Sense of Coherence in Nurses: A Systematic Review

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Methods
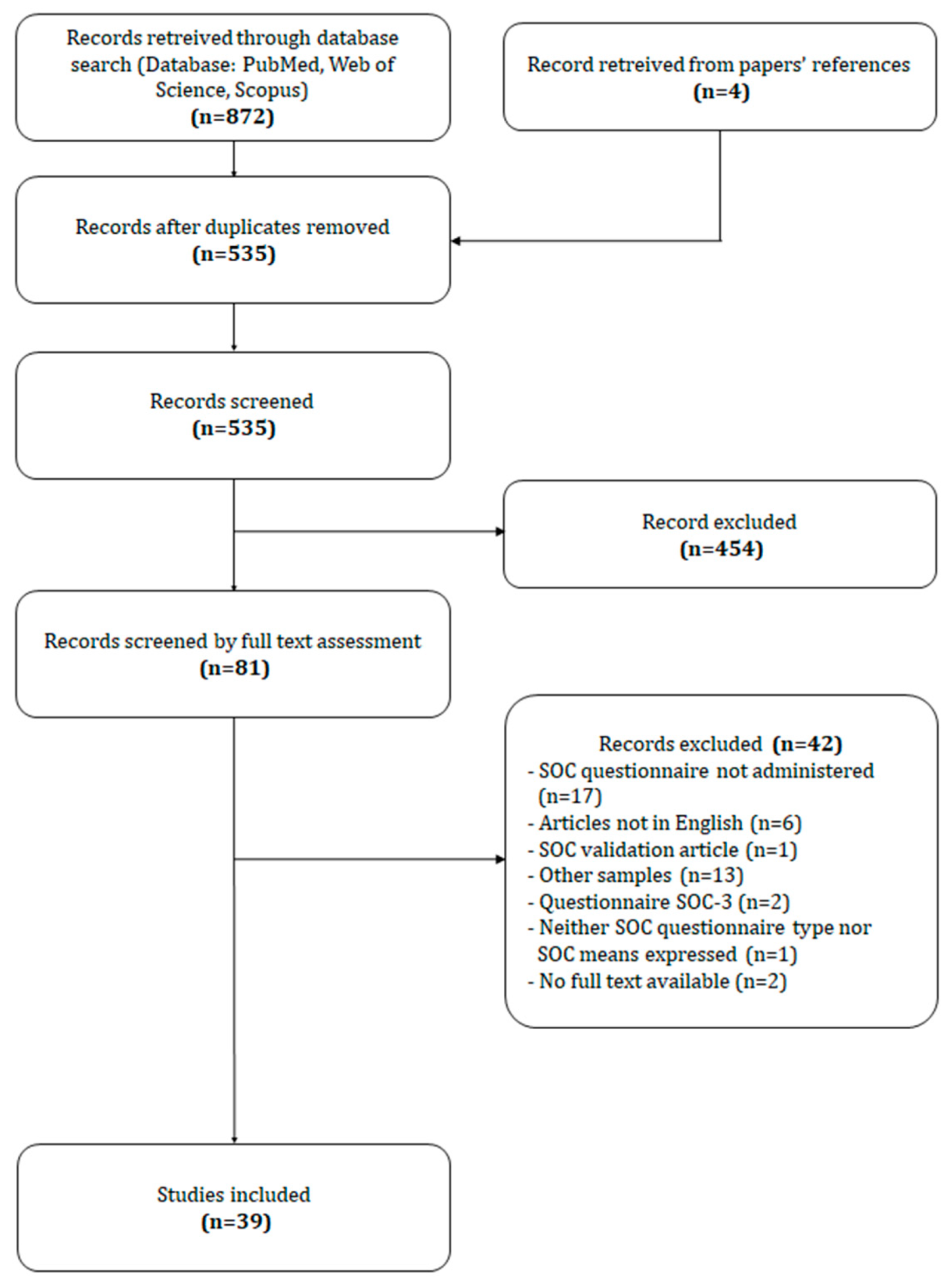
2.2. Articles Selection
2.3. Data Extraction and Synthesis
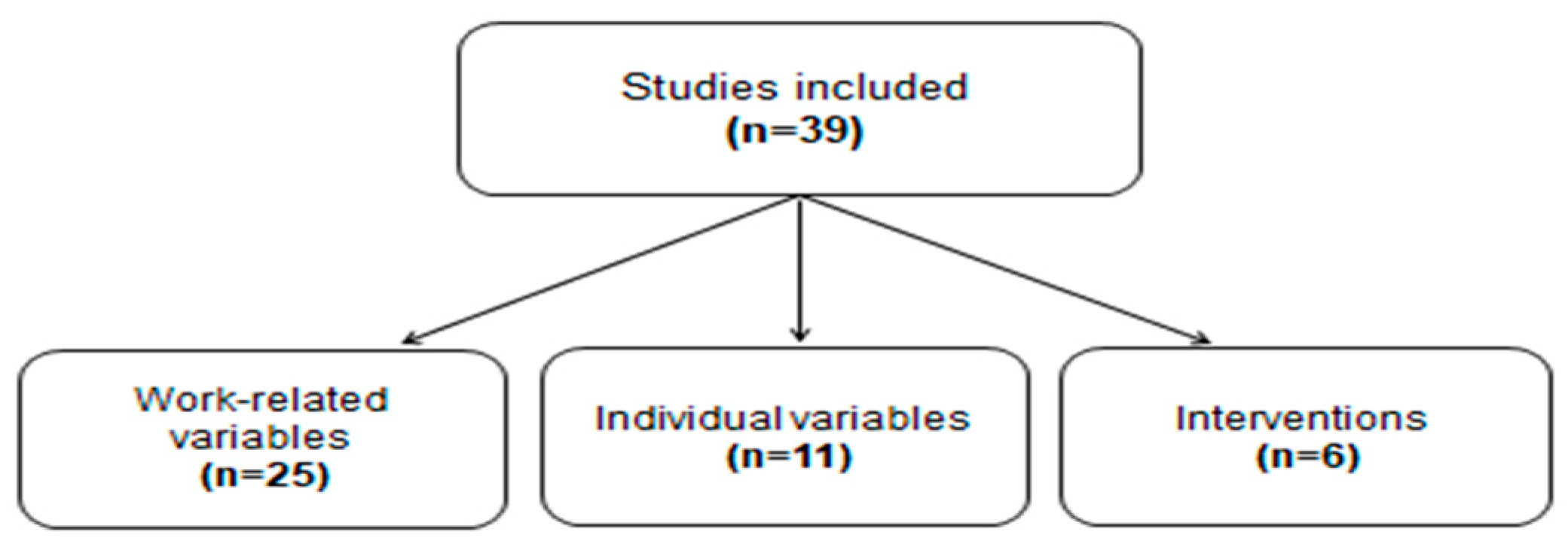
3. Results
3.1. Work-Related Variables
3.1.1. Job Characteristics
3.1.2. Work-Life Balance
3.1.3. Work Related Trauma
3.1.4. Social Support
3.1.5. Stress and Burnout
3.2. Individual Variables
3.2.1. Individual Characteristics
3.2.2. Individual Physical and Mental Health
3.2.3. Personality Traits and Characteristics
3.2.4. Negative Life Events
3.3. Intervention Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Stock, E. Exploring salutogenesis as a concept of health and wellbeing in nurses who thrive professionally. Br. J. Nurs. 2017, 26, 238–241. [Google Scholar] [CrossRef]
- Kowitlawkul, Y.; Yap, S.F.; Makabe, S.; Chan, S.; Takagai, J.; Tam WW, S.; Nurumal, M.S. Investigating nurses’ quality of life and work-life balance statuses in Singapore. Int. Nurs. Rev. 2018, 66, 61–69. [Google Scholar] [CrossRef]
- Ilić, I.M.; Arandjelović, M.Ž.; Jovanović, J.M.; Nešić, M.M. Relationships of Work-Related Psychosocial Risks, Stress, Individual Factors and Burnout—Questionnaire survey among emergency physicians and nurses. Med. Pr. J. 2017, 68, 167–178. [Google Scholar] [CrossRef][Green Version]
- Antonovky, A. Health, Stress, and Coping; Jossey-Bass: San Francisco, CA, USA, 1979. [Google Scholar]
- Mittelmark, M.B.; Sagy, S.; Eriksson, M.; Bauer, G.F.; Pelikan, J.M.; Lindström, B.; Espnes, G.A. The Handbook of Salutogenesis; Springer: Berlin, Germany, 2017. [Google Scholar]
- Hobfoll, S.E. Conservation of Resources: A New Attempt at Conceptualizing Stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef]
- Dębska, G.; Pasek, M.; Wilczek-Rużyczka, E. Sense of coherence vs. mental load in nurses working at a chemotherapy ward. Cent. Eur. J. Public Health 2017, 25, 35–40. [Google Scholar] [CrossRef]
- Kretowicz, K.; Bieniaszewski, L. Determinants of sense of coherence among managerial nursing staff. Ann. Agric. Environ. Med. 2015, 22, 713–717. [Google Scholar] [CrossRef]
- Lewis, S.L.; Campbell, M.A.; Becktell, P.J.; Cooper, C.L.; Bonner, P.N.; Hunt, W.C. Work stress, burnout, and sense of coherence among dialysis nurses. ANNA J. 1992, 19, 545–554. [Google Scholar]
- Miyata, C.; Arai, H.; Suga, S. Characteristics of the nurse manager’s recognition behavior and its relation to sense of coherence of staff nurses in Japan. Collegian 2015, 22, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Fusz, K.; Tóth, Á.; Varga, B.; Rozmann, N.; Oláh, A.; Tudományegyetem, P. Different work schedules of nurses in Hungary and their effects on health. Ideggyógyászati Szle. Clin. Neurosci. 2017, 70, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, Y.; Nakaya, M.; Ikeda, M.; Okuzumi, S.; Takeda, M.; Nishi, M. Sense of Coherence and Personality Traits Related to Depressive State. Psychiatry J. 2014, 2014, 738923. [Google Scholar] [CrossRef] [PubMed]
- Lindmark, U.; Wagman, P.; Rolander, B. Workplace health in dental care—A salutogenic approach. Int. J. Dent. Hyg. 2018, 16, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Kawano, M. Relationships among moral distress, sense of coherence, and job satisfaction. Nurs. Ethics 2018, 25, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Ida, H.; Miura, M.; Komoda, M.; Yakura, N.; Mano, T.; Hamaguchi, T.; Yamazaki, Y.; Kato, K.; Yamauchi, K. Relationship between stress and performance in a Japanese nursing organization. Int. J. Health Care Qual. Assur. 2009, 22, 642–657. [Google Scholar] [CrossRef] [PubMed]
- Van der Colff, J.J.; Rothmann, S. Occupational stress, sense of coherence, coping, burnout and work engagement of registered nurses in South Africa. SA J. Ind. Psychol. 2009, 35, 1–10. [Google Scholar] [CrossRef]
- Hall-lord, M.L.; Larsson, B.W. Registered nurses’ and student nurses’ assessment of pain and distress related to specific patient and nurse characteristics. Nurse Educ. Today 2006, 26, 377–387. [Google Scholar] [CrossRef]
- Makabe, S.; Takagai, J.; Asanuma, Y.; Ohtomo, K.; Kimura, Y. Impact of work-life imbalance on job satisfaction and quality of life among hospital nurses in Japan. Ind. Health 2015, 53, 152–159. [Google Scholar] [CrossRef]
- Michael, R.; Jenkins, H.J. Recovery from work-related trauma by perioperative nurses. Collegian 2001, 8, 8–13. [Google Scholar] [CrossRef]
- Yam, B.M.C.; Shiu, A.T. Perceived stress and sense ofcoherence among critical care nurses in Hong Kong: A pilot study. J. Clin. Nurs. 2003, 12, 144–146. [Google Scholar] [CrossRef]
- Höge, T.; Büssing, A. The Impact of Sense of Coherence and Negative Affectivity on the Work Stressor-Strain Relationship. J. Occup. Health Psychol. 2004, 9, 195–205. Available online: http://doi.apa.org/getdoi.cfm?doi=10.1037/1076-8998.9.3.195 (accessed on 10 February 2020). [CrossRef]
- Berg, A.; Hallberg, I.R. Effects of systematic clinical supervision on psychiatric nurses’ sense of coherence, creativity, work-related strain, job satisfaction and view of the effects from clinical supervision: A pre-post test design. J. Psychiatr. Ment. Health Nurs. 1999, 6, 371–381. [Google Scholar] [CrossRef]
- Lewis, S.L.; Bonner, P.N.; Campbell, M.A.; Cooper, C.L.; Willard, A. Personality, stress, coping, and sense of coherence among nephrology nurses in dialysis settings. ANNA J. 1994, 21, 325–335; discussion 336. [Google Scholar] [PubMed]
- Palsson, M.; Norberg, A.; Bjorvell, H. Burnout, Empathy and Sense of Coherence among Swedish District Nurses before and after Systematic Clinical Supervision. Scand. J. Caring Sci. 1996, 10, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Vifladt, A.; Simonsen, B.O.; Lydersen, S.; Farup, P.G. The association between patient safety culture and burnout and sense of coherence: A cross-sectional study in restructured and not restructured intensive care units. Intensive Crit. Care Nurs. 2016, 36, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Basinska, M.; Andruszkiewicz, A.; Grabowska, M. Nurses’ sense of coherence and their work related patterns of behaviour. Int. J. Occup. Med. Environ. Health 2011, 24, 256–266. [Google Scholar] [CrossRef]
- Tselebis, A.; Moulou, A.; Ilias, I. Burnout versus depression and sense of coherence: Study of Greek nursing staff. Nurs. Health Sci. 2001, 3, 69–71. [Google Scholar] [CrossRef]
- Cilliers, F. Burnout and salutogenic functioning of nurses. Curationis 2003, 26, 62–74. [Google Scholar] [CrossRef]
- Kikuchi, Y.; Nakaya, M.; Ikeda, M.; Okuzumi, S.; Takeda, M.; Nishi, M. Relationship between depressive state, job stress, and sense of coherence among female nurses. Indian J. Occup. Environ. Med. 2014, 18, 32–35. [Google Scholar] [CrossRef]
- Hochwalder, J. Test of antonovsky’s postulate: High sense of coherence helps people avoid negative life events 1. Psychol. Rep. 2015, 116, 363–376. [Google Scholar] [CrossRef]
- Schäfer, S.K.; Lass-hennemann, J.; Groesdonk, H.; Volk, T.; Michael, T. Mental Health in Anesthesiology and ICU Staff: Sense of Coherence Matters. Front. Psychiatry 2018, 9, 440. [Google Scholar] [CrossRef]
- Takeuchi, T.; Yamazaki, Y. Relationship between work—Family conflict and a sense of coherence among Japanese registered nurses. Jpn. J. Nurs. Sci. 2010, 7, 158–168. [Google Scholar] [CrossRef]
- Langius, A.; Bjorvell, H.; Antonovsky, A. The Sense of Coherence Concept and its Relation to Personality Traits in Swedish Samples. Scand. J. Caring Sci. 1992, 6, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Shiu, A.T.Y. The Significance of Sense of Coherence for the Perceptions of Task Characteristics and Stress During Interruptions Amongst a Sample of Public Health Nurses in Hong Kong: Implications for Nursing Management. Public Health Nurs. 1998, 15, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Orita, M.; Goto, A.; Kumagai, A.; Yasui, K.; Ohtsuru, A.; Hayashida, N.; Kudo, T.; Yamashita, S.; Takamura, N. Radiation-related anxiety among public health nurses in the Fukushima Prefecture after the accident at the Fukushima Daiichi Nuclear Power Station: A cross-sectional study. BMJ Open 2016, 6, e013564. [Google Scholar] [CrossRef] [PubMed]
- Hochwa¨lder, J.; Forsell, Y. Is Sense of Coherence Lowered by Negative Life Events ? J. Happiness Stud. 2011, 12, 475–492. [Google Scholar] [CrossRef]
- Ando, M.; Natsume, T.; Kukihara, H.; Shibata, H.; Ito, S. Efficacy of mindfulness-based meditation therapy on the sense of coherence and mental health of nurses. Health 2011, 3, 118–122. [Google Scholar] [CrossRef]
- Sarid, O.; Berger, R.; Segal-engelchin, D. The impact of cognitive behavioral interventions on SOC, perceived stress and mood states of nurses. Procedia. Soc. Behav. Sci. 2010, 2, 928–932. Available online: http://dx.doi.org/10.1016/j.sbspro.2010.03.128 (accessed on 10 February 2020). [CrossRef]
- Orly, S.; Rivka, B.; Rivka, E.; Dorit, S. Are cognitive—Behavioral interventions effective in reducing occupational stress among nurses? Appl. Nurs. Res. 2012, 25, 152–157. [Google Scholar] [CrossRef]
- Shimizu, T.; Kubota, S.; Mishima, N.; Nagata, S. Relationship between Self-Esteem and Assertiveness Training among Japanese. J. Occup. Health 2004, 46, 296–298. [Google Scholar] [CrossRef]
- Kuraoka, Y. Effect of an experiential learning—Based programme to foster competence among nurse managers. J. Nurs. Manag. 2018, 26, 1015–1023. [Google Scholar] [CrossRef]
- Engström, M.; Ljunggren, B.; Lindqvist, R.; Carlsson, M. Staff perceptions of job satisfaction and life situation before and 6 and 12 months after increased information technology support in dementia care. J. Telemed. Telecare 2005, 11, 304–309. [Google Scholar] [CrossRef]
- Antonovsky, A. Unraveling the Mystery of Health. How People Manage Stress and Stay Well; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Eriksson, M.; Lindstrom, B. Validity of Antonovsky’s sense of coherence scale: A systematic review. J. Epidemiol. Community Health 2005, 59, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Lindström, B. Antonovsky’s sense of coherence scale and the relation with health: A systematic review. J. Epidemiol. Community Health 2006, 60, 376–381. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author | Sample-Size/sex | Sample | Country | Mean Age (SD) | Mean Experience (SD) | SOC Scale | Mean SOC (SD) | Study Design | Other Used Instruments | Sense of Coherence (SOC)-Related Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Kowitlawkul et al. 2018 | 1040 nurses 955 females (91.8%) 69 males (6.6%) 16 missing (1.5%) | Registered nurses and enrolled nurses working in inpatient and outpatient departments at a tertiary hospital (in the hospital for ≥6 months) | Singapore | 30.6 (8.5) | -- | SOC-13 | 50/50 group: 55.7 (9.5) 60/40 group: 56.0 (9.6) 70/30 group: 54.5 (9.2) 80/20 group: 52.4 (10.8) | Descriptive quantitative study | Work life balance (WLB) Job satisfaction questionnaire Social support questionnaire WHO-Quality of Life (WHO-QOL)-BREF-26 questionnaire | - Division in four groups depending on the proportion of time spent on work and private life (50/50 and below, 60/40, 70/30, 80/20 and above) -“50/50 and below” and “60/40” groups’ SOC scores are higher the other two groups-lowest SOC scores are in the “80/20 and above” group -SOC and social support are significant predictors for all QoL domains -A unit increase in SOC results in a 6–12% increase in likelihood of having high QoL for all domains |
| Kuraoka et al. 2018 | 63 nurses 60 females (95.2%) 3 males (4.8%) | Nurse managers in the first 3 years of a supervisory role, working in acute-care hospitals Participation in an experiential learning-based program | Japan | 45.2 (3.4) | 1.4 (0.6) | SOC-13 | Pre-test: 57.17 (10.28) Post-test: 54.97 (10.4) | Quasi-experimental study | Experiential Learning Inventory on the Job (ELI) Ad hoc questionnaire for Knowledge of Experiential Learning Social Support Questionnaire (SSQ) Nurse Managers Competence Inventory (NMCI) | -Mean SOC scores reduction after participation to the experiential learning-based program |
| Schäfer et al. 2018 | 27 nurses 44 females (65.4%) 18 males (34.6%) | Nurses working in ICU and anesthesiology unit | Germany | 39 (10) | -- | SOC-13 | 43.19 (9.63) | Cross sectional study | Resilience Scale (RS-11) Scale for assessment of internal and external control beliefs (IE-4) ICD 10 symptom rating (ISR) PTSD Checklist (PCL-5) | -No differences in resilience, nor SOC or LOC (locus of control) between physicians and nursing staff -SOC, resilience, and internal and external LOC correlate with ISR score and PTSD symptoms -SOC is a significant predictor of mental health problems and of symptom severity -Resilience, internal and external LOC account for 59% of SOC variance and have a significant indirect effects on symptom severity measures mediated by SOC on symptoms severity measures |
| Debska et al. 2017 | 164 nurses (sex unknown) | Nurses working at inpatient chemotherapy wards | Poland | 43.07 (7.99) | In chemotherapy ward: 11.77 (7.65) | SOC-29 | 125.05 (18.30) | Cross-sectional study | Meister Questionnaire | -Highest SOC scores for the Manageability subscale (45.15), lower for Comprehensibility and Meaningfulness subscales (41.18 and 38.73, respectively) - Inverse correlation between SOC and Monotony (r = −0.398, p < 0.001), Unspecific Load (r = −0.370, p < 0.001), - Mental Load (r = −0.378, p < 0.001) and Work experience (r = −0.19, p = 0.016) -No correlation between SOC and work-experience -Inverse correlation between age and Manageability level (r = −0.193, p = 0.014) -No correlation between overall SOC and age, nor educational level |
| Fusz et al. 2017 | 518 nurses 482 females (93.1%) 36 males (6.9%) | Nurses working in eight different hospitals | Hungary | 42.44 (9.59) | -- | SOC -13 | 61.76 | Cross-sectional study | Ad hoc questionnaire for sense of quality, quality of sleep, frequency of psychosomatic symptoms, and work schedule regularity | -Higher SOC score for day-shift workers (65.84), compared to shift workers (61.02) (t = 2.933; p = 0.004) -Lower SOC score for irregular work schedule workers (58.19), compared to flexible work schedule workers (63.17, p = 0.04) -Lower scores in self-heath-assessment for irregular work schedule workers, compared to flexible work schedule workers (p = 0.019) |
| Stock et al. 2017 | 12 nurses 10 females (83.33%) 2 males (16.67%) | Nurses self-described as thriving, experienced (10+ y) or recently retired (<1 y) | Hawaii | 55–64 y: 33.33% | 10–21 y: 33% >34 y: 67% | SOC-13 | 73.58 | Mixed method, exploratory-descriptive study | Ad hoc questionnaire for thriving view and experience | Possible link between SOC and self-described thriving nurses Nurses have a high SOC and the use of GRRs |
| Ando et al. 2016 | 130 nurses 102 females (78.5%) 28 males (21.5%) | Nurses from psychiatric and internal medicine wards at a national hospital | Japan | 40–49 y: 35.4% | 18.7 | SOC-13 | 53.5 (9.7) | Cross-sectional study | Moral Distress Scale for Psychiatric Nurses (MDS-P) General Heath Questionnaire - 12 (GHQ-12) Job Satisfaction Scale (JS) | Inverse correlation between MDS-P and SOC Inverse correlation between MDS-P and JS “Unethical conduct by caregivers” negatively correlates with Manageability (r = −0.28, p < 0.01), Comprehensibility (r =-0.22, p < 0.01) and Meaning (r = −0.017, p < 0.05) “Low staffing” negatively correlated with Comprehensibility (r = −0.30, p < 0.001) and Manageability (r = −0.22, p < 0.01) “Acquiescence to patients’ rights violations” negatively correlates with Manageability (r = −0.31, p < 0.01), Comprehensibility (r = −0.28, p < 0.01) and Meaning (r = −0.22, p < 0,01). “Acquiescence to patients’ rights violations” (standard β = −0,26, p < 0.01) and “Meaning” of SOC (standard β = 0.35, p < 0.001) influence Job Satisfaction more than other variables. |
| Lindmark et al. 2016 | 165 nurses (sex unknown) | Dental nurses working in the Public Dental Service | Sweden | -- | -- | SOC-13 | 68.4 (11.0) | Cross-sectional study | Salutogenic Health Indicator Scale (SHIS) Work Experience Measurement Scale (WEMS) | Clinical coordinators have higher SOC score (75.1; SD 10.0), compared with all other professions, including dental nurses Dental hygienists have higher scores for meaningfulness (23.8; SD 3.3), and dentists have higher scores for manageability (22.1; SD 3.6), compared with dental nurses (22.5; SD 3.4 and 20.3; SD 4.0, respectively) |
| Vifladt et al. 2016 | 143 nurses 126 females (88.1%) 13 males (9.1%) 4 unknown (2.8%) | Nurses working in ICUs in six hospitals for ≥ 3 months | Norway | 41–50 y: 37.4% | ≥21 y: 26.1% | SOC-13 | 72.2 (8.96) | Cross-sectional study | Hospital Survey on Patient Safety Culture (HSOPSC) Bergen Burnout Indicator | Positive safety culture negatively correlates with burnout and positively correlates with SOC (r = −0.451, r = 0.393, respectively, p < 0.001). Inverse correlation between SOC and burnout (r = −0.577, p < 0.001) Positive correlation between SOC and safety culture at the unit level (β = 0.014, 95%CI = 0.005-0.024, p = 0.003) and hospital level (β = 0.017, 95%CI = 0.008–0.026, p < 0.001) |
| Yoshida et al. 2016 | 430 nurses 416 females (96.7%) 14 males (3.3%) | Public health nurses (after the earthquake, tsunami and Fukushima Daiichi Nuclear Power Station accident following the Great East Japan Earthquake in 2011) | Japan | ≥ 50 y: 35.6% | <10 y: 22.8% >10 y: 71.2% | SOC-13 | 43.0 (7.7) | Cross-sectional study | Ad hoc questionnaire for anxiety | Division in two groups based on anxiety score on a 10-point Likert scale: 1–5 ‘anxiety (−)’ and 6–10 ‘anxiety (+)’ No difference in mean SOC between the anxiety (+) and the anxiety (-) groups Higher ratio of nurses <40 years of age in the anxiety (+) group (p < 0.001) Higher ratio of nurses with <10 years of working experience, staff positions and nursing licenses in the anxiety (+) group (p < 0.001) |
| Hochwälder et al. 2015 | 1012 nurses (all females) | Nurses working at three hospitals and two primary health care settings, ≥ 30 y of age, with no negative life events during the previous year | Sweden | 46.6 (8.9) | -- | SOC-29 | 150.21 (20.28) Low SOC (<144) group n = 322): 126.35 (13.82) Moderate SOC (144–160) group n = 348: 152.20 (4.84) High SOC (>160) group n = 342: 170.63 (7.49) | Longitudinal study | Ad hoc questionnaire for Controllable and Uncontrollable Negative Life events | No significant age differences between Low, Moderate and High SOC groups Higher dropout rate in the Low SOC group No significant difference between SOC groups and mean number of uncontrolled negative life events High and Moderate SOC groups have fewer controllable negative life events compared to the Low SOC group (p < 0.001) |
| Kretowicz et al. 2015 | 310 nurses 301 females (97.1%) 9 males (2.9%) | Nurse managers in selected medical units | Poland | 45.7 (6.7) | Mean nursing experience 24.7 (7.2) y Mean managerial experience 8.8 (6.7) y | SOC -29 | 147.00 (20.47) | Cross-sectional study | -- | No correlation between age and SOC Correlation between educational background and SOC (Kruskal-Wallis test 9.04; p = 0.029) and Meaningfulness (Kruskal-Wallis test 12.82; p = 0.005) No correlation between SOC and general working experience, managerial working experience, position at work and characteristics of employment Higher SOC in nurses employed as strategic managers (U Mann-Wallis test -2.74; p = 0.006) |
| Makabe et al. 2015 | 1202 nurses 1116 females (93%) 86 males (7%) | Nurses working in three hospitals | Japan | 37 (11) | 15 (12) | SOC-13 | 50/50 group (A): 55.7 (9.5) 60/40 group (B): 56.0 (9.6) 70/30 group (C): 54.5 (9.2) 80/20 group (D): 52.4 (10.8) | Cross sectional study | Work-Life Balance (WLB) Work-Life Balance Satisfaction Job Satisfaction Scale WHO Quality of Life (26-item) | Division in four groups depending on the proportions of percentages of time spent on work and private life - WLB status [50/50 and below (A), 60/40 (B), 70/30 (C), 80/20 and above (D)] Group A has a higher SOC score than all other groups (ANCOVA p < 0.001) Group D has a lower SOC score than all other groups (ANCOVA p < 0.001) |
| Miyata et al. 2015 | 1425 nurses 1333 females (94%) 92 males (6%) | Nurse staff (n = 1248%–88%) and nurse managers (n = 177–12%) working in 10 hospitals | Japan | 35.5 (9.9) | 12.8 (9.5) | SOC-13 | median: 50 (IQR 45–55) | Cross-sectional study | Recognition behavior scale | No significant correlation between SOC and marital status Positive correlation between SOC and good mental health status (OR = 4.07, 95%CI = 2.53–6.53), good physical health status (OR = 1.08, 95% CI = 1.09–2.89), overall work experience (OR = 1.05, 95%CI= 1.04–1.07), with p < 0.001, and recognition behaviors by the nurse manager (OR = 1.02 (95% CI = 1.01–1.04), p = 0.006 |
| Kikuchi et al. 2014 | 347 nurses (all females) | Nurses working at a general hospital (intensive care, pediatrics, surgery, oncology, and emergency medicine) | Japan | 33.7 (9.2) | -- | SOC-13 | 54.2 (11.9) | Cross-sectional study | Brief Job Stress Questionnaire (BJSQ) K6 short screening questionnaire Ten-item Personality Inventory (TIPI-J) | Age negatively correlates with depressive state (r = −0.18, p = 0.00) and positively to SOC (r = 0.27, p = 0.00) Inverse correlation between SOC and shift work (r = −0.16, p = 0.00), job rank (r = −0.14, p = 0.01), and overtime hours (r = −0.33, p = 0.00). SOC and depressive state correlate negatively with almost all job stressors and personality traits Inverse correlation between SOC and Neuroticism (r = −0.49, p = 0.00). Inverse correlation between SOC and depressive state (r = −0.67, p = 0.00 Positive correlation between SOC and job and life satisfaction (r = 0.47, p = 0.00) |
| Kikuchi et al. 2014 | 348 nurses (all females) | Nurses working at a general hospital (intensive care, pediatrics, surgery, oncology, and emergency medicine) | Japan | 34.4 (9.0) | -- | SOC-29 | 124.4 (21.2) | Cross-sectional study | K6 short screening questionnaire Effort-reward imbalance (ERI) scale | SOC (β = −0.46, p < 0.001), over-commitment, effort-esteem ratio, and age significantly correlate with the depressive state Age correlates positively with SOC (r = 0.12, p < 0.05) |
| Sarid et al. 2012 | 36 nurses (sex unknown) | Nurses working both clinical and administrative roles in one major regional hospital, ≥ 5 y of experience Intervention group (n = 20): Participation in a Cognitive-Behavioral course Control group (n = 16) | Israel | 50.6 (10.7) | -- | SOC-13 | Intervention group T1: 70.83 (7.67) T2: 75.05 (6.7) Control group T1: 72.07 (8.9) T2: 69.61 (7.64) | Pre-post test design, with control | Perceived stress scale (PSS) Profile of Mood states (POMS) | In the intervention group at T2 higher SOC, more vigor, less perceived stress, and less fatigue, compared to T1 At T1 no significant difference in mean SOC scores between the groups At T2 significant difference in mean SOC scores between the two groups F(p) = 10.44 (p < 0.05) |
| Ando et al. 2011 | 28 nurses (sex unknown) | Nurses working in geriatric wards, ≥ 20 y of experience, without severe mental problems Intervention group (n = 15): participation in mindfulness based therapy sessions Control Group (n = 13) | Japan | -- | -- | SOC-13 | Post-intervention Intervention group: 52 Control group: 53 | Pre-post test design, with control | General Health Questionnaire (GHQ) Functional Assessment of Chronic Illness Therapy (FACIT-sp) | - Significant decrease in GHQ after the intervention (improvement in general health) - Significant increase in SOC after the intervention, no change in the control group - Meaningfulness: higher scores and significant increase after intervention: Higher scores and significant increase after intervention, compared to comprehensibility and manageability - No effect on spirituality |
| Basinska et al. 2011 | 331 nurses (all females) | Nurses working shifts in three general care hospitals | Poland | 34.15 (6.61) | -- | SOC-29 | 136.46 (21.43) | Descriptive quantitative study | Work Related Patterns of Behavior and Experience Questionnaire (AVEM) | Division in work related behavior type groups: type G-healthy, type S-frugal, type A-risk (overburdened), type B-burnout Positive correlation between SOC and healthy type G and the frugal type S (r = 0.50, and r = 0.20 respectively, p < 0.001) Inverse correlation between SOC and burnout type B and the overburdened type A (r = −0.57 p < 0.001 and r = −0.13 p < 0.05 respectively) SOC explains 28% of the variability of type B, 21% of type G and 7% of type S |
| Hochwälder et al. 2011 | 1012 nurses (all females) | Nurses working in hospitals and primary health care setting, > 30 y of age Group 0: no negative life events Group 1: ≥1 negative life event in the previous year | Sweden | 46.90 (8.85) | 46.9 (8.85) | SOC-29 | At T1: 150.21 (20.28) At T2: 150.89 (20.38) | Cross sectional study | Ad hoc questionnaire for Negative Life Events | SOC stable from T1 to T2 No strong evidence that negative life events lower SOC No evidence that negative life events lower SOC more in persons with an initially low or moderate SOC that in persons with an initially high SOC. SOC for those who experience a negative life event, is initially weaker, than those who do not experience any negative life events |
| Sarid et al. 2010 | 36 nurses (sex unknow) | Nurses working in all hospital wards, > 5 y of experience, both clinical and administrative roles Study group (n = 20): participation in a CBI course Control group (n = 16) | Israel | 50.6 (10.7) | -- | SOC-13 | -- | Pre-post test design | Perceived Stress Scale (PSS) Profile of Mood States (POMS) | No differences in SOC, perceived stress and mood states between the groups at T1 Intervention group at T2: increased levels of SOC and vigor and decreased levels of perceived stress and fatigue Mean changes in SOC were -4,20 (SD = 1.28) for the study group and 2,11 (SD = 1.46) for the control group, F = 10.44, p < 0.05 |
| Takeuchi et al. 2010 | 138 nurses (all females) | Nurses working at three hospitals, who are also mothers and/or wives | Japan | 36.2 (8.0) | 12.5 (8.3) | SOC-13 | 56.7 (9.9) | Descriptive quantitative study | Job Content Questionnaire (JCQ, 6 items) Cumulative fatigue symptoms index (CFSI-18) Center for Epidemiologic Studies Depression (CES-D) scale Work-to-Family conflicts scale | Inverse correlation between work-family conflict and SOC (β = −0.233, partial r = −0.340, p < 0.01) Inverse correlation between SOC and cumulative fatigue (β = −0.397, p < 0.001) and depression (β = −0.517, p < 0.001). The interaction of SOC and WFC influences depression (β = 0.214, p < 0.05), SOC has a buffering effect on WFC with respect to depression. |
| Ida et al. 2009 | 502 nurses (all females) | Nurses working at a major university hospital | Japan | 32.4 (9.9) | -- | SOC-29 | -- | Cross-sectional study | Job Content Questionnaire (JCQ-12) Ad hoc questionnaire for medical errors and nurses career levels | Positive correlation between Comprehensibility and professional experience (r = 0.125, p < 0.001) Positive correlation between SOC and workplace adaptability (r = 0.335, p < 0.01), and job satisfaction (r = 0.280, p < 0.01) Inverse correlation between SOC and organization environment (r = −0.611, p < 0.01) and health risk (r = −0.364, p < 0.01) SOC affects sickness-absence (OR = 0.982, 95%CI = 0.970–0.995) |
| Van der Colff et al. 2009 | 818 nurses 791 females (97.4%) 21 males (2.6%) 6 sex unknown | Nurses working in hospital wards, psychiatric wards, community/occupational services and nursing management. | South Africa | 40 | 19 | SOC-29 | 137.95 (20.46) | Cross sectional study | Nursing Stress Inventory (NSI) Coping Orientation for Problem Experienced Questionnaire (COPE) Maslach Burnout Inventory- Human Services Survey (MBIHSS) Utrecht Work Engagement Scale (UWES) | Correlation between SOC and burnout subscores. Emotional exhaustion (−0,49), Depersonalization (−0,47) and Personal accomplishment (0.34) (p < 0.05) Positive correlation between SOC and Engagement (0.42) Negative correlation between SOC and Nursing stress inventory (NSI) variables: Lack of organizational support (−0.23), job demands (−0.28) and nursing-specific demands (−0.15) (p < 0.05) SOC correlates with coping strategies: Approach coping (0.0), Seeking emotional/social support (0.18) and Turning to religion (0,11), Avoidance (−0.35) and Focus on and ventilation of emotions (−0.29) (p < 0.05) |
| Hall-Lord et al. 2006 | 71 nurses (sex not specified) | Nurses participating in an educational program | Sweden | 39.2 (8.05) | 16.7 (7.35) | SOC-13 | -- | Cross-sectional study | Ad hoc questionnaire for assessment of pain and distress of patients Five-factor personality inventory (FFPI) | Patients’ age and type of illness seems to influence nurses’ assessments of pain and distress Nurses with high emotional stability and high SOC scores assess pain and distress for acute patients as less intense and assess it more intense for chronic patients |
| Engström et al. 2005 | 33 nurses 31 females (94%) 2 males (6%) | Nurses working in a residential home for persons with dementia Experimental group (n = 17): participation in IT support project Control group (n = 16) | Sweden | 41 | Experimental group -in nursing care 12 (8) -in dementia care 5 (3) Control group -in nursing care 15 (9) -as district nurse 9 (7) | SOC-13 | Intervention group -baseline: 72 (12) -at 6 months: 69 (11) -at 12 months: 75 (9) Control group -baseline: 68 (10) -at 6 months: 69 (9) -at 12 months: 65 (13) | Quasi-experimental non-equivalent groups design | Satisfaction with Work Questionaires (SWQ) Life Satisfaction Questionnaire (LSQ) | Perception of psychosocial job satisfaction and quality of care improve in the experimental group No significant within-subject effect for the total SOC scale and meaningfulness subscale, split on the experimental and control groups Interaction effect for the factors family relation, close friend relation (LSQ), total SOC scale and meaningfulness subscale |
| Höge et al. 2004 | 160 nurses (sex not specified) | Nurses working at two hospitals | Germany | -- | -- | SOC-13 | 68.1 (10.83) | Cross-sectional study | Work load screening TAA-KH-S Negative Affectivity Scale (NAS) Maslach Burnout Inventory (Emotional exhaustion subcategory) Irritation Strain questionnaire Short Form Health Survey (SF-12) | Inverse correlation between SOC and Negative Affectivity (r = −0.61) Inverse correlation between SOC and overall strain (rs = −0.33) and overall stressors (rs = −0.34) |
| Shimizu et al. 2004 | 285 nurses (all females) | Nurses working at a hospital Intervention group (n = 62): participation in an assertiveness training Reference group (n = 196) | Japan | Intervention group: 44 (7.1) Reference group: 27.8 (5.9) | -- | SOC-13 | Intervention group T1: 57.4 (10.5) T2: ΔSOC 2.2 (8.3) Comparison group T1: 52.7 (9.4) T2: ΔSOC 1.5 (8.6) | Pre-post test design, with control | Rosemberg’s self-esteem scale (SES) | -No significant difference between the ΔSOC of the intervention group and that of the reference group. -Improvement in SES at six months after the intervention |
| Cilliers et al. 2003 | 105 nurses (all females) | Nurses working in large hospitals, ≥ 5 y of experience | South Africa | range: 28-57 | SOC-29 | 141.28 (16.44) | Cross-sectional study | Maslach Burnout Inventory (MBI) Personal Views Survey (HAR) Self-Control Schedule (LR) | Inverse correlation between burnout and salutogenic functioning (SOC, HAR and LR) Inverse correlation between SOC and emotional exhaustion (r = −0.21, p < 0.01) and depersonalization (r = −0.25, p < 0.01) Positive correlation between SOC and personal accomplishment (r = 0.35, p < 0.001) | |
| Yam et al. 2003 | 29 nurses 28 females (96.5%) 1 male (3.4%) | Nurses working in critical care in public and private hospitals | Hong Kong | 32 | 7.6 | SOC-13 | -- | Cross-sectional study | Critical Care Nursing stress scale (CCNSS) Perceived Stress Scale (PSS) | Inverse correlation between SOC and CCNSS (r = −0.20, p = 0.30) Inverse correlation between SOC and PSS (r = −0.64, p < 0.001) |
| Michael et al. 2001 | 233 nurses 225 females (96.56%) 8 males (3.43%) | Nurses working in operating suites in private and public hospitals | Australia | 41 | 11 years in operating suite | SOC-13 | 66.75 (9.77) | Mixed method trianglulated study | Ad hoc questionnaire for work-related traumatic events Ad hoc questionnaire for social support | nurses who did not experience a traumatic event had a higher SOC (t(231) = −3.12, p < 0.005) |
| Tselebis et al. 2001 | 79 nurses 62 females (78.5%) 17 males (21.5%) | Nurses working in general internal medicine, general surgery and respiratory medical wards in a major hospital | Greece | 37.7 (5.5) | 11.0 (6.3) | SOC-13 | 63.60 (11.70) | Cross-sectional study | Maslach Burnout Inventory (MBI) Beck’s Depression Inventory (BDI) | No differences in SOC between sexes nor marital status Inverse correlation between SOC and BDI (r = −0.58, p < 0.05) Correlation between SOC and MBI categories, negative correlation with sentimental exhaustion (r = −0.55, p < 0.05) and depersonalization (r = −0.45, p < 0.05), positive correlation with personal achievement (r = 0.44, p < 0.05) |
| Levert et al. 2000 | 94 nurses 67 females (71.3%) 27 male (28.7%) | Nurses working in psychiatric units | South Africa | 39 | -- | SOC-13 | 60.61 (12.42) | Cross-sectional study | Maslach Burnout Inventory (MBI) Work Load and Lack of Collegial Support. Role Conflict and Role Ambiguity | Correlation between SOC and MBI’s components: emotional exhaustion r = 0.41 (p < 0.0001) and depersonalization r = 0.36 (p > 0.001) SOC (t = 4.48; p.OOO) and work load (t = 4.50; p.OOO) together explain the majority of the variance in emotional exhaustion (36.6%) SOC (t = 3.51; p.OOl) and work load (t = 2.61; p.Oll) together explain the majority of the variance in depersonalization (21.3%) |
| Berg et al., 1999 | 22 nurses 16 females (72.7%) 6 male (27.3%) | Nurses working in psychiatric ward, during a year of systematic clinical supervision | Sweden | 39.7 (7.1) | 13.5 (8.3) | SOC-29 | T1: 146.6 (21.2) T2: 153.6 (18.3) | Pre-post-test design | Creative Climate questionnaire (CCQ) Work-related strain inventory (WRSI) Satisfaction with nursing care and work (SNCW) | Not significant Improvement in SOC scores at T1 and T2 Inverse correlation between SOC and WRSI (r = −0.48, p < 0.05) Inverse correlation between SOC and SNCW, factor involvement (r = −0.46, p < 0.05) |
| Shiu et al., 1998 | 20 nurses (all females) | Public health nurses (females, ≥ 1 children, promoted to nursing officer or in charge of a center, unit or team) Work perturbed by interruption signals | Hong Kong | 39 | -- | SOC-29 | 135.75 (12.27) | Cross-sectional study | Experience sampling diary (ESD) | Positive correlation between SOC and perceived goal progress and perceived control Low SOC group (scores <136) has a lower positive affect [t(323)= - 6.79, p < 0.001] and higher negative affect [t(321.98)= 2.88, p < 0.005], than the high SOC group (≥136) in response to interruption signals. |
| Pålsson et al., 1996 | 33 nurses (all females) | District nurses working in 10 primary health care districts Supervisory group (n=21): participation in a training program Comparison group (n = 12) | Sweden | Supervisory group: 49.0 (7.1) Comparison group: 46.3 (8.3) | Supervisory group -in nursing care 24.0 (8.2) -as district nurse 16.1 (6.5) Comparison group -in nursing care 21.8 (6.9) -as district nurse 14.0 (7.3) | SOC-29 | Supervisory group T1: 148 (17.5) T2: 151 (16.6) Comparison group T1: 154 (13.6) T2: 153 (17.3) | Pre-post test design, with control | Karolinska Scales of Personality (KSP) Burnout Measure Empathy Construct Rating Scale (ECRS) | Burnout, empathy and SOC scores are concordant in respect to the KSP variables Inverse correlation between SOC and KSP variables: somatic anxiety (r = −0.44, p < 0.05), impulsiveness (r = −0.40, p < 0.05), monotony avoidance (r = −0.42, p < 0.05), detachment (r = −0.44, p < 0.05), hostility (r = −0.37, p < 0.05) and psychasthenia (r = −0.40, p < 0.05) Positive correlation between SOC and KSP variable, socialization (r = 0.44, p < 0.01) Inverse correlation between SOC and burnout (r = −0.69, p < 0.001) Positive correlation between SOC and empathy (r = 0.76, p < 0.001) No significant change in burnout, empathy and SOC over time within the groups nor between the groups at T1 or at T2 |
| Lewis 1994 | 49 nurses (all female) | Nurses working in dialyses units | USA | 39.6 | -- | SOC-29 | 148.7 | Cross-sectional study | Perceived Stress Scale Nursing Stress Scale Coping Resources Inventory Myers-Briggs Type Indicator (MBTI) Maslach burnout inventory (MBI) | Inverse correlation between SOC and personal stress (r = −0.715) Inverse correlation between SOC and work stress (r = −0.436) Inverse correlation between SOC and burnout (r = −0.395) Positive correlation between SOC and total coping resources (r = 0.667) |
| Langius et al., 1992 | 57 nurses (all females) | Nurses participating in an in-house training program (total 5 groups) Sample 1 (n = 35): SOC through VAS format Sample 2 (n = 22): SOC and SMI through VAS format | Sweden | Sample 1: 41 Sample 2: 43 | -- | SOC-29 | Sample 1: 152 (17) Sample 2: 143 (17) | Cross-sectional study | Self-Motivation Inventory (SMI) | No differences in SOC scores means between the participating groups, who had questionnaire administered through different formats. Negative correlation between SOC and SMI (r = −0,685, p < 0.001) |
| Lewis 1991 | 238 nurses 224 females (94%) 14 males (6%) | Nurses working in dialysis units | USA | 36.1 | -- | SOC-29 | 143.1 | Cross-sectional study | Nursing stress scale Maslach Burnout inventory (MBI) | Men show lower SOC scores than women Inverse correlation between SOC and overall stress (r = −0.39) Correlation between SOC and burnout subscales (emotional exhaustion r = −0.57, depersonalization r = −0.54, personal accomplishment r = 0.53) No relationship between SOC and age, marital status, educational level, position, years in nursing, number of patients or shift unit, shift length or hours worked per week. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michele Masanotti, G.; Paolucci, S.; Abbafati, E.; Serratore, C.; Caricato, M. Sense of Coherence in Nurses: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 1861. https://doi.org/10.3390/ijerph17061861
Michele Masanotti G, Paolucci S, Abbafati E, Serratore C, Caricato M. Sense of Coherence in Nurses: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(6):1861. https://doi.org/10.3390/ijerph17061861
Chicago/Turabian StyleMichele Masanotti, Giuseppe, Silvia Paolucci, Elia Abbafati, Claudio Serratore, and Michela Caricato. 2020. "Sense of Coherence in Nurses: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 6: 1861. https://doi.org/10.3390/ijerph17061861
APA StyleMichele Masanotti, G., Paolucci, S., Abbafati, E., Serratore, C., & Caricato, M. (2020). Sense of Coherence in Nurses: A Systematic Review. International Journal of Environmental Research and Public Health, 17(6), 1861. https://doi.org/10.3390/ijerph17061861