
Proprioceptive and Dual-Task Training: The Key of Stroke Rehabilitation, A Systematic Review

 ,
, 

Abstract
1. Introduction
2. Methods
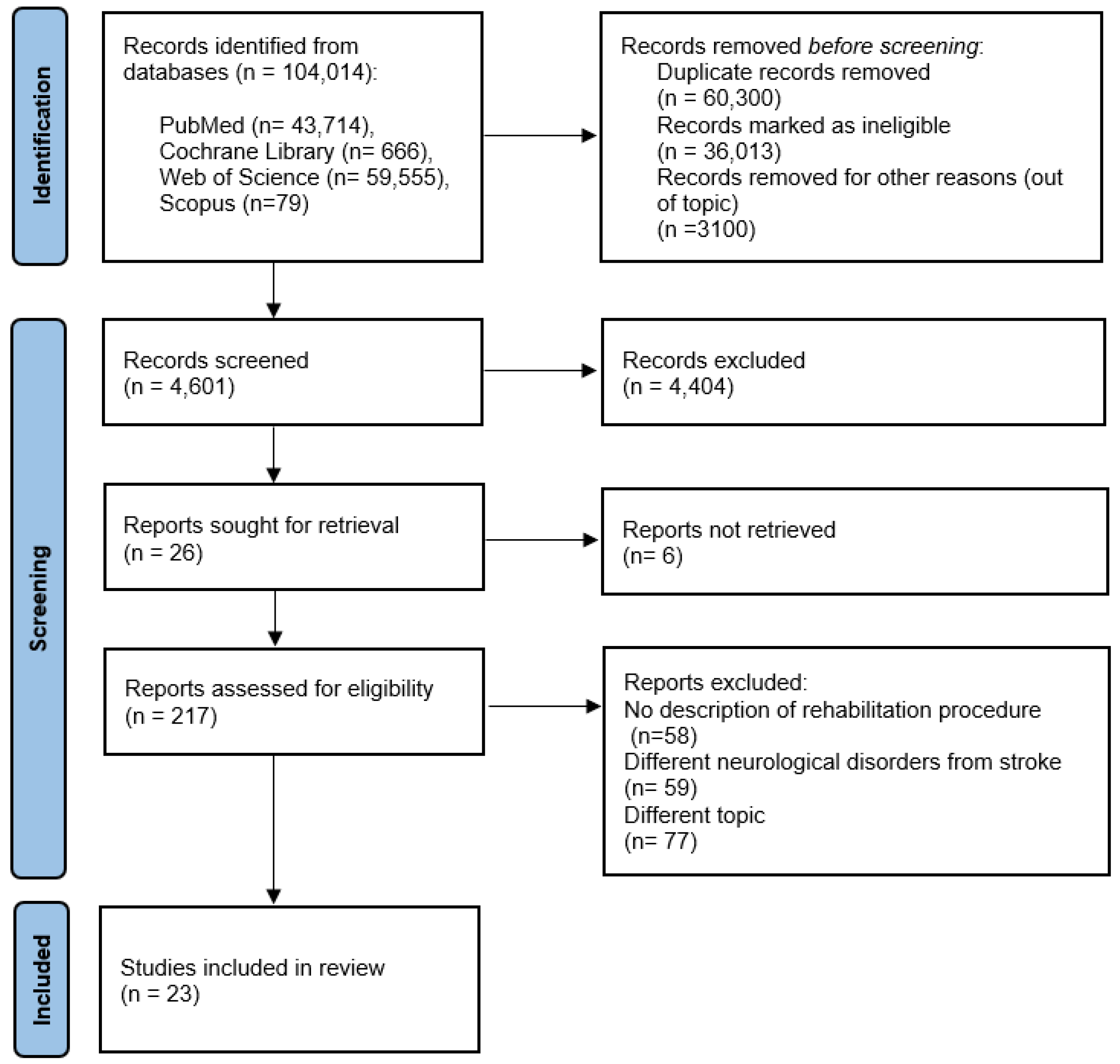
2.1. Search Strategy
2.2. Selection Criteria and Data Extraction
2.3. Description of the Studies
2.4. Comparators
2.5. Quality of Selected Articles and Outcomes
2.6. Risk of Bias
2.7. Statistical Analysis
3. Results
3.1. Variations in Experimental Conditions across the Studies
3.2. Study Characteristics
3.3. Summary of Findings
3.4. Proprioceptive Rehabilitation Program and Dual-Task Exercises
4. Discussion
4.1. Summary of Collected Data
4.2. Task-Oriented Rehabilitation Therapy in the Context of Proprioceptive Rehabilitation
4.3. Be on Guard
4.4. Enjoy Dual-Task and Proprioceptive Training
5. Limits
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Proske, U.; Gandevia, S.C. The proprioceptive senses: Their roles in signaling body shape, body position and movement, and muscle force. Physiol. Rev. 2012, 92, 1651–1697. [Google Scholar] [CrossRef] [PubMed]
- Mirdamadi, J.L.; Block, H.J. Somatosensory versus cerebellar contributions to proprioceptive changes associated with motor skill learning: A theta burst stimulation study. Cortex 2021, 140, 98–109. [Google Scholar] [CrossRef] [PubMed]
- Maurer, C.; Mergner, T.; Peterka, R.J. Multisensory control of human upright stance. Exp. Brain Res. 2006, 171, 231–250. [Google Scholar] [CrossRef]
- Shumsway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice, 3rd ed.; Lippincot Williams & Wilkins: Philadelphia, PA, USA, 2007; pp. 3–83. [Google Scholar]
- Pelicioni, P.H.S.; Tijsma, M.; Lord, S.R.; Menant, J. Prefrontal cortical activation measured by fNIRS during walking: Effects of age, disease and secondary task. PeerJ 2019, 7, e6833. [Google Scholar] [CrossRef]
- Al-Yahya, E.; Johansen-Berg, H.; Kischka, U.; Zarei, M.; Cockburn, J.; Dawes, H. Prefrontal Cortex Activation While Walking Under Dual-Task Conditions in Stroke: A Multimodal Imaging Study. Neurorehabilit. Neural Repair 2016, 30, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Collett, J.; Fleming, M.K.; Meester, D.; Al-Yahya, E.; Wade, D.T.; Dennis, A.; Salvan, P.; Meaney, A.; Cockburn, J.; Dawes, J.; et al. Dual-task walking and automaticity after Stroke: Insights from a secondary analysis and imaging sub-study of a randomised controlled trial. Clin. Rehabil. 2021, 35, 1599–1610. [Google Scholar] [CrossRef] [PubMed]
- Feld, J.A.; Plummer, P. Patterns of cognitive-motor dual-task interference post stroke: An observational inpatient study at hospital discharge. Eur. J. Phys. Rehabil. Med. 2021, 57, 327–336. [Google Scholar] [CrossRef]
- Yang, L.; Lam, F.M.; Huang, M.; He, C.; Pang, M.Y. Dual-task mobility among individuals with chronic stroke: Changes in cognitive-motor interference patterns and relationship to difficulty level of mobility and cognitive tasks. Eur. J. Phys. Rehabil. Med. 2018, 54, 526–535. [Google Scholar] [CrossRef]
- Kelly, C.; Meyer, J.; Hanks, V.; Barefield, C. Neurorehabilitation for an individual with bilateral thalamic stroke and preexisting visual impairment presenting with impaired use of sensory cues: A case report. Physiother. Theory Pract. 2019, 37, 1139–1145. [Google Scholar] [CrossRef]
- Carey, L.M.; Matyas, T.A.; Baum, C. Effects of Somatosensory Impairment on Participation After Stroke. Am. J. Occup. Ther. 2018, 72, 7203205100p1–7203205100p10. [Google Scholar] [CrossRef]
- Plummer, P.; Villalobos, R.M.; Vayda, M.S.; Moser, M.; Johnson, E. Feasibility of Dual-Task Gait Training for Community-Dwelling Adults after Stroke: A Case Series. Stroke Res. Treat. 2014, 2014, 538602. [Google Scholar] [CrossRef]
- An, H.J.; Kim, J.I.; Kim, Y.R.; Lee, K.B.; Kim, D.J.; Yoo, K.T.; Choi, J.H. The Effect of Various Dual Task Training Methods with Gait on the Balance and Gait of Patients with Chronic Stroke. J. Phys. Ther. Sci. 2014, 26, 1287–1291. [Google Scholar] [CrossRef]
- Her, J.G.; Park, K.D.; Yang, Y.; Ko, T. Effects of balance training with various dual-task conditions on stroke patients. J. Phys. Ther. Sci. 2011, 23, 713–717. [Google Scholar] [CrossRef][Green Version]
- Aman, J.E.; Elangovan, N.; Yeh, I.L.; Konczak, J. The effectiveness of proprioceptive training for improving motor function: A systematic review. Front. Hum. Neurosci. 2015, 8, 1075. [Google Scholar] [CrossRef]
- Lewek, M.D.; Feasel, J.; Wentz, E.; Brooks, F.P., Jr.; Whitton, M.C. Use of visual and proprioceptive feedback to improve gait speed and spatiotemporal symmetry following chronic stroke: A case series. Phys. Ther. 2012, 92, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Q.; Pi, Y.L.; Chen, B.L.; Chen, P.J.; Liu, Y.; Wang, R.; Li, X.; Waddington, G. Cognitive motor interference for gait and balance in stroke: A systematic review and meta-analysis. Eur. J. Neurol. 2015, 22, 555-e37. [Google Scholar] [CrossRef] [PubMed]
- Baek, C.Y.; Chang, W.N.; Park, B.Y.; Lee, K.B.; Kang, K.Y.; Choi, M.R. Effects of Dual-Task Gait Treadmill Training on Gait Ability, Dual-Task Interference, and Fall Efficacy in People with Stroke: A Randomized Controlled Trial. Phys. Ther. 2021, 101, pzab067. [Google Scholar] [CrossRef]
- Fishbein, P.; Hutzler, Y.; Ratmansky, M.; Treger, I.; Dunsky, A. A Preliminary Study of Dual-Task Training Using Virtual Reality: Influence on Walking and Balance in Chronic Poststroke Survivors. J. Stroke Cereb. Dis. 2019, 28, 104343. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, C.; Roerdink, M.; Van Ooijen, M.W.; Meskers, C.G.; Janssen, T.W.; Beek, P.J. Walking adaptability therapy after stroke: Study protocol for a randomized controlled trial. Trials 2016, 17, 425. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Kim, M.K.; Lee, H.J.; Lee, W.H. Virtual Reality Training with Cognitive Load Improves Walking Function in Chronic Stroke Patients. Tohoku J. Exp. Med. 2015, 236, 273–280. [Google Scholar] [CrossRef]
- Kim, K.J.; Kim, K.H. Progressive treadmill cognitive dual-task gait training on the gait ability in patients with chronic stroke. J. Exerc. Rehabil. 2018, 14, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Meester, D.; Al-Yahya, E.; Dennis, A.; Collett, J.; Wade, D.T.; Ovington, M.; Liu, F.; Meaney, A.; Cockburn, J.; Johansen-Berg, H.; et al. A randomized controlled trial of a walking training with simultaneous cognitive demand (dual-task) in chronic stroke. Eur. J. Neurol. 2019, 26, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, C.; Roerdink, M.; Meskers, C.G.M.; Beek, P.J.; Janssen, T.W.J. Walking-adaptability therapy after stroke: Results of a randomized controlled trial. Trials 2021, 22, 923. [Google Scholar] [CrossRef]
- Ada, L.; Dean, C.M.; Hall, J.M.; Bampton, J.; Crompton, S. A Treadmill and Overground Walking Program Improves Walking in Persons Residing in the Community after Stroke: A Placebo-Controlled, Randomized Trial. Arch. Phys. Med. Rehabil. 2003, 84, 1486–1491. [Google Scholar] [CrossRef]
- Kim, H.K.; Lee, H.; Seo, K. The Effects of Dual-Motor Task Training on the Gait Ability of Chronic Stroke Patients. J. Phys. Ther. Sci. 2013, 25, 317–320. [Google Scholar] [CrossRef]
- Lee, H.; Kim, H.; Ahn, M.; You, Y. Effects of proprioception training with exercise imagery on balance ability of stroke patients. J. Phys. Ther. Sci. 2015, 27, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Pang, M.Y.C.; Yang, L.; Ouyang, H.; Lam, F.M.H.; Huang, M.; Jehu, D.A. Dual-Task Exercise Reduces Cognitive-Motor Interference in Walking and Falls After Stroke. Stroke 2018, 49, 2990–2998. [Google Scholar] [CrossRef]
- Plummer, P.; Zukowski, L.A.; Feld, J.A.; Najafi, B. Cognitive-motor dual-task gait training within 3 years after stroke: A randomized controlled trial. Physiother. Theory Pract. 2021, 18, 1–16. [Google Scholar] [CrossRef]
- Subramaniam, S.; Hui-Chan, C.W.; Bhatt, T. A Cognitive-Balance Control Training Paradigm Using Wii Fit to Reduce Fall Risk in Chronic Stroke Survivors. J. Neurol. Phys. Ther. 2014, 38, 216–225. [Google Scholar] [CrossRef]
- Yang, Y.R.; Wang, R.Y.; Chen, Y.C.; Kao, M.J. Dual-task exercise improves walking ability in subjects with chronic stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2007, 88, 1236–1240. [Google Scholar] [CrossRef]
- Kim, G.Y.; Han, M.R.; Lee, H.G. Effect of Dual-task Rehabilitative Training on Cognitive and Motor Function of Stroke Patients. J. Phys. Ther. Sci. 2014, 26, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, M.; Arsh, A.; Hammad, S.M.; Haq, I.U.; Darain, H. Comparison of dual task specific training and conventional physical therapy in ambulation of hemiplegic stroke patients: A randomized controlled trial. J. Pak. Med. Assoc. 2020, 70, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.Y.; Moon, Y.; Choi, J.D. Effects of Cognitive Task Training on Dynamic Balance and Gait of Patients with Stroke: A Preliminary Randomized Controlled Study. Med. Sci. Monit. Basic Res. 2020, 26, e925264. [Google Scholar] [CrossRef]
- Kannan, L.; Vora, J.; Bhatt, T.; Hughes, S.L. Cognitive-motor exergaming for reducing fall risk in people with chronic stroke: A randomized controlled trial. NeuroRehabilitation 2019, 44, 493–510. [Google Scholar] [CrossRef]
- Saleh, M.S.M.; Rehab, N.I.; Aly, S.M.A. Effect of aquatic versus land motor dual task training on balance and gait of patients with chronic stroke: A randomized controlled trial. NeuroRehabilitation 2019, 44, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.; Lee, G.; Lee, S. Effect of the cognitive-motor dual-task using auditory cue on balance of surviviors with chronic stroke: A pilot study. Clin. Rehabil. 2015, 29, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015, Elaboration and explanation. BMJ 2015, 350, 7647. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Br. Med. J. 2011, 343, 889–893. [Google Scholar] [CrossRef]
- Kim, K.K.; Lee, D.K.; Kim, E.K. Effect of aquatic dual-task training on balance and gait in stroke patients. J. Phys. Ther. Sci. 2016, 28, 2044–2047. [Google Scholar] [CrossRef][Green Version]
- Powell, L.E.; Myers, A.M. The Activities-specific Balance Confidence (ABC) Scale. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1995, 50, M28–M34. [Google Scholar] [CrossRef]
- Ottonello, M.; Ferriero, G.; Benevolo, E.; Sessarego, P.; Dughi, D. Psychometric evaluation of the Italian version of the Berg Balance Scale in rehabilitation inpatients. Eur. Med. 2003, 39, 181–189. [Google Scholar]
- Ferraresi, G.; Buganè, F.; Cosma, M.; Agarici, M.; Vio, A.; Manca, M.; Casadio, G.; Benedetti, M.G. Timed up and go test (tug) temporal phases assessment using a wireless device (free4act®): Method validation in healthy subjects. Gait Posture 2013, 37, 30–31. [Google Scholar] [CrossRef]
- Cheng, D.K.; Nelson, M.; Brooks, D.; Salbach, N.M. Validation of stroke-specific protocols for the 10-meter walk test and 6-minute walk test conducted using 15-meter and 30-meter walkways. Top Stroke Rehabil. 2020, 27, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Wagner, K.; Rutte, K.; Meissner, D.; Pohl, M. Predictive validity and responsiveness of the functional ambulation category in hemiparetic patients after stroke. Arch. Phys. Med. Rehabil. 2007, 88, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Sackett, D.L. Rules of evidence and clinical recommendations on the use of antithrombotic agents. Chest 1989, 95, 2S–4S. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Montori, V.; Akl, E.A.; Djulbegovic, B.; Falck-Ytter, Y.; et al. GRADE guidelines: 4. Rating the quality of evidence--study limitations (risk of bias). J. Clin. Epidemiol. 2011, 64, 407–415. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; et al. GRADE guidelines: 5. Rating the quality of evidence--publication bias. J. Clin. Epidemiol. 2011, 64, 1277–1282. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Falck-Ytter, Y.; Jaeschke, R.; Vist, G.; et al. GRADE Working Group. GRADE guidelines: 8. Rating the quality of evidence--indirectness. J. Clin. Epidemiol. 2011, 64, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Cochrane Collaboration: Oxford, UK, 2008. [Google Scholar]
- Shekelle, P.G.; Greeley, A.M.; Tanner, E.P.; Mak, S.S.; Begashaw, M.M.; Miake-Lye, I.M.; Beroes-Severin, J.M. APPENDIX B, Risk of Bias in Non-Randomised Studies—Of interventions (ROBINS-I) Tool. In One-to-One Observation: A Systematic Review; Department of Veterans Affairs (US): Washington, DC, USA, 2019. [Google Scholar]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2, A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Hyndman, D.; Yardley, L.; Ashburn, A.; Stack, E. Interference between balance, gait and cognitive task performance among people with stroke living in the community. Disabil. Rehabil. 2006, 28, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Varela-Vásquez, L.A.; Minobes-Molina, E.; Jerez-Roig, J. Dual-task exercises in older adults: A structured review of current literature. J. Frailty Sarcopenia Falls 2020, 5, 31–37. [Google Scholar] [CrossRef]
- Chiaramonte, R.; Cioni, M. Critical spatiotemporal gait parameters for individuals with dementia: A systematic review and meta-analysis. Hong Kong Physiother. J. 2021, 41, 1–14. [Google Scholar] [CrossRef] [PubMed]
- De Freitas, T.B.; Leite, P.H.W.; Doná, F.; Pompeu, J.E.; Swarowsky, A.; Torriani-Pasin, C. The effects of dual task gait and balance training in Parkinson’s disease: A systematic review. Physiother. Theory Pract. 2020, 36, 1088–1096. [Google Scholar] [CrossRef]
- Morelli, N.; Morelli, H. Dual task training effects on gait and balance outcomes in multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2021, 49, 102794. [Google Scholar] [CrossRef]
- Kayabinar, B.; Alemdaroğlu-Gürbüz, İ.; Yilmaz, Ö. The effects of virtual reality augmented robot-assisted gait training on dual-task performance and functional measures in chronic stroke: A randomized controlled single-blind trial. Eur. J. Phys. Rehabil. Med. 2021, 57, 227–237. [Google Scholar] [CrossRef]
- Chen, L.; Lo, W.L.; Mao, Y.R.; Ding, M.H.; Lin, Q.; Li, H.; Zhao, J.L.; Xu, Z.Q.; Bian, R.H.; Huang, D.F. Effect of Virtual Reality on Postural and Balance Control in Patients with Stroke: A Systematic Literature Review. Biomed. Res. Int. 2016, 2016, 7309272. [Google Scholar] [CrossRef]
- Bruni, M.F.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. What does best evidence tell us about robotic gait rehabilitation in stroke patients: A systematic review and meta-analysis. J. Clin. Neurosci. 2018, 48, 11–17. [Google Scholar] [CrossRef]
- Bergmann, J.; Krewer, C.; Bauer, P.; Koenig, A.; Riener, R.; Müller, F. Virtual reality to augment robot-assisted gait training in non-ambulatory patients with a subacute stroke: A pilot randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Hackney, M.E.; Hall, C.D.; Echt, K.V.; Wolf, S.L. Application of adapted tango as therapeutic intervention for patients with chronic stroke. J. Geriatr. Phys. Ther. 2012, 35, 206–217. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors, yr | Study Design | Sample Size, y | Months after Stroke | Outcomes Measure | Rehabilitative Therapy | Duration Therapy | Exercise Description | Results after Therapy |
|---|---|---|---|---|---|---|---|---|
| Ada 2003 [25] | CLT | A: 13 p B: 14 p 66 ± 11 y | >6 | Walking speed, distance, step length, step width, cadence, SA-SIP30 | A: Cognitive task and walking program B: Home exercises | 3 d/w, for 4 w | Cognitive task on treadmill and overground walking program for 30 min. Proprioceptive group walked around an outdoor circuit, such as curbs, slopes, stairs, and rough terrain, while performing a cognitive dual-task. The cognitive task consisted of matching the word “red” with the response “yes” or the word “blue” with the response “no”. For the control group: home exercise program, such as stretching and strengthening exercises of lower limbs and training for balance and coordination. | Effectiveness of treadmill and overground walking training. Gain of 18 cm/s in stroke patients |
| An 2014 [13] | CLT | A: 12 p B: 12 p C: 12 p | Chronic stroke | STI, WDI with open and closed eyes, TUG, FSST, 10 MWT | A: Motor DT gait training B: Cognitive DT gait training C: Motor and cognition DT gait training | 3 d/w, for 8 w | Fifteen minutes of walking on the treadmill, with motor or cognitive tasks or both types of tasks (30′). The motor tasks included: “tossing up and catching a ball”, “rehanging loops on different hooks”, “doing up buttons after unbuttoning”, “holding a cup of water without spilling it”, and “receiving and returning a cup of water”. Dual cognitive tasks included: “discerning colours”, “mathematical subtraction”, “verbal analogical reasoning”, “spelling words backward” and “counting backward”. | Motor and cognitive DT training improved motor performance and balance and gait abilities |
| Baek 2021 [18] | CLT | A:17 p B: 17 p | Chronic stroke | Gait parameters (speed, stride, variability, and cadence), CRR, DTC, FES | A: Gait training on a treadmill and cognitive task exercises at the same time B: Separately, first gait training on a treadmill, then cognitive task exercises | 2 d/w, For 6 w | Sixty minutes of treadmill training with a cognitive task: serial subtraction by three from two-digit numbers randomly selected | Dual-task gait treadmill training was more effective in improving gait ability in dual-task training and dual-task interference than single-task training involving gait and cognitive tasks separately in subjects with chronic stroke |
| Cho 2015 [21] | CLT | A: 11 p 60.0 y B: 11 p 58.6 y | Chronic stroke patients A: 273.9 d B: 263.9 d | Spatio-temporal gait parameters: speed, cadence, step and stride length | A: Virtual reality training with cognitive task B: Virtual reality treadmill training | 5 d/w, for 4 w | The standard rehabilitation program consisted of physical and occupational therapies. Thirty minutes/session of treadmill and cognitive tasks (memory, arithmetic, and verbal tasks) | Effectiveness of virtual reality training with cognitive load L on walking function under the dual-task condition |
| Choi 2014 [37] | CLT | A: 19 p 49.1 11.9 B: 18 p 49.2 ± 7.05 y | 18.2 ± 5.7 | TUG, sway velocity | A: Cognitive–motor dual-task B: Single-task training | 3 d/w, for 4 w | The dual cognitive–motor task group performed rehabilitation for 15 min with a random auditory cue while walking on a treadmill. The sound of a bell was the auditory cue indicating that the participants should move the circle ring from side to side. The single-task group walked on the treadmill. Conventional physical therapy included progressive resistance exercise and postural control, neurodevelopment and occupational training, Brunnstrom movements, and proprioceptive neuromuscular facilitation techniques. | Cognitive and motor dual-task training and auditory cues improved balance |
| Fishbein 2019 [19] | CLT | A: 11 p B: 11 p 65.2 ± 9 y | >12 | 10 MWT, TUG, FRT LRT-L/R, ABC, BBS | A: DT training B: Single-task treadmill walking | 2 d/w, for 4 w | Mobilisation and flexibility exercises for 8 min and walking around for 3 min, treadmill for 3 min. Subsequently, the single-task group walked for 20 min, and the dual-task training group, while walking for 20 min, trained with 3 virtual games: hit the virtual ball, touch the virtual boxes, clean the virtual windows | Improvements in BBS, FRT, LRT-L/R, 10 MWT, ABC in A group; in gait variables. No changes in TUG. |
| Her 2011 [14] | RS | A: 12 p B: 13 p C: 13 p 64.8 ± 5.2 y | >12 | BBS, FIM, centre of pressure | A: MDT B: CDT C: MCDT | 3 d/w, for 6 w | Group A: Exercises comprising motor tasks for 30 min, such as exchanging a ball, receiving a ball with a basket, bouncing a ball on the floor, and holding a glass with water and exchanging a water glass while maintaining balance on an unstable balance pad. Group B: Exercises of cognitive tasks such as counting backwards, calculating two subtractions, calling the correct names of objects, and reciting words in reverse order while maintaining balance. Group C: Motor and cognitive exercises with postural control task. | To obtain improvement in balance and gait, both motor and cognitive DT were needed, not only motor or cognitive DT alone. |
| Hong 2020 [34] | CLT | A: 8 p 56.6 ± 8.7 y B: 9 p 66.2 ± 11.5 y | >6 | TUG, BBS | A: CDT B: General task group | 3 d/w for 4 w | Exercises with a cognitive task for 30 min. The program consisted of maintaining a standing posture while moving the lower extremity of the less-affected side toward the 3 flexion directions of the hip joint and then moving it back in place. | Cognitive task training is a more effective intervention method to improve balance and gait ability after stroke. |
| Iqbal 2020 [33] | CLT | A: 32 p 58.2 ± 7.13 y B: 32 p 58.8 ± 6.13 y | Chronic stroke | Step length, stride length, 10 MWT, TUG, cycle time, cadence | A: Motor dual-task training B: Conventional training | 4 d/w for 4 w | Motor dual-task with exercises were conducted for 40 min. Slowly walking backward, sideways, and forward on a smooth surface while holding a 100 gm sandbag. | Conventional physical therapy and dual-task training effectively improved the gait ability of chronic stroke patients, who showed a significant improvement in all spatial and temporal gait variables. |
| Kannan 2019 [35] | CLT | A: 13 p B: 12 p 59.2 ± 6.3 y | >3 | TUG, 6 MWT, ABC, BBS | A: High-intensity, tapered motor and cognitive rehabilitation B: Conventional balance rehabilitation | 10 sessions, for 6 w | The cognitive tasks and proprioceptive exercises included four Wii Fit games played for 5 min. The control group performed balance training exercises for 90 min: 10 min of stretching, 15 min of functional stretching, 35 min of balance training, and 10–15 min of treadmill walking. The cognitive tasks included: training for semantic memory (i.e., recite as many types of animals as they could within the time limit provided), verbal fluency (i.e., participants recited words that began with the letter provided, such as “A”, while avoiding saying proper nouns), abstract memory (i.e., participants completed phrases according to the relationship of the cue in the sentence), and repetition of letters. | Effectiveness of cognitive and motor rehabilitation in improving balance control and cognition |
| Kim 2013 [26] | RS | A:14 p B: 15 p 56.4 ± 12.3 y | 7 ± 2.4 m | Cadence, speed, step time, cycle time, step length, stride length | A: Conservative physical therapy B: Dual-motor task training | 5 d/w, for 4 w | Neurological developmental treatment for 30 min. The motor dual-task training included passive and active resistance exercises and exercises for coordination, motor sensation, and balance. The proprioceptive neuromuscular facilitation lower limb patterns consisted of: flexion–adduction–external rotation knee flexion or extension–adduction–external rotation knee extension. Dual-task: rising from a chair from the sitting position while picking up plastic cups that lay in front of the feet, then slowly walking forward, sideways, and backward on a flat surface while holding a 100 g sandbag against the affected wrist and going up and down a ramp or stairs while transferring cups from tables of different heights located beside the ramp or stairs in consecutive order. | Improvement in temporal (cadence, speed, step time, and cycle time) and spatial parameters (step length and stride length) in a DT group |
| Kim 2014 [32] | RS | A: 10 p B: 10 p 68.5 ± 7.8 y | 17.9 ± 13 | Stroop test, TUG, 10 MWT, F8WT | A: Traditional rehabilitation program B: Traditional rehabilitation program + DT training | A: 5 d/w 1 w B: 3 d/w, 4 w | Motor dual-task training was conducted for 30 min and consisted of words written using inks of various colours, with the subjects having to state the colour of the ink and gait tasks, which included walking on a level surface, walking while changing gait speeds, walking with vertical or horizontal head turns, walking with pivot turns, stepping over or around obstacles, and walking up and downstairs. | Improvement in cognitive skills and gait after DT training |
| Kim 2016 [40] | RS | A: 10 p B: 10 p 68.5 ± 3.1 y | 10.9 ± 1.1 | BBS, 5-Times Sit-to-Stand Test, Functional Reach Test, TUG, 10 MWT, FGA | A: Neurodevelopmental treatment + aquatic dual-task training B: Neurodevelopmental treatment | 5 d/w, for 6 w | Aquatic motor dual-task training for 30 min a day, including stability exercises, such as standing with eyes closed, stability exercise while playing catch with the therapist, walking 10 m at a comfortable speed, and walking 10 m at a comfortable speed while holding a 200 mL cup of water | Improvement in balance and gait after aquatic DT training |
| Kim 2018 [22] | CLT | A: 13 p 52.62 ± 9.84 y B: 13 p 56.15 ± 10.82 y | Chronic stroke | Speed, cadence, single support time, stride length, 10-MWT | A: Progressive treadmill cognitive dual-task gait training B: Conventional treadmill gait training | 5 d/w, for 4 w | Thirty minutes of treadmill exercises with cognitive dual-task: speaking numbers task, arithmetic subtraction, memory task, and verbal fluency | Progressive treadmill cognitive dual-task gait training had a positive influence on the gait and clinical gait. |
| Lee 2015 [27] | RS | A: 18 p B: 18 p 28 p < 65 y 8 p > 65 y | 11.5 ± 1.9 | BBS, TUG, joint position sense | A: Motor imagery exercises for 5′ and proprioceptive rehabilitation for 25′ B: Proprioceptive rehabilitation for 30′ | 5 d/w, for 8 w | Motor image training and proprioceptive training for 30 min included exercises on a balance pad with 5 different tasks. The program included: standing with the support position of two feet and standing upright by moving both heels up and down. Stretching and eyes-closed exercises, balance board exercises shifting weight left and right and forward and backward to the maximum, and sitting and standing on a balance board | Improvements in K-BBS, TUG, weight-bearing ratio, and joint position sense error in group A > B |
| Meester 2019 [23] | CLT | A: 26 p 60.85 ± 14.86 y B: 24 p 62.25 ± 15.53 y | >6 months | SF-36, EuroQol-5D-5L, PASE, step activity. | A: Traditional treadmill B: Treadmill with dual-task | 2 d/w, for 10 w | Thirty-minute treadmill program at an aerobic training intensity with dual-task: listening task or talking about planning daily activities | Walking with specific additional cognitive distraction (dual-task training) might increase activity more over 12 weeks. |
| Pang 2018 [28] | CLT | A: 25 p B: 28 p 61.2 ± 6.4 y | 75.3 ± 64.9 | ABC, Frenchay Activities Index, Stroke-specific Quality of Life Scale | A: DT balance/mobility training B: Single-task balance/mobility training | 1 d/w, for 8 w | For 60 min a week, the motor dual-task program included walking combined with verbal fluency and with serial-3-subtractions and the timed up and go test combined with verbal fluency. | After DT rehabilitation, improvement in speed, reduction in falls, and no improvement in social participation and quality of life |
| Plummer 2021 [29] | CLT | A: 18 p B: 18 p | <3 years | Gait speed, cognitive task performance | A: Dual-task gait training B: Single-task gait training on cognitive–motor dual-task | 3 d/w for 4 w | Cognitive task performance during walking included spontaneous speech, arithmetic word, backward spelling, working memory, random number, calculating time, backward numbers, and naming opposites. The exercises lasted 60 min. | Both single- and dual-task gait training improved single- and dual-task gait speed but did not change the amount of relative interference. |
| Saleh 2019 [36] | CLT | A: 25 p B: 25 p 49.7 ± 1.8 y | 9.02 ± 1.8 | Stability index, speed, step length, time of support on limb | A: Motor DT in water B: Motor DT on land | 3 d/w, for 6 w | The dual-motor task training included exercises performed during walking: holding a ball, holding a 200 mL cup of water and standing on a balance board, walking forward, walking sideways and walking backward in each condition, and transferring coins from one pocket to another. The exercises lasted 45 min. | Improvement in anteroposterior and mediolateral stability index, speed, step length, and time of support on the affected limb after water exercises |
| Subramaniam 2014 [30] | RS | 8 p 51.75 y | 6.1 ± 4 | BBS, TUG, IMI Reaction time, speed, maximum excursion, directional control | Virtual reality balance training in DT | 110′/d, for 5 d consecutive | Cognitive motor dual-task training for balance in virtual reality consisted of 110 min of balance board games: table tilt, tightrope, soccer, and balance bubble, played while performing cognitive tasks, such as memory tasks, word list generation, letter–number sequencing, and question–answer and memory recall games. | Improvement in balance after DT rehabilitation |
| Timmermans 2016 [20] | CLT | A: 20 p B: 20 p | >3 m | 10 MWT, TUG, FAC, BBS, ABC | A: Treadmill-based C-Mill therapy B: Overground Falls program | 2 d/w, for 5 w | A group performed cognitive–motor dual-task training: the C-Mill treadmill training program, which consisted of 1.5 h each session, twice a w for 5 w. It included practising avoidance of visual obstacles, practising accurate positioning of the foot on a step-to-step basis, walking forwards in a regular or irregular sequence of visual stepping objectives, exercises to practise acceleration and deceleration while maintaining position, and playing a functional and interactive adaptability walking game. The FALLS program consisted of an overground therapy program to reduce the number of falls by practising walking adaptability. It included exercises to practise obstacle avoidance, exercises to practise foot placement while walking over uneven terrain, and tandem walking and slalom. These exercises were also performed under visual constraints. | Improvement after C-Mill therapy with respect to FALLS program |
| Timmermans 2021 [24] | CLT | A: 16 p 52 ± 13 y B: 17 p 59 ± 10 y | >3 months | Speed, 10 MWT | A: Treadmill-based C-Mill therapy B: Overground Falls program | 2 d/w, for 5 w | Ninety minutes/session. A group performed cognitive–motor dual-task training: the C-Mill treadmill training program. The FALLS program for the other group consisted of exercises for walking adaptability. | Greater improvement in context-specific walking speed in C-Mill group |
| Yang 2007 [31] | CLT | A: 12 p B: 13 p 59.3 ± 11.8 y | 64.5 ± 63.1 | Speed, cadence, stride time, stride length, temporal symmetry index | A: Ball exercise program B: No rehabilitation training | 3 d/w for 4 w | Motor dual-task program: 30 min of gait training while manipulating 1 or 2 balls with diameters of 45, 55, 85, and 95 cm and a basketball. The training program included walking while holding 1 or 2 balls in both hands, walking to adapt to the rhythm of bouncing 1 ball with 1 hand or both hands, walking while holding 1 ball in 1 hand and simultaneously kicking another ball from basketball into a net, and walking while bouncing a ball with both hands. Three motor tasks of simple walking included walking with buttoning task and walking with the task of carrying a cup on a tray. | Walking ability was significantly improved after training. Gain of ba29.74 cm/s. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiaramonte, R.; Bonfiglio, M.; Leonforte, P.; Coltraro, G.L.; Guerrera, C.S.; Vecchio, M. Proprioceptive and Dual-Task Training: The Key of Stroke Rehabilitation, A Systematic Review. J. Funct. Morphol. Kinesiol. 2022, 7, 53. https://doi.org/10.3390/jfmk7030053
Chiaramonte R, Bonfiglio M, Leonforte P, Coltraro GL, Guerrera CS, Vecchio M. Proprioceptive and Dual-Task Training: The Key of Stroke Rehabilitation, A Systematic Review. Journal of Functional Morphology and Kinesiology. 2022; 7(3):53. https://doi.org/10.3390/jfmk7030053
Chicago/Turabian StyleChiaramonte, Rita, Marco Bonfiglio, Pierfrancesco Leonforte, Giovanna Loriana Coltraro, Claudia Savia Guerrera, and Michele Vecchio. 2022. "Proprioceptive and Dual-Task Training: The Key of Stroke Rehabilitation, A Systematic Review" Journal of Functional Morphology and Kinesiology 7, no. 3: 53. https://doi.org/10.3390/jfmk7030053
APA StyleChiaramonte, R., Bonfiglio, M., Leonforte, P., Coltraro, G. L., Guerrera, C. S., & Vecchio, M. (2022). Proprioceptive and Dual-Task Training: The Key of Stroke Rehabilitation, A Systematic Review. Journal of Functional Morphology and Kinesiology, 7(3), 53. https://doi.org/10.3390/jfmk7030053