
Effectiveness of Integrated Technology Apps for Supporting Healthy Food Purchasing and Consumption: A Systematic Review

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Searching Strategy
2.2. Eligibility Criteria
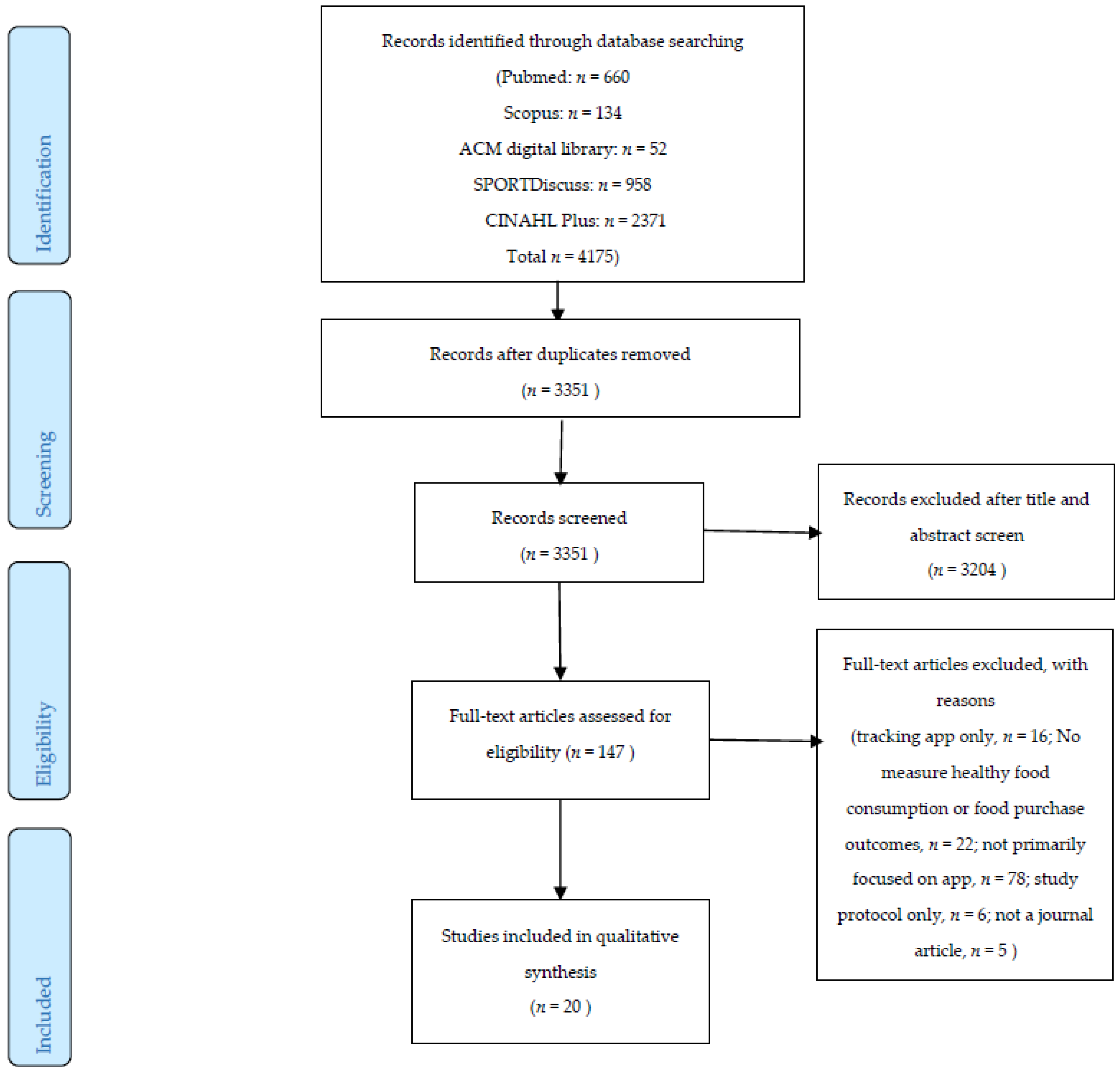
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Analysis
- Efficacy was defined as the ability to produce a desired or intended result [50].
- Technology apps were defined as applications for novel mobile consumer devices with a touchscreen, especially smartphones and tablet PCs [51]. In this review, the terms “app” is sued in the stricter sense with more on self-monitoring apps. Other technology interventions such as text messaging, social media (e.g., facebook), online coaching or telephone counseling were excluded in this review.
- Unhealthy foods were defined as those that were high in salt, sugar and saturated fats [2].
- Healthy foods were generally defined as the food meeting the nutrition standards promoting healthier foods that were low in sugar, salt and saturated fats, while promoting fruits and vegetables, whole grains and lean protein [2].
3. Results
3.1. Description of Included Studies
3.2. Characteristics of Included Studies
3.3. Quality Assessment
3.4. Healthy Food Purchasing and Its Measurement
3.5. Healthy Food Consumption and Its Measurement
3.6. Intervention Efficacy
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flaherty, S.J.; McCarthy, M.B.; Collins, A.M.; McCafferty, C.; McAuliffe, F.M. A phenomenological exploration of change towards healthier food purchasing behaviour in women from a lower socioeconomic background using a health app. Appetite 2020, 147, 104566. [Google Scholar] [CrossRef] [PubMed]
- Raine Kim, D.; Kayla, A.; Lee, D.L.D.; Ferdinands Alexa, R.; Dominique, B.; Susan, B.; Norm, C.; Brian, C.; L’Abbé Mary, L.A.; David, M. Healthy food procurement and nutrition standards in public facilities: Evidence synthesis and consensus policy recommendations. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2018, 38, 6. [Google Scholar] [CrossRef]
- Sandoval-Insausti, H.; Blanco-Rojo, R.; Graciani, A.; López-García, E.; Moreno-Franco, B.; Laclaustra, M.; Donat-Vargas, C.; Ordovás, J.M.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Ultra-processed Food Consumption and Incident Frailty: A Prospective Cohort Study of Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1126–1133. [Google Scholar] [CrossRef]
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Debras, C.; Druesne-Pecollo, N.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultraprocessed Food Consumption and Risk of Type 2 Diabetes Among Participants of the NutriNet-Santé Prospective Cohort. JAMA Intern Med. 2020, 180, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Zhong, G.C.; Gu, H.T.; Peng, Y.; Wang, K.; Wu, Y.Q.; Hu, T.Y.; Jing, F.C.; Hao, F.B. Association of ultra-processed food consumption with cardiovascular mortality in the US population: Long-term results from a large prospective multicenter study. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 21. [Google Scholar] [CrossRef]
- Lim, S.Y.; Zalilah, M.S.; Chin, Y.S.; Ramachandran, V.; Chan, Y.M. Dietary Acid Load, IGF-1 Single Nucleotide Polymorphism and Bone Resorption among Postmenopausal Chinese Women. Nutrients 2018, 10, 915. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of ultra-processed foods and health status: A systematic review and meta-analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. The Global Burden of Disease: Generating Evidence, Guiding Policy; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2013. [Google Scholar]
- Abdissa, D.; Dukessa, A.; Babusha, A. Prevalence and associated factors of overweight/obesity among type2 diabetic outpatients in Southwest Ethiopia. Heliyon 2021, 7, e06339. [Google Scholar] [CrossRef]
- Lee, J.; Shin, A.; Cho, S.; Choi, J.-Y.; Kang, D.; Lee, J.-K. Marital status and the prevalence of obesity in a Korean population. Obes. Res. Clin. Pract. 2020, 14, 217–224. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, Z.; Wang, X.; Chen, Z.; Shao, L.; Tian, Y.; Zheng, C.; Li, S.; Zhu, M.; Gao, R. Prevalence of overweight and obesity in China: Results from a cross-sectional study of 441 thousand adults, 2012–2015. Obes. Res. Clin. Pract. 2020, 14, 119–126. [Google Scholar] [CrossRef]
- Scott-Sheldon, L.A.; Lantini, R.C.; Jennings, E.G.; Thind, H.; Rosen, R.K.; Salmoirago-Blotcher, E.; Bock, B.C. Text messaging-based interventions for smoking cessation: A systematic review and meta-analysis. JMIR mHealth uHealth 2016, 4, e49. [Google Scholar] [CrossRef]
- Vodopivec-Jamsek, V.; de Jongh, T.; Gurol-Urganci, I.; Atun, R.; Car, J. Mobile phone messaging for preventive health care. Cochrane Database Syst. Rev. 2012, 12. [Google Scholar] [CrossRef]
- Reid, A.J. A brief history of the smartphone. In The Smartphone Paradox; Springer: Berlin, Germany, 2018; pp. 35–66. [Google Scholar]
- Chmurzynska, A.; Mlodzik-Czyzewska, M.A.; Malinowska, A.M.; Czarnocinska, J.; Wiebe, D.J. Use of a smartphone application can improve assessment of high-fat food consumption in overweight individuals. Nutrients 2018, 10, 1692. [Google Scholar] [CrossRef] [PubMed]
- Wharton, C.M.; Johnston, C.S.; Cunningham, B.K.; Sterner, D. Dietary self-monitoring, but not dietary quality, improves with use of smartphone app technology in an 8-week weight loss trial. J. Nutr. Educ. Behav. 2014, 46, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Vasiloglou, M.F.; Christodoulidis, S.; Reber, E.; Stathopoulou, T.; Lu, Y.; Stanga, Z.; Mougiakakou, S. What healthcare professionals think of “nutrition & diet” apps: An international survey. Nutrients 2020, 12, 2214. [Google Scholar]
- Spring, B.; Pellegrini, C.A.; Pfammatter, A.; Duncan, J.M.; Pictor, A.; McFadden, H.G.; Siddique, J.; Hedeker, D. Effects of an abbreviated obesity intervention supported by mobile technology: The ENGAGED randomized clinical trial. Obesity 2017, 25, 1191–1198. [Google Scholar] [CrossRef]
- Recio-Rodriguez, J.I.; Agudo Conde, C.; Calvo-Aponte, M.J.; Gonzalez-Viejo, N.; Fernandez-Alonso, C.; Mendizabal-Gallastegui, N.; Rodriguez-Martin, B.; Maderuelo-Fernandez, J.A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A. The effectiveness of a smartphone application on modifying the intakes of macro and micronutrients in primary care: A randomized controlled trial. The EVIDENT II study. Nutrients 2018, 10, 1473. [Google Scholar] [CrossRef]
- Avila-Garcia, P.; Hernandez-Ramos, R.; Nouri, S.S.; Cemballi, A.; Sarkar, U.; Lyles, C.R.; Aguilera, A. Engaging users in the design of an mHealth, text message-based intervention to increase physical activity at a safety-net health care system. JAMIA Open 2019, 2, 489–497. [Google Scholar] [CrossRef]
- Bakırcı-Taylor, A.L.; Reed, D.B.; McCool, B.; Dawson, J.A. mHealth improved fruit and vegetable accessibility and intake in young children. J. Nutr. Educ. Behav. 2019, 51, 556–566. [Google Scholar] [CrossRef]
- Spring, B.; Pellegrini, C.; McFadden, H.; Pfammatter, A.F.; Stump, T.K.; Siddique, J.; King, A.C.; Hedeker, D. Multicomponent mHealth intervention for large, sustained change in multiple diet and activity risk behaviors: The make better choices 2 randomized controlled trial. J. Med. Internet Res. 2018, 20, e10528. [Google Scholar] [CrossRef]
- Ramsey, A.T. Integration of technology-based behavioral health interventions in substance abuse and addiction services. Int. J. Ment. Health Addict. 2015, 13, 470–480. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Allen, J.K.; Stephens, J.; Dennison Himmelfarb, C.R.; Stewart, K.J.; Hauck, S. Randomized controlled pilot study testing use of smartphone technology for obesity treatment. J. Obes. 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Murphy, S.; Moylan, J.; Evensen, D.; Curb, J.D. Improving dietary self-monitoring and adherence with hand-held computers: A pilot study. Am. J. Health Promot. 2006, 20, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Turner-McGrievy, G.M.; Beets, M.W.; Moore, J.B.; Kaczynski, A.T.; Barr-Anderson, D.J.; Tate, D.F. Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mHealth weight loss program. J. Am. Med. Inform. Assoc. 2013, 20, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; Pernal, W.; Matsumoto, A.; Shiyko, M.; Intille, S.; Franko, D.L. Capitalizing on mobile technology to support healthy eating in ethnic minority college students. J. Am. Coll. Health 2016, 64, 125–132. [Google Scholar] [CrossRef]
- Park, Y.-J.; Lee, S.-J.; Shin, N.-M.; Shin, H.; Jeon, S.; Lee, J.; Cho, I. Application and Effect of Mobiletype-Bone Health Intervention in Korean Young Adult Women with Low Bone Mass: A Randomized Control Trial. Asian Nurs. Res. 2017, 11, 56–64. [Google Scholar] [CrossRef]
- Eyles, H.; McLean, R.; Neal, B.; Jiang, Y.; Doughty, R.N.; McLean, R.; Ni Mhurchu, C. A salt-reduction smartphone app supports lower-salt food purchases for people with cardiovascular disease: Findings from the SaltSwitch randomised controlled trial. Eur. J. Prev. Cardiol. 2017, 24, 1435–1444. [Google Scholar] [CrossRef]
- Inauen, J.; Bolger, N.; Shrout, P.E.; Stadler, G.; Amrein, M.; Rackow, P.; Scholz, U. Using smartphone-based support groups to promote healthy eating in daily life: A randomised trial. Appl. Psychol. Health Well Being 2017, 9, 303–323. [Google Scholar] [CrossRef]
- Järvelä-Reijonen, E.; Karhunen, L.; Sairanen, E.; Muotka, J.; Lindroos, S.; Laitinen, J.; Puttonen, S.; Peuhkuri, K.; Hallikainen, M.; Pihlajamäki, J. The effects of acceptance and commitment therapy on eating behavior and diet delivered through face-to-face contact and a mobile app: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–14. [Google Scholar] [CrossRef]
- Sarcona, A.; Kovacs, L.; Wright, J.; Williams, C. Differences in eating behavior, physical activity, and health-related lifestyle choices between users and nonusers of mobile health apps. Am. J. Health Educ. 2017, 48, 298–305. [Google Scholar] [CrossRef]
- Lee, K.-W.; Kim, H.-B.; Lee, S.-H.; Ha, H.-K. Changes in weight and health-related behavior using smartphone applications in patients with colorectal polyps. J. Nutr. Educ. Behav. 2019, 51, 539–546. [Google Scholar] [CrossRef]
- Porter, J.; Huggins, C.E.; Truby, H.; Collins, J. The effect of using mobile technology-based methods that record food or nutrient intake on diabetes control and nutrition outcomes: A systematic review. Nutrients 2016, 8, 815. [Google Scholar] [CrossRef]
- Müller, A.M.; Alley, S.; Schoeppe, S.; Vandelanotte, C. The effectiveness of e-& mHealth interventions to promote physical activity and healthy diets in developing countries: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–14. [Google Scholar]
- McCarroll, R.; Eyles, H.; Mhurchu, C.N. Effectiveness of mobile health (mHealth) interventions for promoting healthy eating in adults: A systematic review. Prev. Med. 2017, 105, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Poly, T.N.; Walther, B.A.; Li, Y.-C.J. Use of mobile phone app interventions to promote weight loss: Meta-analysis. JMIR mHealth uHealth 2020, 8, e17039. [Google Scholar] [CrossRef]
- Greenwood, D.A.; Gee, P.M.; Fatkin, K.J.; Peeples, M. A Systematic Review of Reviews Evaluating Technology-Enabled Diabetes Self-Management Education and Support. J. Diabetes Sci. Technol. 2017, 11, 1015–1027. [Google Scholar] [CrossRef]
- Hammersley, M.L.; Jones, R.A.; Okely, A.D. Parent-Focused Childhood and Adolescent Overweight and Obesity eHealth Interventions: A Systematic Review and Meta-Analysis. J. Med. Internet Res. 2016, 18, e203. [Google Scholar] [CrossRef] [PubMed]
- Stephens, J.; Allen, J. Mobile phone interventions to increase physical activity and reduce weight: A systematic review. J. Cardiovasc. Nurs. 2013, 28, 320. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.G.; Bond, D.S. Review of innovations in digital health technology to promote weight control. Curr. Diabetes Rep. 2014, 14, 485. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.K.; Kwak, S.H.; Jung, H.S.; Koo, B.K.; Moon, M.K.; Lim, S.; Jang, H.C.; Park, K.S.; Cho, Y.M. The effect of a smartphone-based, patient-centered diabetes care system in patients with type 2 diabetes: A randomized, controlled trial for 24 weeks. Diabetes Care 2019, 42, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Whittaker, R.; Jiang, Y.; Maddison, R.; Shepherd, M.; McNamara, C.; Cutfield, R.; Khanolkar, M.; Murphy, R. Effectiveness of text message based, diabetes self management support programme (SMS4BG): Two arm, parallel randomised controlled trial. BMJ 2018, 361, k1959. [Google Scholar] [CrossRef] [PubMed]
- Bovi, A.P.D.; Cesari, G.M.; Rocco, M.C.; Michele, L.D.; Rimauro, I.; Lugiero, A.; Mottola, S.; Anseris, A.G.E.D.; Nazzaro, L.; Massa, G. Healthy Lifestyle Management of Pediatric Obesity with a Hybrid System of Customized Mobile Technology: The PediaFit Pilot Project. Nutrients 2021, 13, 631. [Google Scholar] [CrossRef]
- Whitelock, V.; Kersbergen, I.; Higgs, S.; Aveyard, P.; Halford, J.C.; Robinson, E. User Experiences of a Smartphone-Based Attentive Eating App and Their Association with Diet and Weight Loss Outcomes: Thematic and Exploratory Analyses From a Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e16780. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.; Chaboyer, W.; Hopper, Z.; Marshall, A.P. Using Technology to Promote Patient Engagement in Nutrition Care: A Feasibility Study. Nutrients 2021, 13, 314. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.Y.; Nordin, S.A.; Mohamed, N.A.; Zainudin, N.F. Effectiveness of Integrated Technology Apps for Supporting Healthy Food Purchasing and Consumption: A Systematic Review. PROSPERO 2020 CRD42020218742: 2020. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=218742 (accessed on 1 May 2021).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N.; Group, T. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: The TREND statement. Am. J. Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef]
- Oxford Dictionaries. Definition of Efficacy in English. 2021. Available online: https://en.oxforddictionaries.com/definition/efficacy (accessed on 26 March 2021).
- Gröger, C.; Silcher, S.; Westkämper, E.; Mitschang, B. Leveraging apps in manufacturing. A framework for app technology in the enterprise. Procedia CIRP 2013, 7, 664–669. [Google Scholar] [CrossRef]
- Atienza, A.A.; King, A.C.; Oliveira, B.M.; Ahn, D.K.; Gardner, C.D. Using hand-held computer technologies to improve dietary intake. Am. J. Prev. Med. 2008, 34, 514–518. [Google Scholar] [CrossRef]
- McCarroll, M.L.; Armbruster, S.; Pohle-Krauza, R.J.; Lyzen, A.M.; Min, S.; Nash, D.W.; Roulette, G.D.; Andrews, S.J.; von Gruenigen, V.E. Feasibility of a lifestyle intervention for overweight/obese endometrial and breast cancer survivors using an interactive mobile application. Gynecol. Oncol. 2015, 137, 508–515. [Google Scholar] [CrossRef]
- Palacios, C.; Torres, M.; López, D.; Trak-Fellermeier, M.A.; Coccia, C.; Pérez, C.M. Effectiveness of the nutritional app “mynutricart” on food choices related to purchase and dietary behavior: A pilot randomized controlled trial. Nutrients 2018, 10, 1967. [Google Scholar] [CrossRef]
- Huberty, J.; Green, J.; Glissmann, C.; Larkey, L.; Puzia, M.; Lee, C. Efficacy of the mindfulness meditation mobile app “calm” to reduce stress among college students: Randomized controlled trial. JMIR mHealth uHealth 2019, 7, e14273. [Google Scholar] [CrossRef] [PubMed]
- Dodd, J.M.; Louise, J.; Cramp, C.; Grivell, R.M.; Moran, L.J.; Deussen, A.R. Evaluation of a smartphone nutrition and physical activity application to provide lifestyle advice to pregnant women: The SNAPP randomised trial. Matern. Child Nutr. 2018, 14, e12502. [Google Scholar] [CrossRef] [PubMed]
- Brindal, E.; Hendrie, G.A.; Freyne, J.; Noakes, M. A mobile phone app designed to support weight loss maintenance and well-being (motimate): Randomized controlled trial. JMIR mHealth uHealth 2019, 7, e12882. [Google Scholar] [CrossRef] [PubMed]
- Gill, D.; Blunt, W.; Silva, N.B.S.; Stiller-Moldovan, C.; Zou, G.; Petrella, R. The Health e Steps™ lifestyle prescription program to improve physical activity and modifiable risk factors for chronic disease: A pragmatic randomized controlled trial. BMC Public Health 2019, 19, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, P.; Mendu, V.V.R.; Korrapati, D.; Gavaravarapu, S.M. Calorie counting smart phone apps: Effectiveness in nutritional awareness, lifestyle modification and weight management among young Indian adults. Health Inform. J. 2020, 26, 816–828. [Google Scholar] [CrossRef]
- Alnasser, A.; Kyle, J.; Al-Khalifa, A.; Marais, D. The ‘Twazon’Arabic weight loss app intervention for Saudi women with obesity and overweight: A feasibility study. JMIR mHealth uHealth 2019, 7, e10923. [Google Scholar] [CrossRef]
- Flecha, O.D.; Douglas de Oliveira, D.W.; Marques, L.S.; Gonçalves, P.F. A commentary on randomized clinical trials: How to produce them with a good level of evidence. Perspect. Clin. Res. 2016, 7, 75–80. [Google Scholar] [CrossRef]
- Dennison, L.; Morrison, L.; Conway, G.; Yardley, L. Opportunities and challenges for smartphone applications in supporting health behavior change: Qualitative study. J. Med. Internet Res. 2013, 15, e86. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Bacao, F. What factors determining customer continuingly using food delivery apps during 2019 novel coronavirus pandemic period? Int. J. Hosp. Manag. 2020, 91, 102683. [Google Scholar] [CrossRef] [PubMed]
- Zarnowiecki, D.; Mauch, C.E.; Middleton, G.; Matwiejczyk, L.; Watson, W.L.; Dibbs, J.; Dessaix, A.; Golley, R.K. A systematic evaluation of digital nutrition promotion websites and apps for supporting parents to influence children’s nutrition. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 17. [Google Scholar] [CrossRef]
- Husain, I.; Spence, D. Can healthy people benefit from health apps? BMJ 2015, 350, h2520. [Google Scholar] [CrossRef][Green Version]
- Schoeppe, S.; Alley, S.; Van Lippevelde, W.; Bray, N.A.; Williams, S.L.; Duncan, M.J.; Vandelanotte, C. Efficacy of interventions that use apps to improve diet, physical activity and sedentary behaviour: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–26. [Google Scholar] [CrossRef]
- Rodrigues, A.L.; Ball, J.; Ski, C.; Stewart, S.; Carrington, M.J. A systematic review and meta-analysis of primary prevention programmes to improve cardio-metabolic risk in non-urban communities. Prev. Med. 2016, 87, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Appleton, K.M.; Hemingway, A.; Saulais, L.; Dinnella, C.; Monteleone, E.; Depezay, L.; Morizet, D.; Perez-Cueto, F.A.; Bevan, A.; Hartwell, H. Increasing vegetable intakes: Rationale and systematic review of published interventions. Eur. J. Nutr. 2016, 55, 869–896. [Google Scholar] [CrossRef] [PubMed]
- Greaves, C.J.; Sheppard, K.E.; Abraham, C.; Hardeman, W.; Roden, M.; Evans, P.H.; Schwarz, P. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Andone, I.; Błaszkiewicz, K.; Eibes, M.; Trendafilov, B.; Montag, C.; Markowetz, A. How age and gender affect smartphone usage. In Proceedings of the 2016 ACM International Joint Conference on Pervasive and Ubiquitous Computing: Adjunct, Heidelberg, Germany, 12–16 September 2016; pp. 9–12. [Google Scholar]
- Sutton, K.; Caldwell, J.; Yoshida, S.; Thompson, J.; Kuo, T. Healthy food marketing and purchases of fruits and vegetables in large grocery stores. Prev. Med. Rep. 2019, 14, 100861. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, S.I.; Dodd, K.W.; Reedy, J.; Krebs-Smith, S.M. Income and race/ethnicity are associated with adherence to food-based dietary guidance among US adults and children. J. Acad. Nutr. Diet. 2012, 112, 624–635.e626. [Google Scholar] [CrossRef]
- Best, M.; Papies, E.K. Lower socioeconomic status is associated with higher intended consumption from oversized portions of unhealthy food. Appetite 2019, 140, 255–268. [Google Scholar] [CrossRef]
- Flaherty, S.J.; McCarthy, M.B.; Collins, A.M.; McAuliffe, F.M. A different perspective on consumer engagement: Exploring the experience of using health apps to support healthier food purchasing. J. Mark. Manag. 2019, 35, 310–337. [Google Scholar] [CrossRef]
- Morrison, A.; Polisena, J.; Husereau, D.; Moulton, K.; Clark, M.; Fiander, M.; Mierzwinski-Urban, M.; Clifford, T.; Hutton, B.; Rabb, D. The effect of English-language restriction on systematic review-based meta-analyses: A systematic review of empirical studies. Int. J. Technol. Assess. Health Care 2012, 28, 138. [Google Scholar] [CrossRef]


{kind=link}
| Search Category | Search Terms |
|---|---|
| Apps | Application* OR app* OR smartphone* OR “smart phone*” OR “cellular phone*” OR “mobile phone*” OR “mobile telephone*” OR tablet* OR “e-learning” OR “e-health” OR “iPad*” OR “mobile health” OR “social media” |
| Food purchasing and Food consumption | “food purchasing” OR “food purchase*” OR “food choice*” OR “food planning” OR “food shopping” OR “food consumption*” OR “food intake*” OR “dietary intake*” OR “healthy eating” OR “eating behaviour*” OR “healthy food” OR “food behaviour*” OR “food value*” OR “food diary” OR “food diaries” OR “nutrition assessment*” OR “diet record*” OR “diet survey*” OR “energy intake*” OR “nutrition survey*” OR “dietary assessment*” |
| Intervention | Intervention* OR program* OR programme* OR “health promotion*” OR trial* OR effectiveness |
| Domain | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| 1. Publication year | Studies published between 1 January 2006 and 31 December 2020. | Studies published before or after the inclusion dates. |
| 2. Publication type | Original studies published in peer-reviewed journals only. | Letters, commentaries, conference proceedings, reviews, narrative articles or other materials that was not a peer-reviewed primarily study. |
| 3. Language | Studies limited to English-language publications. | Studies were not published in English. |
| 4. Targeted population | Any population. | No restriction on population. |
| 5. Targeted group | Adults who are aged 18 or above. | Children or adolescents below 18 years old. |
| 6. Research design | Quantitative studies involved experimental and cross-sectional study design. | Qualitative study or any non-experimental study designs were utilised (e.g., protocol, studies reporting prevalence or trend data, feasibility studies, measurement studies or theoretical papers). |
| 7. Study scope/variables | (1) Technology apps [e.g., smartphone or personal digital assistant (PDA)] in an intervention to improve healthy food purchasing and consumption for prevention. (2) Interventions could be stand-alone interventions using an app only, or multi-component interventions including an app as one of several intervention components (e.g., physical education, face-to-face counselling) with the condition that individual apps record was provided. (3) All types and units of measurements for the healthy food purchasing and consumption outcomes were acceptable (e.g., food group, self-report, servings, calories, kilograms, nutrition assessment). (4) reported data regarding efficacy for behaviour change (e.g., change in healthy food groups). (5) Interventions covering aspects of large-scale management of food (retail, restaurants, public preparation and consumption of food in school kitchens, hospitals, etc.). | (1) tracking app only but not focused on apps intervention on food purchasing or food consumption. (2) Other technology intervention than apps intervention (e.g., text messaging, apps, social media, telephone counselling or online coaching). (3) No measure of healthy food purchasing or food consumption outcomes. |
| First Author (Year), Country | Study Name/Apps Name | Device | Study Design | Sample Characteristics, Mean Age | Female (%) | Grouping | Intervention Time Frame | Outcomes and Measures | Findings | Quality |
|---|---|---|---|---|---|---|---|---|---|---|
| Allen (2013), USA [24] | SLIM (Smart coach for LIfestyleManagement) study | smartphone | RCT | 68 obese adults | 78% | (1) intensive counseling intervention, (2) intensive counseling + smartphone intervention, (3) a less intensive counseling + smartphone intervention, and (4) smartphone intervention only | baseline and 6-month | self-reported dietary intake | Not significant. | Poor |
| Alnasser (2019), Saudi Arabia [60] | Twazon app. | smartphone | pre-post single-arm pilot study | 40 overweight adult; engaged: n = 26, age = 31 years, Unengaged: n = 14, age = 31 years | 100% | engaged users (65%) and unengaged users (35%) | baseline, 2- and 4-months | Dietary intake | The daily energy consumption was decreased by >600 calories in the engaged users group compare with the unengaged group. | Poor |
| Atienza (2008), USA [52] | NR | PDA | RCT | 27 healthy mid-life and older adults (≥50 years); AG: n = 16, age = 63 years; CG: n = 11, age = 58 years | AG: 69% CG: 70% | PDA program vs. control | baseline and 8 weeks | vegetable and whole-grain intake | Intervention participants reported significantly greater increases in vegetable servings and dietary fibre from grains. | Poor |
| Banerjee (2020), India [59] | S Health®, Calorie Counter—MyFitnessPal®, and Calorie Counter | smartphone | prospective controlled trial | 58 healthy young adults (18–45 years); AP: n = 30; CG: n = 28 | AG: 63%; CG: 46% | apps group vs. control | baseline and 8 weeks | Food consumption | Not significant. | Poor |
| Brindal (2019), Australia [57] | MotiMate | smartphone | RCT | 88 healthly adults; AG: n = 45, age = 45 years; CG: n = 43, age = 46 years | AG:75%; CG: 69% | intervention app (MotiMate) vs. control app | baseline, 4, 8, 12 and 24 weeks | healthy eating | Not significant. | Poor |
| Dodd (2017), Australia [56] | SNAPP trial | smartphone | RCT | 162 healthy pregnant women; AG: n = 77, age = 31 years; CG: n = 85, age = 31 years | 100% | Lifestyle Advice + Smartphone App vs. Lifestyle Advice Only | baseline, 28 and 36 weeks | healthy eating index (HEI) | Not significant. | Good |
| Eyles (2017), New Zealand [29] | SaltSwitch | smartphone | RCT | 66 adults with diagnosed cardiovascular disease; AG: n = 33, age = 64 years; CG: n = 33, age = 65 years | AG:9%; CG: 24% | SaltSwitch app vs. control group (usual care). | baseline and 4 weeks | (1) salt content of household packaged food purchases (2) saturated fat content (g/MJ), energy content (kJ/kg) and expenditure (NZ$) of household food purchases | A significant reduction in mean household purchases of salt was observed. Not significant for the second outcome. | Good |
| Gill (2019), Canada [58] | HealtheSteps™ | smartphone | RCT | 118 adults at risk or diagnosed with a chronic disease; AG: n= 59, age = 57 years; CG: n = 59, age = 59 years | AG:76%; CG: 81% | HealtheSteps™ smartphone app and Healthe-Steps™ website vs. wait-list control | baseline and 18 months. | self-reported eating habits | Improved their overall healthful eating | Good |
| Glanz (2006), USA [25] | NR | PDA | Intervention pilot test | 33 healthy women, 64 years | 100% | PDA diet-monitoring system | baseline and 1 month | food choice and dietary intakes | Reported total fat intake and percent energy from fat decreased significantly. | Poor |
| Huberty (2019). USA [55] | Calm | smartphone | RCT | 88 healthy adult; AG: n = 41, age = 20 years; CG: n = 47, age = 22 years | AG:41%; CG: 49% | Calm app vs. wait-list control | baseline, 8 and 12 weeks | alcohol consumption and healthy eating (fruit and vegetable consumption) | Not significant. | Poor |
| Inauen (2017), USA [30] | NR | smartphone | RCT | 140 healthy adult; AG: n = 70, age 27.5 years; CG: n = 70. Age = 27.5 years | 75.5% | Whatsapp support group (1. eating more fruit and vegetables 2. eating fewer unhealthy snacks) vs. control | baseline, 1- and 2-months | Self-reported healthy eating (fruits, vegetables and unhealthy snacks) | Intervention group showed a gradual increase in healthy eating over time, ate more fruits and vegetables, and less unhealthy snacks compare to the control group on Day 10. However, it is not significant at the follow ups. | Poor |
| Jarvela (2018), Finland [31] | NR | smartphone | RCT | 219 healthy adult; face to face group: n = 70, age = 50 years; AG: n = 78, age = 49; CG: n = 71, age = 49 years | (1) Face-to-face: 87% (2) AG: 85% 3) CG: 82% | (1) Face-to-face (2) mobile app (3) control | baseline, 10 and 36 weeks | eating behaviour | App group showed beneficial effects on reported eating behaviour. | Poor |
| Lee (2019), Korea [33] | NR | smartphone | RCT pilot test | 65 adult who diagnosis of colorectal polyps; AG: n = 32, age = 49 years; CG: n = 33, age 21 years | AG:34%; CG: 46% | intervention app vs. control (traditional mail) | baseline and 3 month | changes in dietary intake, such as that of vegetables, fruits, and fatty food. | Not significant. | Poor |
| McCarroll (2015), USA [53] | LoseIt! | smartphone | Prospective intervention | 50 adult women cancer survivors, age = 58 years | 100% | web- or mobile-based apps | baseline and 4 weeks | macronutrient (carbohydrate, fat and protein) and fibre consumption | Not significant. | Poor |
| Palacios (2018), USA [54] | MyNutriCart | smartphone | pilot randomised trial | 51 overweight and obese adult; AG: n = 24, age = 34 years; TG: n = 27, age = 37 years | AG:92%; TG: 89% | intervention app vs. face-to-face counseling session | baseline and 8 weeks. | healthy food choice and dietary behaviour | “MyNutriCart” app use led to significant improvements in food-related behaviours compared to baseline, with no significant differences when compared to the traditional group. | Poor |
| Park (2016), Korea [28] | Strong bone, Fit body (SbFb) | smartphone | RCT | 82 young adult women with low bone mass; AG: n = 28, age = 24 years; Group education: n = 32, age = 25 years; CG: n = 22, age = 23 years | 100% | (1) apps (2) group education (3) control | baseline and 20 weeks | nutrient intake | calcium intake is higher in app and group education than control group. | Poor |
| Recio-Rodriguez (2018), Spain [19] | EVIDENT II study | smartphone | RCT | 833 healthy adult; AG: n = 415, age = 51 years; CG: n = 418, age = 52 years | AG:60%; CG: 64% | intervention: counseling + application group; control: counseling group | baseline and 12-month | Macro and Micronutrients intake | The app group reported a higher percentage intake of carbohydrates, and lower percentage intakes of fats and saturated fats | Good |
| Rodgers (2015), France [27] | NR | smartphone | Intervention only | 40 healthy female adults, age = 19 years | 100% | intervention: app (food journal + messages) | baseline and 3 weeks | fruit, vegetable, and sugar-sweetened beverage consumption. | Among participants with body mass index (BMI) ≥25, fruit and vegetable consumption increased with time. Among participants with BMI <21, consumption of fruit decreased, whereas the consumption of vegetables remained stable. No effects were found for sugar-sweetened beverage consumption. | Poor |
| Sarcona (2017), USA [32] | NR | smartphone | cross-sectional study | 401 university students | 73% | Users and Nonusers of Mobile Health Apps | NA | healthy eating behaviour | App users were found to have more positive eating behaviours than nonusers, and the impact of using more than one type of mobile-based health app significantly improved eating behaviour. | Poor |
| Turner (2013), USA [26] | Fat Secret’s Calorie Counter, My Fitness Pal, and Lose it | smartphone | RCT | 78 overweight and obese adult; AG: n = 37, age = 41 years; website: n = 24, age = 45 years; paper journal: n = 17, age = 47 years; | AG: 70%; website: 87%; paper journal: 76%; | (1) mobile app, (2) website, and (3) paper journal | baseline and 6 months | dietary intake (energy intake, fat, added sugar, fruit, vegetables) and eating behaviour | App users consumed less energy than paper journal users. No significant difference on the dietary intake and eating behaviour. | Poor |
| Study | Healthy Food Purchasing | Healthy Food Consumption | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Energy Intake | Carbohydrate | Protein | Fat | Micronutrients | Grains | Vegetables | Fruits | Fibre | Added Sugar | Salt | Unhealthy Snack | Healthy Eating Index | Healthy Eating Behaviour | ||
| Allen (2013) [10] | 0 | 0 | 0 | 0 | 0 | ||||||||||
| Alnasser (2019) [39] | + (b) | 0 | 0 | + (b), | + (b), | + (w) | + (w) | ||||||||
| Atienza (2008) [30] | + (b) | + (b) | + (b) | ||||||||||||
| Banerjee (2020) [38] | 0 | 0 | 0 | ||||||||||||
| Brindal (2019) [35] | 0 | 0 | 0 | 0 | 0 | ||||||||||
| Dodd (2017) [34] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Eyles (2017) [15] | + (b) (salt content); 0 (saturated fat, energy content and expenditure) | ||||||||||||||
| Gill (2019) [37] | 0 | 0 | 0 | 0 | + (b) | ||||||||||
| Glanz (2006) [11] | + (b) | + (b) | 0 | 0 | 0 | 0 | |||||||||
| Huberty (2019) [33] | 0 | 0 | |||||||||||||
| Inauen (2017) [16] | + (b) (at day 10); 0 (at 2 months) | + (b) (at day 10); 0 (at 2 months) | + (b) (at day 10); 0 (at 2 months) | + (b) (at day 10); 0 (at 2 months) | |||||||||||
| Jarvela (2018) [17] | + (b) | ||||||||||||||
| Lee (2019) [19] | + (w) | + (w) | + (w) | ||||||||||||
| McCarroll (2015) [31] | 0 | 0 | 0 | 0 | 0 | ||||||||||
| Palacios (2018) [32] | + (w) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | + (b) | |||||
| Park (2016) [14] | 0 | 0 | 0 | 0 | + (b) | 0 | |||||||||
| Recio-Rodriguez (2018) [36] | + (w) | + (b), + (w) | 0 | + (b), + (w) | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Rodgers (2015), (participants with BMI ≥25) [13] | + (b) | + (b) | 0 | ||||||||||||
| Rodgers (2015) (participants with BMI <21) [13] | 0 | − (b) | 0 | ||||||||||||
| Sarcona (2017) [18] | + (b) | ||||||||||||||
| Turner (2013) [12] | + (b) | 0 | 0 | 0 | 0 | 0 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, S.Y.; Lee, K.W.; Seow, W.-L.; Mohamed, N.A.; Devaraj, N.K.; Amin-Nordin, S. Effectiveness of Integrated Technology Apps for Supporting Healthy Food Purchasing and Consumption: A Systematic Review. Foods 2021, 10, 1861. https://doi.org/10.3390/foods10081861
Lim SY, Lee KW, Seow W-L, Mohamed NA, Devaraj NK, Amin-Nordin S. Effectiveness of Integrated Technology Apps for Supporting Healthy Food Purchasing and Consumption: A Systematic Review. Foods. 2021; 10(8):1861. https://doi.org/10.3390/foods10081861
Chicago/Turabian StyleLim, Sook Yee, Kai Wei Lee, Wen-Li Seow, Nurul Azmawati Mohamed, Navin Kumar Devaraj, and Syafinaz Amin-Nordin. 2021. "Effectiveness of Integrated Technology Apps for Supporting Healthy Food Purchasing and Consumption: A Systematic Review" Foods 10, no. 8: 1861. https://doi.org/10.3390/foods10081861
APA StyleLim, S. Y., Lee, K. W., Seow, W.-L., Mohamed, N. A., Devaraj, N. K., & Amin-Nordin, S. (2021). Effectiveness of Integrated Technology Apps for Supporting Healthy Food Purchasing and Consumption: A Systematic Review. Foods, 10(8), 1861. https://doi.org/10.3390/foods10081861