Cardiovascular Safety and Possible Benefit of a 5-Alpha Reductase Inhibitor among Benign Prostatic Hyperplasia Patients, A Nationally Representative Cohort of Korean Men


Abstract
1. Introduction
2. Materials and Methods
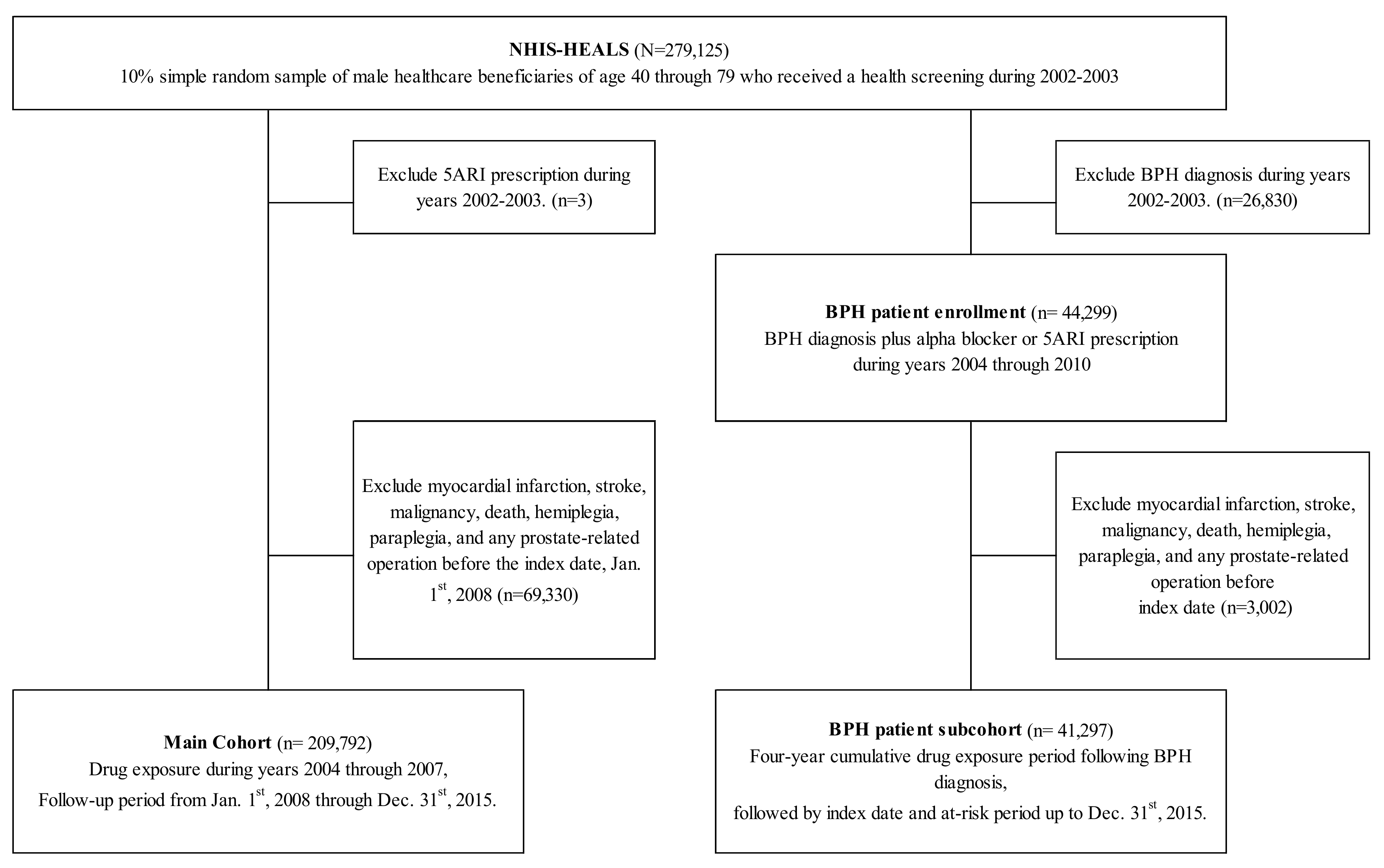
2.1. Study Sample
2.2. Study Design of the Main Cohort
2.3. Study Design of the BPH Patient Subcohort
2.4. Ascertainment of Event Outcomes
2.5. Drug Exposure
2.6. Determination of Covariates
2.7. Statistical Analysis
3. Results
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Azzouni, F.; Godoy, A.; Li, Y.; Mohler, J. The 5 alpha-reductase isozyme family: A review of basic biology and their role in human diseases. Adv. Urol. 2012, 2012, 530121. [Google Scholar] [CrossRef] [PubMed]
- Roehrborn, C.G.; Boyle, P.; Nickel, J.C.; Hoefner, K.; Andriole, G. Efficacy and safety of a dual inhibitor of 5-alpha-reductase types 1 and 2 (dutasteride) in men with benign prostatic hyperplasia. Urology 2002, 60, 434–441. [Google Scholar] [CrossRef]
- Uygur, M.C.; Arik, A.I.; Altug, U.; Erol, D. Effects of the 5 alpha-reductase inhibitor finasteride on serum levels of gonadal, adrenal, and hypophyseal hormones and its clinical significance: A prospective clinical study. Steroids 1998, 63, 208–213. [Google Scholar] [CrossRef]
- McVary, K.T.; Roehrborn, C.G.; Avins, A.L.; Barry, M.J.; Bruskewitz, R.C.; Donnell, R.F.; Foster, H.E., Jr.; Gonzalez, C.M.; Kaplan, S.A.; Penson, D.F.; et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J. Urol. 2011, 185, 1793–1803. [Google Scholar] [CrossRef] [PubMed]
- Yeap, B.B.; Alfonso, H.; Chubb, S.A.; Handelsman, D.J.; Hankey, G.J.; Almeida, O.P.; Golledge, J.; Norman, P.E.; Flicker, L. In older men an optimal plasma testosterone is associated with reduced all-cause mortality and higher dihydrotestosterone with reduced ischemic heart disease mortality, while estradiol levels do not predict mortality. J. Clin. Endocrinol. Metab. 2014, 99, E9–E18. [Google Scholar] [CrossRef]
- Saylor, P.J.; Smith, M.R. Metabolic Complications of Androgen Deprivation Therapy for Prostate Cancer. J. Urol. 2013, 189, S34–S44. [Google Scholar] [CrossRef] [PubMed]
- Keating, N.L.; O’Malley, A.J.; Freedland, S.J.; Smith, M.R. Diabetes and Cardiovascular Disease During Androgen Deprivation Therapy: Observational Study of Veterans With Prostate Cancer. J. Natl. Cancer Inst. 2010, 102, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Jespersen, C.G.; Nørgaard, M.; Borre, M. Androgen-deprivation Therapy in Treatment of Prostate Cancer and Risk of Myocardial Infarction and Stroke: A Nationwide Danish Population-based Cohort Study. Eur. Urol. 2014, 65, 704–709. [Google Scholar] [CrossRef]
- Shores, M.M.; Biggs, M.L.; Arnold, A.M.; Smith, N.L.; Longstreth, W.T., Jr.; Kizer, J.R.; Hirsch, C.H.; Cappola, A.R.; Matsumoto, A.M. Testosterone, dihydrotestosterone, and incident cardiovascular disease and mortality in the cardiovascular health study. J. Clin. Endocrinol. Metab. 2014, 99, 2061–2068. [Google Scholar] [CrossRef]
- Shores, M.M.; Arnold, A.M.; Biggs, M.L.; Longstreth, W.T., Jr.; Smith, N.L.; Kizer, J.R.; Cappola, A.R.; Hirsch, C.H.; Marck, B.T.; Matsumoto, A.M. Testosterone and dihydrotestosterone and incident ischaemic stroke in men in the Cardiovascular Health Study. Clin. Endocrinol. (Oxf.) 2014, 81, 746–753. [Google Scholar] [CrossRef]
- Andriole, G.L.; Bostwick, D.G.; Brawley, O.W.; Gomella, L.G.; Marberger, M.; Montorsi, F.; Pettaway, C.A.; Tammela, T.L.; Teloken, C.; Tindall, D.J.; et al. Effect of dutasteride on the risk of prostate cancer. N. Engl. J. Med. 2010, 362, 1192–1202. [Google Scholar] [CrossRef] [PubMed]
- Loke, Y.K.; Ho, R.; Smith, M.; Wong, O.; Sandhu, M.; Sage, W.; Singh, S. Systematic review evaluating cardiovascular events of the 5-alpha reductase inhibitor—Dutasteride. J. Clin. Pharm. Ther. 2013, 38, 405–415. [Google Scholar] [CrossRef]
- Hsieh, T.F.; Yang, Y.W.; Lee, S.S.; Lin, T.H.; Liu, H.H.; Tsai, T.H.; Chen, C.C.; Huang, Y.S.; Lee, C.C. Use of 5-Alpha-Reductase Inhibitors Did Not Increase the Risk of Cardiovascular Diseases in Patients with Benign Prostate Hyperplasia: A Five-Year Follow-Up Study. PLoS ONE 2015, 10, e0119694. [Google Scholar] [CrossRef]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data Resource Profile: The National Health Information Database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef] [PubMed]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed]
- Guidelines for ATC classification and DDD assignment. WHO Collaborating Centre for Drug Statistics Methodology 2018, Oslo, Norway 2017. Available online: https://www.whocc.no/news/guidelines_for_atc_classification_and_ddd_assignment (accessed on 22 May 2018).
- ATC classification index with DDDs. WHO Collaborating Centre for Drug Statistics Methodology, Oslo, Norway 2018. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 22 May 2018).
- Nishiyama, T.; Hashimoto, Y.; Takahashi, K. The influence of androgen deprivation therapy on dihydrotestosterone levels in the prostatic tissue of patients with prostate cancer. Clin. Cancer Res. 2004, 10, 7121–7126. [Google Scholar] [CrossRef]
- Page, S.T.; Lin, D.W.; Mostaghel, E.A.; Hess, D.L.; True, L.D.; Amory, J.K.; Nelson, P.S.; Matsumoto, A.M.; Bremner, W.J. Persistent Intraprostatic Androgen Concentrations after Medical Castration in Healthy Men. J. Clin. Endocrinol. Metab. 2006, 91, 3850–3856. [Google Scholar] [CrossRef]
- Araujo, A.B.; Kupelian, V.; Page, S.T.; Handelsman, D.J.; Bremner, W.J.; McKinlay, J.B. Sex steroids and all-cause and cause-specific mortality in men. Arch. Intern. Med. 2007, 167, 1252–1260. [Google Scholar] [CrossRef] [PubMed]
- Swerdloff, R.S.; Dudley, R.E.; Page, S.T.; Wang, C.; Salameh, W.A. Dihydrotestosterone: Biochemistry, Physiology, and Clinical Implications of Elevated Blood Levels. Endocr. Rev. 2017, 38, 220–254. [Google Scholar] [CrossRef] [PubMed]
- Bosco, C.; Bosnyak, Z.; Malmberg, A.; Adolfsson, J.; Keating, N.L.; Van Hemelrijck, M. Quantifying observational evidence for risk of fatal and nonfatal cardiovascular disease following androgen deprivation therapy for prostate cancer: A meta-analysis. Eur. Urol. 2015, 68, 386–396. [Google Scholar] [CrossRef]
- Crawford, E.D.; Schally, A.V.; Pinthus, J.H.; Block, N.L.; Rick, F.G.; Garnick, M.B.; Eckel, R.H.; Keane, T.E.; Shore, N.D.; Dahdal, D.N.; et al. The potential role of follicle-stimulating hormone in the cardiovascular, metabolic, skeletal, and cognitive effects associated with androgen deprivation therapy. Urol. Oncol. 2017, 35, 183–191. [Google Scholar] [CrossRef]
- Klotz, L.; Nabid, A.; Higano, C.; Ryanm, C.; Kebabdjian, M.; Chin, J. Effect of dutasteride in men receiving intermittent androgen ablation therapy: The AVIAS trial. Can. Urol. Assoc. J. 2014, 8, E789–E794. [Google Scholar] [CrossRef]
- Ghanadian, R.; Lewis, J.G.; Chisholm, G.D.; O’Donoghue, E.P. Serum dihydrotestosterone in patients with benign prostatic hypertrophy. Br. J. Urol. 1977, 49, 541–544. [Google Scholar] [CrossRef]
- Horton, R.; Hsieh, P.; Barberia, J.; Pages, L.; Cosgrove, M. Altered blood androgens in elderly men with prostate hyperplasia. J. Clin. Endocrinol. Metab. 1975, 41, 793–796. [Google Scholar] [CrossRef]
- Hammond, G.L.; Kontturi, M.; Vihko, P.; Vihko, R. Serum steroids in normal males and patients with prostatic diseases. Clin. Endocrinol. (Oxf.) 1978, 9, 113–121. [Google Scholar] [CrossRef]
- Borst, S.E.; Shuster, J.J.; Zou, B.; Ye, F.; Jia, H.; Wokhlu, A.; Yarrow, J.F. Cardiovascular risks and elevation of serum DHT vary by route of testosterone administration: A systematic review and meta-analysis. BMC Med. 2014, 12, 211. [Google Scholar] [CrossRef]
- Ajayi, A.A.L.; Mathur, R.; Halushka, P.V. Testosterone Increases Human Platelet Thromboxane A2 Receptor Density and Aggregation Responses. Circulation 1995, 91, 2742–2747. [Google Scholar] [CrossRef]
- Thompson, I.M.; Goodman, P.J.; Tangen, C.M.; Lucia, M.S.; Miller, G.J.; Ford, L.G.; Lieber, M.M.; Cespedes, R.D.; Atkins, J.N.; Lippman, S.M.; et al. The influence of finasteride on the development of prostate cancer. N. Engl. J. Med. 2003, 349, 215–224. [Google Scholar] [CrossRef]
- McKee, M.; Britton, A.; Black, N.; McPherson, K.; Sanderson, C.; Bain, C. Methods in health services research. Interpreting the evidence: Choosing between randomised and non-randomised studies. BMJ 1999, 319, 312–315. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| %, Unless Otherwise Stated | Main Cohort | BPH Patient Subcohort | ||||
|---|---|---|---|---|---|---|
| Non-User | User | p Value * | Non-User | User | p Value * | |
| n (number) | 200,641 | 9151 | 20,749 | 20,548 | ||
| Age | <0.001 | <0.001 | ||||
| 40–50 | 33.4 | 9.3 | 15.4 | 8.4 | ||
| 50–60 | 40.4 | 31.1 | 39.8 | 32.3 | ||
| 60–70 | 19.2 | 37.6 | 29.2 | 36.6 | ||
| ≥70 | 7.0 | 22.1 | 15.6 | 22.7 | ||
| Body Mass Index, kg/m2 | 0.388 | 0.130 | ||||
| <23 | 35.9 | 35.2 | 35.8 | 35.0 | ||
| 23–25 | 28.8 | 29.0 | 28.9 | 29.7 | ||
| ≥25 | 35.3 | 35.7 | 35.3 | 35.3 | ||
| Smoking Habit | <0.001 | <0.001 | ||||
| Never | 39.2 | 49.2 | 40.7 | 44.5 | ||
| Past | 14.7 | 16.6 | 32.3 | 31.5 | ||
| Current | 41.9 | 29.9 | 24.4 | 21.5 | ||
| Alcohol Consumption, per week | <0.001 | <0.001 | ||||
| Fewer than once | 52.2 | 59.0 | 46.6 | 51.3 | ||
| 1–2 | 27.3 | 22.4 | 31.6 | 28.7 | ||
| ≥3 | 19.2 | 17.1 | 21.1 | 19.2 | ||
| Exercise Frequency, per week | <0.001 | 0.101 | ||||
| Fewer than once | 46.8 | 46.9 | 12.3 | 12.4 | ||
| 1–2 | 30.5 | 26.3 | 35.9 | 36.8 | ||
| ≥3 | 20.0 | 24.4 | 51.8 | 50.8 | ||
| Socioeconomic Status, quartiles | <0.001 | <0.001 | ||||
| Q1, Lowest | 23.7 | 26.3 | 24.7 | 27.2 | ||
| Charlson Comorbidity Index | <0.001 | <0.001 | ||||
| ≥3 | 9.8 | 20.3 | 45.2 | 49.8 | ||
| Outpatient Visits, tertiles | <0.001 | <0.001 | ||||
| Q3, most frequent | 33.2 | 67.9 | 30.2 | 39.2 | ||
| High cholesterol | 12.4 | 13.4 | 0.001 | 9.4 | 8.8 | 0.064 |
| Hypertension | 35.8 | 38.4 | <0.001 | 22.6 | 23.5 | 0.027 |
| Benign Prostatic Hyperplasia | 10.6 | 96.5 | <0.001 | 100 | 100 | |
| Diabetes | 11.5 | 14.2 | <0.001 | 13.0 | 13.0 | 0.902 |
| Atrial Fibrillation or Flutter | 1.2 | 2.5 | <0.001 | 1.0 | 1.0 | 0.869 |
| Angina | 9.2 | 18.0 | <0.001 | 6.2 | 6.3 | 0.689 |
| Acute Urinary Retention | 0.1 | 1.6 | <0.001 | 0.4 | 0.7 | <0.001 |
| Alpha-blocker use † | 2.3 | 48.2 | <0.001 | 45.5 | 65.1 | <0.001 |
| Aspirin use † | 9.9 | 18.5 | <0.001 | 25.8 | 29.5 | <0.001 |
| Non-aspirin NSAID use † | 24.2 | 45.0 | <0.001 | 48.5 | 54.7 | <0.001 |
| HMG-CoA reductase inhibitor use † | 7.0 | 11.7 | <0.001 | 22.0 | 23.9 | <0.001 |
| Exposure to 5ARI | ||
|---|---|---|
| Non-User (0 cDDD) | User (≥1 cDDD) | |
| Main cohort | ||
| CVD (Stroke or MI) | ||
| Cases | 10,101 | 744 |
| aHR * (95% CI) | 1(ref.) | 1.06 (0.91–1.23) |
| Myocardial Infarction | ||
| Cases | 2387 | 148 |
| aHR * (95% CI) | 1(ref.) | 1.11 (0.81–1.53) |
| Stroke | ||
| Cases | 7682 | 587 |
| aHR * (95% CI) | 1(ref.) | 1.04 (0.88–1.23) |
| BPH patient subcohort | ||
| CVD (Stroke or MI) | ||
| Cases | 1348 | 1536 |
| aHR * (95% CI) | 1(ref.) | 0.95 (0.88–1.03) |
| Myocardial Infarction | ||
| Cases | 285 | 282 |
| aHR * (95% CI) | 1(ref.) | 0.86 (0.72–1.02) |
| Stroke | ||
| Cases | 1067 | 1256 |
| aHR * (95% CI) | 1(ref.) | 0.97 (0.89–1.06) |
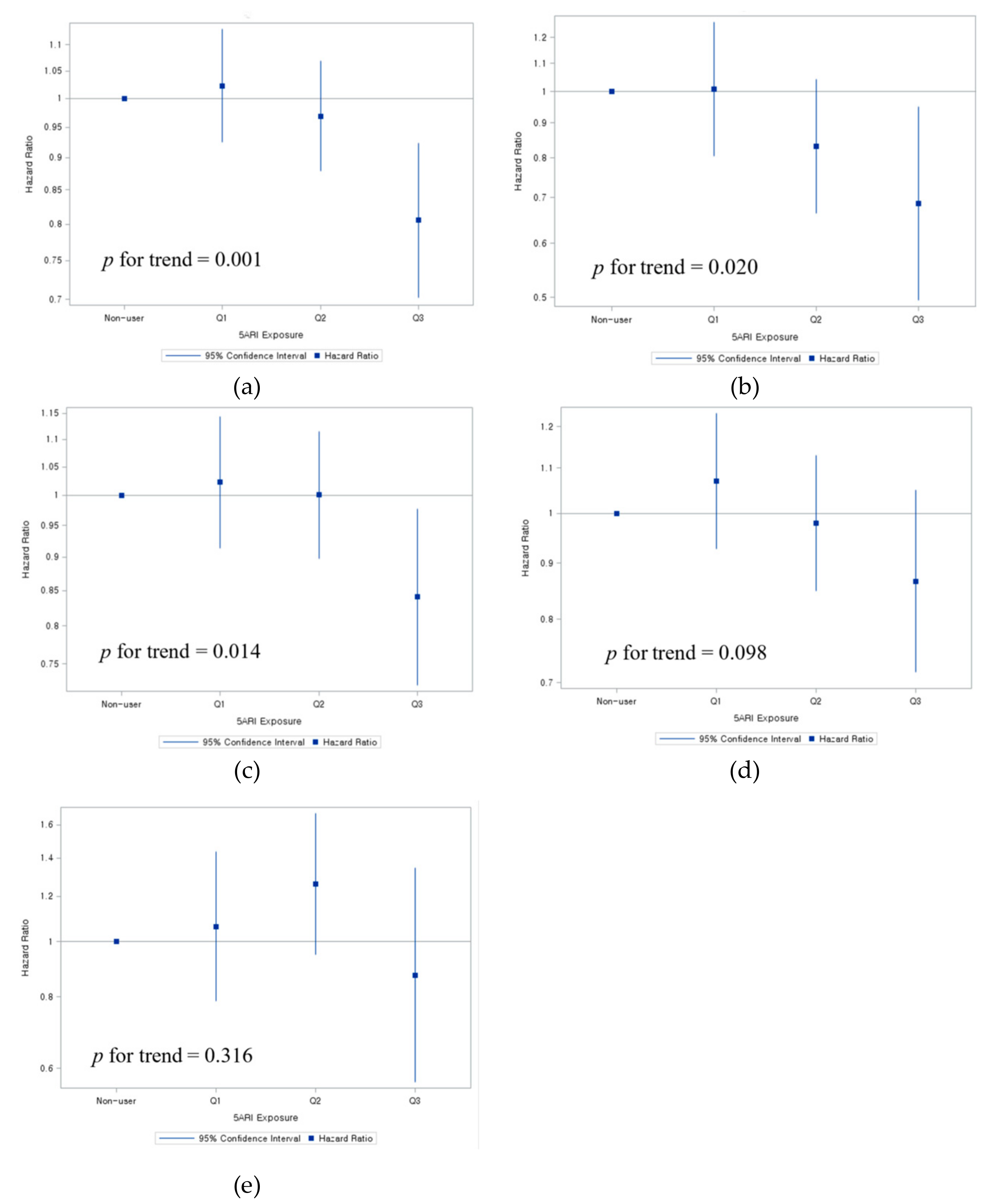
| BPH Patient Subcohort | Non-User | 5ARI Exposure | ||||
|---|---|---|---|---|---|---|
| Q1 of User (1–42 cDDD) aHR * (95% CI) | Q2 of User (43–216 cDDD) aHR * (95% CI) | Q3 of User (≥217 cDDD) aHR * (95% CI) | ||||
| Aspirin User (>30 cDDD) | CVD | 1(ref.) | 0.95 (0.81–1.10) | 0.93 (0.80–1.09) | 0.90 (0.77–1.06) | |
| MI | 1(ref.) | 0.85 (0.62–1.17) | 0.69 (0.50-0.96) | 0.78 (0.56–1.09) | ||
| Stroke | 1(ref.) | 0.98 (0.82–1.16) | 1.01 (0.85–1.20) | 0.95 (0.79–1.13) | ||
| Aspirin Non-user | CVD | 1(ref.) | 1.00 (0.87–1.16) | 1.02 (0.87–1.19) | 0.74 (0.61–0.89) | |
| MI | 1(ref.) | 1.19 (0.84–1.68) | 0.81 (0.53–1.22) | 0.72 (0.45–1.16) | ||
| Stroke | 1(ref.) | 0.96 (0.82–1.13) | 1.05 (0.89–1.25) | 0.74 (0.61–0.91) | ||
| Age ≥60 years | CVD | 1 (ref.) | 1.01 (0.90–1.13) | 0.98 (0.87–1.11) | 0.81 (0.71–0.92) | |
| MI | 1 (ref.) | 0.97 (0.73–1.27) | 0.85 (0.63–1.15) | 0.69 (0.50–0.96) | ||
| Stroke | 1 (ref.) | 1.01 (0.89–1.15) | 1.00 (0.88–1.14) | 0.84 (0.73–0.97) | ||
| Age <60 years | CVD | 1 (ref.) | 1.06 (0.86–1.32) | 1.03 (0.82–1.28) | 0.95 (0.73–1.26) | |
| MI | 1 (ref.) | 1.13 (0.75–1.69) | 0.66 (0.41–1.06) | 1.08 (0.66–1.77) | ||
| Stroke | 1 (ref.) | 1.04 (0.81–1.35) | 1.18 (0.92–1.52) | 0.90 (0.65–1.26) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, J.; Choi, S.; Kim, K.; Park, S.M. Cardiovascular Safety and Possible Benefit of a 5-Alpha Reductase Inhibitor among Benign Prostatic Hyperplasia Patients, A Nationally Representative Cohort of Korean Men. J. Clin. Med. 2019, 8, 733. https://doi.org/10.3390/jcm8050733
Chang J, Choi S, Kim K, Park SM. Cardiovascular Safety and Possible Benefit of a 5-Alpha Reductase Inhibitor among Benign Prostatic Hyperplasia Patients, A Nationally Representative Cohort of Korean Men. Journal of Clinical Medicine. 2019; 8(5):733. https://doi.org/10.3390/jcm8050733
Chicago/Turabian StyleChang, Jooyoung, Seulggie Choi, Kyuwoong Kim, and Sang Min Park. 2019. "Cardiovascular Safety and Possible Benefit of a 5-Alpha Reductase Inhibitor among Benign Prostatic Hyperplasia Patients, A Nationally Representative Cohort of Korean Men" Journal of Clinical Medicine 8, no. 5: 733. https://doi.org/10.3390/jcm8050733
APA StyleChang, J., Choi, S., Kim, K., & Park, S. M. (2019). Cardiovascular Safety and Possible Benefit of a 5-Alpha Reductase Inhibitor among Benign Prostatic Hyperplasia Patients, A Nationally Representative Cohort of Korean Men. Journal of Clinical Medicine, 8(5), 733. https://doi.org/10.3390/jcm8050733