 | n = 81,796 |
| SARS-CoV-2-positive swab | 8.5 (8460) | -- | -- | 12.8 (2207) | 7.0 (5748) |
| COVID-19 hospitalization | 0.02 (22) | -- | -- | 0.01 (1) | 0.02 (19) |
| COVID-19-related death | 0.01 (6) | -- | -- | 0.01 (1) | 0.00 (3) |
| Follow-up duration H | |||||
| Subjects infected within 6 months from the last dose | n = 102,216 D | n = 8973 | n = 3654 | n = 71,888 | n = 16,192 |
| COVID-19 among the infected | 1.24 (1267) | 9.48 (851) | 1.51 (55) | 0.25 (177) | 1.00 (162) |
| Death among the infected | 0.86 (883) | 8.47 (760) | 0.96 (35) | 0.08 (54) | 0.19 (31) |
| Subjects infected after 6 months from the last dose | n = 68,545 D | n = 50,797 | n = 399 | n = 17,348 | n = 1 |
| COVID-19 among the infected | 0.94 (643) | 0.82 (419) | 2.76 (11) | 1.23 (213) | 0.00 (0) |
| Death among the infected | 0.24 (167) | 0.22 (112) | 1.00 (4) | 0.29 (51) | 0.00 (0) |
| Variables | SARS-CoV-2 | COVID-19 Hospitalization A | COVID-19-Related Death |
|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Health status | |||
| Whole period | |||
| Vaccine doses | |||
| All subjects | |||
| Unvaccinated | 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| 1 dose | 0.71 (0.68–0.73) * | 0.53 (0.41–0.67) * | 0.49 (0.35–0.67) * |
| 2 doses | 0.75 (0.74–0.76) * | 0.12 (0.10–0.13) * | 0.06 (0.05–0.07) * |
| 3 doses | 0.74 (0.73–0.76) * | 0.21 (0.18–0.26) * | 0.24 (0.16–0.37) * |
| Infected subjects only | |||
| Unvaccinated | -- | 1 (Ref. cat.) | 1 (Ref. cat.) |
| 1 dose | -- | 0.44 (0.33–0.58) * | 0.33 (0.23–0.47) * |
| 2 doses | -- | 0.10 (0.09–0.11) * | 0.05 (0.04–0.06) * |
| 3 doses | -- | 0.18 (0.15–0.23) * | 0.15 (0.10–0.24) * |
| Omicron wave B | |||
| All subjects | |||
| Unvaccinated | 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| 2 doses | 0.98 (0.97–1.00) | 0.34 (0.29–0.40) * | 0.68 (0.43–1.09) |
| 3 doses | 0.81 (0.80–0.83) * | 0.25 (0.20–0.30) * | 0.42 (0.26–0.68) * |
| Infected subjects only | |||
| Unvaccinated | 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| 2 doses | -- | 0.21 (0.18–0.25) * | 0.31 (0.20–0.49) * |
| 3 doses | -- | 0.19 (0.16–0.24) * | 0.23 (0.14–0.37) * |
| Vaccine type (2 doses vs. none) | |||
| Unvaccinated | 1 (Ref. cat.) | 1 (Ref. cat.) | 1 (Ref. cat.) |
| BNT162b2 | 0.76 (0.75–0.77) * | 0.14 (0.12–0.16) * | 0.08 (0.06–0.10) * |
| mRNA-1273 | 0.68 (0.66–0.69) * | 0.10 (0.07–0.14) * | 0.04 (0.02–0.08) * |
| ChAdOx1 nCoV-19 | 0.96 (0.94–0.99) ** | 0.07 (0.05–0.08) * | 0.02 (0.01–0.04) * |
| JNJ-78436735 | 0.88 (0.83–0.93) * | 0.13 (0.06–0.27) * | 0.00 (NE) |
| Mixed C | 0.76 (0.72–0.79) * | 0.02 (0.00–0.16) * | 0.04 (0.01–0.28) * |
| Age category, years (2 doses vs. none) | |||
| 60 or more | 0.79 (0.76–0.82) * | 0.14 (0.12–0.16) * | 0.06 (0.05–0.07) * |
| 30–59 | 0.90 (0.88–0.91) * | 0.07 (0.05–0.10) * | 0.01 (0.00–0.03) * |
| 0–29 | 0.85 (0.83–0.87) * | 0.10 (0.03–0.30) * | NE |
| Variables | COVID-19 Hospitalization A | COVID-19-Related Death |
|---|---|---|
| Follow-up duration B | OR (95% CI) | OR (95% CI) |
| ≤6 months of follow-up | ||
| Unvaccinated | 1 (Ref. cat.) | 1 (Ref. cat.) |
| 2 doses | 0.03 (0.02–0.03) * | 0.01 (0.01–0.02) * |
| 3 doses | 0.18 (0.15–0.23) * | 0.15 (0.10–0.24) * |
| >6 months of follow-up | ||
| Unvaccinated | 1 (Ref. cat.) | 1 (Ref. cat.) |
| 2 doses | 0.31 (0.26–0.37) * | 0.25 (0.17–0.35) * |
| 3 doses | NE | NE |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acuti Martellucci, C.; Flacco, M.E.; Soldato, G.; Di Martino, G.; Carota, R.; Caponetti, A.; Manzoli, L. Effectiveness of COVID-19 Vaccines in the General Population of an Italian Region before and during the Omicron Wave. Vaccines 2022, 10, 662. https://doi.org/10.3390/vaccines10050662
Acuti Martellucci C, Flacco ME, Soldato G, Di Martino G, Carota R, Caponetti A, Manzoli L. Effectiveness of COVID-19 Vaccines in the General Population of an Italian Region before and during the Omicron Wave. Vaccines. 2022; 10(5):662. https://doi.org/10.3390/vaccines10050662
Chicago/Turabian StyleAcuti Martellucci, Cecilia, Maria Elena Flacco, Graziella Soldato, Giuseppe Di Martino, Roberto Carota, Antonio Caponetti, and Lamberto Manzoli. 2022. "Effectiveness of COVID-19 Vaccines in the General Population of an Italian Region before and during the Omicron Wave" Vaccines 10, no. 5: 662. https://doi.org/10.3390/vaccines10050662
APA StyleAcuti Martellucci, C., Flacco, M. E., Soldato, G., Di Martino, G., Carota, R., Caponetti, A., & Manzoli, L. (2022). Effectiveness of COVID-19 Vaccines in the General Population of an Italian Region before and during the Omicron Wave. Vaccines, 10(5), 662. https://doi.org/10.3390/vaccines10050662