

Proposal of a New Rating Concept for Digital Health Applications in Orthopedics and Traumatology

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Setting
2.2. Pilot Validation
- Sprunggelenks-App (“Ankle-Joint-App”), Mediploy GmBH, 40764 Langenfeld, Germany.
- Therapie-App (“Therapy app”), Bauerfeind®, 07937 Zeulenroda-Triebes, Germany.
2.3. Recommendations for Orthopedic Societies
2.4. Justification of Methods Used
3. Results
3.1. Self-Declaration Sheet
3.2. Society Evaluation Sheet
3.3. Pilot Validation
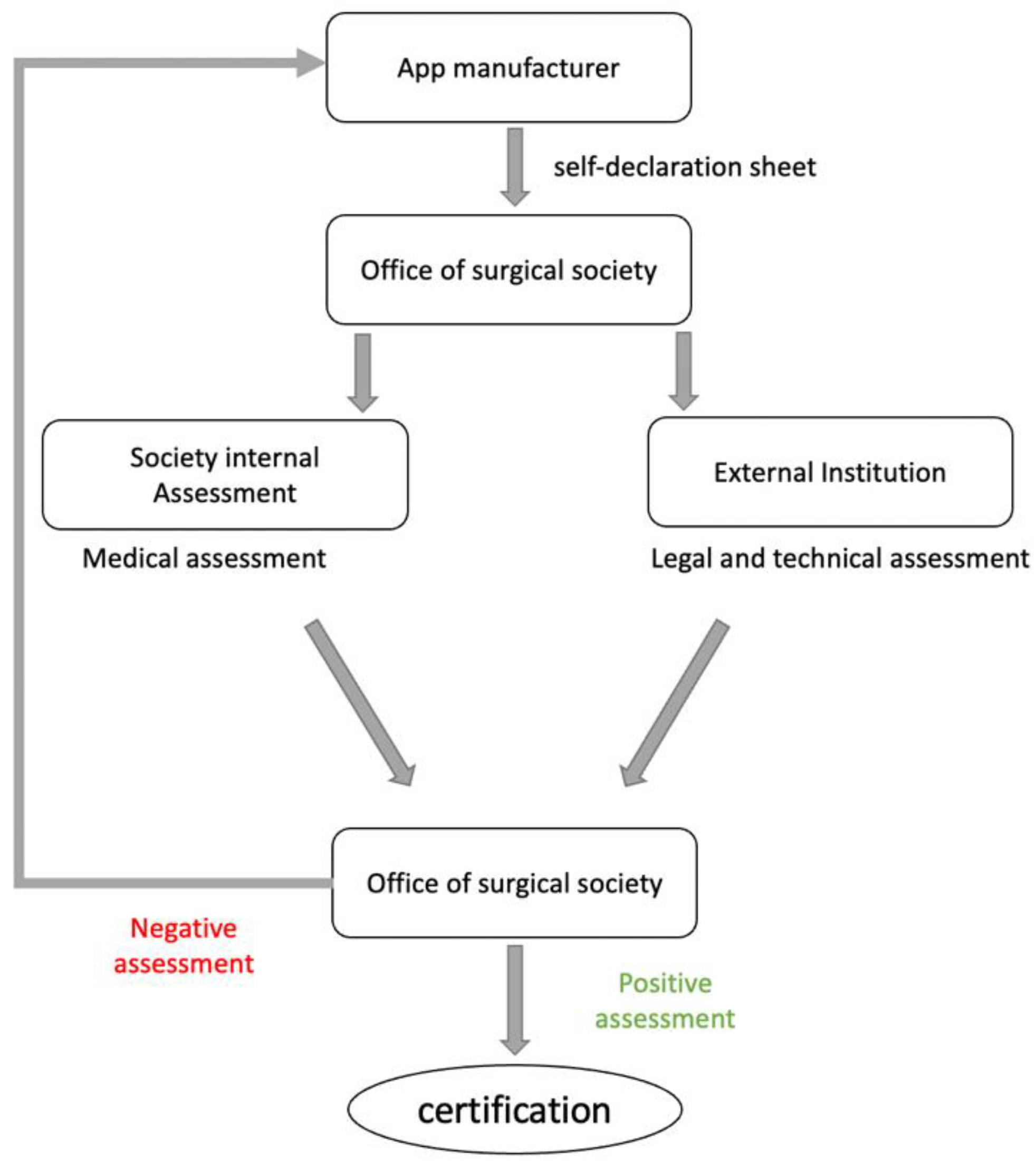
3.4. Proposal for Society Assessment
3.5. Practical Implications
- The initial reviewing process takes 2–3 h.
- In case of uncertainties and the need to contact the manufacturer, the initial reviewing process can be significantly prolonged.
- A coordinator between the society and the reviewer should be chosen for an initial briefing regarding the process.
- An external institution must review the legal and technical requirements of the apps. Apparent violations of legal and technical requirements would, therefore, already lead to the exclusion of the app from the rating process, even before the professional content assessment.
- Financial compensation for coordinators and reviewers should be considered to maintain a general willingness to review proposed health applications. We suggest that the individual manufacturer covers this.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krebs, P.; Duncan, D.T. Health App Use Among US Mobile Phone Owners: A National Survey. JMIR Mhealth Uhealth 2015, 3, e4924. [Google Scholar] [CrossRef] [PubMed]
- Wongworawat, M.D.; Capistrant, G.; Stephenson, J.M. The Opportunity Awaits to Lead Orthopaedic Telehealth Innovation: AOA Critical Issues. J. Bone Jt. Surg. Am. 2017, 99, e93. [Google Scholar] [CrossRef] [PubMed]
- Ashfaq, A.; Esmaili, S.; Najjar, M.; Batool, F.; Mukatash, T.; Al-Ani, H.A.; Koga, P.M. Utilization of Mobile Mental Health Services among Syrian Refugees and Other Vulnerable Arab Populations—A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 1295. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030; World Health Organization: Geneva, Switzerland, 2016.
- Higgins, J.P. Smartphone Applications for Patients’ Health and Fitness. Am. J. Med. 2016, 129, 11–19. [Google Scholar] [CrossRef]
- Statista. Number of mHealth Apps Available in the Google Play Store from 1st Quarter 2015 to 2nd Quarter 2022. online2022. Available online: https://www.statista.com/statistics/779919/health-apps-available-google-play-worldwide/ (accessed on 12 October 2022).
- Albrecht, U.V.; Hillebrand, U.; von Jan, U. Relevance of Trust Marks and CE Labels in German-Language Store Descriptions of Health Apps: Analysis. JMIR Mhealth Uhealth 2018, 6, e10394. [Google Scholar] [CrossRef] [PubMed]
- Henson, P.; David, G.; Albright, K.; Torous, J. Deriving a practical framework for the evaluation of health apps. Lancet Digit. Health 2019, 1, e52–e54. [Google Scholar] [CrossRef]
- Wyatt, J.C. How can clinicians, specialty societies and others evaluate and improve the quality of apps for patient use? BMC Med. 2018, 16, 225. [Google Scholar] [CrossRef]
- Singh, K.; Drouin, K.; Newmark, L.P.; Lee, J.; Faxvaag, A.; Rozenblum, R.; Pabo, E.A.; Landman, A.; Klinger, E.; Bates, D.W. Many Mobile Health Apps Target High-Need, High-Cost Populations, But Gaps Remain. Health Aff. 2016, 35, 2310–2318. [Google Scholar] [CrossRef]
- McMillan, B.; Hickey, E.; Mitchell, C.; Patel, M. The need for quality assurance of health apps. BMJ Br. Med. J. 2015, 351, h5915. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Torous, J.; Nicholas, J.; Larsen, M.E.; Firth, J.; Christensen, H. Clinical review of user engagement with mental health smartphone apps: Evidence, theory and improvements. Evid. Based Ment. Health 2018, 21, 116–119. [Google Scholar] [CrossRef]
- Lewis, T.L.; Wyatt, J.C. mHealth and mobile medical Apps: A framework to assess risk and promote safer use. J. Med. Internet Res. 2014, 16, e210. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.E.; Davenport, T.A.; Wong, T.; Moon, H.-W.; Hickie, I.B.; LaMonica, H.M. Evaluating the quality and safety of health-related apps and e-tools: Adapting the Mobile App Rating Scale and developing a quality assurance protocol. Internet Interv. 2021, 24, 100379. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, U.V.; Malinka, C.; Long, S.; Raupach, T.; Hasenfuss, G.; von Jan, U. Quality Principles of App Description Texts and Their Significance in Deciding to Use Health Apps as Assessed by Medical Students: Survey Study. JMIR Mhealth Uhealth 2019, 7, e13375. [Google Scholar] [CrossRef] [PubMed]
- Malinka, C.; von Jan, U.; Albrecht, U.V. Prioritization of Quality Principles for Health Apps Using the Kano Model: Survey Study. JMIR Mhealth Uhealth 2022, 10, e26563. [Google Scholar] [CrossRef] [PubMed]
- Nouri, R.; R Niakan Kalhori, S.; Ghazisaeedi, M.; Marchand, G.; Yasini, M. Criteria for assessing the quality of mHealth apps: A systematic review. J. Am. Med. Inform. Assoc. 2018, 25, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Bundesministerium für Gesundheit. Ärzte Sollen Apps Verschreiben Können Gesetz für eine Bessere Versorgung durch Digitalisierung und Innovation (Digitale-Versorgung-Gesetz—DVG). 2019. Available online: https://www.bundesgesundheitsministerium.de/digitale-versorgung-gesetz.html#:~:text=Apps%20auf%20Rezept%2C%20Videosprechstunden%20einfach,2019%20in%20Kraft%20getreten%20ist (accessed on 1 August 2022).
- Bundesministerium für Gesundheit. Gesetzentwurf der Bundesregierung Entwurf eines Gesetzes für eine Bessere Versorgung durch Digitalisierung und Innovation (Digitale-Versorgung-Gesetz—DVG). 2019. Available online: https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/3_Downloads/Gesetze_und_Verordnungen/GuV/D/Digitale-Versorgung-Gesetz_DVG_Kabinett.pdf (accessed on 1 August 2022).
- Bundesgesetzblatt. Gesetz für eine Bessere Versorgung durch Digitalisierung und Innovation (Digitale-Versorgung-Gesetz) Vom 09. Dezember 2019. Bundesgesetzblatt Jahrgang 2019 Teil 1 Nr. 49: Bundesanzeiger Verlag GmbH. 2019. Available online: https://dejure.org/BGBl/2019/BGBl._I_S._2562 (accessed on 1 August 2022).
- EndoCert GmbH. Das Weltweit Erste Zertifizierungssystem in der Endoprothetik; 2020. Available online: https://endocert.de/?view=article&id=12:das-weltweit-erste-zertifizierungssystem-in-der-endoprothetik&catid=14 (accessed on 1 August 2022).
- KTQ-GmbH. Kooperation für Transparenz und Qualität im Gesundheitswesen GmbH; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- NHS. NHS Apps Library; NHS: London, UK, 2019.
- DIA Event und Promotion GmbH. DiaDigital; DIA Event und Promotion GmbH: Berlin, Germany, 2020. [Google Scholar]
- Johannes Bittner, T.T. AppQ: Gütekriterien-Kernset für mehr Transparenz bei Digitalen Gesundheitsanwendungen; 2019. Available online: https://www.bertelsmann-stiftung.de/de/unsere-projekte/der-digitale-patient/projektnachrichten/appq/ (accessed on 1 August 2022).
- Messner, E.M.; Terhorst, Y.; Barke, A.; Baumeister, H.; Stoyanov, S.; Hides, L.; Kavanagh, D.; Pryss, R.; Sander, L.; Probst, T. Development and Validation of the German Version of the Mobile Application Rating Scale (MARS-G). JMIR Mhealth Uhealth 2020, 8, e14479. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Tjondronegoro, D.; Mani, M. Mobile app rating scale: A new tool for assessing the quality of health mobile apps. JMIR Mhealth Uhealth 2015, 3, e27. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, U.-V. APP-SYNOPSIS—USER-DEUTSCHE VERSION. Available online: http://www.app-synopsis.de (accessed on 1 August 2022).
- Albrecht, U.-V. Einheitlicher Kriterienkatalog zur Selbstdeklaration der Qualität von Gesundheits-Apps; Version 1.2 vom 22.06.2019 ed: Ehealth Suisse. 2019. Available online: https://www.researchgate.net/publication/334192980_Einheitlicher_Kriterienkatalog_zur_Selbstdeklaration_der_Qualitat_von_Gesundheits-Apps (accessed on 1 August 2022).
- Datillo, J.R.; Gittings, D.J.; Sloan, M.; Hardaker, W.M.; Deasey, M.J.; Sheth, N.P. “Is There An App For That?” Orthopaedic Patient Preferences For A Smartphone Application. Appl. Clin. Inform. 2017, 8, 832–844. [Google Scholar] [CrossRef]
- Scherer, J.; Keller, F.; Pape, H.-C.; Osterhoff, G. Would patients undergo postoperative follow-up by using a smartphone application? BMC Surg. 2020, 20, 229. [Google Scholar] [CrossRef]
- Scherer, J.; Osterhoff, G.; Kaufmann, E.; Estel, K.; Neuhaus, V.; Willy, C.; Hepp, P.; Pape, H.; Back, D.A. What is the acceptance of video consultations among orthopedic and trauma outpatients? A multi-center survey in 780 outpatients. Injury 2021, 52, 3304–3308. [Google Scholar] [CrossRef]
- Toelle, T.R.; Utpadel-Fischler, D.A.; Haas, K.-K.; Priebe, J.A. App-based multidisciplinary back pain treatment versus combined physiotherapy plus online education: A randomized controlled trial. NPJ Digit. Med. 2019, 2, 34. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.J.; Robertson, G.A.; Connor, K.L.; Brady, R.R.; Wood, A.M. Smartphone apps for orthopaedic sports medicine—A smart move? BMC Sports Sci. Med. Rehabil. 2015, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, U.V.; Framke, T.; von Jan, U. Quality Awareness and Its Influence on the Evaluation of App Meta-Information by Physicians: Validation Study. JMIR Mhealth Uhealth 2019, 7, e16442. [Google Scholar] [CrossRef]
- Airaksinen, N.K.; Nurmi-Luthje, I.S.; Kataja, J.M.; Kroger, H.P.J.; Luthje, P.M.J. Cycling injuries and alcohol. Injury 2018, 49, 945–952. [Google Scholar] [CrossRef]
- Han, M.; Lee, E. Effectiveness of Mobile Health Application Use to Improve Health Behavior Changes: A Systematic Review of Randomized Controlled Trials. Healthc. Inf. Res. 2018, 24, 207–226. [Google Scholar] [CrossRef] [PubMed]
- Tangari, G.; Ikram, M.; Sentana, I.W.B.; Ijaz, K.; Kaafar, M.A.; Berkovsky, S. Analyzing security issues of android mobile health and medical applications. J. Am. Med. Inform. Assoc. 2021, 28, 2074–2084. [Google Scholar] [CrossRef]
- Mahmood, A.; Kedia, S.; Wyant, D.K.; Ahn, S.; Bhuyan, S.S. Use of mobile health applications for health-promoting behavior among individuals with chronic medical conditions. Digit. Health 2019, 5, 2055207619882181. [Google Scholar] [CrossRef]
- de Chantal, P.L.; Chagnon, A.; Cardinal, M.; Faieta, J.; Guertin, A. Evidence of User-Expert Gaps in Health App Ratings and Implications for Practice. Front. Digit. Health 2022, 4, 765993. [Google Scholar] [CrossRef]
- Handel, M.J. mHealth (Mobile Health)—Using Apps for Health and Wellness. Explore 2011, 7, 256–261. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Wilson, H. Development and Validation of the User Version of the Mobile Application Rating Scale (uMARS). JMIR Mhealth Uhealth 2016, 4, e72. [Google Scholar] [CrossRef]
- Nichols, D.G. Maintenance of Certification and the Challenge of Professionalism. Pediatrics 2017, 139, e20164371. [Google Scholar] [CrossRef] [PubMed]
- Bentley, D. CE marking—What does it really mean? J. Tissue Viability 1999, 9, 11–15. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. | Quality Principle | Explanation |
|---|---|---|
| I | Transparency | Valid, reliable and target-group-specific information is available on the quality requirements that the health app and underlying software meet to support their evaluation as well as individual and collective usage decisions. |
| II | Practicality | The health app is suitable for the intended purpose and opens corresponding areas of application and context. Proof of fulfilling the stated purpose, i.e., the benefit, is provided using appropriate methods. It is also clearly recognizable for which purpose and user group the health app is unsuitable. |
| III | Risk adequacy | The health app can be used without exposing the user or his environment to disproportionate health, social or economic risk. Appropriate methods are chosen to demonstrate the relationship between the benefits and the risks. The manufacturer takes precautions to rule out risks of use as far as possible. |
| IV | Ethical soundness | The health app is ethically sound regarding development, distribution, operation and use (e.g., concerning professional and/or research ethics). Discrimination and stigmatization of users are avoided. |
| V | Legal conformity | The health app is legally compliant (including medical device law, professional law and data protection law). Legal compliance is guaranteed with respect to development, distribution, operation and use. |
| VI | Content validity | The health-related content used and presented in the health app is up to date, valid and trustworthy. The manufacturer ensures that the content is regularly updated in a manner that is recognizable to the user and is up to date with the latest knowledge and regulatory requirements. |
| VII | Technical adequacy | The health app is state of the art regarding development, operation, maintenance and use and guarantees sustainability in the sense of maintainability, portability, interoperability and compatibility. |
| VIII | Usability | The health app enables target-group-specific use (e.g., in terms of accessibility and individualization). In addition, there is the possibility of contacting the manufacturer and/or other affected persons or health professionals if anything is unclear. |
| IX | Resource efficiency | The health app is resource efficient to use (e.g., in terms of power consumption, computing power, memory, data transfer, time and costs). |
| No. | Quality Principle | Basic Requirements for Self-Declaration |
|---|---|---|
| 1 | Transparency | The self-declaration must provide information about the app in accordance with the “transparency” quality principle to be sufficient as a basis for individual and collective usage decisions and evaluations of the software. |
| (A) Completeness of the information | ||
| No. | Questions and manufacturer information | |
| A1 | Name of the application | |
| A2 | Version of the application and date of upload/update | |
| A3 | Costs for the user | |
| A4 | On which operational systems can the app be used? (URLs) | |
| A5 | Provide manufacturer’s name and contact details | |
| A6 | Describe the financing model (e.g., adverts, in-app purchases) | |
| 2 | Expediency | The self-declaration for the quality principle “Expediency” should show the extent to which the software is appropriate for the intended purpose. |
| (A) Intended use | ||
| (B) Purpose fulfillment (C) Evidence or information on the fulfillment of the purpose / suitability | ||
| No. | Questions and manufacturer information | |
| A1 | Give a short description of your app (approx. 100 words) that clearly shows the purpose and the goals (target groups of your app, limitations or limits of the app use?): | |
| B1 | With which technical functions or content-related methods contained in your app (e.g., implementation of scores, training plans, etc.) do you ensure that the goal of your app is achieved? | |
| B2 | Does your app process data or user information? If so, please specify these functions: | |
| C1 | Can you provide data to prove that your app achieves the purpose to be fulfilled? If so, please provide specific sources: | |
| 3 | Appropriateness of Risk | The self-declaration for the quality principle “risk appropriateness” should show the extent to which the app can be used in a risk-appropriate manner without exposing the user or his environment to a disproportionate health, social or economic risk. |
| (A) Risk awareness (B) Risk management | ||
| No. | Questions and manufacturer information | |
| A1 | Do you see potential or actual economic, social or health risks when using your app? | |
| A2 | Is there a risk or the danger of a third party being endangered by using the app? | |
| B1 | What measures have you taken to exclude or minimize risks and dangers that (could) arise from using the app? | |
| B2 | Have you set up a risk management system (in case problems / risks for users should arise)? If so, which? | |
| 4 | Ethical Clearance | The self-declaration on the quality principle “ethical harmlessness” should show the extent to which development, supply, operation and use are ethically harmless in order to prevent discrimination and stigmatization and to enable fair access. |
| (A) Compliance with ethical principles (B) Disclosure of Conflicts of Interest (C) Good scientific practice | ||
| No. | Questions and manufacturer information | |
| A1 | Before the download (homepage / store description), will the end users of your app receive clear, understandable information on purpose description, data processing (data protection provisions), conditions of use (EULA) and financing? | |
| A2 | Can every end user use the app equally? What are the usage hurdles (e.g., technical understanding required)? | |
| B1 | Is advertising used in your app? Is this also clearly recognizable as advertising for the end user? | |
| B2 | Is there a conflict of interest (e.g., has the sponsorship influenced the content of the app, etc.)? | |
| C1 | Is your app being used in a scientific context? If so, does it comply with the principles of good scientific practice and is there a valid vote from the responsible ethics committee? | |
| 5 | Legal Conformity | The self-declaration for the quality principle “legal conformity” should show the extent to which legal conformity (including medical device law, professional law, data protection law) of development, offer, operation and use is guaranteed to protect all parties involved (e.g., providers, store operators, users). |
| (A) General (e.g., data protection) (B) Health related (e.g., medical device law) | ||
| No. | Questions and manufacturer information | |
| A1 | Is your app GDPR (General Data Protection Regulation) compliant? Do end users have to actively consent to the collection of personal data and are they named? | |
| A2 | For what purposes are the collected data used? Do you process the data and, if necessary, pass on collected user-associated data to third parties? Are users informed about this? | |
| A3 | Where is the geographic location of the server on which the app or the collected data is stored? Are the data on the server protected from unauthorized access by third parties? | |
| B1 | If your app falls under the Medical Devices Act (if applicable), please indicate the associated class (justification): | |
| B2 | Does your app have the current CE certification, and does it meet all of the relevant regulations for its class? | |
| 6 | Content Validity | The self-declaration for the quality principle “content validity” should show the extent to which the health-related content presented and used is valid and trustworthy. |
| (A) Valid sources (B) Topicality of the content | ||
| No. | Questions and manufacturer information | |
| A1 | What sources is the content of your app based on (scientific findings, guidelines, studies)? Are these sources available to the end user? | |
| B1 | How do you technically ensure that the content of your app remains up to date (e.g., when guidelines are updated)? | |
| B2 | Who is responsible for updating the content and, if necessary, checking guidelines or specialist literature after changes? | |
| 7 | Technical Adequacy | The self-declaration for the quality principle “Technical adequacy” should show the extent to which development, operation, maintenance, and use correspond to the state of the art to ensure sustainability in terms of maintainability, interoperability and compatibility. |
| (A) Technical timeliness (B) Platform-independent use, scalability | ||
| No. | Questions and manufacturer information | |
| A1 | How often is your app updated (when was the last update? When are you planning the next?)? | |
| A2 | Do you use a secure and encrypted connection according to the latest technical standards for data transmission? | |
| A3 | How do you ensure that your app remains technically up to date (e.g., when updating operating systems)? Who is responsible? | |
| B1 | Is it possible for the user to transfer the data collected via the app and is this necessary (e.g., when changing the mobile platform or the device used)? | |
| B2 | Does your app interact / communicate with hardware, medical device, homepage, or backend? If yes how? | |
| 8 | Usability | The self-declaration for the quality principle “Usability” is intended to show the extent to which the software enables use according to the target group and contributes to the satisfaction of the user. |
| (A) Proof of usability (B) User involvement | ||
| No. | Questions and manufacturer information | |
| A1 | Can you provide evidence of the usability of your app? Has the app been tested on the target group? | |
| A2 | Can your app be adapted to the needs of a target group (customization, e.g., doctors / patients with regard to content, or patients with certain diseases, magnifying glass function for older people)? | |
| B1 | Have you implemented the option of a feedback function or an error reporting system via your app? | |
| B2 | Are users involved in the app (e.g., the possibility of comparing them with other users, via social media, saving own results for motivation, etc.)? | |
| 9 | Resource Efficiency | The self-declaration for the “Resource Efficiency” quality principle should show the extent to which the app takes resource-efficient use into account. |
| (A) Efficient use of resources | ||
| No. | Questions and manufacturer information | |
| A1 | Is a permanent internet connection necessary for the stable usability of your app after the download? | |
| A2 | How much storage capacity does your app take up on the mobile device? | |
| A3 | How much time does the adequate use of the app take (e.g., per day)? | |
| Reviewer Rating Sheet: | |||
|---|---|---|---|
| Title of the app to be rated: Manufacturer: Costs: Target group: Physician | Patient | Physician and Patient Category: Education/Information | Therapy | Prevention | Research | Other Purpose description (max. 100 words): The self-declaration has been completed in full: Yes / No The manufacturer ensures compliance with the quality criteria in all points: Yes / No Technical evaluation: | |||
| P | MA | Criteria | Fulfilled? |
| Transparency: | |||
| 1 | A2 | Was the update / upload date within the last 2 years? | [yes] [no] [do not know] |
| A4 | App available in Applestore and Google Play Store? | [yes] [no] [do not know] | |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Expediency: | |||
| 2 | A1/2 | Are the purpose and goals of the app clear? | [yes] [no] [do not know] |
| B1 | Do the technical functions that the app uses to fulfill its purpose appear plausible? | [yes] [no] [do not know] | |
| B2 | Do the explanations regarding the data processing appear plausible? | [yes] [no] [do not know] | |
| C1 | Is suitable evidence provided that supports the information on the purpose of the app (e.g., references to studies, guidelines, tests, quality seals)? | [yes] [no] [do not know] | |
| C1/2 | Is any danger for the patient through limitations and exclusion criteria securely excluded? | [yes] [no] [do not know] | |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Appropriateness of Risk: | |||
| 3 | A1/2 | Are relevant potential or actual risks (health, economic, social) for the users or their environment when using the app described? | [yes] [no] [do not know] |
| B1/2 | Have adequate precautions been implemented to avoid health, economic and / or social risks when using the app? | [yes] [no] [do not know] | |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Ethical Clearance: | |||
| 4 | A1/2 | Is the end user adequately and transparently informed about the app before downloading the app and can they use the app equally? | [yes] [no] [do not know] |
| B1/2 | Are there no relevant conflicts of interest (e.g., authors with company participation) or only those that are explained transparently and do not compromise the quality of the app? | [yes] [no] [do not know] | |
| C1 | Is it described whether the app follows the principles of good scientific practice when used in a research context? | [yes] [no] [do not know] | |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Legal Conformity: | |||
| 5 | A1 | Is it described which relevant general legal requirements, such as requirements of data protection law, GDPR, telemedia law or commercial law are considered by the manufacturer / provider of the app and are these complied with? | [yes] [no] [do not know] |
| A2/3 | Are the purposes of the data collection plausible and are they based on a secure concept? | [yes] [no] [do not know] | |
| B1/2 | If the app falls under the MDA, are all regulations met? | [yes] [no] [do not know] | |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Content Validity: | |||
| 6 | A1–3 | Is a plausible concept drawn up as to how the quality of the content is guaranteed (e.g., inclusion of experts in the field) and which valid sources are used (e.g., consideration of current scientific findings, guidelines)? | [yes] [no] [do not know] |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Technical Adequacy: | |||
| 7 | A1–3 | Does the app correspond to the current state of art? | [yes] [no] [do not know] |
| B1 | Is there a concept to what extent it is possible to switch to a different operating system or device without losing data? | [yes] [no] [do not know] | |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Usability: | |||
| 8 | A1 | Can valid proof of usability or target group conformity (e.g., usability tests) be made? | [yes] [no] [do not know] |
| A2 | Can the function of the app be adapted to specific target groups / barrier-free? | [yes] [no] [do not know] | |
| B1 | Can the end user interact or give feedback via the app (e.g., social media, etc.)? | [yes] [no] [do not know] | |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Resource Efficiency: | |||
| 9 | A1–3 | Would you describe the use of the available technical resources (e.g., required memory, computing power, internal or external sensors, power consumption, etc.) as efficient? | [yes] [no] [do not know] |
| Questions answered adequately, an assessment is possible. | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Test quality criteria of the manufacturer’s information: | |||
| Is the information about the app sufficient, i.e., is it adequately given in terms of scope and depth of information? | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Is valid, i.e., complete and reliable, information given about the app? | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Is the information about the app described in a way that is appropriate for the target group? | [yes] [no] [do not know] | ||
| Is the content of the criterion met? | [yes] [no] [do not know] | ||
| Overall evaluation / additional comments: Recommendation for approval: [yes] [no] | |||
| Title | Sprunggelenks-App | Therapie-App |
| Manufacturer | Mediploy GmbH | Bauerfeind® |
| Costs | No costs | No costs |
| Target group | Physicians and patients | Patients |
| Category | Education, Information, Therapy, Prevention | Education/Information, Therapy |
| Purpose description | The purpose of this app is to optimize aftercare of patients with ankle sprains (without bone lesion) using information/education, videos, diary as well as the Cumberland Ankle Instability Tool. | Supportive information and training program for patient who received a Bauerfeind® product |
| Self-declaration completion | Yes | Yes |
| Compliance with quality criteria | Yes | Yes/No |
| Technical evaluation | ||
| Transparency | ||
| A2 | Yes | Yes |
| A4 | Yes | Yes |
| Are questions answered adequately, and is an assessment possible? | Yes | Yes |
| Is the content of the criterion met? | Yes | Yes |
| Expediency | ||
| A1/2 | Yes | N/A (Target is not well defined) |
| B1 | Yes | Yes |
| B2 | Yes | Yes |
| C1 | Yes | N/A (No evidence displayed in the App) |
| C1/2 | Yes | N/A (No limitations displayed) |
| Are questions answered adequately, and is an assessment possible? | Yes | Yes |
| Is the content of the criterion met? | Yes | N/A |
| Appropriateness of Risk: | ||
| A1/2 | Yes | N/A (not displayed) |
| B1/2 | Yes | N/A (not displayed) |
| Are questions answered adequately, and is an assessment possible? | Yes | Yes |
| Is the content of the criterion met? | Yes | N/A |
| Ethical Clearance | ||
| A1/2 | Yes | No |
| B1/2 | Yes | No (App description suggests that the app can only be used in combination with a Bauerfeind® product, but the app itself is a general training program) |
| C1 | Yes | No |
| Are questions answered adequately, and is an assessment possible? | Yes | No |
| Is the content of the criterion met? | Yes | No |
| Legal Conformity | ||
| A1 | Yes | Yes |
| A2/3 | Yes | Yes |
| B1/2 | Yes | Yes |
| Are questions answered adequately, and is an assessment possible? | Yes | Yes |
| Is the content of the criterion met? | Yes | Yes |
| Content Validity | ||
| A1–3 | Yes | Yes |
| Are questions answered adequately, and is an assessment possible? | Yes | Yes |
| Is the content of the criterion met? | Yes | Yes |
| Technical Adequacy | ||
| A1–3 | Yes | Yes |
| B1 | no | Yes |
| Are questions answered adequately, and is an assessment possible? | Yes | Yes |
| Is the content of the criterion met? | Yes | Yes |
| Usability | ||
| A1 | Yes | Yes |
| A2 | Yes | No |
| B1 | Yes | No |
| Are questions answered adequately, and is an assessment possible? | Yes | N/A |
| Is the content of the criterion met? | Yes | N/A |
| Resource Efficiency | ||
| A1–3 | Yes | N/A |
| Are questions answered adequately, and is an assessment possible? | Yes | N/A |
| Is the content of the criterion met? | Yes | N/A |
| Test quality criteria: | ||
| Is the information about the app sufficient? | Yes | Yes (but no references within the app) |
| Is the content of the criterion met? | Yes | Yes |
| Is valid information given about the app? | Yes | Yes (but in-store description not precise) |
| Is the content of the criterion met? | Yes | Yes |
| Is the information about the app appropriate for the target group? | Yes | Yes |
| Is the content of the criterion met? | Yes | Yes |
| Overall evaluation / additional comments: | Overall positive, relevant topic, clear goal definition, technical criteria met, no risk for user | Nice application for therapy of musculoskeletal disorders. Innovative professional approach. Things which should be addressed in the future:
|
| Recommendation for approval: | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scherer, J.; Youssef, Y.; Dittrich, F.; Albrecht, U.-V.; Tsitsilonis, S.; Jung, J.; Pförringer, D.; Landgraeber, S.; Beck, S.; Back, D.A. Proposal of a New Rating Concept for Digital Health Applications in Orthopedics and Traumatology. Int. J. Environ. Res. Public Health 2022, 19, 14952. https://doi.org/10.3390/ijerph192214952
Scherer J, Youssef Y, Dittrich F, Albrecht U-V, Tsitsilonis S, Jung J, Pförringer D, Landgraeber S, Beck S, Back DA. Proposal of a New Rating Concept for Digital Health Applications in Orthopedics and Traumatology. International Journal of Environmental Research and Public Health. 2022; 19(22):14952. https://doi.org/10.3390/ijerph192214952
Chicago/Turabian StyleScherer, Julian, Yasmin Youssef, Florian Dittrich, Urs-Vito Albrecht, Serafeim Tsitsilonis, Jochen Jung, Dominik Pförringer, Stefan Landgraeber, Sascha Beck, and David A. Back. 2022. "Proposal of a New Rating Concept for Digital Health Applications in Orthopedics and Traumatology" International Journal of Environmental Research and Public Health 19, no. 22: 14952. https://doi.org/10.3390/ijerph192214952
APA StyleScherer, J., Youssef, Y., Dittrich, F., Albrecht, U.-V., Tsitsilonis, S., Jung, J., Pförringer, D., Landgraeber, S., Beck, S., & Back, D. A. (2022). Proposal of a New Rating Concept for Digital Health Applications in Orthopedics and Traumatology. International Journal of Environmental Research and Public Health, 19(22), 14952. https://doi.org/10.3390/ijerph192214952