
Regulation of Alcohol and Acetaldehyde Metabolism by a Mixture of Lactobacillus and Bifidobacterium Species in Human

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Test Supplements
2.2. Subjects
2.3. Genotyping
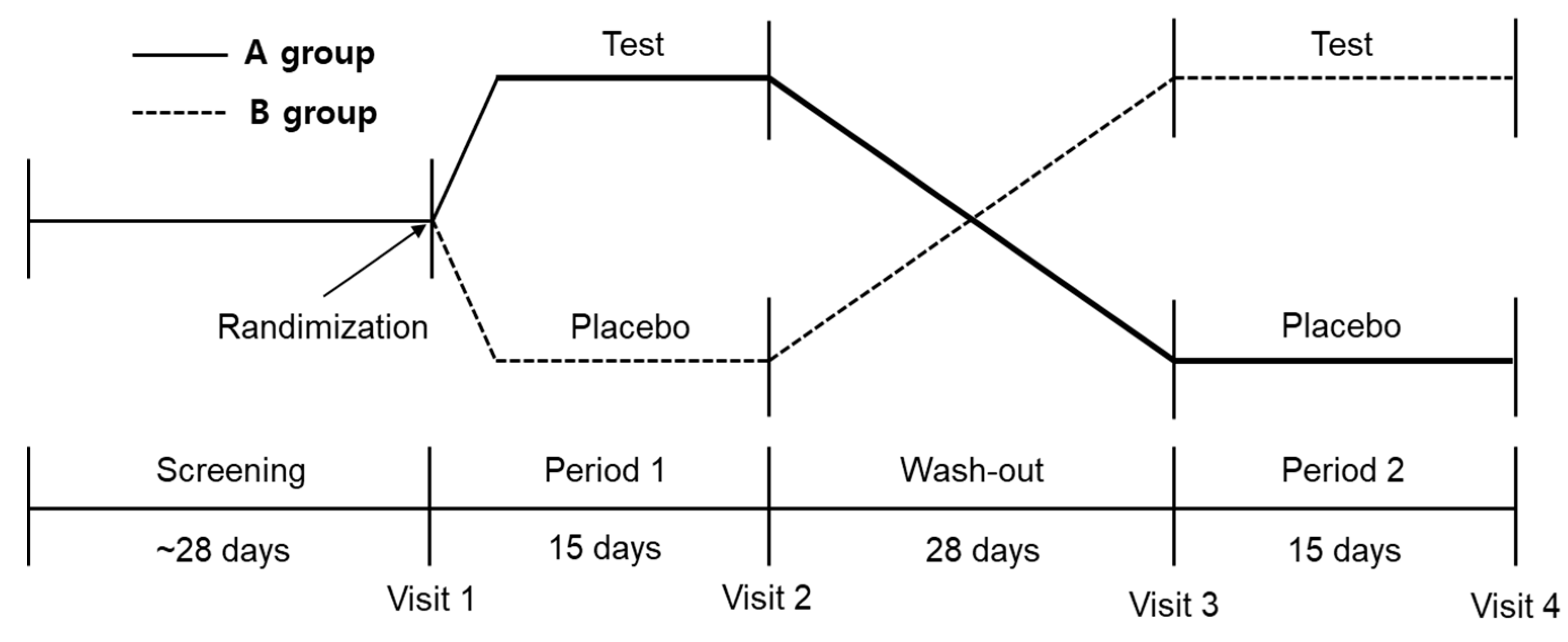
2.4. Study Design
2.5. Alcohol Challenge Test
2.6. Outcome Measurements
2.6.1. Primary Outcomes
2.6.2. Secondary Outcomes
2.7. Safety Outcome Measurements
2.8. Evaluation of Diet and Physical Activity
2.9. Sample Size
2.10. Statistical Analysis
3. Results
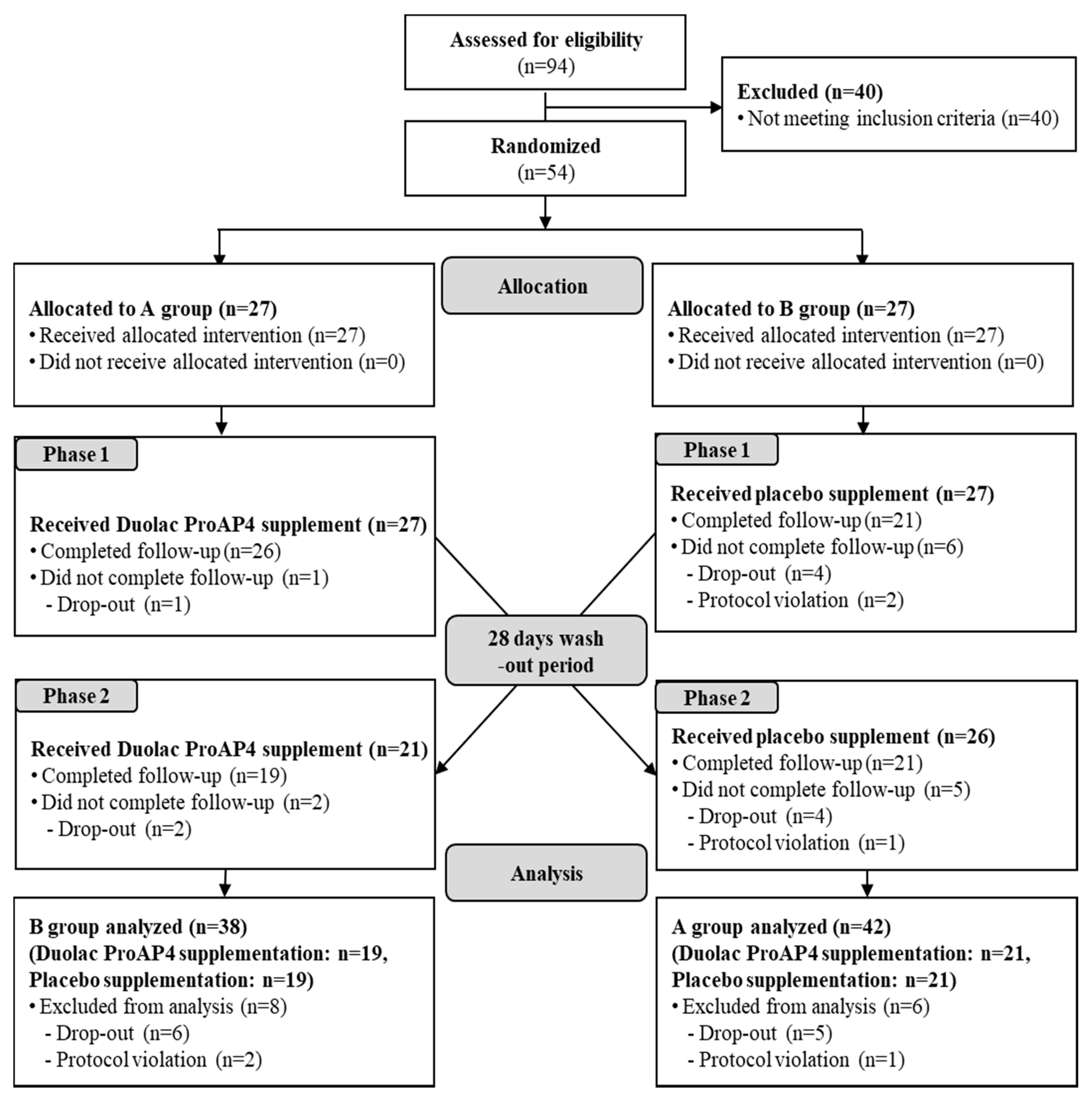
3.1. Demographic Characteristics of Participants
3.2. Diet Intake and Physical Activity
3.3. Efficacy Evaluation
3.3.1. Primary Outcome
3.3.2. Secondary Outcomes
3.4. Safety and Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seitz, H.K.; Bataller, R.; Cortez-Pinto, H.; Gao, B.; Gual, A.; Lackner, C.; Mathurin, P.; Mueller, S.; Szabo, G.; Tsukamoto, H. Alcoholic liver disease. Nat. Rev. Dis. Primers 2018, 4, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Edenberg, H.J.; McClintick, J.N. Alcohol dehydrogenases, aldehyde dehydrogenases, and alcohol use disorders: A critical review. Alcohol. Clin. Exp. Res. 2018, 42, 2281–2297. [Google Scholar] [CrossRef]
- Eng, M.Y.; Luczak, S.E.; Wall, T.L. ALDH2, ADH1B, and ADH1C genotypes in Asians: A literature review. Alcohol Res. Health 2007, 30, 22. [Google Scholar]
- Yokoyama, M.; Yokoyama, A.; Yokoyama, T.; Funazu, K.; Hamana, G.; Kondo, S.; Yamashita, T.; Nakamura, H. Hangover susceptibility in relation to aldehyde dehydrogenase-2 genotype, alcohol flushing, and mean corpuscular volume in Japanese workers. Alcohol. Clin. Exp. Res. 2005, 29, 1165–1171. [Google Scholar] [CrossRef]
- Gu, Z.; Wu, Y.; Wang, Y.; Sun, H.; You, Y.; Piao, C.; Liu, J.; Wang, Y. Lactobacillus rhamnosus granules dose-dependently balance intestinal microbiome disorders and ameliorate chronic alcohol-induced liver injury. J. Med. Food 2020, 23, 114–124. [Google Scholar] [CrossRef]
- Tian, F.; Chi, F.; Wang, G.; Liu, X.; Zhang, Q.; Chen, Y.; Zhang, H.; Chen, W. Lactobacillus rhamnosus CCFM1107 treatment ameliorates alcohol-induced liver injury in a mouse model of chronic alcohol feeding. J. Microbiol. 2015, 53, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Wang, Y.; You, Y.; Ai, Z.; Dai, W.; Piao, C.; Liu, J.; Wang, Y. Fermented ginseng improved alcohol liver injury in association with changes in the gut microbiota of mice. Food Funct. 2019, 10, 5566–5573. [Google Scholar] [CrossRef]
- Kirpich, I.A.; Solovieva, N.V.; Leikhter, S.N.; Shidakova, N.A.; Lebedeva, O.V.; Sidorov, P.I.; Bazhukova, T.A.; Soloviev, A.G.; Barve, S.S.; McClain, C.J. Probiotics restore bowel flora and improve liver enzymes in human alcohol-induced liver injury: A pilot study. Alcohol 2008, 42, 675–682. [Google Scholar] [CrossRef]
- Lu, J.; Zhu, X.; Zhang, C.; Lu, F.; Lu, Z.; Lu, Y. Co-expression of alcohol dehydrogenase and aldehyde dehydrogenase in Bacillus subtilis for alcohol detoxification. Food Chem. Toxicol. 2020, 135, 110890. [Google Scholar] [CrossRef]
- Lim, T.-J.; Lim, S.; Yoon, J.H.; Chung, M.J. Effects of multi-species probiotic supplementation on alcohol metabolism in rats. J. Microbiol. 2021, 59, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersen, L.; Stormyhr, L.-E.; Smith-Kielland, A. Headspace gas chromatographic determination of ethanol: The use of factorial design to study effects of blood storage and headspace conditions on ethanol stability and acetaldehyde formation in whole blood and plasma. Forensic Sci. Int. 2006, 161, 151–157. [Google Scholar] [CrossRef]
- Ochs, S.d.M.; Fasciotti, M.; Netto, A.D.P. Analysis of 31 hydrazones of carbonyl compounds by RRLC-UV and RRLC-MS (/MS): A comparison of methods. J. Spectrosc. 2015, 2015, 890836. [Google Scholar] [CrossRef]
- Wolever, T.M.; Jenkins, D.J.; Jenkins, A.L.; Josse, R.G. The glycemic index: Methodology and clinical implications. Am. J. Clin. Nutr. 1991, 54, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Hong, S. Establishment of Functionality Evaluation System for Hangover Settlement of Health Functional Food; Ministry of Food and Drug Safety: Seoul, Korea, 2004; Volume 14, pp. 300–343. [Google Scholar]
- Armstrong, T.; Bull, F. Development of the world health organization global physical activity questionnaire (GPAQ). J. Public Health 2006, 14, 66–70. [Google Scholar] [CrossRef]
- Yoon, Y.; Lee, K. The effects of extract powder of fruits and vegetables on hangover. Korea J. Waters 2011, 2, 36–42. [Google Scholar]
- Nosova, T.; Jousimies-Somer, H.; Jokelainen, K.; Heine, R.; Salaspuro, M. Acetaldehyde production and metabolism by human indigenous and probiotic Lactobacillus and Bifidobacterium strains. Alcohol Alcohol. 2000, 35, 561–568. [Google Scholar] [CrossRef]
- Nosova, T.; Jokelainen, K.; Kaihovaara, P.; Jousimies-Somer, H.; Siitonen, A.; Heine, R.; Salaspuro, M. Aldehyde dehydrogenase activity and acetate production by aerobic bacteria representing the normal flora of human large intestine. Alcohol Alcohol. 1996, 31, 555–564. [Google Scholar] [CrossRef]
- Konkit, M.; Kim, K.; Kim, J.-H.; Kim, W. Protective effects of Lactococcus chungangensis CAU 28 on alcohol-metabolizing enzyme activity in rats. J. Dairy Sci. 2018, 101, 5713–5723. [Google Scholar] [CrossRef]
- Qing, L.; Wang, T. Lactic acid bacteria prevent alcohol-induced steatohepatitis in rats by acting on the pathways of alcohol metabolism. Clin. Exp. Med. 2008, 8, 187–191. [Google Scholar] [CrossRef]
- Yan, A.W.; Fouts, D.E.; Brandl, J.; Stärkel, P.; Torralba, M.; Schott, E.; Tsukamoto, H.; Nelson, K.E.; Brenner, D.A.; Schnabl, B. Enteric dysbiosis associated with a mouse model of alcoholic liver disease. Hepatology 2011, 53, 96–105. [Google Scholar] [CrossRef]
- Meroni, M.; Longo, M.; Dongiovanni, P. Alcohol or gut microbiota: Who is the guilty? Int. J. Mol. Sci. 2019, 20, 4568. [Google Scholar] [CrossRef] [PubMed]
- Peana, A.T.; Sánchez-Catalán, M.J.; Hipólito, L.; Rosas, M.; Porru, S.; Bennardini, F.; Romualdi, P.; Caputi, F.F.; Candeletti, S.; Polache, A. Mystic acetaldehyde: The never-ending story on alcoholism. Front. Behav. Neurosci. 2017, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- Mackus, M.; van de Loo, A.J.; Garssen, J.; Kraneveld, A.D.; Scholey, A.; Verster, J.C. The role of alcohol metabolism in the pathology of alcohol hangover. J. Clin. Med. 2020, 9, 3421. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Wild Type (ALDH2*1/*1, n = 27) | Heterozygote (ALDH2*2/*1, n = 27) | Total Group (n = 54) | ||
|---|---|---|---|---|---|
| Age (years) | 25.26 ± 2.61 | 24.89 ± 2.97 | 25.07 ± 2.77 | ||
| Height (cm) | 176.15 ± 4.82 | 175.07 ± 5.27 | 175.61 ± 5.03 | ||
| Weight (kg) | 70.61 ± 8.06 | 70.37 ± 8.03 | 70.49 ± 7.97 | ||
| Body mass index (kg/m2) | 22.77 ± 2.14 | 22.93 ± 1.84 | 22.85 ± 1.98 | ||
| Drinking (yes/no) | non-drinker (n, %) | 0, 0 | 0, 0 | 0, 0 | |
| past drinker (n, %) | 0, 0 | 0, 0 | 0, 0 | ||
| drinker (n, %) | 27, 100 | 27, 100 | 54, 100 | ||
| Alcohol period (years) | 6.00 ± 1.96 | 5.81 ± 2.32 | 5.91 ± 2.13 | ||
| Alcohol consumption (units/week) | 7.38 ± 2.41 | 4.13 ± 2.22 | 5.75 ± 2.82 | ||
| Drinking within a week | yes (n, %) | 23, 85 | 25, 93 | 48, 89 | |
| no (n, %) | 4, 15 | 2, 7 | 6, 11 | ||
| Smoking | non-smoker (n, %) | 17, 63 | 18, 67 | 35, 65 | |
| past smoker (n, %) | 0, 0 | 0, 0 | 0, 0 | ||
| Smoker (n, %) | 10, 37 | 9, 33 | 19, 35 | ||
| Smoking period (years) | 6.30 ± 2.71 | 3.67 ± 2.40 | 5.05 ± 2.84 | ||
| Smoking consumption (units/week) | 10.10 ± 5.34 | 7.44 ± 4.69 | 8.84 ± 5.09 | ||
| Smoking within a week | yes (n, %) | 10, 100 | 8, 89 | 18, 95 | |
| no (n, %) | 0, 0 | 1, 11 | 1, 5 | ||
| Systolic blood pressure (mmHg) | 119.81 ± 8.26 | 119.04 ± 10.36 | 119.43 ± 9.29 | ||
| Diastolic blood pressure (mmHg) | 71.70 ± 8.88 | 70.48 ± 8.17 | 71.09 ± 8.47 | ||
| Pulse (BPM) | 80.48 ± 9.93 | 72.56 ± 7.71 | 76.52 ± 9.67 | ||
| Temperature | 36.2 ± 0.21 | 36.24 ± 0.24 | 36.22 ± 0.23 | ||
| Thyroid stimulating hormone | 1.84 ± 1.32 | 1.73 ± 0.65 | 1.79 ± 1.03 | ||
| Wild Type (ALDH2*1/*1) | Heterozygote (ALDH2*2/*1) | Total Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Duolac ProAP4 Group (n = 19) | Placebo Group (n = 19) | p-Value (1) | Duolac ProAP4 Group (n = 21) | Placebo Group (n = 21) | p-Value (1) | Duolac ProAP4 Group (n = 40) | Placebo Group (n = 40) | p-Value (1) | ||
| Blood acetaldehyde level (mg/dL) | 0 h | 0.000 ± 0.000 | 0.001 ± 0.002 | 0.117 | 0.000 ± 0.000 | 0.000 ± 0.001 | 0.553 | 0.000 ± 0.0002 | 0.001 ± 0.000 | 0.094 |
| 0.5 h | 0.007 ± 0.000 | 0.005 ± 0.006 | 0.660 | 0.113 ± 0.059 | 0.150 ± 0.085 | 0.018 | 0.063 ± 0.070 | 0.081 ± 0.096 | 0.040 | |
| 1 h | 0.004 ± 0.010 | 0.005 ± 0.010 | 0.773 | 0.108 ± 0.063 | 0.147 ± 0.092 | 0.005 | 0.059 ± 0.070 | 0.080 ± 0.097 | 0.006 | |
| 2 h | 0.002 ± 0.004 | 0.002 ± 0.004 | 0.941 | 0.050 ± 0.042 | 0.065 ± 0.052 | 0.130 | 0.027 ± 0.039 | 0.035 ± 0.049 | 0.129 | |
| 4 h | 0.000 ± 0.000 | 0.000 ± 0.001 | 0.181 | 0.019 ± 0.026 | 0.028 ± 0.037 | 0.197 | 0.010 ± 0.021 | 0.015 ± 0.030 | 0.184 | |
| 6 h | 0.000 ± 0.000 | 0.000 ± 0.001 | 0.331 | 0.005 ± 0.006 | 0.010 ± 0.010 | 0.020 | 0.003 ± 0.005 | 0.005 ± 0.009 | 0.019 | |
| Cmax (mg/dL) | 0.008 ± 0.025 | 0.007 ± 0.010 | 0.829 | 0.121 ± 0.065 | 0.170 ± 0.096 | 0.002 | 0.068 ± 0.076 | 0.092 ± 0.108 | 0.007 | |
| Tmax Median (min-max) | 0.68 ± 0.38 0.50 (0.50–2.00) | 0.63 ± 0.23 0.50 (0.50–1.00) | 0.542 | 0.76 ± 0.26 1.00 (0.50–1.00) | 0.71 ± 0.25 0.50 (0.50–1.00) | 0.329 | 0.73 ± 0.32 0.50 (0.50–2.00) | 0.68 ± 0.24 0.50 (0.50–1.00) | 0.291 | |
| iAUC (mg·hr/dL) | 0.010 ± 0.024 | 0.008 ± 0.014 | 0.774 | 0.254 ± 0.173 | 0.347 ± 0.236 | 0.022 | 0.138 ± 0.176 | 0.186 ± 0.241 | 0.029 | |
| Wild Type (ALDH2*1/*1) | Heterozygote (ALDH2*2/*1) | Total Group | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Duolac ProAP4 Group (n = 19) | Placebo Group (n = 19) | p-Value (1) | Duolac ProAP4 Group (n = 21) | Placebo Group (n = 21) | p-Value (1) | Duolac ProAP4 Group (n = 40) | Placebo Group (n = 40) | p-Value (1) | ||
|
Blood alcohol level (mg/dL) | 0 h | 0.00 ± 0.00 | 0.00 ± 0.00 | - | 0.00 ± 0.00 | 0.00 ±0.00 | - | 0.00 ± 0.00 | 0.00 ± 0.00 | - |
| 0.5 h | 62.71 ± 29.85 | 66.27 ± 27.54 | 0.558 | 81.34 ± 31.55 | 77.28 ± 29.39 | 0.425 | 72.49 ± 31.79 | 72.05 ± 28.70 | 0.909 | |
| 1 h | 85.54 ± 24.08 | 90.35 ± 23.44 | 0.348 | 90.80 ± 24.72 | 92.38 ± 15.98 | 0.750 | 88.30 ± 24.25 | 91.42 ± 19.64 | 0.374 | |
| 2 h | 82.37 ± 10.05 | 81.51 ± 16.79 | 0.769 | 74.57 ± 24.19 | 79.40 ± 20.01 | 0.123 | 78.27 ± 19.03 | 80.40 ± 18.34 | 0.320 | |
| 4 h | 49.53 ± 9.60 | 51.05 ± 14.72 | 0.511 | 57.16 ± 22.64 | 62.46 ± 20.23 | 0.159 | 53.54 ± 17.90 | 57.04 ± 18.52 | 0.116 | |
| 6 h | 11.98 ± 7.79 | 16.69 ± 9.0 | 0.009 | 25.03 ± 13.44 | 31.99 ± 14.94 | 0.039 | 18.83 ± 12.81 | 24.73 ± 14.56 | 0.002 | |
| Cmax (mg/dL) | 92.39 ± 18.0 | 91.98 ± 21.16 | 0.909 | 94.35 ± 28.50 | 96.48 ± 17.89 | 0.673 | 93.42 ± 23.82 | 94.34 ± 19.39 | 0.763 | |
| Tmax Median (min-max) | 1.37 ± 0.57 1.00 (0.50–2.00) | 1.18 ± 0.45 1.00 (0.50–2.00) | 0.185 | 0.95 ± 0.31 1.00 (0.50–2.00) | 1.19 ± 0.83 1.00 (0.50–4.00) | 0.180 |
1.15 ± 0.50 1.00 (0.50–2.00) | 1.19 ± 0.67 1.00 (0.50–2.00) | 0.744 | |
| iAUC (mg·hr/dL) | 330.11 ± 56.49 | 341.95 ± 81.03 | 0.361 | 359.97 ± 118.97 | 383.95 ± 93.41 | 0.127 | 345.79 ± 94.65 | 363.40 ± 89.20 | 0.072 | |
| Wild Type (ALDH2*1/*1) | Heterozygote (ALDH2*2/*1) | Total Group | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Liver Enzymes (Standard Range) | Time | Duolac ProAP4 Group (n = 19) | Diff | Placebo Group (n = 19) | Diff | p-Value (1) | Duolac ProAP4 Group (n = 21) | Diff | Placebo Group (n = 21) | Diff | p-Value (1) | Duolac ProAP4 Group (n = 40) | Diff | Placebo Group (n = 40) | Diff | p-Value (1) |
| AST (12~33 IU/L) | 0 h | 22.79 ± 4.43 | - | 23.47 ± 8.64 | - | 0.752 | 21.14 ± 4.52 | - | 20.57 ± 4.93 | - | 0.574 | 21.93 ± 4.50 | - | 21.95 ± 7.01 | - | 0.983 |
| 1 h | 22.16 ± 5.00 | −0.63 ± 2.09 | 22.53 ± 8.12 | −0.95 ± 1.99 | 0.672 (2) | 21.00 ± 3.97 | −0.14 ± 2.22 | 21.90 ± 5.46 | 1.33 ± 2.03 | 0.032 (2) | 21.55 ± 4.47 | −0.38 ± 2.14 | 22.20 ± 6.77 | 0.25 ± 2.30 | 0.217 (2) | |
| 6 h | 23.53 ± 5.73 | 0.74 ± 2.62 | 23.11 ± 7.52 | −0.37 ± 2.79 | 0.241 (2) | 21.48 ± 4.11 | 0.33 ± 1.91 | 21.52 ± 4.73 | 0.95 ± 1.99 | 0.374 (2) | 22.45 ± 4.99 | 0.53 ± 2.25 | 22.28 ± 6.18 | 0.33 ± 2.46 | 0.728 (2) | |
| ALT (5~35 IU/L) | 0 h | 25.42 ± 10.17 | - | 25.84 ± 14.66 | - | 0.903 | 24.00 ± 9.59 | - | 23.05 ± 10.13 | - | 0.598 | 24.68 ± 9.77 | - | 24.38 ± 12.4 | - | 0.871 |
| 1 h | 24.47 ± 10.40 | −0.95 ± 2.76 | 25.16 ± 14.65 | −0.68 ± 3.00 | 0.810 (2) | 22.00 ± 9.64 | −2.00 ± 3.00 | 23.24 ± 9.32 | 0.19 ± 3.40 | 0.029 (2) | 23.18 ± 9.96 | −1.50 ± 2.90 | 24.15 ± 12.02 | −0.23 ± 3.21 | 0.082 (2) | |
| 6 h | 24.74 ± 10.44 | −0.68 ± 3.54 | 24.95 ± 14.19 | −0.89 ± 2.81 | 0.864 (2) | 22.24 ± 9.97 | −1.76 ± 2.96 | 22.10 ± 9.90 | −0.95 ± 2.89 | 0.402 (2) | 23.43 ± 10.14 | −1.25 ± 3.26 | 23.45 ± 12.06 | −0.93 ± 2.81 | 0.669 (2) | |
| ALP (45~129 IU/L) | 0 h | 62.26 ± 11.58 | - | 59.53 ± 11.30 | - | 0.069 | 64.57 ± 12.27 | - | 59.62 ± 12.74 | - | 0.010 | 63.48 ± 14.70 | - | 59.58 ± 11.92 | - | 0.001 |
| 1 h | 62.74 ± 11.11 | 0.47 ± 3.13 | 60.89 ± 11.44 | 1.37 ± 2.61 | 0.371 (2) | 66.86 ± 17.24 | 2.29 ± 3.65 | 62.48 ± 13.28 | 2.86 ± 2.71 | 0.505 (2) | 64.90 ± 14.62 | 1.43 ± 3.49 | 61.73 ± 12.31 | 2.15 ± 2.73 | 0.259 (2) | |
| 6 h | 61.84 ± 11.56 | −0.42 ± 3.19 | 60.58 ± 11.21 | 1.05 ± 2.46 | 0.106 (2) | 64.05 ± 16.84 | −0.52 ± 2.79 | 61.86 ± 13.76 | 2.24 ± 2.55 | 0.003 (2) | 63.00 ± 14.44 | −0.48 ± 2.94 | 61.25 ± 12.47 | 1.68 ± 2.65 | 0.001 (2) | |
| γ-GT (12~73 IU/L) | 0 h | 25.05 ± 13.36 | - | 24.63 ± 14.01 | - | 0.814 | 17.48 ± 6.31 | - | 18.05 ± 5.55 | - | 0.616 | 21.08 ± 10.84 | - | 21.18 ± 10.84 | - | 0.922 |
| 1 h | 23.16 ± 12.46 | −1.89 ± 2.51 | 23.37 ± 13.44 | −1.26 ± 2.83 | 0.448 (2) | 15.33 ± 6.19 | −2.14 ± 1.98 | 15.86 ± 4.98 | −2.19 ± 3.37 | 0.957 (2) | 19.05 ± 10.35 | −2.03 ± 2.22 | 19.43 ± 10.51 | −1.75 ± 3.12 | 0.645 (2) | |
| 6 h | 23.26 ± 11.74 | −1.79 ± 3.34 | 23.58 ± 13.64 | −1.05 ± 2.30 | 0.419 (2) | 16.67 ± 5.13 | −0.81 ± 2.34 | 16.62 ± 5.40 | −1.43 ± 3.30 | 0.508 (2) | 19.80 ± 9.39 | −1.28 ± 2.86 | 19.93 ± 10.64 | −1.25 ± 2.84 | 0.969 (2) | |
| Blood glucose (mg/dL) | 0 h | 86.00 ± 4.58 | - | 88.30 ± 7.41 | - | 0.434 | 83.20 ± 3.52 | - | 90.09 ± 7.45 | - | 0.015 | 84.53 ± 4.19 | - | 89.24 ± 7.30 | - | 0.016 |
| 6 h | 85.89 ± 4.20 | −0.11 ± 5.93 | 84.80 ± 3.71 | −3.50 ± 9.22 | 0.556 0.360 (2) | 81.0 ± 5.89 | −2.20 ± 5.98 | 82.27 ± 4.52 | −7.82 ± 9.81 | 0.583 0.134 (2) | 83.32 ± 5.61 | −1.21 ± 5.88 | 83.48 ± 4.25 | −5.76 ± 9.55 | 0.919 0.076 (2) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, S.-J.; Hwang, J.-H.; Park, E.-O.; Lee, S.-O.; Chung, Y.-J.; Chung, M.-J.; Lim, S.; Lim, T.-J.; Ha, Y.; Park, B.-H.; et al. Regulation of Alcohol and Acetaldehyde Metabolism by a Mixture of Lactobacillus and Bifidobacterium Species in Human. Nutrients 2021, 13, 1875. https://doi.org/10.3390/nu13061875
Jung S-J, Hwang J-H, Park E-O, Lee S-O, Chung Y-J, Chung M-J, Lim S, Lim T-J, Ha Y, Park B-H, et al. Regulation of Alcohol and Acetaldehyde Metabolism by a Mixture of Lactobacillus and Bifidobacterium Species in Human. Nutrients. 2021; 13(6):1875. https://doi.org/10.3390/nu13061875
Chicago/Turabian StyleJung, Su-Jin, Ji-Hyun Hwang, Eun-Ock Park, Seung-Ok Lee, Yun-Jo Chung, Myung-Jun Chung, Sanghyun Lim, Tae-Joong Lim, Yunhi Ha, Byung-Hyun Park, and et al. 2021. "Regulation of Alcohol and Acetaldehyde Metabolism by a Mixture of Lactobacillus and Bifidobacterium Species in Human" Nutrients 13, no. 6: 1875. https://doi.org/10.3390/nu13061875
APA StyleJung, S.-J., Hwang, J.-H., Park, E.-O., Lee, S.-O., Chung, Y.-J., Chung, M.-J., Lim, S., Lim, T.-J., Ha, Y., Park, B.-H., & Chae, S.-W. (2021). Regulation of Alcohol and Acetaldehyde Metabolism by a Mixture of Lactobacillus and Bifidobacterium Species in Human. Nutrients, 13(6), 1875. https://doi.org/10.3390/nu13061875