Determinants of the Public Health Promotion Behavior: Evidence from Repurchasing Health Foods for Improving Gastrointestinal Tract Functions


Abstract
:1. Introduction
2. Literature Review
2.1. Health Foods Improving Gastrointestinal Functions
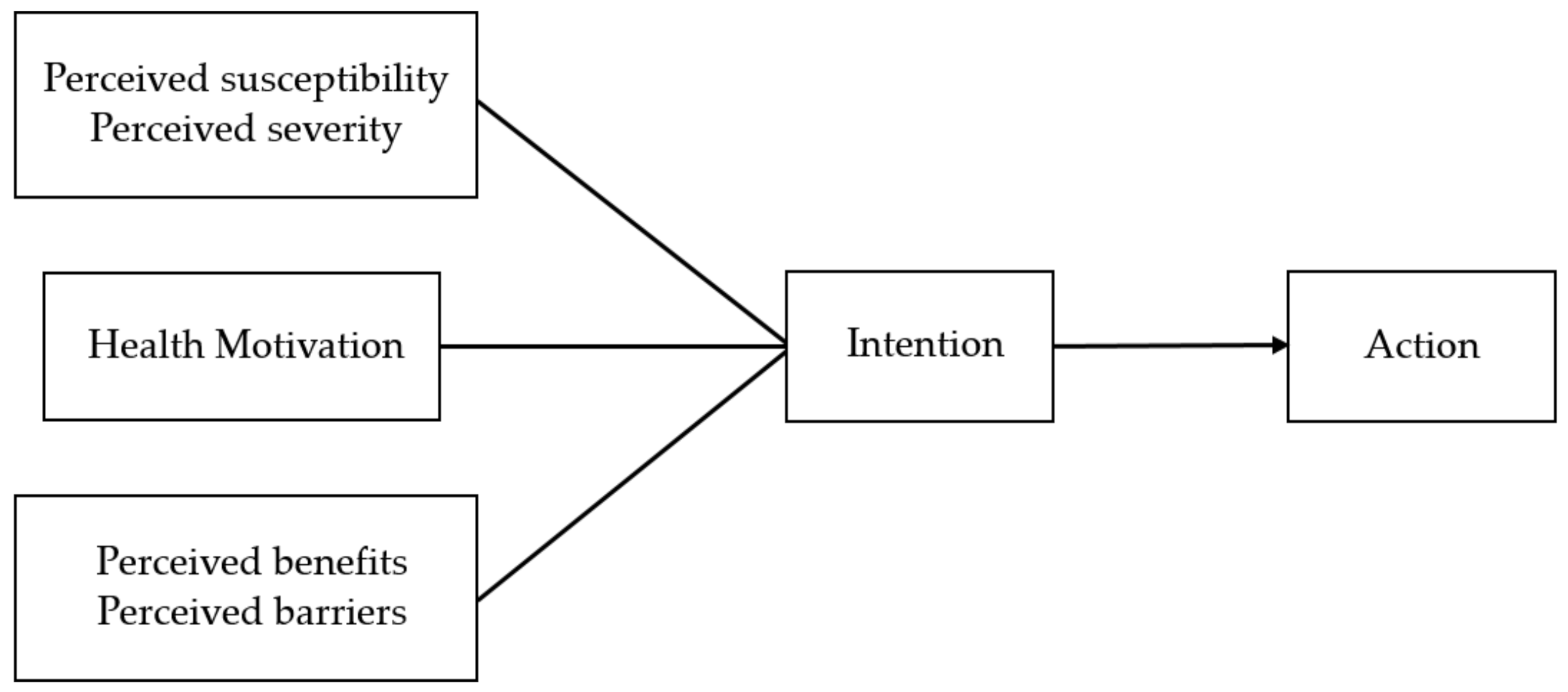
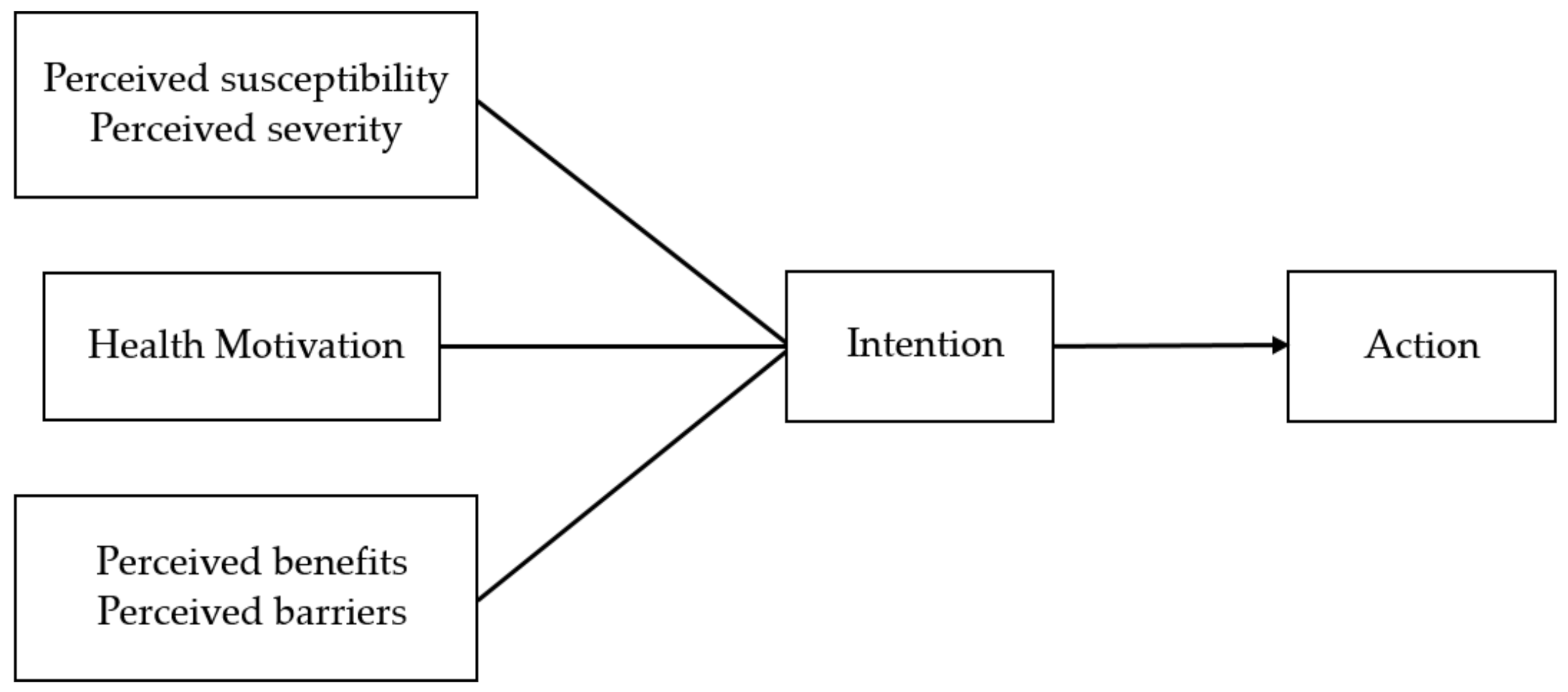
2.2. Health Belief Model (HBM)
2.2.1. Individual Perceptions
2.2.2. Estimated Effects of an Individual Taking Action
2.2.3. Cues to Action
3. Methodology
3.1. Measurement Scale Development
3.2. Data Collection Procedures and Analysis Approaches
4. Results
4.1. Descriptive Statistics Analysis
4.2. Reliability and Validity Analysis
4.3. Analysis of Research Model Results
5. Discussions and Suggestions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Minister of Health and Welfare. The Mortality Rate of Taiwan People in 2019; Minister of Health and Welfare: Taipei City, Taiwan, 2020. [Google Scholar]
- Rosenstock, I.M. Historical origins of the health belief model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Schafer, R.B.; Schafer, E.; Bultena, G.L.; Hoiberg, E.O. Food safety: An application of the health belief model. J. Nutr. Educ. 1993, 25, 17–24. [Google Scholar] [CrossRef]
- Lee, S.Y.; Chou, P.; Yen, E.H. Retrospect and Prospect of Health Belief Model. Taiwan J. Public Health 1989, 9, 123–137. [Google Scholar]
- Achterberg, C.; Miller, C. Is one theory better than another in nutrition education? A viewpoint: More is better. J. Nutr. Educ. Behav. 2004, 36, 40–42. [Google Scholar] [CrossRef]
- Food Industry Research and Development Institute. 2018 Food Industry. Available online: File:///C:/Users/Allen/Downloads/69169900.pdf (accessed on 17 September 2020).
- Evaluation Method for Improving Gastrointestinal Function with Healthy Food Ministry of Health and Welfare. Available online: http://www.rootlaw.com.tw/LawContent.aspx?LawID=A040170051015000-0921117 (accessed on 25 September 2020).
- Rosenstock, I.M. The Health Belief Model: Explaining Health Behavior through Expectancies. In Health Behavior and Health Education: Theory, Research and Practice; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 1990. [Google Scholar]
- Asare, M.; Sharma, M. Role of Health Belief Model on Sexual Communication among African Immigrants. Am. J. Health Stud. 2012, 27, 97–106. [Google Scholar]
- Schwartz, K.; Fakhouri, M.; Bartoces, M.; Monsur, J.; Younis, A. Mammography screening among Arab American women in metropolitan Detroit. J. Immigr. Minor. Health 2008, 10, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Reimann, D.I.; Nicassio, P.; Reimann, J.O.; Gallegos, P.I.; Olmedo, E.L. Acculturation and health beliefs of Mexican Americans regarding tuberculosis prevention. J. Immigr. Health 2004, 6, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Wai, C.T.; Wong, M.L.; Ng, S.; Cheok, A.; Tan, M.H.; Chua, W.; Lim, S.G. Utility of the Health Belief Model in predicting compliance of screening in patients with chronic hepatitis B. Aliment. Pharmacol. Ther. 2005, 21, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Tseng, K.S. Study on willingness of health foods intaking in senior and vocational high school students using health belief model—An example of Tainan city. Creat. Think. J. 2016, 35, 53–89. [Google Scholar]
- Abraham, C.; Sheeran, P. The Health Belief Model. In Predicting Health Behaviour; McGraw-Hill Education: Berkshire, UK, 1996; Volume 2, pp. 28–80. [Google Scholar]
- Taylor, S.; Todd, P.A. Understanding information technology usage: A Test of Competing Models. Inf. Syst. Res. 1995, 6, 144–176. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Macmillan: Basingstoke, UK, 1997. [Google Scholar]
- Lin, Y.C.; Feng, L.J. A Study of Factors Affecting Adolescents’ Behavior Intentions toward Tea-based Drinks. J. Health Manag. 2010, 8, 23–36. [Google Scholar]
- Bish, A.; Sutton, S.; Golombok, S. Predicting uptake of a routine cervical smear test: A comparison of the health belief model and the theory of planned behaviour. Psychol. Health 2000, 15, 35–50. [Google Scholar] [CrossRef]
- Guvenc, G.; Akyuz, A.; Açikel, C.H. Health belief model scale for cervical cancer and Pap smear test: Psychometric testing. J. Adv. Nurs. 2011, 67, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.F.; Wang, R.H.; Schneider, J.K.; Tsai, C.T.; Jiang, D.D.S.; Hung, M.N.; Lin, L.J. Using the health belief model to understand caregiver factors influencing childhood influenza vaccinations. J. Community Health Nurs. 2011, 28, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, L.G.; Kanuk, L.L. Consumer Behavior, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2000. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Dodds, W.B.; Monroe, K.B. The effect of brand and price information on subjective product evaluations. ACR N. Am. Adv. 1985, 12, 85–90. [Google Scholar]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5th ed.; Prentice-Hall International: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Hwang, F.M. Theories and Application of Structural Equation Modeling Taipei; Wu-Nan Book Inc.: Taipei, Taiwan, 2003. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Feng, C.K.; Lin, C.H.; Chang, A.C.; Chang, B.W. To Analyze Exercise Behavior by Applying Health Belief Model among College Students in Taichung City. J. Sport Recreat. Res. 2017, 12, 42–54. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Construct | Items | Source Literature |
|---|---|---|
| Perceived susceptibility |
| Rosenstock [2] Bish et al. [18] |
| Perceived severity |
| Rosenstock [2] Guvenc et al. [19] |
| Perceived benefits of action |
| Rosenstock [2] Chen et al. [20] |
| Perceived barriers of action |
| Rosenstock [2] Chen et al. [20] |
| Cues to action |
| Rosenstock [2] Schiffman and Kanuk [21] |
| Perceived behavioral control |
| Ajzen [22] Taylor and Todd [15] |
| Repurchase intention |
| Dodds and Monroe [23] |
| Repurchase behavior |
| Schiffman and Kanuk [21] |
| Construct | Cronbach’s α | Construct | Cronbach’s α |
|---|---|---|---|
| Perceived susceptibility | 0.921 | Cues to action | 0.851 |
| Perceived severity | 0.821 | Perceived behavioral control | 0.902 |
| Perceived benefits of action | 0.906 | Repurchase intention | 0.848 |
| Perceived barriers of action | 0.807 | Repurchase behavior | 0.920 |
| Latent Variable | CR | AVE | Latent Variable | CR | AVE |
|---|---|---|---|---|---|
| Perceived susceptibility | 0.872 | 0.695 | Cues to action | 0.875 | 0.707 |
| Perceived severity | 0.829 | 0.621 | Perceived behavioral control | 0.905 | 0.761 |
| Perceived benefits of action | 0.757 | 0.609 | Repurchase intention | 0.798 | 0.664 |
| Perceived barriers of action | 0.808 | 0.585 | Repurchase behavior | 0.862 | 0.757 |
| Test Statistic | Criterion | Value in This Study | |
|---|---|---|---|
| Absolute fit indices | χ2 | 515.731 | |
| d.f. | 287 | ||
| χ2/d.f. | <5 | 1.796 | |
| GFI | ≥0.8 | 0.932 | |
| AGFI | >0.8 | 0.912 | |
| RMSEA | <0.08 | 0.038 | |
| Incremental fit indices | NNFI | ≥0.9 | 0.980 |
| CFI | ≥0.9 | 0.982 | |
| IFI | >0.9 | 0.982 | |
| Parsimony fit indices | PNFI | ≥0.5 | 0.792 |
| PGFI | ≥0.5 | 0.712 | |
| CN | >200 | 372.63 |
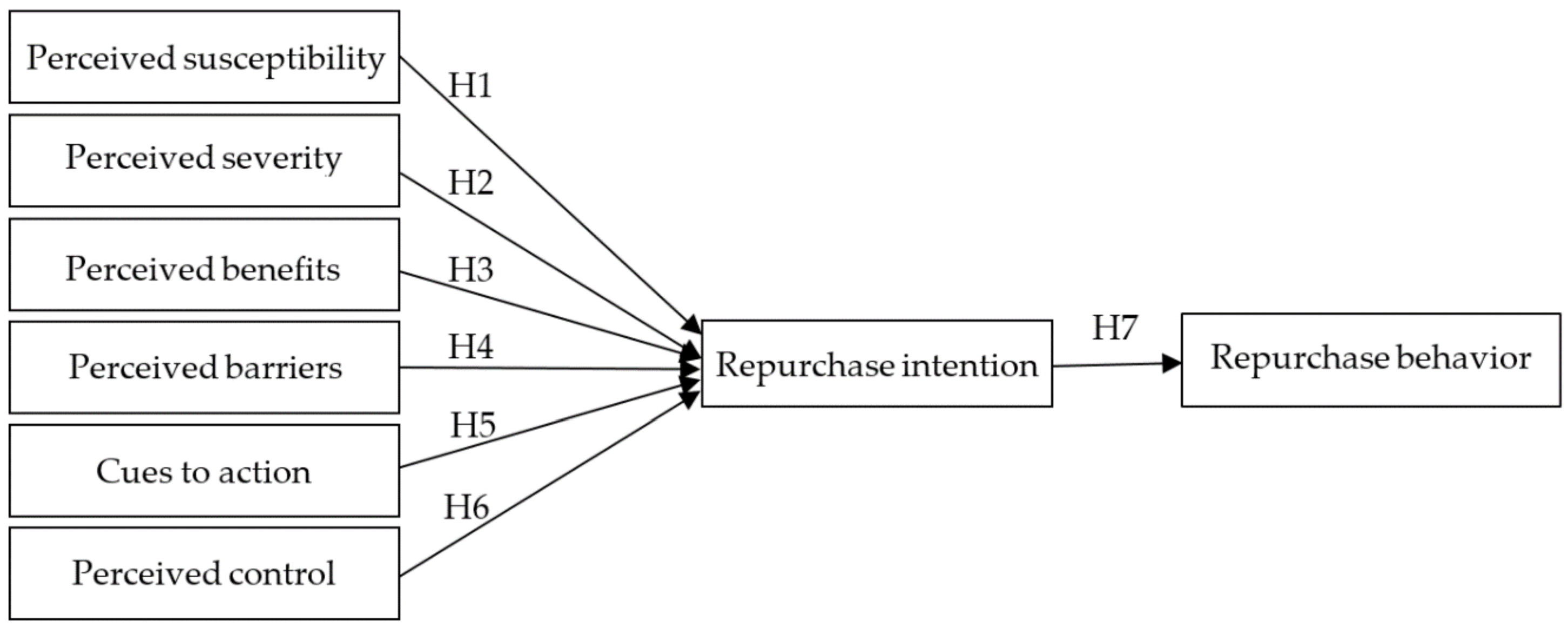
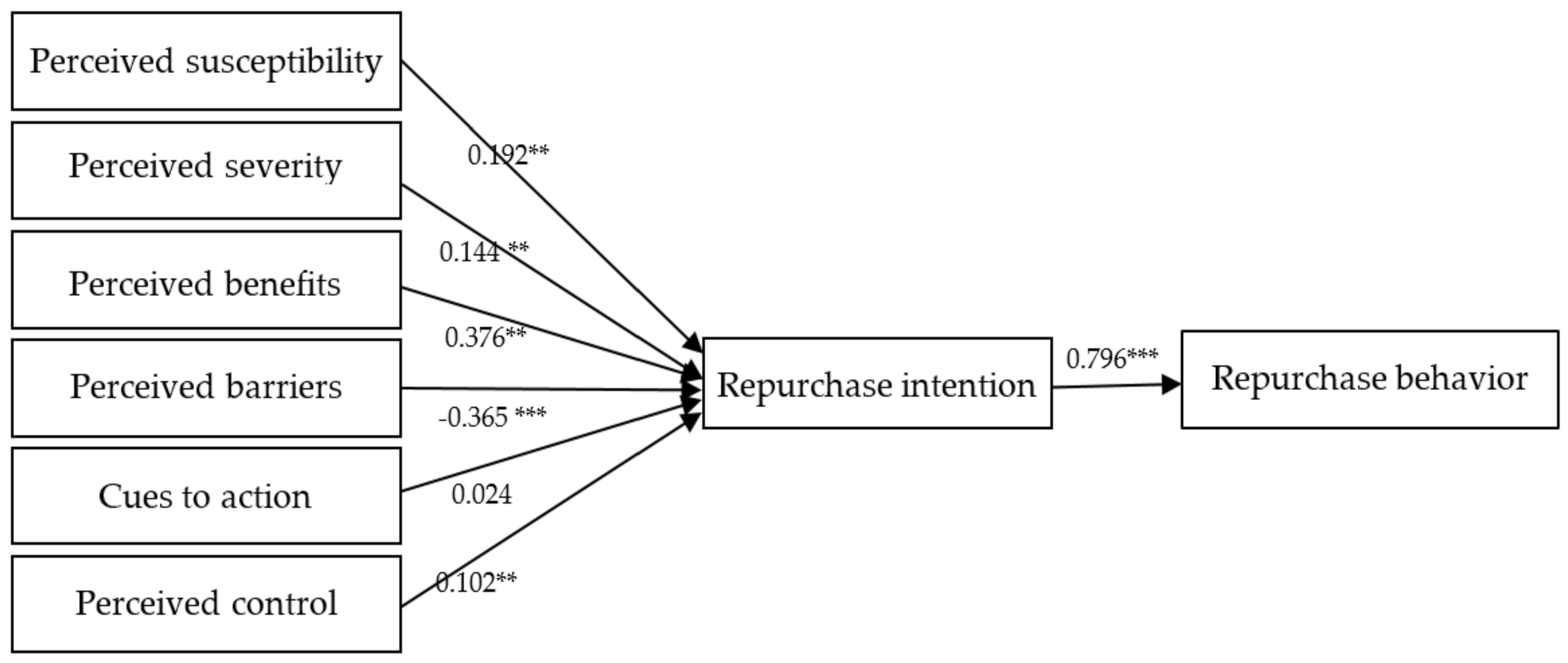
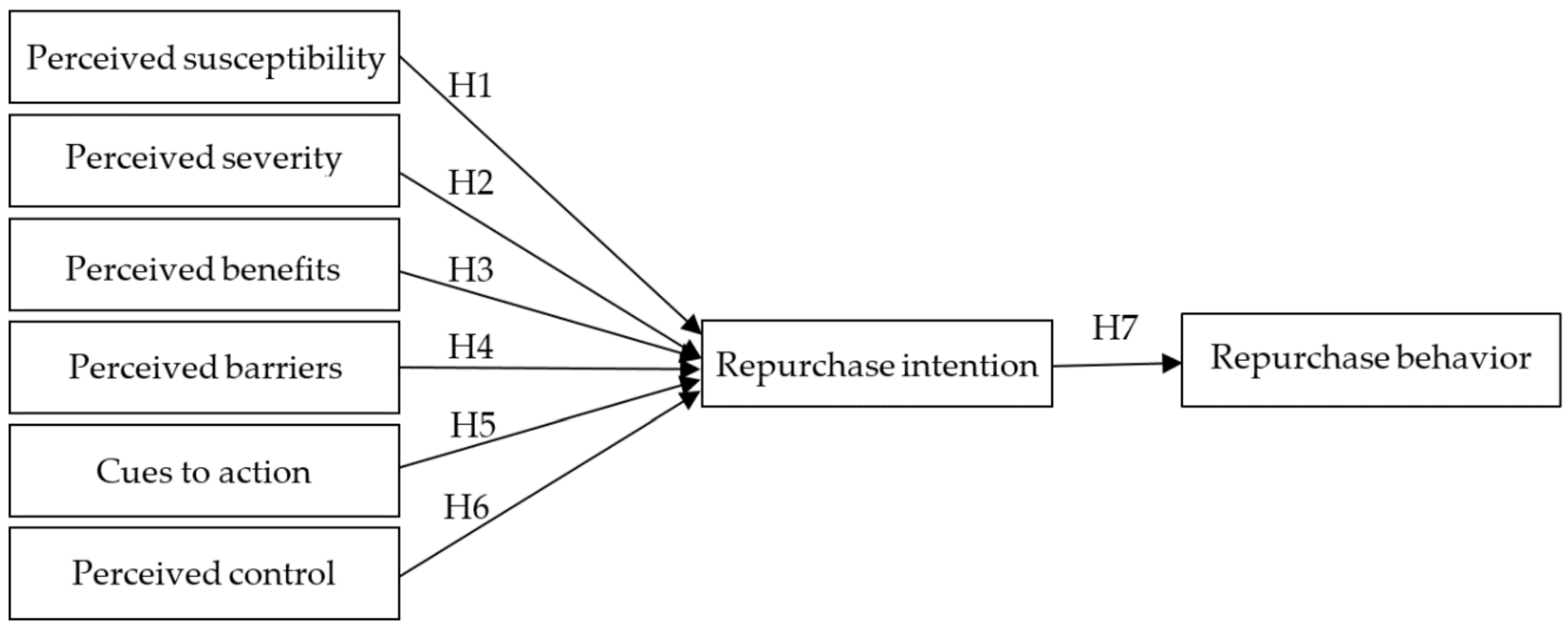
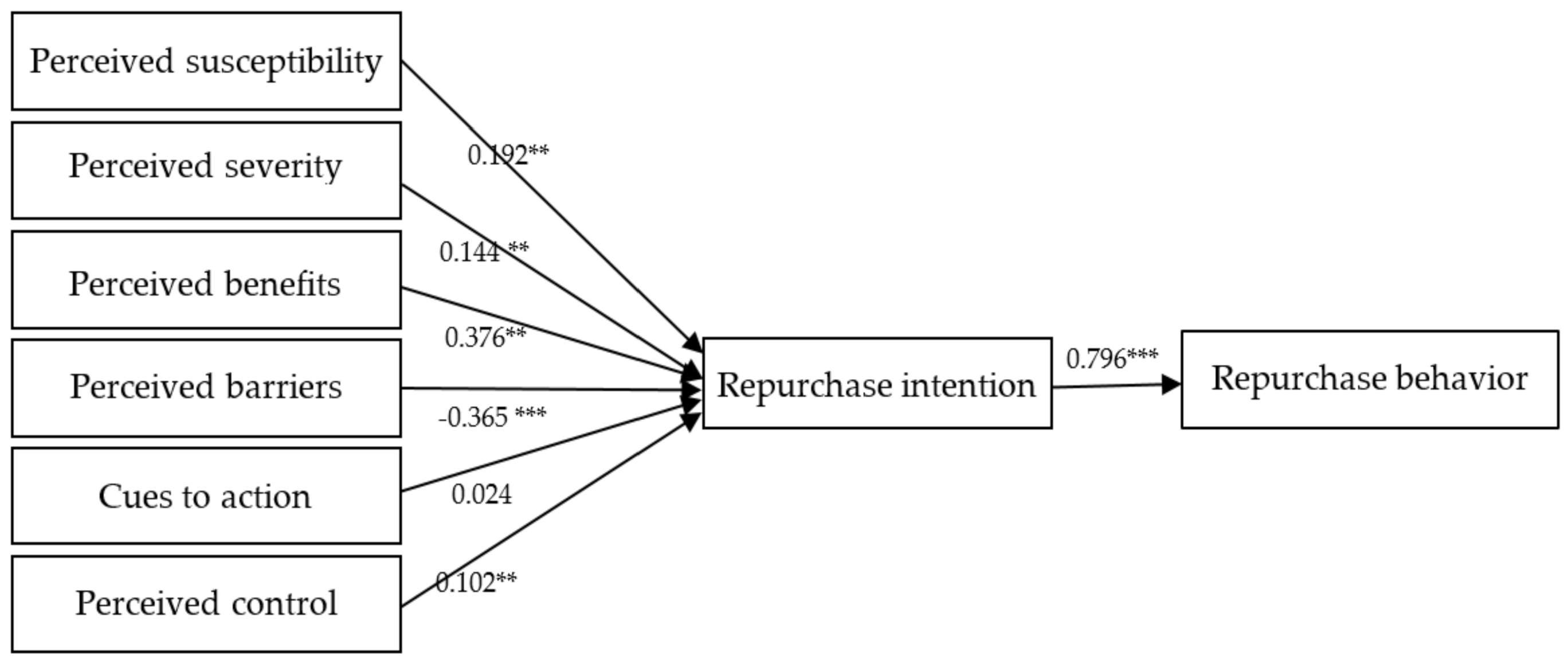
| Path | Expected Sign | Path Coefficient | Test Result |
|---|---|---|---|
| H1: Perceived susceptibility → repurchase intention | + | 0.192 ** | Supported |
| H2: Perceived severity → repurchase intention | + | 0.144 ** | Supported |
| H3: Perceived benefits of action → repurchase intention | + | 0.376 *** | Supported |
| H4: Perceived barriers of action → repurchase intention | − | −0.365 *** | Supported |
| H5: Cues to action → repurchase intention | + | 0.024 | Not supported |
| H6: Perceived behavioral control → repurchase intention | + | 0.102 ** | Supported |
| H7: Repurchase intention → repurchase behavior | + | 0.796 *** | Supported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.-Y.; Wei, C.-Y.; Wu, M.-H.; Hsieh, C.-M. Determinants of the Public Health Promotion Behavior: Evidence from Repurchasing Health Foods for Improving Gastrointestinal Tract Functions. Int. J. Environ. Res. Public Health 2020, 17, 7604. https://doi.org/10.3390/ijerph17207604
Lee K-Y, Wei C-Y, Wu M-H, Hsieh C-M. Determinants of the Public Health Promotion Behavior: Evidence from Repurchasing Health Foods for Improving Gastrointestinal Tract Functions. International Journal of Environmental Research and Public Health. 2020; 17(20):7604. https://doi.org/10.3390/ijerph17207604
Chicago/Turabian StyleLee, Ku-Yuan, Chien-Yu Wei, Min-Hua Wu, and Chi-Ming Hsieh. 2020. "Determinants of the Public Health Promotion Behavior: Evidence from Repurchasing Health Foods for Improving Gastrointestinal Tract Functions" International Journal of Environmental Research and Public Health 17, no. 20: 7604. https://doi.org/10.3390/ijerph17207604
APA StyleLee, K.-Y., Wei, C.-Y., Wu, M.-H., & Hsieh, C.-M. (2020). Determinants of the Public Health Promotion Behavior: Evidence from Repurchasing Health Foods for Improving Gastrointestinal Tract Functions. International Journal of Environmental Research and Public Health, 17(20), 7604. https://doi.org/10.3390/ijerph17207604