Abstract
Interventional oncology (IO) is the field of Interventional Radiology that provides minimally invasive procedures under imaging guidance for the diagnosis and treatment of malignant tumors. Sophisticated devices can be utilized to increase standardization, accuracy, outcomes, and “repeatability” in performing percutaneous Interventional Oncology techniques. These technologies can reduce variability, reduce human error, and outperform human hand-to-eye coordination and spatial relations, thus potentially normalizing an otherwise broad diversity of IO techniques, impacting simulation, training, navigation, outcomes, and performance, as well as verification of desired minimum ablation margin or other measures of successful procedures. Stereotactic navigation and robotic systems may yield specific advantages, such as the potential to reduce procedure duration and ionizing radiation exposure during the procedure and, at the same time, increase accuracy. Enhanced accuracy, in turn, is linked to improved outcomes in many clinical scenarios. The present review focuses on the current role of percutaneous navigation systems and robotics in diagnostic and therapeutic Interventional Oncology procedures. The currently available alternatives are presented, including their potential impact on clinical practice as reflected in the peer-reviewed medical literature. A review of such data may inform wiser investment of time and resources toward the most impactful IR/IO applications of robotics and navigation to both standardize and address unmet clinical needs.
1. Introduction
Percutaneous interventions in Interventional Oncology require precision and accuracy to maximize safety and efficacy while keeping radiation dose and procedure time as low as possible. The evolution of hardware, computer science tools, computational power, navigation, imaging, and robotic technology has improved the targeting and treatment of small and difficult-to-reach lesions with minimally invasive image-guided therapies. Navigation and robotic guidance systems have increasingly been used in IO, aiming not only to improve precision and safety but also to minimize the effects of operator skill and experience variabilities while reducing radiation exposure. These systems have been studied in multiple phases of development and in a variety of percutaneous image-guided therapy applications, including tumor biopsy and ablation, drainage, vertebroplasty, drilling of osteochondral lesions [1], percutaneous pelvic fracture fixation [2], as well as nerve and facet blocks and neurolysis [3,4,5,6]. Most systems available in the market are designed for percutaneous non-vascular applications with a spectrum of image guidance modalities, including computed tomography (CT), cone beam CT (CBCT), magnetic resonance imaging (MRI), positron emission tomography (PET), fluoroscopy, ultrasonography either independently, or a combination by the application of fusion imaging tools. Depending on the system and role of the operator, the interventional procedure can be performed in an autonomous or semiautonomous way, with the potential for remote operation. Navigation and robotic systems can be patient, ceiling, floor, or table-mounted and can interface with imaging systems as plug-in add-ons, with a spectrum from autonomous to completely integrated architecture.
Presently, percutaneous ablation is usually applied with a curative intent, aiming to provide local tumor control in a wide variety of both primary and metastatic tumors. In such cases, ablation with clear margins (AO) improves technical and clinical efficacy as well as local control and oncologic outcomes. Pre-requisites for a successful ablation procedure include proper selection of lesions and patients, as well as real-time imaging confirmation of margins, which implements and necessitates three-dimensional software technology [7,8,9,10].
The present narrative review paper focuses on the current role of percutaneous navigation systems and robotics in Interventional Oncology procedures. The currently available alternatives are reviewed, including their impact on clinical practice, as shown in published clinical experience. This is not a systematic review of the literature. We conducted the search in three databases (Pubmed/MEDLINE, Embase, and Google Scholar). The keywords (“robotics”, “navigation”, and “stereotactic”) were searched. There was no limitation date with the search conducted until May 2023. Non-English studies and case reports were excluded from this study. All references to the obtained articles were also evaluated for any additional information.
2. Basics of Navigation and Robotic Systems
Percutaneous image-guided needle procedures are dependent on accurate planning and precise needle placement during the procedure to ensure safety and efficacy. Sophisticated devices assist image-guided IO procedures by enabling the guidance of instruments and needles into the patient to reach target lesions, sometimes also providing real-time spatial feedback, which is a requisite to improved targeting via iterative (closed or open-loop) procedures [11]. These systems allow for the laser-, hybrid-, deep learning-, optical-, or electromagnetic-based tracking of the instruments to be used during the interventional procedure [12]. Real-time imaging and the use of image fusion additionally improve visualization of the needle track, targets, and treatment effects [3,13,14].
Laser guidance has already been used for decades to improve accuracy during CT-guided percutaneous interventions. The puncture point and trajectory angle of the needle are shown exactly by a laser ray on the patient’s skin. Laser guidance systems can be hand-held, mounted to a circular rail placed immediately in front of the CT gantry, or fixed elsewhere in the CT room or gantry itself [15,16]. Laser guidance has been used for biopsy and drainage procedures [15,17], offering improved accuracy, speed, and safety of the interventions and reducing radiation exposure during the procedure [17].
Augmented reality (AR) navigation shows comparable accuracy to CBCT-guided fluoroscopy but significantly reduces procedure time and radiation exposure [14,18]. Radiopaque fiducials are attached to the patient’s skin and on the needle to be tracked in real time. After the CT scan with fiducials is taken, the software allows for automatically segmenting the organs of interest and the target lesion(s) and automatically registering the fiducials on the patient with the ones segmented by the software. By using AR goggles, the physician can very rapidly see the superimposed 3D reconstruction of organs and lesions on the patient in the correct location with very high precision. Moreover, the fiducials placed on the needle show when the needle reaches the target lesion with high accuracy [19,20,21]. Improvements were reported for depth perception and understanding of spatial anatomic relationships [22]. The use of radiation is not required, but fluoroscopy may enable real-time monitoring and adjusting for respiratory deformation or needle deviation. Thus, AR can be used in conjunction with CBCT-guided fluoroscopy imaging to overcome this drawback [14,23].
Cone-beam CT is an imaging modality that is based on the rotational movement of a C-arm equipped with a flat panel detector around the patient, obtaining multiple radiographic images during unit rotation [24]. Acquired data are automatically reconstructed into three-dimensional CT-like datasets that can be analyzed and postprocessed on a workstation, like multidetector CT, but with a smaller field of view. Visualization of skin and deep targets may, however, be challenging in large patients. Navigational software can be combined with cone-beam CT and fusion of fluoroscopic images on the preliminary cone-beam CT, allowing for the monitoring of the trajectory tract and improving accuracy, safety, and effectiveness (even in the case of complex needle paths) without the need for additional equipment [25,26]. Cone-beam CT has been used for percutaneous tumor biopsy and ablation [27,28,29,30,31,32]. Limitations of this technique are artifacts related to rotational X-ray imaging, greater risk of motion artifacts, and limited field of view compared to CT, necessitating trained staff and careful planning before image acquisition to ensure that the appropriate region of interest is included in the field of view [11,24].
Frameless stereotactic navigation systems consist of an electromagnetic or optical localization system, a workstation, a monitor, dedicated software, and various trackable instruments, including ultrasound probes. They allow for localizing a point within the patient in the 3D coordinate system of a CT or MR image dataset in real time. In addition, the navigation system software allows for the planning of needle trajectories in a cartesian coordinate system. The frameless stereotactic navigation systems continuously calculate spatial positions, allowing for the guidance of an instrument or an ablation probe along a controlled path to the target using a virtual line [11].
A crucial part of the optical and electromagnetic navigation workflow is image-to-patient registration. It is achieved by using markers (fiducials, trackers, or references) during pre-interventional image acquisition, so, subsequently, these markers can be linked together and referenced for registration to visualize the trace [3,14,33].
Electromagnetic (EM) navigation utilizes an EM field generator that is placed in proximity to or on the patient and generates a local EM field surrounding the target anatomy (Figure 1) [11]. Fiducial and EM sensors are used so they can be localized within the EM field, and their position can be calculated in relation to each other or to imaging and the patient [34]. The EM field is incompatible with MRI [11,13,35], and large metallic objects may decrease the localization accuracy.
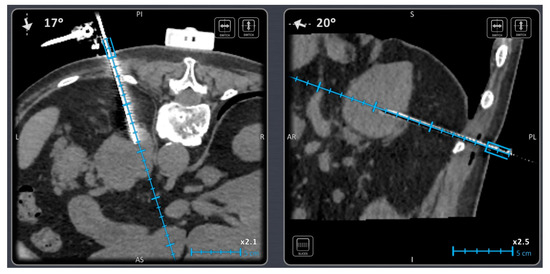
Figure 1.
A 58-year-old male patient with a mass in the left adrenal gland. Biopsy was performed using an electromagnetic navigation device.
Optical tracking utilizes video cameras or sensors detecting infrared or visible light, which is emitted or reflected by fiducials. A free line of sight between the cameras and optical markers is, however, required [36,37]. Both electromagnetic and optical navigation systems have successfully been used to define, localize, and reach lesions that are difficult to access or even inaccessible with conventional CT techniques. This has been associated with lower procedural times and radiation dose, number of needle adjustments, and skin punctures [35,38,39,40,41,42]. By combining optical navigation systems with a rigid aiming device, the accuracy of needle/probe placement can even be improved [43]. This stereotactic approach has been successfully applied in various anatomical regions, including liver [44,45,46].
While the aiming device in passive navigation systems is adjusted manually, robot-assisted systems carry out these settings (semi-)automatically Figure 2 and Figure 3.
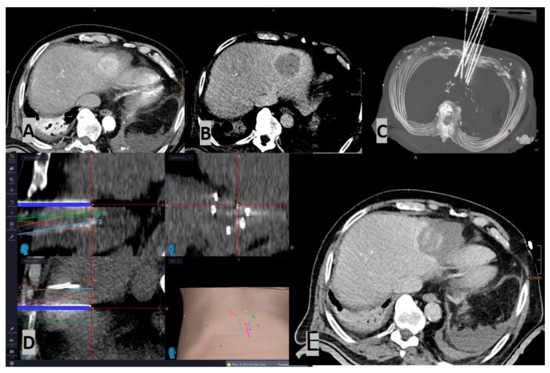
Figure 2.
Case of a stereotactic radiofrequency ablation (SRFA) in an 85-year-old male with a sub-cardiac HCC (4.8 cm): (A) Arterial phase planning CT; (B) Portal-venous phase planning CT; (C) MIP of the control CT, showing in total 7 inserted coaxial needles; (D) Screenshot of the frameless stereotactic navigation system: Superposition of the needle control CT on the planning CT, with the pathways showing precise placement of all needles; (E) Contrast-enhanced control CT (portalvenous phase), showing the large ablation zone covering the HCC, including a sufficient safety margin, which was confirmed by image fusion.
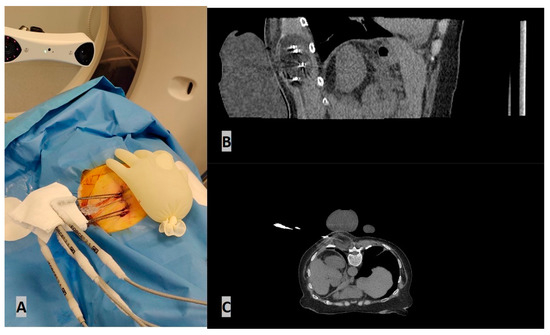
Figure 3.
An 82-year-old female RCC patient with multiple metastatic lesions was treated with percutaneous cryoablation of a soft tissue mass in the posterior paravertebral muscles for pain palliation. (A) The ablation procedure was performed under CT guidance using a robotic navigation device. (B) Four cryoprobes were placed under CT guidance using the robotic navigation device. (C) Axial CT scan during ablation illustrating the ice ball and a sterile glove filled with warm water placed on the skin for protection.
Robotic systems provide active or passive guidance for the placement of needles and instruments. Prior to this procedure, the target is properly visualized using different image guidance modalities, such as computed tomography (CT), cone-beam CT, fluoroscopy, ultrasound, or magnetic resonance imaging (MRI) (Figure 2). Using the imaging data, a registration of the position of the robotic device versus the patient is performed, and a robotic arm moves to the proper position (often with a prior calibration confirmation). The arm is linked to a predefined entry point, angle of insertion, and depth of target (Figure 3). The correct position is confirmed by procedural imaging, and the insertion of instruments is performed through a holder mounted on the hand (“end-effector”) of the robotic arm [3,4]. The main advantage of percutaneous robot-guided interventions is the prevention of unnecessary radiation exposure while ensuring the precision of the procedure [47,48]. Some robotic systems may be used in real time with CT fluoroscopic or CBCT-registered fluoroscopy to monitor the depth and angle of insertions, accounting for respiratory motion.
3. Clinical Applications and the Literature Evidence
The feasibility and safety of the robotic-assisted insertion of biopsy introducer needles have been assessed with a variety of systems in a spectrum of studies, including different target locations [49,50,51,52,53,54,55,56,57,58,59,60,61]. Biopsy sessions were feasible in all patients with accurate needle targeting of the lesion [49,50,51,52,53,54,55,56,57,58,59,60,61]. The performance of a robotic system for CT-guided lung biopsy in comparison to the conventional manual technique was evaluated in a study of 100 patients, which showed that robot-assisted CT-guided lung biopsy was safe, with high diagnostic accuracy, and reduced procedure times and radiation doses in comparison to the conventional freehand technique. In this large study, the precision of needle positioning, diagnostic performance, and rate of complications were similar in patients treated with either robotic-assisted or conventional manual techniques [49]. Evaluation of an electromagnetic navigation system for lung biopsies reported that the system was safe, efficient, and reliable when compared to standard CT guidance, with high diagnostic yield and comparable or not significantly different needle insertion times and complication rates [59].
Prostate cancer is the most common malignancy in men, and the most common biopsy method was traditionally for decades freehand transrectal ultrasound, but a targeted biopsy approach guided by multiparametric MRI has become the current trend, if not standard for certain situations [50]. Robotic systems have been clinically used for transrectal [50,51], trans-gluteal [52,53], and trans-perineal [54] prostate biopsies. Schouten et al. evaluated a robotic device for transrectal MRI-guided prostate biopsy in eight patients, achieving comparable accuracy and speed in comparison to patients that underwent manual biopsy; authors reported that the robotic technique demanded higher technical effort, although it prevented the need to move the patient in and out of the scanner for manipulation and imaging of the needle [51]. Robot-assisted transrectal ultrasound-guided prostate biopsy has been successfully used in a small study including five patients and achieved the millimeter targeting accuracy required for biopsy of clinically significant prostate cancer [50]. A robotic system has been used for MR-guided trans-gluteal prostate biopsy in 20 patients, showing sufficient histopathologic assessment in 19 patients, with high accuracy in needle placement and no procedure-related complications [52]. A single-center nonrandomized prospective trial evaluated prostate-specific membrane antigen (PSMA) positron emission tomography (PET)-guided trans-gluteal prostate biopsy by using an automated robotic arm in 56 subjects [53]. This study has shown that the robotic approach was safe, with a high diagnostic yield of prostate cancer for PSMA-avid lesions, with a low rate of minor complications [53]. A mixed prospective–retrospective study evaluated the utility of a robotic needle-guidance template device (motorized template with an ability to set the needle insertion hole with a control resolution of 0.001 mm) for in-bore 3T trans-perineal MR guided prostate biopsy as compared to a manual template in a study involving 96 patients; this study has shown that the robotic needle-guidance template resulted in better targeting accuracy, more positive tissue from the cancer core, and reduced overall procedure time when compared with the manual approach [54]. Diagnostic rates were similar between the two groups, and there were no statistically significant differences in complication rates between the groups [54]. However, from an outsider’s perspective, one should mention the added cost as well as the complexities of in-gantry procedures. A study evaluating an electromagnetic navigation system for percutaneous CT-guided procedures, including biopsy and drainage accuracy, showed that it was improved by a factor of 2, and significantly lower acquisitions were performed during the utilization of the system [62]. EM tracking for prostate US/MRI fusion biopsy has become a standard method for increasing detection rates of cancer and improving the classification of cancer [63,64]. Navigation tools for prostate cancer have markedly altered the way prostate cancer is diagnosed and managed via cost-effective and accurate application of imaging information in an office setting for biopsy or focal ablation with fusion or robotic-guided laser, HIFU, IRE, or cryoablation. Robotic systems have been clinically applied to a variety of percutaneous ablative procedures, including a plethora of locations and tumor histologies [65,66,67], with excellent results [68,69]. Numerous studies upon navigation-guided or robotic arm-assisted needle positioning during thermal ablation report high rates of feasibility, significant technical ease, and ergonomics, with improved targeting accuracy, reduction in patient radiation dose, and increased procedural performance related to probe placement by a lower number of insertions and readjustments during ablation when compared to manual guidance [36,37,38,39,40]. Specifically for robots, a single insertion without adjustment was achieved in 71% of targeted lesions, whilst for EM navigation systems, accuracy was improved by a factor of 1.6, with a significantly lower number of CT acquisitions and radiation doses noted [70]. Navigation techniques and robotic assistance are particularly useful when treating technically challenging lesions, when multiple needles are required to ensure a large ablation area is achieved, and when the operator must perform the procedure at complex angles. For robotic systems that do not insert automatically (and only guide), the actual insertion of the instruments is performed by the physician, which preserves the haptic experience, allowing for the early detection of incorrect needle positioning. Therefore, utilization of navigation and robotic systems constitutes an attractive option in the management of challenging liver tumors, such as lesions hidden in US or to non-contrast-enhanced CT, large-sized tumors, or tumors located in technically difficult locations, such as in proximity to hepatic venous confluence, diaphragm, hepatic capsule, and heart, among others [71,72,73,74,75,76].
Apart from improving the efficacy, safety, and variability of ablative techniques, navigation, and robotic systems also contribute to the education of students, residents, and less experienced IOs. Navigation systems allow for the learning curves to be shortened, thus allowing the less experienced practitioners to have performance metrics like the experienced or expert [18,77]. As robotic procedures are becoming more widespread, early exposure to their applications for medical students and residents could be an integral part of training, helping them to have more meaningful observation experiences and allowing them to recognize the significance of utilizing such technologies in everyday clinical practices or for training. In a comparative trial evaluating the results of a novice with those of experienced interventional radiologists (IRs) for stereotactic radiofrequency ablation (SRFA) in terms of safety, technical success, and local tumor control, it has been shown that favorable outcomes could be achieved even by inexperienced operators with minimal supervision [77].
Navigation and Robotic systems have been clinically used for other minimally invasive percutaneous procedures, including nerve and facet block, neurolysis, peripheral bone and spine ablation, as well as vertebral augmentation and percutaneous bone fixation procedures [5,34,35,36,37,38,55,78,79,80]. In all these studies, apart from feasibility, safety, and efficacy, radiation dose reduction was also shown. Furthermore, the lack of limitation in acute angles was another advantage noted [81,82].
Augmented reality (AR) can also be used for imaging guidance and navigation in IO procedures using stationary, hand-held, or wearable devices (Figure 4) [14,83]. Needle trajectory is visualized on smartphones or smart glasses, providing a direct line of sight and real-time access to patient information, improving reproducibility, shortening learning curves, and reducing interobserver variability [14] of the interventional techniques [14,18]. In a study of eight patients, AR was used as a unique guidance modality for percutaneous thermal ablation of liver tumors [20]. Technical success was obtained in all cases with no complications or operator cybersickness (Figure 4). The same AR system was employed for bone biopsies in eight patients and proved to decrease radiation exposure, and the number of CT passes compared to the traditional CT guidance [21].
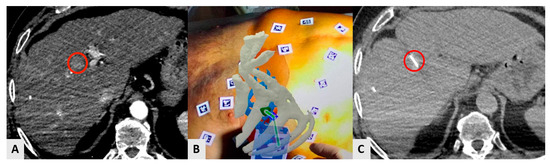
Figure 4.
A 73-year-old male HCC patient was treated with percutaneous radiofrequency ablation in segment VIII. The ablation procedure was performed under CT guidance using an AR navigation device. (A) The small HCC (red circle) is visible in arterial phase. (B) AR guidance from the physician’s point of view. The liver is in red; the bones of thoracic case are in white; the liver vessels are in light-blue, and the lesion is in green. The green line shows the trajectory that connects the tip of the needle to the center of the target in real time. (C) Axial CT scan showing the tip of the needle (red circle) precisely located in the center of the lesion after the guidance by AR.
Globally, the need for medical imaging studies is increasing, with the number of Radiologists remaining the same. From a diagnostic point of view, AR, apart from overcoming geographical barriers, results in more accurate and efficient patient care by allowing for real-time visualization of complex medical data with exceptional precision. Regarding IR/IO techniques, the utilization of AR offers clear advantages, including, among other things, the short learning curve, the reduction in performance variability among users with different levels of experience, as well as the projection of treatment information overlay directly on the procedural environment and not in a monitor away from the patient; all these render AR significantly less expensive [77].
4. Where Are We Heading?
While the utilization of robotics and navigation is rapidly growing in everyday clinical practice, it is a fact that medical students and residents still have limited experience and hands-on familiarity. To enhance the engagement of medical students and residents with robotics, the inclusion of their application in the current curricula is a pre-requisite and will reduce reliance upon apprenticeships later in training or early careers. Once this is achieved, educators will be able to consider hands-on and other simulation programs for medical students and residents aiming to shift training in robotics earlier in their careers, during IR and other specialty/subspecialty training. The addition of navigation and robotics skills and simulation to the core curriculum of IR residency and training pathways might encourage earlier engagement of these paradigm-shifting technologies. As minimum ablation margin assessment and verification tools gain traction and evidence as critical elements for ablation success, tools to train will be even more critical. Utilizing navigation and robotic systems may serve as a useful learning tool in medical training, helping inexperienced operators understand their own inaccuracies and refine their skills. Thus, the end result will be related to learning curve reduction, improved technique performance, and greater patient safety.
Furthermore, the current limitation of navigation and robotic systems is the challenge of funding limitations, thus hindering widespread adoption and utilization. Vendors could start reaching out to users with more flexible and less rigid financial models before the discussion for reimbursing navigation systems and robotics in IR procedures has properly begun.
Finally, there is a need to develop a system that will contribute to ease of use, reliability, and repeatability in all the chronological steps of a procedure, starting from simulation to performance (through navigation) and verification of success. Published results suggest that we are moving toward the goal of ablation as a curative alternative to a surgical procedure. Verification of ablation zone margins by a three-dimensional software (or hardware–software platform) is key for the evolution of ablative procedures [7,8,84,85,86]. It goes without saying that navigation and robotic systems of today and tomorrow should include such verification systems.
Magnetic resonance imaging (MRI) can be used for imaging-guided procedures, providing real-time navigation along with higher resolution images and better soft tissue contrast or functional flow, dynamic, or molecular data when compared to computed tomography (CT), ultrasound, and X-ray. Experimental and clinical research in the areas of interventional tools, endovascular micro-robots, and closed-loop controlled MRI robots is trying to provide solutions for challenges such as MRI-complaint propulsion and control, navigation of medical devices through the body, clinical adaptability, ergonomics, cost, specialized equipment, and regulatory issues [87]. At present, MRI-compatible medical devices remain an emerging field, however, with immense potential clinical impact. MR-guided HIFU systems have shown promise in early trials for the brain, liver, kidney, prostate, and bone cancers. Robotic histotripsy is in early trials for certain liver cancers. Targeted navigation toward neoantigens identified within tumors partly treated with immunotherapies may also provide future pathways toward the use of robotic and navigated needles in IO.
5. Conclusions
Navigation or Robotic guidance offers high-accuracy needle placement and reduces the number of manipulations. Utilization of these technologies could contribute to expanding the limits and indications by treating lesions in extremely challenging locations during a technically easier, shorter, and more cost-efficient session. However, navigation systems and robotics for IO procedures are not a panacea, a solution, or a remedy for all difficulties, and they will never be a substitute for clinical judgment. They should be used as tools for providing better and more reliable clinical care for our patients. Soon, these systems will be invaluable tools assisting all operators in implementing their clinical thought and judgment in practice. Further comprehensive and integrated ergonomics that can be applied to pre-, during-, and post-procedural challenges are requisite to broader adoption. Standardization of tools, techniques, and training methods will allow the field to report meaningful results more accurately, with higher impact and value. The benefits of precision medicine are clear and will create a demand that robotic and navigation tools be used for better and more uniform outcomes in specific settings. Robotic, navigated, and stereotactic multimodality image-guided procedures are here and will only grow as we reach consensus on their absolute requirement to ensure the best outcomes.
Author Contributions
Conceptualization, D.F., B.C.O. and B.W.; methodology, D.F., B.C.O., R.B. and B.W.; software, G.C.; validation, L.S., D.F., B.C.O., R.B. and B.W; formal analysis, L.S., D.F., B.C.O., R.B. and B.W; investigation, G.C.; resources, G.C.; data curation, D.F., B.C.O., R.B., L.S. and B.W; writing—original draft preparation, G.C.; writing—review and editing, L.S., D.F., B.C.O., R.B. and B.W; visualization, L.S., D.F., B.C.O., R.B. and B.W supervision, D.F., B.C.O., R.B. and B.W.; project administration, L.S., D.F., B.C.O., R.B. and B.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created.
Conflicts of Interest
Reto Bale is a consultant for Interventional Systems.
References
- Bale, R.J.; Hoser, C.; Rosenberger, R.; Rieger, M.; Benedetto, K.P.; Fink, C. Osteochondral lesions of the talus: Computer-assisted retrograde drilling—Feasibility and accuracy in initial experiences. Radiology 2001, 218, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Bale, R.J.; Kovacs, P.; Dolati, B.; Hinterleithner, C.; Rosenberger, R.E. Stereotactic CT-guided percutaneous stabilization of posterior pelvic ring fractures: A preclinical cadaver study. J. Vasc. Interv. Radiol. 2008, 19, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Lanza, C.; Carriero, S.; Buijs, E.F.M.; Mortellaro, S.; Pizzi, C.; Sciacqua, L.V.; Biondetti, P.; Angileri, S.A.; Ianniello, A.A.; Ierardi, A.M.; et al. Robotics in Interventional Radiology: Review of Current and Future Applications. Technol. Cancer Res. Treat. 2023, 22, 15330338231152084. [Google Scholar] [CrossRef] [PubMed]
- Najafi, G.; Kreiser, K.; Abdelaziz, M.E.M.K.; Hamady, M.S. Current State of Robotics in Interventional Radiology. Cardiovasc. Interv. Radiol. 2023, 46, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Grigoriadis, S.; Filippiadis, D.; Stamatopoulou, V.; Alexopoulou, E.; Kelekis, N.; Kelekis, A. Navigation Guidance for Percutaneous Splanchnic Nerve Radiofrequency Neurolysis: Preliminary Results. Medicina 2022, 58, 1359. [Google Scholar] [CrossRef]
- Laimer, G.; Schullian, P.; Bale, R. Stereotactic Thermal Ablation of Liver Tumors: 3D Planning, Multiple Needle Approach, and Intraprocedural Image Fusion Are the Key to Success-A Narrative Review. Biology 2021, 10, 644. [Google Scholar] [CrossRef]
- Soulen, M.C.; Sofocleous, C.T. Achieving Curative Ablation Outcomes: It Is All about the Imaging. Radiology 2021, 298, 219–220. [Google Scholar] [CrossRef]
- Lin, Y.-M.; Paolucci, I.; O’connor, C.S.; Anderson, B.M.; Rigaud, B.; Fellman, B.M.; Jones, K.A.; Brock, K.K.; Odisio, B.C. Ablative Margins of Colorectal Liver Metastases Using Deformable CT Image Registration and Autosegmentation. Radiology 2023, 307, e221373. [Google Scholar] [CrossRef]
- Laimer, G.; Schullian, P.; Jaschke, N.; Putzer, D.; Eberle, G.; Alzaga, A.; Odisio, B.; Bale, R. Minimal ablative margin (MAM) assessment with image fusion: An independent predictor for local tumor progression in hepatocellular carcinoma after stereotactic radiofrequency ablation. Eur. Radiol. 2020, 30, 2463–2472. [Google Scholar] [CrossRef]
- Laimer, G.; Jaschke, N.; Schullian, P.; Putzer, D.; Eberle, G.; Solbiati, M.; Solbiati, L.; Goldberg, S.N.; Bale, R. Volumetric assessment of the periablational safety margin after thermal ablation of colorectal liver metastases. Eur. Radiol. 2021, 31, 6489–6499. [Google Scholar] [CrossRef]
- Chehab, M.A.; Brinjikji, W.; Copelan, A.; Venkatesan, A.M. Navigational Tools for Interventional Radiology and Interventional Oncology Applications. Semin. Interv. Radiol. 2015, 32, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Wood, B.J.; Kruecker, J.; Abi-Jaoudeh, N.; Locklin, J.K.; Levy, E.; Xu, S.; Solbiati, L.; Kapoor, A.; Amalou, H.; Venkatesan, A.M. Navigation Systems for Ablation. J. Vasc. Interv. Radiol. 2010, 21 (Suppl. 8), S257–S263. [Google Scholar] [CrossRef] [PubMed]
- Faiella, E.; Castiello, G.; Bernetti, C.; Pacella, G.; Altomare, C.; Andresciani, F.; Zobel, B.B.; Grasso, R.F. Impact of an Augmented Reality Navigation System (SIRIO) on Bone Percutaneous Procedures: A Comparative Analysis with Standard CT-Guided Technique. Curr. Oncol. 2021, 28, 1751–1760. [Google Scholar] [CrossRef] [PubMed]
- Long, D.J.; Li, M.; De Ruiter, Q.M.B.; Hecht, R.; Li, X.; Varble, N.; Blain, M.; Kassin, M.T.; Sharma, K.V.; Sarin, S.; et al. Comparison of Smartphone Augmented Reality, Smartglasses Augmented Reality, and 3D CBCT-guided Fluoroscopy Navigation for Percutaneous Needle Insertion: A Phantom Study. Cardiovasc. Interv. Radiol. 2021, 44, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.W.; Xu, S.; Imbesi, K.L.; Wood, B.J. Integrated laser-guided CT biopsy. Clin. Imaging 2013, 37, 1135–1137. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Moser, C.; Becker, J.; Deli, M.; Busch, M.; Boehme, M.; Groenemeyer, D.H. A novel Laser Navigation System reduces radiation exposure and improves accuracy and workflow of CT-guided spinal interventions: A prospective, randomized, controlled, clinical trial in comparison to conventional freehand puncture. Eur. J. Radiol. 2013, 82, 627–632. [Google Scholar] [CrossRef]
- Gruber-Rouh, T.; Lee, C.; Bolck, J.; Naguib, N.N.; Schulz, B.; Eichler, K.; Aschenbach, R.; Wichmann, J.L.; Vogl, T.J.; Zangos, S. Intervention Planning Using a Laser Navigation System for CT-Guided Interventions: A Phantom and Patient Study. Korean J. Radiol. 2015, 16, 729–735. [Google Scholar] [CrossRef]
- Hecht, R.; Li, M.; de Ruiter, Q.M.B.; Pritchard, W.F.; Li, X.; Krishnasamy, V.; Saad, W.; Karanian, J.W.; Wood, B.J. Smartphone Augmented Reality CT-Based Platform for Needle Insertion Guidance: A Phantom Study. Cardiovasc. Interv. Radiol. 2020, 43, 756–764. [Google Scholar] [CrossRef]
- Solbiati, M.; Passera, K.M.; Rotilio, A.; Oliva, F.; Marre, I.; Goldberg, S.N.; Ierace, T.; Solbiati, L. Augmented reality for interventional oncology: Proof-of-concept study of a novel high-end guidance system platform. Eur. Radiol. Exp. 2018, 2, 18. [Google Scholar] [CrossRef]
- Solbiati, M.; Ierace, T.; Muglia, R.; Pedicini, V.; Iezzi, R.; Passera, K.M.; Rotilio, A.C.; Goldberg, S.N.; Solbiati, L.A. Thermal Ablation of Liver Tumors Guided by Augmented Reality: An Initial Clinical Experience. Cancers 2022, 14, 1312. [Google Scholar] [CrossRef]
- Albano, D.; Messina, C.; Gitto, S.; Chianca, V.; Sconfienza, L.M. Bone biopsies guided by augmented reality: A pilot study. Eur. Radiol. Exp. 2023, 7, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Gadodia, G.; Yanof, J.; Hanlon, A.; Bustos, S.; Weunski, C.; West, K.; Martin, C. Early Clinical Feasibility Evaluation of an Augmented Reality Platform for Guidance and Navigation during Percutaneous Tumor Ablation. J. Vasc. Interv. Radiol. 2022, 33, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Racadio, J.M.; Nachabe, R.; Homan, R.; Schierling, R.; Racadio, J.M.; Babić, D. Augmented Reality on a C-Arm System: A Preclinical Assessment for Percutaneous Needle Localization. Radiology 2016, 281, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Bapst, B.; Lagadec, M.; Breguet, R.; Vilgrain, V.; Ronot, M. Cone Beam Computed Tomography (CBCT) in the Field of Interventional Oncology of the Liver. Cardiovasc. Interv. Radiol. 2016, 39, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Key, B.M.; Tutton, S.M.; Scheidt, M.J. Cone-Beam CT With Enhanced Needle Guidance and Augmented Fluoroscopy Overlay: Applications in Interventional Radiology. Am. J. Roentgenol. 2023, 221, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Busser, W.M.H.; Braak, S.J.; Fütterer, J.J.; van Strijen, M.J.L.; Hoogeveen, Y.L.; de Lange, F.; Kool, L.J.S. Cone beam CT guidance provides superior accuracy for complex needle paths compared with CT guidance. Br. J. Radiol. 2013, 86, 20130310. [Google Scholar] [CrossRef] [PubMed]
- Cazzato, R.L.; Battistuzzi, J.B.; Catena, V.; Grasso, R.F.; Zobel, B.B.; Schena, E.; Buy, X.; Palussiere, J. Cone-Beam Computed Tomography (CBCT) Versus CT in Lung Ablation Procedure: Which is Faster? Cardiovasc. Intervent. Radiol. 2015, 38, 1231–1236. [Google Scholar] [CrossRef]
- Floridi, C.; Muollo, A.; Fontana, F.; Rotolo, N.; Ierardi, A.M.; Duka, E.; Pellegrino, C.; Carrafiello, G. C-arm cone-beam computed tomography needle path overlay for percutaneous biopsy of pulmonary nodules. La Radiol. Med. 2014, 119, 820–827. [Google Scholar] [CrossRef]
- Braak, S.J.; van Melick, H.H.; Onaca, M.G.; van Heesewijk, J.P.; van Strijen, M.J. 3D cone-beam CT guidance, a novel technique in renal biopsy--results in 41 patients with suspected renal masses. Eur. Radiol. 2012, 22, 2547–2552. [Google Scholar] [CrossRef]
- Tselikas, L.; Joskin, J.; Roquet, F.; Farouil, G.; Dreuil, S.; Hakimé, A.; Teriitehau, C.; Auperin, A.; de Baere, T.; Deschamps, F. Percutaneous bone biopsies: Comparison between flat-panel cone-beam CT and CT-scan guidance. Cardiovasc. Interv. Radiol. 2014, 38, 167–176. [Google Scholar] [CrossRef]
- Wallace, M.J.; Kuo, M.D.; Glaiberman, C.; Binkert, C.A.; Orth, R.C.; Soulez, G. Three-dimensional C-arm cone-beam CT: Applications in the interventional suite. J. Vasc. Interv. Radiol. 2008, 19, 799–813. [Google Scholar] [CrossRef] [PubMed]
- Iwazawa, J.; Ohue, S.; Hashimoto, N.; Muramoto, O.; Mitani, T. Survival after C-arm CT-assisted chemoembolization of unresectable hepatocellular carcinoma. Eur. J. Radiol. 2012, 81, 3985–3992. [Google Scholar] [CrossRef] [PubMed]
- Fuhrmann, I.; Probst, U.; Wiggermann, P.; Beyer, L. Navigation Systems for Treatment Planning and Execution of Percutaneous Irreversible Electroporation. Technol. Cancer Res. Treat. 2018, 17, 1533033818791792. [Google Scholar] [CrossRef] [PubMed]
- Ward, T.J.; Goldman, R.E.; Weintraub, J.L. Electromagnetic navigation with multimodality image fusion for image-guided percutaneous interventions. Tech. Vasc. Interv. Radiol. 2013, 16, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Appelbaum, L.; Solbiati, L.; Sosna, J.; Nissenbaum, Y.; Greenbaum, N.; Goldberg, S.N. Evaluation of an electromagnetic image-fusion navigation system for biopsy of small lesions: Assessment of accuracy in an in vivo swine model. Acad. Radiol. 2013, 20, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Appelbaum, L.; Mahgerefteh, S.Y.; Sosna, J.; Goldberg, S.N. Image-guided fusion and navigation: Applications in tumor ablation. Tech. Vasc. Interv. Radiol. 2013, 16, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Phee, S.J.; Yang, K. Interventional navigation systems for treatment of unresectable liver tumor. Med. Biol. Eng. Comput. 2010, 48, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Narsule, C.K.; Dos Santos, R.S.; Gupta, A.; Ebright, M.I.; Rivas, R.; Daly, B.D.; Fernando, H.C. The efficacy of electromagnetic navigation to assist with computed tomography-guided percutaneous thermal ablation of lung tumors. Innovations 2012, 7, 187–190. [Google Scholar]
- Penzkofer, T.; Bruners, P.; Isfort, P.; Schoth, F.; Günther, R.W.; Schmitz-Rode, T.; Mahnken, A.H. Free-hand CT-based electromagnetically guided interventions: Accuracy, efficiency and dose usage. Minim. Invasive Ther. Allied Technol. 2011, 20, 226–233. [Google Scholar] [CrossRef]
- Wu, B.; Xiao, Y.-Y.; Zhang, X.; Zhang, A.-L.; Li, H.-J.; Gao, D.-F. Magnetic resonance imaging-guided percutaneous cryoablation of hepatocellular carcinoma in special regions. Hepatobiliary Pancreat. Dis. Int. 2010, 9, 384–392. [Google Scholar]
- Maeda, T.; Hong, J.; Konishi, K.; Nakatsuji, T.; Yasunaga, T.; Yamashita, Y.-I.; Taketomi, A.; Kotoh, K.; Enjoji, M.; Nakashima, H.; et al. Tumor ablation therapy of liver cancers with an open magnetic resonance imaging-based navigation system. Surg. Endosc. 2009, 23, 1048–1053. [Google Scholar] [CrossRef] [PubMed]
- Faiella, E.; Frauenfelder, G.; Santucci, D.; Luppi, G.; Schena, E.; Zobel, B.B.; Grasso, R.F. Percutaneous low-dose CT-guided lung biopsy with an augmented reality navigation system: Validation of the technique on 496 suspected lesions. Clin. Imaging 2018, 49, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Schullian, P.; Widmann, G.; Lang, T.B.; Knoflach, M.; Bale, R. Accuracy and diagnostic yield of CT-guided stereotactic liver biopsy of primary and secondary liver tumors. Comput. Aided Surg. 2011, 16, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Bale, R.; Widmann, G. Navigated CT-guided interventions. Minim. Invasive Ther. Allied Technol. 2007, 16, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Bale, R.; Widmann, G.; Stoffner, D.R. Stereotaxy: Breaking the limits of current radiofrequency ablation techniques. Eur. J. Radiol. 2010, 75, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Bale, R.; Laimer, G.; Schullian, P.; Alzaga, A. Stereotactic ablation: A game changer? J. Med. Imaging. Radiat. Oncol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.B.; Patriciu, A.; Bohlman, M.E.; Kavoussi, L.R.; Stoianovici, D.; Hiraki, T.; Kamegawa, T.; Matsuno, T.; Sakurai, J.; Kirita, Y.; et al. Robotically driven interventions: A method of using CT fluoroscopy without radiation exposure to the physician. Radiology 2002, 225, 277–282. [Google Scholar] [CrossRef]
- Stoffner, R.; Augschöll, C.; Widmann, G.; Böhler, D.; Bale, R. Accuracy and feasibility of frameless stereotactic and robot-assisted CT-based puncture in interventional radiology: A comparative phantom study. Rofo 2009, 181, 851–858. [Google Scholar] [CrossRef]
- Anzidei, M.; Argirò, R.; Porfiri, A.; Boni, F.; Anile, M.; Zaccagna, F.; Vitolo, D.; Saba, L.; Napoli, A.; Leonardi, A.; et al. Preliminary clinical experience with a dedicated interventional robotic system for CT-guided biopsies of lung lesions: A comparison with the conventional manual technique. Eur. Radiol. 2015, 25, 1310–1316. [Google Scholar] [CrossRef]
- Lim, S.; Jun, C.; Chang, D.; Petrisor, D.; Han, M.; Stoianovici, D. Robotic Transrectal Ultrasound Guided Prostate Biopsy. IEEE Trans. Biomed. Eng. 2019, 66, 2527–2537. [Google Scholar] [CrossRef]
- Schouten, M.G.; Bomers, J.G.R.; Yakar, D.; Huisman, H.; Rothgang, E.; Bosboom, D.; Scheenen, T.W.J.; Misra, S.; Fütterer, J.J. Evaluation of a robotic technique for transrectal MRI-guided prostate biopsies. Eur. Radiol. 2012, 22, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Zangos, S.; Melzer, A.; Eichler, K.; Sadighi, C.; Thalhammer, A.; Bodelle, B.; Wolf, R.; Gruber-Rouh, T.; Proschek, D.; Hammerstingl, R.; et al. MR-compatible assistance system for biopsy in a high-field-strength system: Initial results in patients with suspicious prostate lesions. Radiology 2011, 259, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Singh, S.K.; Mittal, B.R.; Vadi, S.K.; Kakkar, N.; Singh, H.; Krishnaraju, V.S.; Kumar, S.; Bhattacharya, A. Safety and Diagnostic Yield of 68Ga Prostate-specific Membrane Antigen PET/CT-guided Robotic-assisted Transgluteal Prostatic Biopsy. Radiology 2022, 303, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Tilak, G.; Tuncali, K.; Song, S.-E.; Tokuda, J.; Olubiyi, O.; Fennessy, F.; Fedorov, A.; Penzkofer, T.; Tempany, C.; Hata, N. 3T MR-guided in-bore transperineal prostate biopsy: A comparison of robotic and manual needle-guidance templates. J. Magn. Reson. Imaging 2015, 42, 63–71. [Google Scholar] [CrossRef]
- Cleary, K.; Watson, V.; Lindisch, D.; Taylor, R.H.; Fichtinger, G.; Xu, S.; White, C.S.; Donlon, J.; Taylor, M.; Patriciu, A.; et al. Precision placement of instruments for minimally invasive procedures using a "needle driver" robot. Int. J. Med. Robot 2005, 1, 40–47. [Google Scholar] [CrossRef]
- Hiraki, T.; Kamegawa, T.; Matsuno, T.; Sakurai, J.; Komaki, T.; Yamaguchi, T.; Tomita, K.; Uka, M.; Matsui, Y.; Iguchi, T.; et al. Robotic needle insertion during computed tomography fluoroscopy–guided biopsy: Prospective first-in-human feasibility trial. Eur. Radiol. 2020, 30, 927–933. [Google Scholar] [CrossRef]
- Levy, S.; Goldberg, S.N.; Roth, I.; Shochat, M.; Sosna, J.; Leichter, I.; Flacke, S. Clinical evaluation of a robotic system for precise CT-guided percutaneous procedures. Abdom. Imaging 2021, 46, 5007–5016. [Google Scholar] [CrossRef]
- Christou, A.S.; Amalou, A.; Lee, H.; Rivera, J.; Li, R.; Kassin, M.T.; Varble, N.; Tse, Z.T.H.; Xu, S.; Wood, B.J. Image-Guided Robotics for Standardized and Automated Biopsy and Ablation. Semin. Interv. Radiol. 2021, 38, 565–575. [Google Scholar] [CrossRef]
- Witkowska, A.; Levy, S.; Roth, I.; Shochat, M.; Bradbury, D.; Sosna, J.; Leichter, I.; Goldberg, S.N.; Flacke, S. Feasibility and Accuracy of a Novel Hands-Free Robotic System for Percutaneous Needle Insertion and Steering. Surg. Technol. Int. 2022, 41, sti41-1624. [Google Scholar]
- Ben-David, E.; Shochat, M.; Roth, I.; Nissenbaum, I.; Sosna, J.; Goldberg, S.N. Evaluation of a CT-Guided Robotic System for Precise Percutaneous Needle Insertion. J. Vasc. Interv. Radiol. 2018, 29, 1440–1446. [Google Scholar] [CrossRef]
- Lanouzière, M.; Varbédian, O.; Chevallier, O.; Griviau, L.; Guillen, K.; Popoff, R.; Aho-Glélé, S.-L.; Loffroy, R. Computed Tomography-Navigation™ Electromagnetic System Compared to Conventional Computed Tomography Guidance for Percutaneous Lung Biopsy: A Single-Center Experience. Diagnostics 2021, 11, 1532. [Google Scholar] [CrossRef] [PubMed]
- Durand, P.; Moreau-Gaudry, A.; Silvent, A.-S.; Frandon, J.; Chipon, E.; Médici, M.; Bricault, I. Computer assisted electromagnetic navigation improves accuracy in computed tomography guided interventions: A prospective randomized clinical trial. PLoS ONE 2017, 12, e0173751. [Google Scholar] [CrossRef] [PubMed]
- Ahdoot, M.; Wilbur, A.R.; Reese, S.E.; Lebastchi, A.H.; Mehralivand, S.; Gomella, P.T.; Bloom, J.; Gurram, S.; Siddiqui, M.; Pinsky, P.; et al. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. New Engl. J. Med. 2020, 382, 917–928. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Turkbey, B.; George, A.K.; Rothwax, J.; Shakir, N.; Okoro, C.; Raskolnikov, D.; Parnes, H.L.; Linehan, W.M.; et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA 2015, 313, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, B.J.J.; Yeong, C.H.; Goh, K.L.; Yoong, B.K.; Ho, G.F.; Yim, C.C.W.; Kulkarni, A. Robot-assisted radiofrequency ablation of primary and secondary liver tumours: Early experience. Eur. Radiol. 2014, 24, 79–85. [Google Scholar] [CrossRef]
- Beyer, L.P.; Pregler, B.; Michalik, K.; Niessen, C.; Dollinger, M.; Müller, M.; Schlitt, H.J.; Stroszczynski, C.; Wiggermann, P. Evaluation of a robotic system for irreversible electroporation (IRE) of malignant liver tumors: Initial results. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 803–809. [Google Scholar] [CrossRef]
- Mbalisike, E.C.; Vogl, T.J.; Zangos, S.; Eichler, K.; Balakrishnan, P.; Paul, J. Image-guided microwave thermoablation of hepatic tumours using novel robotic guidance: An early experience. Eur. Radiol. 2015, 25, 454–462. [Google Scholar] [CrossRef]
- Braunwarth, E.; Schullian, P.; Kummann, M.; Reider, S.; Putzer, D.; Primavesi, F.; Stättner, S.; Öfner, D.; Bale, R. Aggressive local treatment for recurrent intrahepatic cholangiocarcinoma—Stereotactic radiofrequency ablation as a valuable addition to hepatic resection. PLoS ONE 2022, 17, e0261136. [Google Scholar] [CrossRef]
- Schullian, P.; Laimer, G.; Johnston, E.; Putzer, D.; Eberle, G.; Scharll, Y.; Widmann, G.; Kolbitsch, C.; Bale, R. Technical efficacy and local recurrence after stereotactic radiofrequency ablation of 2653 liver tumors: A 15-year single-center experience with evaluation of prognostic factors. Int. J. Hyperth. 2022, 39, 421–430. [Google Scholar] [CrossRef]
- de Baere, T.; Roux, C.; Deschamps, F.; Tselikas, L.; Guiu, B. Evaluation of a New CT-Guided Robotic System for Percutaneous Needle Insertion for Thermal Ablation of Liver Tumors: A Prospective Pilot Study. Cardiovasc. Intervent Radiol. 2022, 45, 1701–1709. [Google Scholar] [CrossRef]
- Schullian, P.; Johnston, E.; Laimer, G.; Scharll, Y.; Putzer, D.; Eberle, G.; Kolbitsch, C.; Amann, A.; Stättner, S.; Bale, R. Stereotactic radiofrequency ablation of tumors at the hepatic venous confluence. HPB 2022, 24, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- Schullian, P.; Laimer, G.; Putzer, D.; Levy, E.; Braunwarth, E.; Stättner, S.; Bale, R. Stereotactic radiofrequency ablation as first-line treatment of recurrent HCC following hepatic resection. Eur. J. Surg. Oncol. 2020, 46, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Schullian, P.; Johnston, E.W.; Putzer, D.; Laimer, G.; Waroschitz, G.; Braunwarth, E.; Amann, A.; Maglione, M.; Bale, R. Stereotactic radiofrequency ablation (SRFA) for recurrent colorectal liver metastases after hepatic resection. Eur. J. Surg. Oncol. (EJSO) 2021, 47, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Schullian, P.; Johnston, E.W.; Putzer, D.; Eberle, G.; Laimer, G.; Bale, R. Safety and efficacy of stereotactic radiofrequency ablation for very large (≥8 cm) primary and metastatic liver tumors. Sci. Rep. 2020, 10, 1618. [Google Scholar] [CrossRef] [PubMed]
- Filippiadis, D.K.; Velonakis, G.; Mazioti, A.; Tsochatzis, A.; Vrachliotis, T.; Kelekis, A.; Kelekis, N. Percutaneous Navigation under Local Anesthesia for Computed Tomography-Guided Microwave Ablation of Malignant Liver Lesions Located in the Hepatic Dome. Medicina 2021, 57, 1056. [Google Scholar] [CrossRef]
- Volpi, S.; Tsoumakidou, G.; Loriaud, A.; Hocquelet, A.; Duran, R.; Denys, A. Electromagnetic navigation system combined with High-Frequency-Jet-Ventilation for CT-guided hepatic ablation of small US-Undetectable and difficult to access lesions. Int. J. Hyperth. 2019, 36, 1051–1057. [Google Scholar] [CrossRef]
- Schullian, P.; Laimer, G.; Johnston, E.; Putzer, D.; Eberle, G.; Widmann, G.; Scharll, Y.; Bale, R. Reliability of Stereotactic Radiofrequency Ablation (SRFA) for Malignant Liver Tumors: Novice versus Experienced Operators. Biology 2023, 12, 175. [Google Scholar] [CrossRef]
- Moulin, B.; Tselikas, L.; De Baere, T.; Varin, F.; Abed, A.; Debays, L.; Bardoulat, C.; Hakime, A.; Teriitehau, C.; Deschamps, F.; et al. CT guidance assisted by electromagnetic navigation system for percutaneous fixation by internal cemented screws (FICS). Eur. Radiol. 2020, 30, 943–949. [Google Scholar] [CrossRef]
- Teriitehau, C.; Rabeh, H.; Pessis, E.; Sénéchal, Q.; Besse, F.; Bravetti, M. Reduction of patient radiation dose during percutaneous CT vertebroplasty: Impact of a new computer-assisted navigation (CAN) system. Radioprotection 2020, 55, 11–16. [Google Scholar] [CrossRef]
- Schubert, T.; Jacob, A.L.; Pansini, M.; Liu, D.; Gutzeit, A.; Kos, S. CT-guided interventions using a free-hand, optical tracking system: Initial clinical experience. Cardiovasc. Interv. Radiol. 2013, 36, 1055–1062. [Google Scholar] [CrossRef]
- Boeken, T.; Pouliquen, G.; Premat, K.; Benac, B.; Shotar, E.; Cormier; Talbi, A.; Bonaccorsi, R.; Morardet, L.; Morel, V.; et al. Initial experience, feasibility, and technical development with an electromagnetic navigation assistance in percutaneous pelvic bone cementoplasty: Retrospective analysis. Eur. Radiol. 2023, 33, 2605–2611. [Google Scholar] [CrossRef] [PubMed]
- Boeken, T.; Shotar, E.; Cormier; Puyraimond-Zemmour, D.; Talbi, A.; Bonaccorsi, R.; Mahtout, J.; Drir, M.; Clarençon, F.; Premat, K. The “Eiffel Tower” technique: Novel long-axis sacroplasty under electromagnetic navigation assistance; feasibility and descriptive study. Eur. Radiol. 2022, 32, 7640–7646. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J.; Hunt, S.J.; Martin, C.; Nadolski, G.J.; Wood, B.J.; Gade, T.P. Augmented and Mixed Reality: Technologies for Enhancing the Future of IR. J. Vasc. Interv. Radiol. 2020, 31, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Kim, J.H.; Yang, S.G.; Park, S.H.; Choi, H.-K.; Chun, S.-Y.; Kim, P.N.; Park, J.; Lee, M. A Single-Center Retrospective Analysis of Periprocedural Variables Affecting Local Tumor Progression after Radiofrequency Ablation of Colorectal Cancer Liver Metastases. Radiology 2021, 298, 212–218. [Google Scholar] [CrossRef]
- Paolucci, I.; Lin, Y.-M.; Jones, A.K.; Brock, K.K.; Odisio, B.C. Use of Contrast Media During CT-guided Thermal Ablation of Colorectal Liver Metastasis for Procedure Planning is Associated with Improved Immediate Outcomes. Cardiovasc. Interv. Radiol. 2023, 46, 327–336. [Google Scholar] [CrossRef]
- Sofocleous, C.T. Automated Segmentation of CT-guided Ablation Margins in Colorectal Liver Metastases: How We Move Forward to a Standardization of Ablation Zone Assessment. Radiology 2023, 307, e223276. [Google Scholar] [CrossRef]
- Hovet, S.; Ren, H.; Xu, S.; Wood, B.; Tokuda, J.; Tse, Z.T.H. MRI-powered biomedical devices. Minim. Invasive Ther. Allied Technol. 2018, 27, 191–202. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).