
Experiences of the COVID-19 Lockdown and Telehealth in Aotearoa New Zealand: Lessons and Insights from Mental Health Clinicians


Abstract
:1. Introduction
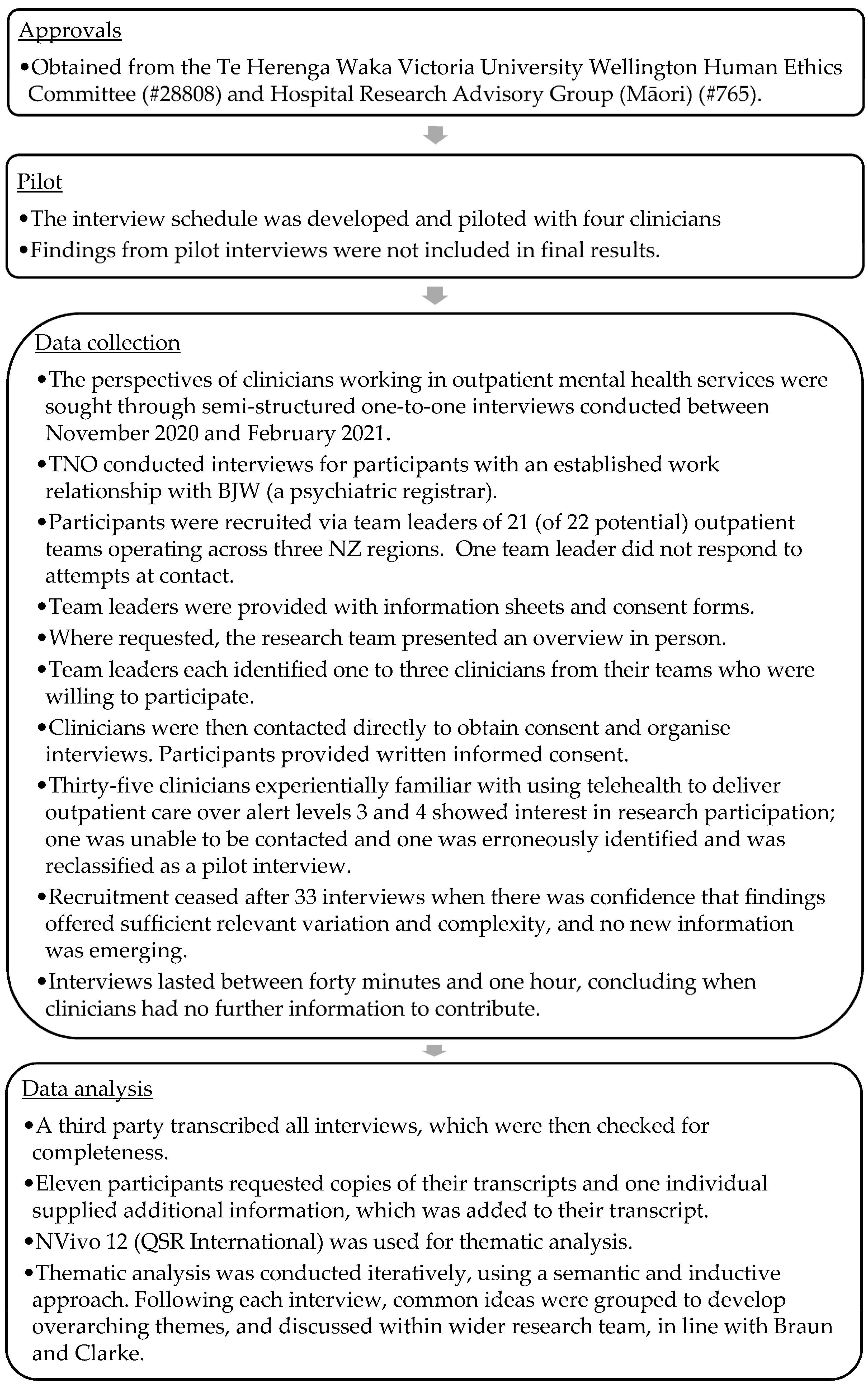
2. Materials and Methods
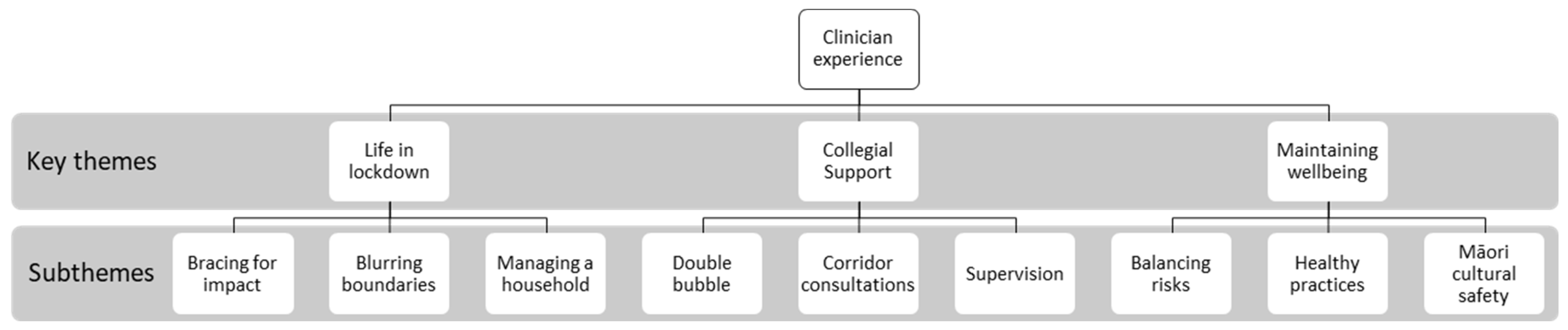
3. Results
3.1. Life in Lockdown
3.1.1. Bracing for Impact
I wasn’t sure how catastrophic the situation might develop… I was prepared to be really in an acute scenario similar to Italy, so no sleep, no contact with partner, to live in hospital environment, long working hours almost to the exhaustion.(P19)
…there was no PPE gear, which I also didn’t know how to use.(P17)
We only ever had four laptops across both teams [24 clinicians]… we automatically had to assume that our tangata motuhake [people special to the participant, in this case, other staff] had Zoom for starters, had equipment themselves in order to be able to do that.(P8)
Operations or management, the decree-ers, acknowledged that if they were to do it again, they’d probably do it differently and might actually listen more to what we were saying.(P8)
3.1.2. Blurring Boundaries
Because bringing the work into your own bedroom, having some rather unpleasant conversations with some unpleasant people, there are those energies coming into the space of your own home, was a little bit tough… I started off thinking I could work in my garden shed, that was too uncomfortable. Then we tried to pitch a tent in the front garden.(P4)
Some of my colleagues they were getting lots of verbal abuse from clients and felt attacked. That was a bit more confronting for them being at home… Whereas at work, you’ve got a bit more of a barrier up.(P6)
3.1.3. Managing a Household
Trying to share a space with them, and my husband was working-from-home… Space-wise, one was needing to work on the dining room table and I needed to work on the computer in the corner of the dining room, was tricky because whenever the phone rang, I had to run to another room and either shut myself in the living room for confidentiality or in my bedroom.(P15)
3.2. Collegial Support
3.2.1. Double Bubble
We’re a small enough team as it is and having to split, we’re so used to working together as a team, and being a small team, one person that’s away can throw the rest of the team’s work, especially if there are issues with clients.(P33)
You kind of feel lost without having that instant team interaction like someone sitting next to you or you’d just be able to walk down the hallway and ask for help… so you do feel isolated.(P13)
There was some lack of equity really because my colleagues although they were working week on and week off, they were obliged to go out into the community and have potentially infectious contact with people on a regular basis every day and I didn’t have to do that.(P14)
3.2.2. Corridor Consultations
Hallway discussions are actually quite important. Many a time I’ve ran a discussion that’s turned into more of… a mini-MDT [multidisciplinary team], organically happens… those office discussions that are often valuable which we didn’t have with COVID.(P3)
To be accessible and that you can access colleagues for professional meetings in an easier way… as a supportive communication within the professional field, definitely a must. Parts I like are screen sharing, for a lot of discussions, it’s becoming an absolutely vital tool. Talking about data, talking about information sharing, developing ideas.(P19)
3.2.3. Supervision
If there was some sort of buddy system where people are encouraged to match up with somebody or have a smaller group and do that, that would be really cool. Yeah, maybe EAP [employee assistance programme] but a bit more casual.(P21)
During the lockdown, you were able to contact me on other days rather than just when we were seeing each other face to face, so I think in some ways it was an advantage. In some ways, it improved access because the medium of communication was technology and there was less of a barrier.(P17)
We got quite a bit of information from that OCE (observed clinical examination) about that [client]… I think as a consultant, because of the on-call situation, I’m used to being on the phone… Zoom was kind of an added bonus because we could see each other.(P17)
3.3. Maintaining Wellbeing
3.3.1. Balancing Risks
I did go in and see somebody face-to-face at the hospital, they weren’t socially distancing, they weren’t wearing masks. And at that point, we thought every surface had COVID on it.(P12)
I was kind of worried that we weren’t going to be able to keep safe and make adequate assessments… I think masking, when you’re seeing people face-to-face, is difficult, because you’re not showing your expression and they’re not showing their expression if they have a mask on.(P12)
3.3.2. Healthy Practices
I was able to get out more, so I thought that that was nice to have that mix of work and getting some fresh air because you could still go for a walk… It felt like it kept my sanity a bit more intact. Because, for me, I lose focus quite easily, so the stopping and starting and coming back and focusing for shorter periods of time is pretty effective.(P28)
We were really surprised at how fatigued we got doing Zoom. It was really, really tiring… because you are focused on a small screen and also it’s very intense. You’re having to be on the whole time because you’re in front of a camera so you can’t be doing things… I think it might be that having to concentrate a lot more and having to listen to multiple people.(P1)
It’s definitely much nicer being back and seeing clients face-to-face. That’s why I’m in this job. Not seeing people face to face certainly does take something away. I guess that’s why we do the job that we do because that’s what we enjoy.(P26)
3.3.3. Māori Cultural Safety
It was that knee-jerk reaction… but especially here as a kaupapa (Māori knowledge and values) service, it was really hard… on our energy and our mauri and our wairua.(P8)
When things are down it’s important for myself and our kaumātua to jump in and support our kaimahi because we know in this mahi (work), burnout is so intense, it’s so high. It’s again, replenishing our mauri and reinforcing that.(P11)
There’s no aroha (love)… we hug people. We let people cry, we cry with them. It’s not the same connection, there’s no connection over the phone that there is when you see people.(P10)
Every morning [we started] with a karakia together as a team. Then I introduced what we called a mauri session… Mauri is one of the components of wellness within our workspace… Tikanga [customary practice] wasn’t just about looking at a Māori paradigm, it was about [implementing] the tikanga here for the whare [house].(P11)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hale, T.; Sam, W.; Anna, P.; Toby, P.; Beatriz, K. Oxford COVID-19 Government Response Tracker; Blavatnik School of Government: Oxford, UK, 2022.
- New Zealand Government. New Zealand COVID-19 Alert Levels Summary. Available online: https://covid19.govt.nz/about-our-covid-19-response/history-of-the-covid-19-alert-system/#printable-resources (accessed on 1 December 2022).
- Bell, C.; Williman, J.; Beaglehole, B.; Stanley, J.; Jenkins, M.; Gendall, P.; Rapsey, C.; Every-Palmer, S. Psychological distress, loneliness, alcohol use and suicidality in New Zealanders with mental illness during a strict COVID-19 lockdown. Aust. N. Z. J. Psychiatry 2021, 56, 800–810. [Google Scholar] [CrossRef] [PubMed]
- Every-Palmer, S.; Jenkins, M.; Gendall, P.; Hoek, J.; Beaglehole, B.; Bell, C.; Williman, J.; Rapsey, C.; Stanley, J. Psychological distress, anxiety, family violence, suicidality, and wellbeing in New Zealand during the COVID-19 lockdown: A cross-sectional study. PLoS ONE 2020, 15, e0241658. [Google Scholar] [CrossRef] [PubMed]
- Officer, T.N.; Imlach, F.; McKinlay, E.; Kennedy, J.; Pledger, M.; Russell, L.; Churchward, M.; Cumming, J.; McBride-Henry, K. COVID-19 pandemic lockdown and wellbeing: Experiences from Aotearoa New Zealand in 2020. Int. J. Environ. Res. Public Health 2022, 19, 2269. [Google Scholar] [CrossRef] [PubMed]
- Sibley, C.G.; Greaves, L.M.; Satherley, N.; Wilson, M.S.; Overall, N.C.; Lee, C.H.J.; Milojev, P.; Bulbulia, J.; Osborne, D.; Milfont, T.L.; et al. Effects of the COVID-19 pandemic and nationwide lockdown on trust, attitudes toward government, and well-being. Am. Psychol. 2020, 75, 618–630. [Google Scholar] [CrossRef] [PubMed]
- Prickett, K.C.; Fletcher, M.; Chapple, S.; Doan, N.; Smith, C. Life in Lockdown: The Economic and Social Effect of Lockdown during Alert Level 4 in New Zealand; Victoria University of Wellington: Wellington, New Zealand, 2020. [Google Scholar]
- Tanielu, R.; Ika, A. The State of Our Communities 2020; SPPU: Auckland, New Zealand, 2020. [Google Scholar]
- Druss, B.G.; Cohen, A.N.; Brister, T.; Cotes, R.O.; Hendry, P.; Rolin, D.; Torous, J.; Ventura, J.; Gorrindo, T. Supporting the mental health workforce during and after COVID-19. Psychiatr. Serv. 2021, 72, 1222–1224. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Salazar de Pablo, G.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Arpacioglu, S.; Gurler, M.; Cakiroglu, S. Secondary traumatization outcomes and associated factors among the health care workers exposed to the COVID-19. Int. J. Soc. Psychiatry 2021, 67, 84–89. [Google Scholar] [CrossRef]
- Holroyd, E.; Long, N.J.; Appleton, N.S.; Davies, S.G.; Deckert, A.; Fehoko, E.; Laws, M.; Martin-Anatias, N.; Simpson, N.; Sterling, R.; et al. Community healthcare workers’ experiences during and after COVID-19 lockdown: A qualitative study from Aotearoa New Zealand. Health Soc. Care Community 2022, 30, e2761–e2771. [Google Scholar] [CrossRef]
- Ministry of Health. Office of the Director of Mental Health and Addiction Services: Annual Report 2017; Ministry of Health: Wellington, New Zealand, 2019.
- Adams, R.; Ryan, T.; Wood, E. Understanding the factors that affect retention within the mental health nursing workforce: A systematic review and thematic synthesis. Int. J. Ment. Health Nurs. 2021, 30, 1476–1497. [Google Scholar] [CrossRef]
- New Zealand Government. He Ara Oranga: Report of the Government Inquiry into Mental Health and Addiction; New Zealand Government: Wellington, New Zealand, 2018.
- Te Pou o te Whakaaro Nui. DHB Mental Health and Addiction Employees: 2019 Profile; Te Pou o te Whakaaro Nui: Auckland, New Zealand, 2020.
- Young, D. Turnover and retention strategies among mental health workers. Fortune J. Health Sci. 2022, 5, 352–362. [Google Scholar] [CrossRef]
- Goetter, E.M.; Iaccarino, M.A.; Tanev, K.S.; Furbish, K.E.; Xu, B.; Faust, K.A. Telemental health uptake in an outpatient clinic for veterans during the COVID-19 pandemic and assessment of patient and provider attitudes. Prof. Psychol. Res. Pract. 2022, 53, 151–159. [Google Scholar] [CrossRef]
- Ministry of Health. Wai 2575 Māori Health Trends Report; Ministry of Health: Wellington, New Zealand, 2019.
- Ministry of Health. Wai 2575 Health Services and Outcomes Kaupapa Inquiry; Ministry of Health, New Zealand: Wellington, New Zealand, 2020.
- Te Pou o te Whakaaro Nui. Workforce Stocktake; Department of Internal Affairs: Wellington, New Zealand, 2018.
- Ministry of Health. Mental Health and Addiction: Service Use Web Tool. Available online: https://www.tewhatuora.govt.nz/our-health-system/data-and-statistics/mental-health-and-addiction-service-use-web-tool/ (accessed on 12 January 2023).
- Thorne, S.; Kirkham, S.R.; MacDonald-Emes, J. Interpretive description: A noncategorical qualitative alternative for developing nursing knowledge. Res. Nurs. Health 1997, 20, 169–177. [Google Scholar] [CrossRef]
- Thorne, S. Interpretive Description, 1st ed.; Left Coast Press: Walnut Creek, CA, USA, 2008. [Google Scholar]
- Thorne, S. Interpretive Description: Qualitative Research for Applied Practice, 2nd ed.; Taylor & Francis: Oxfordshire, UK, 2016. [Google Scholar]
- Matthews, B.; Ross, L. Research Methods: A practical Guide for the Social Sciences; Pearson Longman: London, UK, 2010. [Google Scholar]
- Patton, M.Q. Qualitative Research & Evaluation Methods; SAGE Publications: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Traditions; Sage Publications, Inc: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Ministry of Health. Te Tiriti o Waitangi. Available online: https://www.health.govt.nz/our-work/populations/maori-health/te-tiriti-o-waitangi (accessed on 7 November 2022).
- Sibeoni, J.; Manolios, E.; Costa-Drolon, E.; Meunier, J.-P.; Verneuil, L.; Revah-Levy, A. Clinical practice during the COVID-19 pandemic: A qualitative study among child and adolescent psychiatrists across the world. Child Adolesc. Psychiatry Ment. Health 2021, 15, 68. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak, 18 March 2020; World Health Organization: Geneva, Switzerland, 2020.
- Fegert, J.; Vitiello, B.; Plener, P.; Clemens, V. Challenges and burden of the Coronavirus 2019 (COVID-19) pandemic for child and adolescent mental health: A narrative review to highlight clinical and research needs in the acute phase and the long return to normality. Child Adolesc. Psychiatry Ment. Health 2020, 14, 20. [Google Scholar] [CrossRef]
- Dwyer, A.J. Medical managers in contemporary healthcare organisations: A consideration of the literature. Aust. Health Rev. 2010, 34, 514–522. [Google Scholar] [CrossRef]
- Callaly, T.; Minas, H. Reflections on clinician leadership and management in mental health. Australas. Psychiatry 2005, 13, 27–32. [Google Scholar] [CrossRef]
- Simpson, S.; Richardson, L.; Pietrabissa, G.; Castelnuovo, G.; Reid, C. Videotherapy and therapeutic alliance in the age of COVID-19. Clin. Psychol. Psychother. 2021, 28, 409–421. [Google Scholar] [CrossRef] [PubMed]
- Sunjaya, A.P.; Chris, A.; Novianti, D. Efficacy, patient-doctor relationship, costs and benefits of utilizing telepsychiatry for the management of post-traumatic stress disorder (PTSD): A systematic review. Trends Psychiatry Psychother. 2020, 42, 102–110. [Google Scholar] [CrossRef]
- Sheather, J.; Slattery, D. The great resignation—How do we support and retain staff already stretched to their limit? BMJ 2021, 375, n2533. [Google Scholar] [CrossRef]
- Pavlova, A.; Paine, S.-J.; Sinclair, S.; O′Callaghan, A.; Consedine, N. Working in values-discrepant environments inhibits clinicians ability to provide compassion and reduces wellbeing: A cross-sectional study. medRxiv 2022, preprint. [Google Scholar] [CrossRef]
- Browne, D.; Roy, S.; Phillips, M.; Shamon, S.; Stephenson, M. Supporting patient and clinician mental health during COVID-19: Via trauma-informed interdisciplinary systems. Can. Fam. Physician 2020, 66, e190–e192. [Google Scholar] [PubMed]
- Snowdon, D.A.; Sargent, M.; Williams, C.M.; Maloney, S.; Caspers, K.; Taylor, N.F. Effective clinical supervision of allied health professionals: A mixed methods study. BMC Health Serv. Res. 2019, 20, 2. [Google Scholar] [CrossRef]
- McLeod, M.; Gurney, J.; Harris, R.; Cormack, D.; King, P. COVID-19: We must not forget about indigenous health and equity. Aust. N. Z. J. Public Health 2020, 44, 253. [Google Scholar] [CrossRef] [PubMed]
- New Zealand Government. Royal Commission of Inquiry (COVID-19 Lessons) Order 2022 (2022/323). Available online: https://www.parliament.nz/en/pb/papers-presented/current-papers/document/PAP_130228/royal-commission-of-inquiry-covid-19-lessons-order-2022 (accessed on 12 January 2023).
- Ministry of Health. Mental Health and Addiction Services Data: Calculating Waiting Times; Ministry of Health: Wellington, New Zealand, 2021.
- Ministry of Health. Office of the Director of Mental Health and Addiction Services Annual Report 2018 and 2019; Ministry of Health: Wellington, New Zealand, 2021.

{kind=link}
{kind=link}
| Role | Ethnicity | Age Range | Gender | ||||
|---|---|---|---|---|---|---|---|
| Doctor | 7 | Māori | 5 | 25–35 years | 6 | Male | 10 |
| Nurse | 6 | NZ European | 18 | 35–44 years | 6 | Female | 23 |
| Clinical psychologist | 5 | Other European | 4 | 45–54 years | 10 | ||
| Team leader | 5 | Pacific | 2 | 55–65 years | 6 | ||
| Social worker | 4 | Other | 4 | 65+ years | 5 | ||
| Occupational therapist | 2 | ||||||
| Kaumātua | 1 | ||||||
| Cultural therapist | 1 | ||||||
| Psychotherapist | 1 | ||||||
| Case manager | 1 | ||||||
| Total | 33 | Total | 33 | Total | 33 | Total | 33 |
| Outpatient Teams | Health System Management |
|---|---|
| Address disparate access to basic resources (PPE, desks, chairs, and suitable work computers). | Include clinician stakeholders in service planning and policy making. |
| Develop best practice guidelines for creating safe spaces and boundaries to conduct work at home. | Improve communication between senior management and health professionals. |
| Foster relationships with local communities to support ongoing connection with (Māori and non-Māori) clients. | Establish monitored disaster relief locum pools. |
| Develop collegial support and supervision networks. | Improve cultural safety through consulting with Māori stakeholders. |
| Include protected time for clinicians to provide peer support, mentoring, and formal supervision. | Implement and review policies for monitoring clinician well-being during pandemics or as part of emergency management. |
| Create supervision protocols for occupational therapists, social workers, and case managers. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Werkmeister, B.J.; Haase, A.M.; Fleming, T.; Officer, T.N. Experiences of the COVID-19 Lockdown and Telehealth in Aotearoa New Zealand: Lessons and Insights from Mental Health Clinicians. Int. J. Environ. Res. Public Health 2023, 20, 4791. https://doi.org/10.3390/ijerph20064791
Werkmeister BJ, Haase AM, Fleming T, Officer TN. Experiences of the COVID-19 Lockdown and Telehealth in Aotearoa New Zealand: Lessons and Insights from Mental Health Clinicians. International Journal of Environmental Research and Public Health. 2023; 20(6):4791. https://doi.org/10.3390/ijerph20064791
Chicago/Turabian StyleWerkmeister, Benjamin J., Anne M. Haase, Theresa Fleming, and Tara N. Officer. 2023. "Experiences of the COVID-19 Lockdown and Telehealth in Aotearoa New Zealand: Lessons and Insights from Mental Health Clinicians" International Journal of Environmental Research and Public Health 20, no. 6: 4791. https://doi.org/10.3390/ijerph20064791
APA StyleWerkmeister, B. J., Haase, A. M., Fleming, T., & Officer, T. N. (2023). Experiences of the COVID-19 Lockdown and Telehealth in Aotearoa New Zealand: Lessons and Insights from Mental Health Clinicians. International Journal of Environmental Research and Public Health, 20(6), 4791. https://doi.org/10.3390/ijerph20064791