A Systematic Review on the Cognitive Benefits and Neurophysiological Correlates of Exergaming in Healthy Older Adults


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Selection Process and Data Extraction
2.4. Categorization of Cognitive Outcome Parameters
2.5. Assessment of Methodological Quality
3. Results
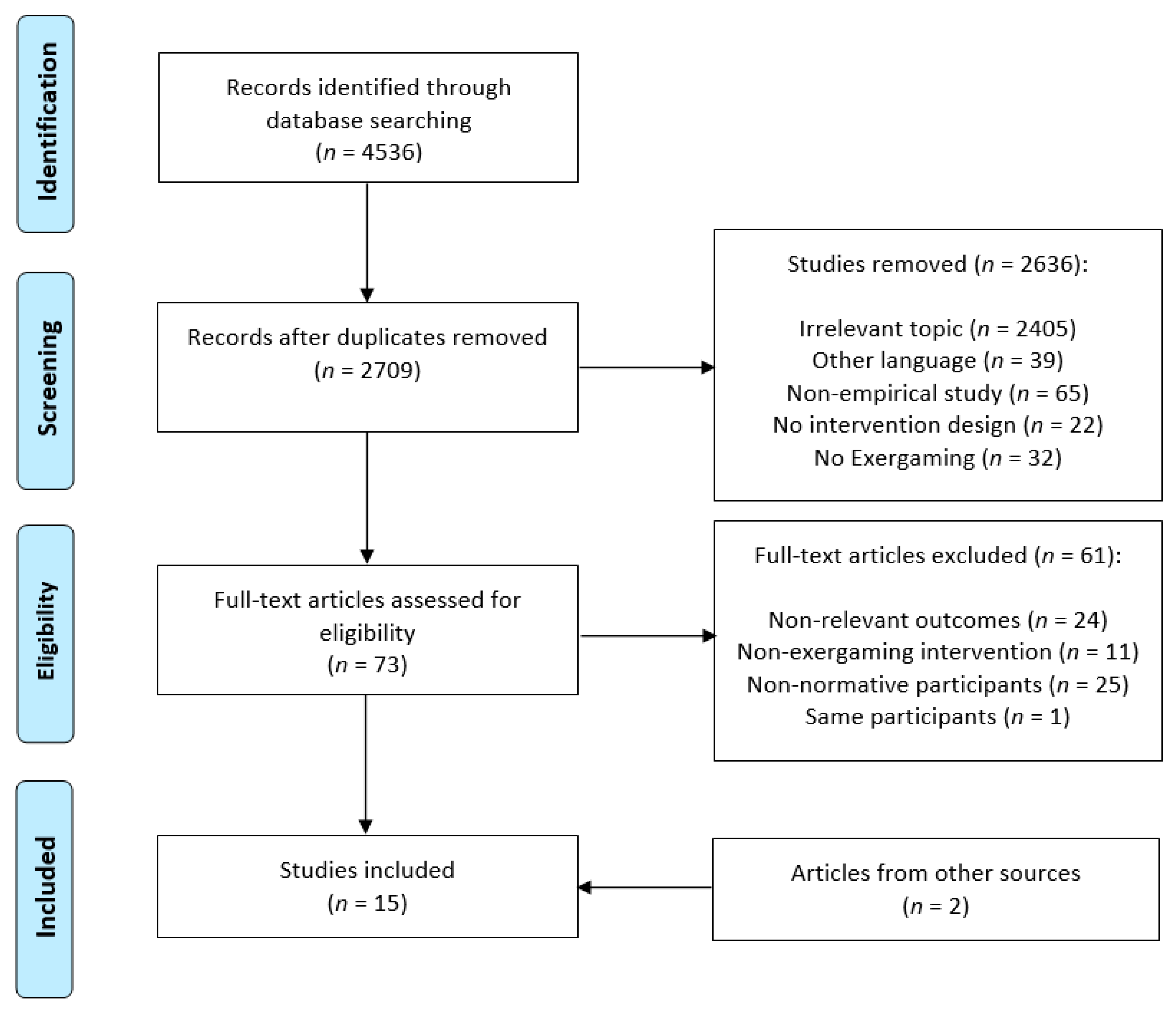
3.1. Search Results
3.2. Study Design and Participant Characteristics
3.3. Intervention Characteristics and Types of Exergames
3.4. Cognitive Outcome Measures
3.5. Intervention Effects on Cognitive Outcomes
3.6. Potential Moderators of Intervention Effects
3.7. Neurophysiological Correlates of Exergame Training
3.8. Methodological Quality
4. Discussion
4.1. Types of Exergames
4.2. Intervention Effects on Cognitive Outcomes
4.3. Potential Moderators of Exergame Intervention Efficacy
4.4. Neurophysiological Correlates of Exergaming
4.5. Potential Microbiological Mechanisms Underlying Exergaming
4.6. Methodological Considerations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kontis, V.; Bennett, J.E.; Mathers, C.D.; Li, G.; Foreman, K.; Ezzati, M. Future life expectancy in 35 industrialised countries: Projections with a bayesian model ensemble. Lancet 2017, 389, 1323–1335. [Google Scholar] [CrossRef]
- Rossi, A.; Berger, K.; Chen, H.; Leslie, D.; Mailman, R.B.; Huang, X. Projection of the prevalence of parkinson’s disease in the coming decades: Revisited. Mov. Disord. 2018, 33, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Rocca, W.A.; Petersen, R.C.; Knopman, D.S.; Hebert, L.E.; Evans, D.A.; Hall, K.S.; Gao, S.; Unverzagt, F.W.; Langa, K.M.; Larson, E.B.; et al. Trends in the incidence and prevalence of alzheimer’s disease, dementia, and cognitive impairment in the united states. Alzheimer’s Dement. 2011, 7, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Guerchet, M.; Ali, G.C.; Wu, Y.T.; Prina, A.M.; Winblad, B.; Jonsson, L.; Liu, Z.; Prince, M. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimer’s Dement. 2017, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kowal, S.L.; Dall, T.M.; Chakrabarti, R.; Storm, M.V.; Jain, A. The current and projected economic burden of parkinson’s disease in the united states. Mov. Disord. 2013, 28, 311–318. [Google Scholar] [CrossRef] [PubMed]
- United Nations, Department of Economic and Social Affairs. Population Division. World Population Ageing 2015; ST/ESA/SER.A/390; Department of Economic and Social Affairs: New York, NY, USA, 2015. [Google Scholar]
- Park, D.C.; Reuter-Lorenz, P.A. The adaptive brain: Aging and neurocognitive scaffolding. Annu. Rev. Psychol. 2009, 60, 173–196. [Google Scholar] [CrossRef] [PubMed]
- Murman, D.L. The impact of age on cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef]
- Harada, C.N.; Natelson Love, M.C.; Triebel, K. Normal cognitive aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef]
- Salthouse, T.A. When does age-related cognitive decline begin? Neurobiol. Aging 2009, 30, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Raz, N.; Lindenberger, U.; Rodrigue, K.M.; Kennedy, K.M.; Head, D.; Williamson, A.; Dahle, C.; Gerstorf, D.; Acker, J.D. Regional brain changes in aging healthy adults: General trends, individual differences and modifiers. Cereb. Cortex 2005, 15, 1676–1689. [Google Scholar] [CrossRef]
- Hafkemeijer, A.; Altmann-Schneider, I.; de Craen, A.J.M.; Slagboom, P.E.; van der Grond, J.; Rombouts, S. Associations between age and gray matter volume in anatomical brain networks in middle-aged to older adults. Aging Cell 2014, 13, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Peters, R. Ageing and the brain. Postgrad. Med. J. 2006, 82, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Liu, K. Structural brain network changes across the adult lifespan. Front. Aging Neurosci. 2017, 9, 275. [Google Scholar] [CrossRef] [PubMed]
- Kerchner, G.A.; Racine, C.A.; Hale, S.; Wilheim, R.; Laluz, V.; Miller, B.L.; Kramer, J.H. Cognitive processing speed in older adults: Relationship with white matter integrity. PLoS ONE 2012, 7, e50425. [Google Scholar] [CrossRef]
- Sonntag, W.E.; Eckman, D.M.; Ingraham, J.; Riddle, D.R. Regulation of cerebrovascular aging. In Brain Aging: Models, Methods, and Mechanisms; Riddle, D.R., Ed.; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Tarumi, T.; Zhang, R. Cerebral blood flow in normal aging adults: Cardiovascular determinants, clinical implications, and aerobic fitness. J. Neurochem. 2018, 144, 595–608. [Google Scholar] [CrossRef]
- Raj, D.; Yin, Z.; Breur, M.; Doorduin, J.; Holtman, I.R.; Olah, M.; Mantingh-Otter, I.J.; Van Dam, D.; De Deyn, P.P.; den Dunnen, W.; et al. Increased white matter inflammation in aging- and alzheimer’s disease brain. Front. Mol. Neurosci. 2017, 10, 206. [Google Scholar] [CrossRef] [PubMed]
- Sparkman, N.L.; Johnson, R.W. Neuroinflammation associated with aging sensitizes the brain to the effects of infection or stress. Neuroimmunomodulation 2008, 15, 323–330. [Google Scholar] [CrossRef]
- Budni, J.; Bellettini-Santos, T.; Mina, F.; Garcez, M.L.; Zugno, A.I. The involvement of bdnf, ngf and gdnf in aging and alzheimer’s disease. Aging Dis. 2015, 6, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Lommatzsch, M.; Zingler, D.; Schuhbaeck, K.; Schloetcke, K.; Zingler, C.; Schuff-Werner, P.; Virchow, J.C. The impact of age, weight and gender on bdnf levels in human platelets and plasma. Neurobiol. Aging 2005, 26, 115–123. [Google Scholar] [CrossRef]
- Kaasinen, V.; Vilkman, H.; Hietala, J.; Nagren, K.; Helenius, H.; Olsson, H.; Farde, L.; Rinne, J. Age-related dopamine d2/d3 receptor loss in extrastriatal regions of the human brain. Neurobiol. Aging 2000, 21, 683–688. [Google Scholar] [CrossRef]
- Wahlstrom, D.; Collins, P.; White, T.; Luciana, M. Developmental changes in dopamine neurotransmission in adolescence: Behavioral implications and issues in assessment. Brain Cogn. 2010, 72, 146–159. [Google Scholar] [CrossRef] [PubMed]
- Frith, C.; Dolan, R. The role of the prefrontal cortex in higher cognitive functions. Brain Res. Cogn. Brain Res. 1996, 5, 175–181. [Google Scholar] [CrossRef]
- Yuan, P.; Raz, N. Prefrontal cortex and executive functions in healthy adults: A meta-analysis of structural neuroimaging studies. Neurosci. Biobehav. Rev. 2014, 42, 180–192. [Google Scholar] [CrossRef]
- Siddiqui, S.V.; Chatterjee, U.; Kumar, D.; Siddiqui, A.; Goyal, N. Neuropsychology of prefrontal cortex. Indian J. Psychiatry 2008, 50, 202–208. [Google Scholar]
- Driscoll, I.; Davatzikos, C.; An, Y.; Wu, X.; Shen, D.; Kraut, M.; Resnick, S.M. Longitudinal pattern of regional brain volume change differentiates normal aging from mci. Neurology 2009, 72, 1906–1913. [Google Scholar] [CrossRef]
- Scahill, R.I.; Frost, C.; Jenkins, R.; Whitwell, J.L.; Rossor, M.N.; Fox, N.C. A longitudinal study of brain volume changes in normal aging using serial registered magnetic resonance imaging. Arch. Neurol. 2003, 60, 989–994. [Google Scholar] [CrossRef]
- Davis, S.W. Qué pasa? The posterior-anterior shift in aging. Cereb. Cortex 2008, 18, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, P.; Benuskova, L.; Franz, E.A. The age-related posterior-anterior shift as revealed by voxelwise analysis of functional brain networks. Front. Aging. Neurosci. 2014, 6, 301. [Google Scholar] [CrossRef] [PubMed]
- Glisky, E.L. Changes in cognitive function in human aging. In Brain Aging: Models, Methods, and Mechanisms; Riddle, D.R., Ed.; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Berlingeri, M.; Danelli, L.; Bottini, G.; Sberna, M.; Paulesu, E. Reassessing the harold model: Is the hemispheric asymmetry reduction in older adults a special case of compensatory-related utilisation of neural circuits? Exp. Brain Res. 2013, 224, 393–410. [Google Scholar] [CrossRef]
- Ballesteros, S.; Prieto, A.; Mayas, J.; Toril, P.; Pita, C.; Ponce de Leon, L.; Reales, J.M.; Waterworth, J. Corrigendum: Brain training with non-action video games enhances aspects of cognition in older adults: A randomized controlled trial. Front. Aging Neurosci. 2015, 7, 82. [Google Scholar] [CrossRef]
- Cabeza, R. Hemispheric asymmetry reduction in older adults: The harold model. Psychol. Aging 2002, 17, 85–100. [Google Scholar] [CrossRef] [PubMed]
- Martins, R.; Joanette, Y.; Monchi, O. The implications of age-related neurofunctional compensatory mechanisms in executive function and language processing including the new temporal hypothesis for compensation. Front. Hum. Neurosci. 2015, 9, 221. [Google Scholar] [CrossRef]
- Reuter-lorenz, P.A.; Mikels, J.A. The aging mind and brain: Implications of enduring plasticity for behavioral and cultural change. In Lifespan Development and the Brain: The Perspective of Biocultural Co-Constructivism; Rösler, F., Reuter-Lorenz, P.A., Baltes, P.B., Eds.; Cambridge University Press: Cambridge, UK, 2006; pp. 255–276. [Google Scholar]
- Reuter-Lorenz, P.A.; Lustig, C. Brain aging: Reorganizing discoveries about the aging mind. Curr. Opin. Neurobiol. 2005, 15, 245–251. [Google Scholar] [CrossRef]
- Reuter-Lorenz, P.A.; Park, D.C. How does it stac up? Revisiting the scaffolding theory of aging and cognition. Neuropsychol. Rev. 2014, 24, 355–370. [Google Scholar] [CrossRef] [PubMed]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. Physical exercise and brain functions in older adults. J. Aging Res. 2013, 2013, 197326. [Google Scholar] [CrossRef]
- Voelcker-Rehage, C.; Niemann, C. Structural and functional brain changes related to different types of physical activity across the life span. Neurosci. Biobehav. Rev. 2013, 37, 2268–2295. [Google Scholar] [CrossRef]
- Chang, Y.K.; Pan, C.Y.; Chen, F.T.; Tsai, C.L.; Huang, C.C. Effect of resistance-exercise training on cognitive function in healthy older adults: A review. J. Aging. Phys. Act. 2012, 20, 497–517. [Google Scholar] [CrossRef] [PubMed]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Ballesteros, S.; Kraft, E.; Santana, S.; Tziraki, C. Maintaining older brain functionality: A targeted review. Neurosci. Biobehav. Rev. 2015, 55, 453–477. [Google Scholar] [CrossRef]
- Kueider, A.M.; Parisi, J.M.; Gross, A.L.; Rebok, G.W. Computerized cognitive training with older adults: A systematic review. PLoS ONE 2012, 7, e40588. [Google Scholar] [CrossRef]
- Lampit, A.; Hallock, H.; Valenzuela, M. Computerized cognitive training in cognitively healthy older adults: A systematic review and meta-analysis of effect modifiers. PLoS Med. 2014, 11, e1001756. [Google Scholar] [CrossRef] [PubMed]
- Lustig, C.; Shah, P.; Seidler, R.; Reuter-Lorenz, P.A. Aging, training, and the brain: A review and future directions. Neuropsychol. Rev. 2009, 19, 504–522. [Google Scholar] [CrossRef] [PubMed]
- Bherer, L. Cognitive plasticity in older adults: Effects of cognitive training and physical exercise. Ann. N. Y. Acad. Sci. 2015, 1337, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Clare, L.; Wu, Y.T.; Teale, J.C.; MacLeod, C.; Matthews, F.; Brayne, C.; Woods, B. Potentially modifiable lifestyle factors, cognitive reserve, and cognitive function in later life: A cross-sectional study. PLoS Med. 2017, 14, e1002259. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Pinilla, F.; Hillman, C. The influence of exercise on cognitive abilities. Compr. Physiol. 2013, 3, 403–428. [Google Scholar]
- Diamond, A. Executive functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Papp, K.V.; Walsh, S.J.; Snyder, P.J. Immediate and delayed effects of cognitive interventions in healthy elderly: A review of current literature and future directions. Alzheimer’s Dement. 2009, 5, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Martin, M.; Clare, L.; Altgassen, A.M.; Cameron, M.H.; Zehnder, F. Cognition-based interventions for healthy older people and people with mild cognitive impairment. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.E.; Loughrey, D.; Lawlor, B.A.; Robertson, I.H.; Walsh, C.; Brennan, S. The impact of exercise on the cognitive functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 16, 12–31. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.E.; Loughrey, D.; Lawlor, B.A.; Robertson, I.H.; Walsh, C.; Brennan, S. The impact of cognitive training and mental stimulation on cognitive and everyday functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 15, 28–43. [Google Scholar] [CrossRef]
- Young, J.; Angevaren, M.; Rusted, J.; Tabet, N. Aerobic exercise to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Angevaren, M.; Vanhees, L.; Wendel-Vos, W.; Verhaar, H.J.; Aufdemkampe, G.; Aleman, A.; Verschuren, W.M. Intensity, but not duration, of physical activities is related to cognitive function. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Bamidis, P.D.; Fissler, P.; Papageorgiou, S.G.; Zilidou, V.; Konstantinidis, E.I.; Billis, A.S.; Romanopoulou, E.; Karagianni, M.; Beratis, I.; Tsapanou, A.; et al. Gains in cognition through combined cognitive and physical training: The role of training dosage and severity of neurocognitive disorder. Front. Aging Neurosci. 2015, 7, 152. [Google Scholar] [CrossRef]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef]
- Zhu, X.; Yin, S.; Lang, M.; He, R.; Li, J. The more the better? A meta-analysis on effects of combined cognitive and physical intervention on cognition in healthy older adults. Ageing Res. Rev. 2016, 31, 67–79. [Google Scholar] [CrossRef]
- Tait, J.L.; Duckham, R.L.; Milte, C.M.; Main, L.C.; Daly, R.M. Influence of sequential vs. Simultaneous dual-task exercise training on cognitive function in older adults. Front. Aging Neurosci. 2017, 9, 368. [Google Scholar] [CrossRef] [PubMed]
- Miyachi, M.; Yamamoto, K.; Ohkawara, K.; Tanaka, S. Mets in adults while playing active video games: A metabolic chamber study. Med. Sci. Sports Exerc. 2010, 42, 1149–1153. [Google Scholar] [CrossRef]
- Lyons, E.J.; Tate, D.F.; Ward, D.S.; Bowling, J.M.; Ribisl, K.M.; Kalyararaman, S. Energy expenditure and enjoyment during video game play: Differences by game type. Med. Sci. Sports Exerc. 2011, 43, 1987–1993. [Google Scholar] [CrossRef] [PubMed]
- O’Donovan, C.; Hirsch, E.; Holohan, E.; McBride, I.; McManus, R.; Hussey, J. Energy expended playing xbox kinect and wii games: A preliminary study comparing single and multiplayer modes. Physiotherapy 2012, 98, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.M.; Maddison, R.; Pfaeffli, L.A.; Rawstorn, J.C.; Gant, N.; Kerse, N.M. Activity and energy expenditure in older people playing active video games. Arch. Phys. Med. Rehabil. 2012, 93, 2281–2286. [Google Scholar] [CrossRef]
- Toril, P.; Reales, J.M.; Ballesteros, S. Video game training enhances cognition of older adults: A meta-analytic study. Psychol. Aging 2014, 29, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Stanmore, E.; Stubbs, B.; Vancampfort, D.; de Bruin, E.D.; Firth, J. The effect of active video games on cognitive functioning in clinical and non-clinical populations: A meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2017, 78, 34–43. [Google Scholar] [CrossRef]
- Howes, S.C.; Charles, D.K.; Marley, J.; Pedlow, K.; McDonough, S.M. Gaming for health: Systematic review and meta-analysis of the physical and cognitive effects of active computer gaming in older adults. Phys. Ther. 2017, 97, 1122–1137. [Google Scholar] [CrossRef] [PubMed]
- Bamidis, P.D.; Vivas, A.B.; Styliadis, C.; Frantzidis, C.; Klados, M.; Schlee, W.; Siountas, A.; Papageorgiou, S.G. A review of physical and cognitive interventions in Aging. Neurosci. Biobehav. Rev. 2014, 44, 206–220. [Google Scholar] [CrossRef] [PubMed]
- Monteiro-Junior, R.S.; Vaghetti, C.A.; Nascimento, O.J.; Laks, J.; Deslandes, A.C. Exergames: Neuroplastic hypothesis about cognitive improvement and biological effects on physical function of institutionalized older persons. Neural Regen Res. 2016, 11, 201–204. [Google Scholar] [CrossRef]
- Fissler, P.; Kuster, O.; Schlee, W.; Kolassa, I.T. Novelty interventions to enhance broad cognitive abilities and prevent dementia: Synergistic approaches for the facilitation of positive plastic change. Prog. Brain Res. 2013, 207, 403–434. [Google Scholar] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The, P.G. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, P.L.; Kanfer, R.; Calderwood, C. Use it or lose it? Wii brain exercise practice and reading for domain knowledge. Psychol. Aging 2010, 25, 753–766. [Google Scholar] [CrossRef] [PubMed]
- Gschwind, Y.J.; Eichberg, S.; Ejupi, A.; de Rosario, H.; Kroll, M.; Marston, H.R.; Drobics, M.; Annegarn, J.; Wieching, R.; Lord, S.R.; et al. Ict-based system to predict and prevent falls (istoppfalls): Results from an international multicenter randomized controlled trial. Eur. Rev. Aging Phys. Act. 2015, 12, 10. [Google Scholar] [CrossRef]
- Gschwind, Y.J.; Schoene, D.; Lord, S.R.; Ejupi, A.; Valenzuela, T.; Aal, K.; Woodbury, A.; Delbaere, K. The effect of sensor-based exercise at home on functional performance associated with fall risk in older people—A comparison of two exergame interventions. Eur. Rev. Aging Phys. Act. 2015, 12, 11. [Google Scholar] [CrossRef]
- Schoene, D.; Valenzuela, T.; Toson, B.; Delbaere, K.; Severino, C.; Garcia, J.; Davies, T.A.; Russell, F.; Smith, S.T.; Lord, S.R. Interactive cognitive-motor step training improves cognitive risk factors of falling in older adults—A randomized controlled trial. PLoS ONE 2015, 10, e0145161. [Google Scholar] [CrossRef] [PubMed]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Cowan, N. What are the differences between long-term, short-term, and working memory? Prog. Brain Res. 2008, 169, 323–338. [Google Scholar] [PubMed]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol. Aging 2012, 27, 589–600. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, 5928. [Google Scholar] [CrossRef]
- Anderson-Hanley, C.; Arciero, P.J.; Brickman, A.M.; Nimon, J.P.; Okuma, N.; Westen, S.C.; Merz, M.E.; Pence, B.D.; Woods, J.A.; Kramer, A.F.; et al. Exergaming and older adult cognition: A cluster randomized clinical trial. Am. J. Prev. Med. 2012, 42, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Bacha, J.M.R.; Gomes, G.C.V.; de Freitas, T.B.; Viveiro, L.A.P.; da Silva, K.G.; Bueno, G.C.; Varise, E.M.; Torriani-Pasin, C.; Alonso, A.C.; Luna, N.M.S.; et al. Effects of kinect adventures games versus conventional physical therapy on postural control in elderly people: A randomized controlled trial. Games Health J. 2018, 7, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Barcelos, N.; Shah, N.; Cohen, K.; Hogan, M.J.; Mulkerrin, E.; Arciero, P.J.; Cohen, B.D.; Kramer, A.F.; Anderson-Hanley, C. Aerobic and cognitive exercise (ace) pilot study for older adults: Executive function improves with cognitive challenge while exergaming. J. Int. Neuropsychol. Soc. 2015, 21, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Eggenberger, P.; Schumacher, V.; Angst, M.; Theill, N.; de Bruin, E.D. Does multicomponent physical exercise with simultaneous cognitive training boost cognitive performance in older adults? A 6-month randomized controlled trial with a 1-year follow-up. Clin. Interv. Aging 2015, 10, 1335–1349. [Google Scholar] [PubMed]
- Eggenberger, P.; Wolf, M.; Schumann, M.; de Bruin, E.D. Exergame and balance training modulate prefrontal brain activity during walking and enhance executive function in older adults. Front. Aging Neurosci. 2016, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, A.V.; Barbosa, A.R.; Meneghini, V. Active videogame-based physical activity vs. Aerobic exercise and cognitive performance in older adults: A randomized controlled trial. J. Phys. Educ. Sport 2018, 18, 203–209. [Google Scholar]
- Ordnung, M.; Hoff, M.; Kaminski, E.; Villringer, A.; Ragert, P. No overt effects of a 6-week exergame training on sensorimotor and cognitive function in older adults. A preliminary investigation. Front. Hum. Neurosci. 2017, 11, 160. [Google Scholar] [CrossRef]
- Park, J.; Yim, J. A new approach to improve cognition, muscle strength, and postural balance in community-dwelling elderly with a 3-d virtual reality kayak program. Tohoku J. Exp. Med. 2016, 238, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Schättin, A.; Arner, R.; Gennaro, F.; de Bruin, E.D. Adaptations of prefrontal brain activity, executive functions, and gait in healthy elderly following exergame and balance training: A randomized-controlled study. Front. Aging Neurosci. 2016, 8, 278. [Google Scholar] [CrossRef]
- Schoene, D.; Lord, S.R.; Delbaere, K.; Severino, C.; Davies, T.A.; Smith, S.T. A randomized controlled pilot study of home-based step training in older people using videogame technology. PLoS ONE 2013, 8, e57734. [Google Scholar] [CrossRef]
- Chuang, L.Y.; Hung, H.Y.; Huang, C.J.; Chang, Y.K.; Hung, T.M. A 3-month intervention of dance dance revolution improves interference control in elderly females: A preliminary investigation. Exp. Brain Res. 2015, 233, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Kayama, H.; Okamoto, K.; Nishiguchi, S.; Yamada, M.; Kuroda, T.; Aoyama, T. Effect of a kinect-based exercise game on improving executive cognitive performance in community-dwelling elderly: Case control study. J. Med. Internet Res. 2014, 16, e61. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Perera, S.; Hile, E.; Keller, V.; Spadola-Bogard, J.; Garcia, J. Interactive video dance games for healthy older adults. J. Nutr. Health Aging 2010, 14, 850–852. [Google Scholar] [CrossRef] [PubMed]
- de Boissieu, P.; Denormandie, P.; Armaingaud, D.; Sanchez, S.; Jeandel, C. Exergames and elderly: A non-systematic review of the literature. Eur. Geriatr. Med. 2017, 8, 111–116. [Google Scholar] [CrossRef]
- Chao, Y.Y.; Scherer, Y.K.; Montgomery, C.A. Effects of using nintendo wii exergames in older adults: A review of the literature. J. Aging Health 2015, 27, 379–402. [Google Scholar] [CrossRef]
- Ogawa, E.F.; You, T.; Leveille, S.G. Potential benefits of exergaming for cognition and dual-task function in older adults: A systematic review. J. Aging Phys. Act. 2016, 24, 332–336. [Google Scholar] [CrossRef] [PubMed]
- Sell, K.; Lillie, T.; Taylor, J. Energy expenditure during physically interactive video game playing in male college students with different playing experience. J. Am. Coll. Health 2008, 56, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.; Aziz, A.R.; Chua, K.; Teh, K.C. Aerobic demands of the dance simulation game. Int. J. Sports Med. 2002, 23, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Graves, L.E.; Ridgers, N.D.; Williams, K.; Stratton, G.; Atkinson, G.; Cable, N.T. The physiological cost and enjoyment of wii fit in adolescents, young adults, and older adults. J. Phys. Act. Health 2010, 7, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Canabrava, K.L.R.; Faria, F.R.; Lima, J.R.P.; Guedes, D.P.; Amorim, P.R.S. Energy expenditure and intensity of active video games in children and adolescents. Res. Q. Exerc. Sport. 2018, 89, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Fabel, K.; Wolf, S.A.; Ehninger, D.; Babu, H.; Leal-Galicia, P.; Kempermann, G. Additive effects of physical exercise and environmental enrichment on adult hippocampal neurogenesis in mice. Front. Neurosci. 2009, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Barnes, J.N. Exercise, cognitive function, and Aging. Adv. Physiol. Educ. 2015, 39, 55–62. [Google Scholar] [CrossRef]
- Park, D.C.; Bischof, G.N. The aging mind: Neuroplasticity in response to cognitive training. Dialogues Clin. Neurosci. 2013, 15, 109–119. [Google Scholar]
- Willis, S.L.; Schaie, K.W. Cognitive training and plasticity: Theoretical perspective and methodological consequences. Restor. Neurol. Neurosci. 2009, 27, 375–389. [Google Scholar]
- Voelcker-Rehage, C.; Godde, B.; Staudinger, U.M. Physical and motor fitness are both related to cognition in old age. Eur. J. Neurosci. 2010, 31, 167–176. [Google Scholar] [CrossRef]
- Holtzer, R.; Shuman, M.; Mahoney, J.R.; Lipton, R.; Verghese, J. Cognitive fatigue defined in the context of attention networks. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2011, 18, 108–128. [Google Scholar] [CrossRef]
- Gangemi, A.; Caprì, T.; Fabio, R.; Paola, P.; Falzone, A.; Martino, G. Transcranial direct current stimulation (tdcs) and cognitive empowerment for the functional recovery of diseases with chronic impairment and genetic etiopathogenesis. Adv. Genet. Res. 2018, 18, 179–196. [Google Scholar]
- Marseglia, A.; Xu, W.; Fratiglioni, L.; Fabbri, C.; Berendsen, A.A.M.; Bialecka-Debek, A.; Jennings, A.; Gillings, R.; Meunier, N.; Caumon, E.; et al. Effect of the nu-age diet on cognitive functioning in older adults: A randomized controlled trial. Front. Physiol. 2018, 9, 349. [Google Scholar] [CrossRef]
- Klimesch, W. Eeg alpha and theta oscillations reflect cognitive and memory performance: A review and analysis. Brain Res. Brain Res. Rev. 1999, 29, 169–195. [Google Scholar] [CrossRef]
- Trammell, J.P.; MacRae, P.G.; Davis, G.; Bergstedt, D.; Anderson, A.E. The relationship of cognitive performance and the theta-alpha power ratio is age-dependent: An eeg study of short term memory and reasoning during task and resting-state in healthy young and old adults. Front. Aging Neurosci. 2017, 9, 364. [Google Scholar] [CrossRef] [PubMed]
- Salthouse, T.A. The processing-speed theory of adult age differences in cognition. Psychol. Rev. 1996, 103, 403–428. [Google Scholar] [CrossRef]
- Kuznetsova, K.A.; Maniega, S.M.; Ritchie, S.J.; Cox, S.R.; Storkey, A.J.; Starr, J.M.; Wardlaw, J.M.; Deary, I.J.; Bastin, M.E. Brain white matter structure and information processing speed in healthy older age. Brain Struct. Funct. 2016, 221, 3223–3235. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.H.; Lee, G.J.; Tishler, T.A.; Meghpara, M.; Thompson, P.M.; Bartzokis, G. Myelin breakdown mediates age-related slowing in cognitive processing speed in healthy elderly men. Brain Cogn. 2013, 81, 131–138. [Google Scholar] [CrossRef]
- Tseng, B.; Gundapuneedi, T.; Khan, M.; Diaz-Arrastia, R.; Levine, B.; Lu, H.; Huang, H.; Zhang, R. White matter integrity in physically fit older adults. Neuroimage 2013, 82, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Feter, N.; Freitas, M.P.; Gonzales, N.G.; Umpierre, D.; Cardoso, R.K.; Rombaldi, A.J. Effects of physical exercise on myelin sheath regeneration: A systematic review and meta-analysis. Sci. Sports 2018, 33, 8–21. [Google Scholar] [CrossRef]
- Bott, N.T.; Bettcher, B.M.; Yokoyama, J.S.; Frazier, D.T.; Wynn, M.; Karydas, A.; Yaffe, K.; Kramer, J.H. Youthful processing speed in older adults: Genetic, biological, and behavioral predictors of cognitive processing speed trajectories in Aging. Front. Aging Neurosci. 2017, 9, 55. [Google Scholar] [CrossRef] [PubMed]
- Desjardins-Crepeau, L.; Berryman, N.; Vu, T.T.; Villalpando, J.M.; Kergoat, M.J.; Li, K.Z.; Bosquet, L.; Bherer, L. Physical functioning is associated with processing speed and executive functions in community-dwelling older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2014, 69, 837–844. [Google Scholar] [CrossRef]
- Langlois, F.; Vu, T.T.; Chasse, K.; Dupuis, G.; Kergoat, M.J.; Bherer, L. Benefits of physical exercise training on cognition and quality of life in frail older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2013, 68, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.A. Exercise builds brain health: Key roles of growth factor cascades and inflammation. Trends Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Vaynman, S.; Gomez-Pinilla, F. License to run: Exercise impacts functional plasticity in the intact and injured central nervous system by using neurotrophins. Neurorehabil. Neural Repair 2005, 19, 283–295. [Google Scholar] [CrossRef]
- Cotman, C.W.; Berchtold, N.C. Exercise: A behavioral intervention to enhance brain health and plasticity. Trends Neurosci. 2002, 25, 295–301. [Google Scholar] [CrossRef]
- Maass, A.; Duzel, S.; Brigadski, T.; Goerke, M.; Becke, A.; Sobieray, U.; Neumann, K.; Lovden, M.; Lindenberger, U.; Backman, L.; et al. Relationships of peripheral igf-1, vegf and bdnf levels to exercise-related changes in memory, hippocampal perfusion and volumes in older adults. Neuroimage 2016, 131, 142–154. [Google Scholar] [CrossRef]
- van Praag, H.; Kempermann, G.; Gage, F.H. Running increases cell proliferation and neurogenesis in the adult mouse dentate gyrus. Nat. Neurosci. 1999, 2, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Kempermann, G.; Fabel, K.; Ehninger, D.; Babu, H.; Leal-Galicia, P.; Garthe, A.; Wolf, S.A. Why and how physical activity promotes experience-induced brain plasticity. Front. Neurosci. 2010, 4. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.J.; Tschakovsky, M.E. Exercise and circulating bdnf: Mechanisms of release and implications for the design of exercise interventions. Appl. Physiol. Nutr. Metab. 2018, 43, 1095–1104. [Google Scholar] [CrossRef]
- Wrann, C.D.; White, J.P.; Salogiannnis, J.; Laznik-Bogoslavski, D.; Wu, J.; Ma, D.; Lin, J.D.; Greenberg, M.E.; Spiegelman, B.M. Exercise induces hippocampal bdnf through a pgc-1α;/fndc5 pathway. Cell Metab. 2013, 18, 649–659. [Google Scholar] [CrossRef]
- Greenberg, M.E.; Xu, B.; Lu, B.; Hempstead, B.L. New insights in the biology of bdnf synthesis and release: Implications in cns function. J. Neurosci. 2009, 29, 12764–12767. [Google Scholar] [CrossRef]
- Je, H.S.; Yang, F.; Ji, Y.; Nagappan, G.; Hempstead, B.L.; Lu, B. Role of pro-brain-derived neurotrophic factor (probdnf) to mature bdnf conversion in activity-dependent competition at developing neuromuscular synapses. Proc. Natl. Acad. Sci. USA 2012, 109, 15924–15929. [Google Scholar] [CrossRef]
- Bolijn, S.; Lucassen, P.J. How the body talks to the brain; peripheral mediators of physical activity-induced proliferation in the adult hippocampus. Brain Plast. 2015, 1, 5–27. [Google Scholar] [CrossRef]
- Kramer, A.F.; Erickson, K.I. Capitalizing on cortical plasticity: Influence of physical activity on cognition and brain function. Trends Cogn. Sci. 2007, 11, 342–348. [Google Scholar] [CrossRef]
- Jeon, Y.K. Expression of brain-derived neurotrophic factor, igf-1 and cortisol elicited. J. Phys. Ther. Sci. 2015, 27, 737–741. [Google Scholar] [CrossRef]
- Morland, C.; Andersson, K.A.; Haugen, Ø.P.; Hadzic, A.; Kleppa, L.; Gille, A.; Rinholm, J.E.; Palibrk, V.; Diget, E.H.; Kennedy, L.H.; et al. Exercise induces cerebral vegf and angiogenesis via the lactate receptor hcar1. Nat. Commun. 2017, 8. [Google Scholar] [CrossRef]
- Ding, Y.H.; Li, J.; Zhou, Y.; Rafols, J.A.; Clark, J.C.; Ding, Y. Cerebral angiogenesis and expression of angiogenic factors in aging rats after exercise. Curr. Neurovasc. Res. 2006, 3, 15–23. [Google Scholar] [CrossRef]
- Black, J.E.; Isaacs, K.R.; Anderson, B.J.; Alcantara, A.A.; Greenough, W.T. Learning causes synaptogenesis, whereas motor activity causes angiogenesis, in cerebellar cortex of adult rats. Proc. Natl. Acad. Sci. USA 1990, 87, 5568–5572. [Google Scholar] [CrossRef]
- Erickson, K.I.; Weinstein, A.M.; Sutton, B.P.; Prakash, R.S.; Voss, M.W.; Chaddock, L.; Szabo, A.N.; Mailey, E.L.; White, S.M.; Wojcicki, T.R.; et al. Beyond vascularization: Aerobic fitness is associated with n-acetylaspartate and working memory. Brain Behav. 2012, 2, 32–41. [Google Scholar] [CrossRef]
- Spielman, L.J.; Little, J.P.; Klegeris, A. Physical activity and exercise attenuate neuroinflammation in neurological diseases. Brain Res. Bull. 2016, 125, 19–29. [Google Scholar] [CrossRef]
- Svensson, M.; Lexell, J.; Deierborg, T. Effects of physical exercise on neuroinflammation, neuroplasticity, neurodegeneration, and behavior: What we can learn from animal models in clinical settings. Neurorehabil. Neural Repair 2015, 29, 577–589. [Google Scholar] [CrossRef]
- Simioni, C.; Zauli, G.; Martelli, A.M.; Vitale, M.; Sacchetti, G.; Gonelli, A.; Neri, L.M. Oxidative stress: Role of physical exercise and antioxidant nutraceuticals in adulthood and Aging. Oncotarget 2018, 9, 17181–17198. [Google Scholar] [CrossRef]
- Young, S.N. How to increase serotonin in the human brain without drugs. J. Psychiatry Neurosci. 2007, 32, 394–399. [Google Scholar]
- Lin, T.W.; Kuo, Y.M. Exercise benefits brain function: The monoamine connection. Brain Sci. 2013, 3, 39–53. [Google Scholar] [CrossRef]
- Meeusen, R.; De Meirleir, K. Exercise and brain neurotransmission. Sports Med. 1995, 20, 160–188. [Google Scholar] [CrossRef]
- Boot, W.R.; Simons, D.J.; Stothart, C.; Stutts, C. The pervasive problem with placebos in psychology: Why active control groups are not sufficient to rule out placebo effects. Perspect. Psychol. Sci. 2013, 8, 445–454. [Google Scholar] [CrossRef]
- Neupert, S.D.; Lachman, M.E.; Whitbourne, S.B. Exercise self-efficacy and control beliefs predict exercise behavior after an exercise intervention for older adults. J. Aging Phys. Act. 2009, 17, 1–16. [Google Scholar] [CrossRef]
- McAuley, E.; Szabo, A.; Gothe, N.; Olson, E.A. Self-efficacy: Implications for physical activity, function, and functional limitations in older adults. Am. J. Lifestyle Med. 2011, 5. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Sample | Study Design | Intervention | Measures of Exercise Intensity | Outcome Measures | Results | Risk of Bias |
|---|---|---|---|---|---|---|---|
| Anderson-Hanley et al. (2012) [81] | Pre EG: n = 38, Age = 75.7 (9.9), F = 87% CG: n = 41, Age = 81.6 (6.2), F = 71% Post (12 weeks) EG: n = 30 CG: n = 33 R = 58–99 years | USA Two Groups RCT Supervised | 12 weeks, 5 × up to 45 min per week recommended, minimum of 25 rides for “completers” EG: stationary cycling with 3D virtual bike tour CG: stationary cycling | Controlled with HRR (60%) | EF (n = 3) PS (n =1) VF (n = 2) STM (n = 5) VSS (n = 2) BDNF (ELISA) | EG ↑in EF (2/3, d = 0.5) CG ↓ in EF (1/3) EG > CG in *EF (np2 = 0.21) EG > CG in BDNF Adherence: EG (79%), CG (80%) | High |
| Bacha et al. (2018) [82] | Pre EG: n = 25 CG: n = 25 Post (7 weeks) EG: n = 23, Age = 71.0, F = 65% CG: n = 23, Age = 66.5, F = 83% Retention (4 weeks after post-test) | Brazil Two Groups RCT Supervised | 7 weeks, 2 × 60 min per week EG: Xbox Kinect Adventure Games CG: Conventional Physiotherapy | n.a. | MoCA | EG ↑ in MoCA CG ↑ in MoCA Adherence: EG (92%), CG (92%) | Low |
| Barcelos et al. (2015) [83] | Pre EGI: n = 23 EGII: n = 25 Post (12 weeks) EGI: n = 10, Age = 84.8 (11.3), F = 25% EGII: n = 10, Age = 85.3 (6.9), F = 80% | USA and Ireland Two Groups RCT Pilot Unsupervised | 12 weeks, 2 × 20 min per week (minimum threshold, recommended increase 3–5 × up to 45 min per week) EGI: stationary Cybercycling plus video game EGII: stationary Cybercycling plus virtual tour | Controlled with HR | EF (n = 3) MoCA | Results on healthy subsamples EGI > EGII (1/3, np2 = 0.69) (Full) Adherence: EG (40%), EGII (43%) | High |
| Chuang et al. (2015). [91] | Pre n = 32, F = 100% Post (12 weeks) EG: n = 7, Age = 69.4 (3.8) CGI: n = 11, Age = 67.0 (1.7) CGII: n = 8, Age = 68.3 (4) | Taiwan Three Groups UCT Supervised | 12 weeks, 3 × 30 min per week EG: Dance Dance Revolution CGI: brisk walking CGII: passive | Controlled with HRmax (40–60%), RPE | EF (n = 1) MMSE EEG: ERPs during Flanker task | EG/CGI ↑ in EF (d = 1.18 (EG) and 0.37 (CGI)) CGII ↓ in EF (d = 0.72) N2 latency: EG and CGI < CGII (d = 2.02 (EG), d = 2.51 (CGI)) P3 latency: EG and CGI < CG II (d = 1.03 (EG), d = 1.21 (CGI)) Adherence: overall (81%) | High |
| Eggenberger et al. (2015) [84] | Pre EG: n = 30 CGI: n = 29 CGII: n = 30 Between (3 Month) EG: n = 25 CGI: n = 24 CGII: n = 26 Post (6 Month) EG: n = 24, Age = 77.3 (6.3), F = 58% CGI: n = 22, Age = 78.5 (5.1), F = 72% CGII: n = 25, Age = 80.8 (4.7), F = 64% Retention (12 month after post-test) | Switzerland Three Groups RCT Supervised (except 4 weeks) | 26 weeks, 2 × 60 min per week in group settings, 20 min group specific training (EG, CGI, CGII) + 40 min balance and strength training EG: Virtual Reality Dance Video Game (Platform) CGI: treadmill + stimulus verbal memory training CGII: treadmill + strength and balance exercises for each group | RPE (monitored only for CGs) | EF (n = 2) PS (n = 4) STM (n = 1) LTM (n = 2) | EG/CGI/CGII ↑ in *EF EG/CGI/CGII ↑ in *LTM EG/CGI/CGII ↑in *PS Adherence: 3 m 6 m 18 m EG (83%, 80%, 50%), CGI (83%, 75%, 58%), CGII (87%, 83%, 50%) | Moderate |
| Eggenberger et al. (2016) [85] | Pre EG: n = 22 CG: n = 20 Post (8 weeks) EG: n = 19, Age = 72.8 (5.9), F = 63% CG: n = 14, Age = 77.8 (7.4), F = 64% | Switzerland Two Groups RCT Supervised | 8 weeks, 3 × 30 min per week EG: Virtual Reality Dance Video Game (Platform) CG: balance and stretching | RPE (monitored) | EF (n = 3) PS (n = 1) MoCA fNIRS: HbO2 level during preferred and fast treadmill walking (PFC) | EG > CG in EF (1/3) EG/CG ↓ PFC activity (first 7 s of preferred walking, r = 0.32/0.36, trend fast walking, r = 0.25) EG < CG PFC activity (last 7 s of fast walking r = 0.32) EG/CG: lPFC > rPFC activity after training, r = 0.26–0.32 EG > CG: lPFC activity (r = 0.23/0.27) Adherence: EG (86%), CG (64%) | Moderate |
| Guimaraes et al., (2018) [86] | Pre n = 36, F = 61% Post (12 weeks) EG: n = 13, Age = 60.0 (4.0), F = 77% CG: n = 14, Age = 60.7 (3.6), F = 43% | Brazil Two Groups RCT Supervised | 12 weeks, 3 × 60 min per week (+ 3 previous sessions) EG: Microsoft Kinect Sport Games CG: Treadmill and cycle ergometers Both: 5–10 min warm up and 5–10 min stretching | HR (EG monitored; CG controlled: 40–59% HRR) | EF (n = 2) PS (n = 2) STM (n = 2) MMSE | EG ↑ in EF (1/2) EG ↑ in STM (1/2) CG ↑ in EF (1/2) CG ↑ in PS (1/2) CG ↑ in *STM CG ↑ in MMSE Adherence: EG: (91%), CG (87%) | low |
| Kayama et al. (2014) [92] | Pre Age ≥ 65EG: n = 30 CG: n = 18 Post (12 weeks) EG: n = 26 CG: n = 15 | Japan Two Groups UCT Supervised | 12 weeks, 1 × 80 min per week EG: 75 min traditional training (cf. CG) + 5 min Dual Task Tai Chi (Kinect) CG: 80 min aerobic, strength, balance, and flexibility training | n.a. | EF (n = 2) PS (n = 1) VF (n = 1) | EG > CG in EF (1/2) Adherence: EG (87%), CG (83%) | Unclear |
| Maillot et al. (2012) [79] | Pre F = 84% EG: n = 16 CG: n = 16 Post (12 weeks) EG: n = 15, Age = 73.5 (3.0) CG: n = 15, Age = 73.5 (4.1) | France Two Groups RCT Supervised | 12 weeks, 2 × 60 min per week EG: Nintendo Wii CG: No-training no-contact | HR (monitored on 2nd, 12th, and 20th session) | EF (n = 5) PS (n = 4) VSS (n = 4) CP (n = 1) | EG > CG in *EF (np2 = 0.81) EG > CG in *PS (np2 = 0.79) EG > CG in VSS (1/4, np2 = 0.23) Adherence: EG (94%), CG (94%) | Unclear |
| Ordnung et al. (2017) [87] | Pre EG: n = 15, Age = 69.8 (6.3), F = n.a. CG: n = 15, Age = 68.6 (4.7), F = 53% Post (6 weeks) EG: n = 14, F = 50% CG: n = 15, F = 53% | Germany Two Groups RCT Supervised | 6 weeks, 2 × 60 min per week EG: Xbox Kinect Video Sport Games CG: passive | Pulse (only to prevent overexertion) | EF (n = 2) PS (n = 2) | EG ↑ *PS (r = 0.61 and r = 0.55) Adherence: EG (93%), CG (100%) | low |
| Park and Yim (2016) [88] | Pre EG: n = 36, Age = 73 (3), F = 92% CG: n = 36, Age = 74.11 (2.9), F = 97% Post (6 weeks) EG: n = 36 CG: n = 36 | Korea Two Groups RCT Supervised | 6 weeks, 2 × 30 min per week EG: 1 × 30 min of conventional training, then 3D virtual Kayak Tour CG: 1 × 30 min of conventional exercise (then passive) | n.a. | MoCA | EG ↑ in MoCA CG ↓ in MoCA EG > CG in MoCA Adherence: EG (100%), CG (100%) | Low |
| Schättin et al. (2016) [89] | Pre EG: n = 15 CG: n = 14 Post (8 weeks) EG: n = 13, Age = 80, F = 38% CG: n = 14, Age = 80, F = 50% | Switzerland Two Groups RCT Supervised | 8 weeks, 3 × 30 min per week in groups (5 min warm-up, 5 min cool-down, 20 min group specific training) EG: Video Game Dance Platform CG: Conventional Balance Training | n.a. | EF (n = 3) CP (n = 2) EEG: ERO (PFC, 1–30 Hz) | EG ↑ *EF (r = 0.46–0.57) EG ↑ *CP (r = 0.40–0.50) CG ↑ in EF (1/3, r = 0.39) EG ↓ Theta Power during CP Adherence: EG (87%), CG (100%) | Moderate |
| Schoene, et al. (2013) [90] | Pre EG: n = 18 CG: n = 19 Post (8 weeks) EG: n = 15, Age = 77.5 (4.5) CG: n = 17, Age = 78.4 (4.5) | Australia Two Groups Unsupervised RCT | 8 weeks, 2–3 × 15–20 min per week EG: Video-game based Step Pad CG: Passive | n.a. | EF (n = 1) PS (n = 1) CP (n = 1) DT (n = 2) | EG > CG in CP EG > in DT (1/2) Adherence: EG (83%), CG (89%) | Low |
| Schoene, et al. (2015) [76] | Pre EG: n = 47, Age = 82 (7), F = 66% CG: n = 43, Age = 81 (7), F = 67% Post (16 weeks) EG: n = 39 CG: n = 42 | Australia Two Groups Unsupervised RCT | 16 weeks, 3 × 20 min per week EG: electronic step game CG: Passive (brochure on fall prevention) | n.a. | EF (n = 3) PS (n = 3) CP (n = 2) VSS (n =1) DT (n = 2) | EG > CG in PS (2/3) EG > CG in *CP EG > CG in VSS (1/2) EG > CG in DT (1/2) Adherence: EG (83%), CG (98%) | Low |
| Studenski et al. (2010) [93] | Pre EG: n = 36, Age = 80.1 (5.4), F = 83% Post (12 weeks) EG: n = 25, Age = 80.2 (5.4), F = 80% | USA One Group Supervised UT | 12 weeks, 2 × 45–60 min per week EG: Dance Dance Revolution | n.a. | PS (n = 1) | Adherence: EG (70%) | moderate |
| Interaction Effects | Within Group Effects | ||||
|---|---|---|---|---|---|
| Active Controls | Passive Controls | Exergamers | Active Controls | Passive Controls | |
| Executive functions | 4/8 | 1/5 | 5/12 | 4/8 and 1/8 ↓ | 0/6 and 1/6 ↓ |
| Processing speed | 0/5 | 2/5 | 2/10 | 2/5 | 0/4 |
| Controlled processing | 0/1 | 2/3 | 1/4 | 0/1 | 0/3 |
| Visuospatial skills | 0/1 | 2/2 | 0/3 | 0/1 | 0/2 |
| Verbal fluency | 0/2 | n.a. | 0/2 | 0/2 | n.a. |
| Dual-tasking | n.a. | 2/2 | 0/2 | n.a. | 0/2 |
| Short-term memory | 0/3 | n.a. | 1/3 | 1/3 | n.a. |
| Long-term memory | 0/1 | n.a. | 1/1 | 1/1 | n.a. |
| Cognitive state -MoCA | 0/3 | 1/1 | 2/4 | 1/3 | 1/1↓ |
| Cognitive state - MMSE | 0/2 | 0/1 | 0/2 | 1/2 | 0/1 |
| Overall | 4/9 (44%) | 4/6 (66%) | 8/15 (53%) | 5/9 (55%) | 0/6 (0%) and 2/6↓ (33%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stojan, R.; Voelcker-Rehage, C. A Systematic Review on the Cognitive Benefits and Neurophysiological Correlates of Exergaming in Healthy Older Adults. J. Clin. Med. 2019, 8, 734. https://doi.org/10.3390/jcm8050734
Stojan R, Voelcker-Rehage C. A Systematic Review on the Cognitive Benefits and Neurophysiological Correlates of Exergaming in Healthy Older Adults. Journal of Clinical Medicine. 2019; 8(5):734. https://doi.org/10.3390/jcm8050734
Chicago/Turabian StyleStojan, Robert, and Claudia Voelcker-Rehage. 2019. "A Systematic Review on the Cognitive Benefits and Neurophysiological Correlates of Exergaming in Healthy Older Adults" Journal of Clinical Medicine 8, no. 5: 734. https://doi.org/10.3390/jcm8050734
APA StyleStojan, R., & Voelcker-Rehage, C. (2019). A Systematic Review on the Cognitive Benefits and Neurophysiological Correlates of Exergaming in Healthy Older Adults. Journal of Clinical Medicine, 8(5), 734. https://doi.org/10.3390/jcm8050734