
The Association between Lifestyle Changes and Psychological Distress during COVID-19 Lockdown: The Moderating Role of COVID-Related Stressors

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Measures
2.2.1. Demographic Questionnaire
2.2.2. Lifestyle Changes due to COVID-19
2.2.3. COVID-Related Stressors
2.2.4. Depression, Anxiety, and Stress Scale
2.3. Statistical Analysis
3. Results
3.1. Cohort Description of the Main Research Variables
3.2. The Association between the Nature of Lifestyle Change Due to COVID-19 and Psychological Distress
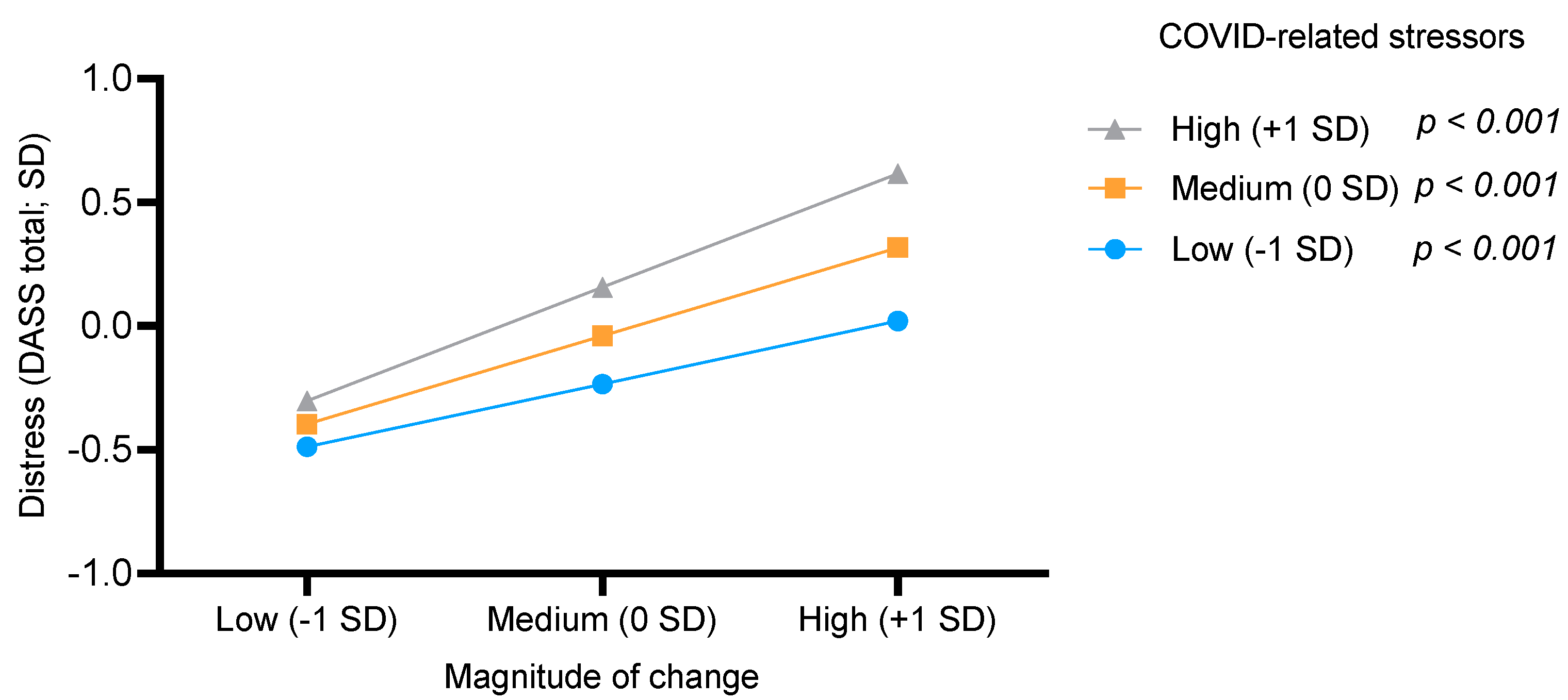
3.3. The Moderating Effect of COVID-Related Stressors on the Association between the Magnitude of Change and Psychological Distress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levy, I.; Cohen-Louck, K.; Herzog, S. Predicting support for community corrections: Crime type and severity, and offender, observer, and victim characteristics. Punishm. Soc. 2021, 1–21. [Google Scholar] [CrossRef]
- Coiro, M.J.; Asraf, K.; Tzischinsky, O.; Hadar-Shoval, D.; Tannous-Haddad, L.; Wolfson, A.R. Sleep quality and COVID-19-related stress in relation to mental health symptoms among Israeli and U.S. adults. Sleep Health 2021, 7, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Rudenstine, S.; McNeal, K.; Schulder, T.; Ettman, C.K.; Hernandez, M.; Gvozdieva, K.; Galea, S. Depression and Anxiety During the COVID-19 Pandemic in an Urban, Low-Income Public University Sample. J. Trauma. Stress 2021, 34, 12–22. [Google Scholar] [CrossRef]
- Gambin, M.; Sękowski, M.; Woźniak-Prus, M.; Wnuk, A.; Oleksy, T.; Cudo, A.; Hansen, K.; Huflejt-Łukasik, M.; Kubicka, K.; Łyś, A.E.; et al. Generalized anxiety and depressive symptoms in various age groups during the COVID-19 lockdown in Poland. Specific predictors and differences in symptoms severity. Compr. Psychiatry 2021, 105, 152222. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with Suspected COVID-19 Symptoms Were More Likely Depressed and Had Lower Health-Related Quality of Life: The Potential Benefit of Health Literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef]
- Liang, L.; Ren, H.; Cao, R.; Hu, Y.; Qin, Z.; Li, C.; Mei, S. The Effect of COVID-19 on Youth Mental Health. Psychiatr. Q. 2020, 91, 841–852. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.; Grey, I. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. J. Health Psychol. 2020, 25, 1155–1163. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.A.; Smith, L.; Tully, M.A.; Andersen, L.L.; López-Sánchez, G.F. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- King’s College London (KCL). Life under Lockdown: Coronavirus in the UK. Available online: https://www.kcl.ac.uk/news/life-under-lockdown-coronavirus-in-the-uk (accessed on 12 June 2020).
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Luhmann, M.; Hofmann, W.; Eid, M.; Lucas, R.E. Subjective well-being and adaptation to life events: A meta-analysis. J. Pers. Soc. Psychol. 2012, 102, 592–615. [Google Scholar] [CrossRef]
- Luhmann, M.; Fassbender, I.; Alcock, M.; Haehner, P. A dimensional taxonomy of perceived characteristics of major life events. J. Pers. Soc. Psychol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mangelsdorf, J.E.; Eid, M.; Luhmann, M. Does growth require suffering? A systematic review and meta-analysis on genuine posttraumatic and postecstatic growth. Psychol. Bull. 2019, 145, 302–338. [Google Scholar] [CrossRef]
- Barzilay, R.; Moore, T.M.; Greenberg, D.M.; DiDomenico, G.E.; Brown, L.A.; White, L.K.; Gur, R.C.; Gur, R.E. Resilience, COVID-19-related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Transl. Psychiatry 2020, 10, 291. [Google Scholar] [CrossRef] [PubMed]
- Kujawa, A.; Green, H.; Compas, B.E.; Dickey, L.; Pegg, S. Exposure to COVID-19 pandemic stress: Associations with depression and anxiety in emerging adults in the United States. Depress. Anxiety 2020, 37, 1280–1288. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef]
- Holingue, C.; Badillo-Goicoechea, E.; Riehm, K.E.; Veldhuis, C.B.; Thrul, J.; Johnson, R.M.; Fallin, M.D.; Kreuter, F.; Stuart, E.A.; Kalb, L.G. Mental distress during the COVID-19 pandemic among US adults without a pre-existing mental health condition: Findings from American trend panel survey. Prev. Med. 2021, 139, 106231. [Google Scholar] [CrossRef] [PubMed]
- Bourassa, K.J.; Sbarra, D.A.; Caspi, A.; Moffitt, T.E. Social Distancing as a Health Behavior: County-Level Movement in the United States During the COVID-19 Pandemic Is Associated with Conventional Health Behaviors. Ann. Behav. Med. 2020, 54, 548–556. [Google Scholar] [CrossRef]
- Jakovljevic, M. Empathy, sense of coherence and resilience: Bridging personal, public and global mental health and conceptual synthesis. Psychiatr. Danub. 2018, 30, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Bulzing, R.A.; Meyer, J.; Vancampfort, D.; Firth, J.; Stubbs, B.; Grabovac, I.; Willeit, P.; Tavares, V.D.O.; Calegaro, V.C.; et al. Associations of moderate to vigorous physical activity and sedentary behavior with depressive and anxiety symptoms in self-isolating people during the COVID-19 pandemic: A cross-sectional survey in Brazil. Psychiatry Res. 2020, 292, 113339. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.D.; Hammarberg, K.; Kirkman, M.; Nguyen, H.T.M.; Fisher, J. Alcohol use and mental health status during the first months of COVID-19 pandemic in Australia. J. Affect. Disord. 2020, 277, 810–813. [Google Scholar] [CrossRef]
- Best, L.A.; Law, M.A.; Roach, S.; Wilbiks, J.M.P. The psychological impact of COVID-19 in Canada: Effects of social isolation during the initial response. Can. Psychol. Can. 2020, 62, 143–145. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Dvies, G.; Caputi, P.; Skarvelis, M.; Ronan, N. The Depression Anxiety and Stress Scales: Reference data from a large psychiatric outpatient sample. Aust. J. Psychol. 2015, 67, 97–104. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- Cao, R.; Gao, T.; Hu, Y.; Qin, Z.; Ren, H.; Liang, L.; Li, C.; Mei, S. Clustering of lifestyle factors and the relationship with depressive symptoms among adolescents in Northeastern China. J. Affect. Disord. 2020, 274, 704–710. [Google Scholar] [CrossRef]
- Fernández-Aranda, F.; Casas, M.; Claes, L.; Bryan, D.C.; Favaro, A.; Granero, R.; Gudiol, C.; Jiménez-Murcia, S.; Karwautz, A.; Le Grange, D.; et al. COVID -19 and implications for eating disorders. Eur. Eat. Disord. Rev. 2020, 28, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Crawley, J.N. Exploratory behavior models of anxiety in mice. Neurosci. Biobehav. Rev. 1985, 9, 37–44. [Google Scholar] [CrossRef]
- Alteba, S.; Portugalov, A.; Hillard, C.J.; Akirav, I. Inhibition of Fatty Acid Amide Hydrolase (FAAH) During Adolescence and Exposure to Early Life Stress may Exacerbate Depression-like Behaviors in Male and Female Rats. Neuroscience 2021, 455, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Reddy, R.K.; Charles, W.N.; Sklavounos, A.; Dutt, A.; Seed, P.T.; Khajuria, A. The effect of smoking on COVID-19 severity: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1045–1056. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Demographic Measures | Descriptive Statistics 1 |
|---|---|
| Age | 40.40 (13.76), Range: 20–75 |
| Years of education | 14.62 (2.50), Range: 10–21 |
| Gender | Female—55.10% (n = 1085) Male—44.90% (n = 884) |
| Income status since COVID-19 | Not affected—35.24% (n = 694) Moderately affected—33.87% (n = 667) Severely affected—30.87% (n = 608) |
| Work status during COVID-19 | Currently working—61.80% (n = 1217) Not currently working—38.19% (n = 752) |
| Variable | Mean | SD | Median | Range | % Above Normal |
|---|---|---|---|---|---|
| DASS Depression | 4.41 | 5.00 | 3 | 0–21 | 35.96% (n = 705) |
| DASS Anxiety | 2.74 | 4.15 | 1 | 0–21 | 25.76% (n = 505) |
| DASS Stress | 4.87 | 5.01 | 3 | 0–21 | 25.86% (n = 507) |
| DASS Total | 12.03 | 13.21 | 7 | 0–63 | - |
| COVID-related stressors | 32.86 | 8.22 | 33 | 13–52 | - |
| Magnitude of change | 3.24 | 1.70 | 3 | 0–10 | - |
| Change Variable | No Change | Positive Change | Negative Change | Welch’s F (df) | p (η2) |
|---|---|---|---|---|---|
| Alcohol consumption | 6.43 (7.00) n = 349 | 11.53 (10.63) n = 166 | 12.85 (10.67) n = 157 | 33.97 (2, 283.73) | <0.001 (0.096) |
| Cigarette smoking | 11.41 (12.68) n = 1603 | 11.92 (13.92) n = 147 | 16.98 (15.55) n = 204 | 12.04 (2, 260.73) | <0.001 (0.017) |
| Eating habits | 5.26 (5.83) n = 406 | 11.09 (11.65) n = 812 | 12.64 (11.26) n = 643 | 126.15 (2, 1216.64) | <0.001 (0.065) |
| Sleep quality | 4.21 (4.39) n = 463 | 14.05 (11.45) n = 972 | 28.98 (17.76) n = 111 | 360.85 (2, 277.03) | <0.001 (0.273) |
| Physical activity | 8.09 (10.05) n = 310 | 10.82 (10.67) n = 290 | 12.53 (12.30) n = 720 | 18.29 (2, 669.66) | <0.001 (0.024) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alon-Tirosh, M.; Hadar-Shoval, D.; Asraf, K.; Tannous-Haddad, L.; Tzischinsky, O. The Association between Lifestyle Changes and Psychological Distress during COVID-19 Lockdown: The Moderating Role of COVID-Related Stressors. Int. J. Environ. Res. Public Health 2021, 18, 9695. https://doi.org/10.3390/ijerph18189695
Alon-Tirosh M, Hadar-Shoval D, Asraf K, Tannous-Haddad L, Tzischinsky O. The Association between Lifestyle Changes and Psychological Distress during COVID-19 Lockdown: The Moderating Role of COVID-Related Stressors. International Journal of Environmental Research and Public Health. 2021; 18(18):9695. https://doi.org/10.3390/ijerph18189695
Chicago/Turabian StyleAlon-Tirosh, Michal, Dorit Hadar-Shoval, Kfir Asraf, Lubna Tannous-Haddad, and Orna Tzischinsky. 2021. "The Association between Lifestyle Changes and Psychological Distress during COVID-19 Lockdown: The Moderating Role of COVID-Related Stressors" International Journal of Environmental Research and Public Health 18, no. 18: 9695. https://doi.org/10.3390/ijerph18189695
APA StyleAlon-Tirosh, M., Hadar-Shoval, D., Asraf, K., Tannous-Haddad, L., & Tzischinsky, O. (2021). The Association between Lifestyle Changes and Psychological Distress during COVID-19 Lockdown: The Moderating Role of COVID-Related Stressors. International Journal of Environmental Research and Public Health, 18(18), 9695. https://doi.org/10.3390/ijerph18189695