Abstract
Peripheral arterial disease (PAD) is an increasingly pathological condition that commonly affects the femoropopliteal arteries. The current fashionable treatment is percutaneous transluminal angioplasty (PTA), often with stenting. However, the in-stent restenosis (ISR) rate after the stenting of the femoropopliteal (FP) district remains high. Many techniques have been proposed for the treatment of femoropopliteal ISR, such as intravascular brachytherapy, laser atherectomy, second stenting and drug-coated balloons angioplasty (DCB). DCB showed a significantly lower rate of restenosis and target lesions revascularization (TLR) compared to conventional PTA. However, further studies and multi-center RCTs with dedicated long-term follow-up are needed to verify the true efficiency of this approach. Nowadays, the correlation between PAD and inflammation biomarkers is well known. Multiple studies have shown that proinflammatory markers (such as C-reactive proteins) and the high plasma levels of microRNA could predict the outcomes after stent placement. In particular, circulating microRNA-320a, microRNA-3937, microRNA-642a-3p and microRNA-572 appear to hold promise in diagnosing ISR in patients with PAD, but also as predictors of stent patency. This narrative review intends to summarize the current knowledge on the value of circulating biomarkers as predictors of ISR and to foster the scientific debate on the advantages of using DCB in the treatment of ISR in the FP district.
1. Introduction
Peripheral arterial disease (PAD) is becoming an increasingly common pathology, with an increase in the world average age and an estimated incidence of 200 million cases per year [1,2]. PAD remains one of the most frequent manifestations of atherosclerosis and cardiovascular pathologies, together with coronary artery and cerebrovascular disease. PAD includes the stenosis of non-coronary and non-cerebral arteries and shares classic risk factors for cardiovascular disease [3]. Classical disease can involve the aorto-iliac, femoro-popliteal district and the below-the-knee arteries. Generally, the below-the-knee arteries are more frequently involved in diabetic patients. The most commonly affected district is the femoropopliteal (FP), which can cause claudication or ischemia of the lower limbs, ischemic ulcers or non-revascularizable conditions, leading to critical limb ischemia (CLI) and a risk of amputation. In the past, open surgery was generally indicated for native arterial disease, mainly bypassed with autologous grafts or with prosthetic material, but with the advent of new technologies, the endovascular approach has become predominant. Nowadays, percutaneous transluminal angioplasty (PTA) represents the first line approach of treatment for obstructive disease of the superficial femoral and popliteal artery. Often, the procedural treatment of this district requires stent implantation after PTA for residual flap dissection or very calcified residual stenosis. However, in-stent restenosis (ISR) after stenting of the FP district remains a daunting problem, resulting in a less than 50% patency rate after 3 years [4]. ISR is believed to be due to neointimal hyperplasia caused by post-PTA endothelial damage [5,6], but similarly to coronary stent disease, other factors are involved such as adherence to antiplatelet therapy [7,8] and specific stent factors [9]. The incidence of ISR also varies according to the type of stent used: 19–35% at 1 year with a grooved tube nitinol stent, and 14–17% with a twisted-wire nitinol stent [4]. The anatomical position can also determine ISR (flexion, stretching, etc.). In the past, there was also stent fracturing, which is particularly common with older self-expanding stents [10]. Many techniques have been proposed for the resolution of ISR such as intravascular brachytherapy, laser atherectomy, second stenting and drug-coated balloon (DCB) [11].
Balloon dilatation and stent implantation is associated with vascular injury, followed by repair processes that include endothelialization and neointimal formation, providing for the activation of the inflammatory response and the release of blood inflammatory markers [9,10,11]. The analysis of these biomarkers could prove useful to physicians to predict an eventual predisposition to ISR.
DCB has been shown to yield excellent results in the setting of PAD. Angiographic and clinical data highlight the superiority of this technique, and the European clinical practice guidelines endorsed its use in the treatment of ISR (class I, Evidence A) [11,12,13]. The DCB is a traditional drug-coated balloon, mainly with Paclitaxel, which significantly improves the short- and medium-term patency of angioplasty by minimizing neo-intimal hyperplasia [14,15,16,17]. Paclitaxel, with a nominal dose between 2 and 3.5 μg/mm2, has lipophilic and hydrophobic properties and, together with a hydrophilic agent, allows the drug to be released to the surface of the artery (Figure 1). There are more than 10 DCBs available in Europe, only three of which are FDA approved. It has been shown that the treatment of ISR with DCB produces better results than traditional angioplasty, while a superiority over drug-eluting stents has not yet been demonstrated [1,18,19]. DCBs are mainly used on the FP axis, particularly on the FP-ISR and rarely on the common iliac or femoral arteries. Another important topic that will be covered in this review are biomarkers. In the literature, microRNA is emerging with great strength as predictors or diagnostic elements for numerous pathologies. ISR, microRNA-320a, microRNA-3937, microRNA-642a-3p and microRNA-572 are proving to be excellent predictors both for evaluating the follow-up and for evaluating the longevity of the patency of the placed stent. This narrative review intends to summarize the value of circulating biomarkers as predictors of ISR, analyze the current knowledge on DCB on ISR and aims to identify the advantages of using DCB in the treatment of ISR of the FP district.
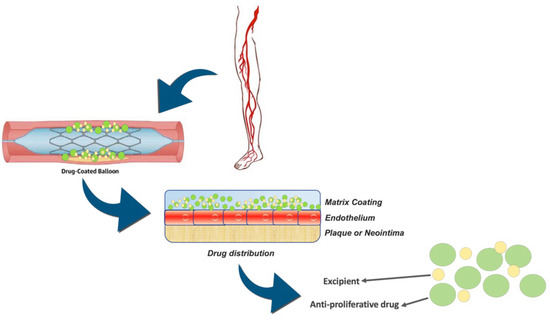
Figure 1.
Mechanism of action of the drug-coated balloon and drug distribution through the endothelium.
2. Materials and Methods
We checked the PubMed and Scopus databases from inception to March 2021. The following key word have been used, with relative MeSH terms: ((“drug eluting” OR “drug coated” OR “coated” OR “eluting” OR “paclitaxel”) AND (“balloon” OR “device” OR “devices” OR “endovascular” OR “stent”) AND (“peripheral” OR “femoral” OR “iliac” OR “popliteal” OR “tibial”) NOT “coronary”) AND (“review” OR “metanalysis” OR “meta-analysis”) AND (“in-stent restenosis”), or (((“drug eluting” OR “drug coated” OR “coated” OR “eluting” OR “paclitaxel”) AND (“balloon” OR “device” OR “devices” OR “endovascular” OR “stent”) AND (“peripheral” OR “femoral” OR “iliac” OR “popliteal” OR “tibial”) NOT “coronary”) AND (“in-stent restenosis”)) NOT (“review” OR “metanalysis” OR “meta-analysis”)). All the articles taken into consideration have been revised; even the references have been checked in order not to lose valuable information, and above all, to verify the relevance with the theme of this review. To be considered, the articles had to have studied ISR in PAD. We initially included randomized studies and observational non-randomized studies. Secondary research articles have been also investigated. We also included, in addition to systematic reviews, prospective studies that examined and compared IRS resolution techniques. Outcomes of interest for selected articles have been included in a shared dataset by three independent authors. All disagreements were resolved by consensus or after consultation with the senior author. Considering the narrative nature of this review, no statistical analysis has been performed.
3. Results
After preliminary evaluation, duplicate removal and manuscript screening, a total of 33 papers have been included in this review. The study design of the included studies is summarized in Table 1, while Table 2 shows the baseline characteristics of the included patients. In all the studies included in this review, the treatment with DCB demonstrated a higher rate of patency and minor rate of restenosis during the follow-up. Furthermore, a significant clinical improvement was highlighted in the majority of the studies, and this result acquires more value if we consider that these data have not been evaluated in all works. Table 3 outlines the results for each study and each treatment arm.

Table 1.
Study design of the included studies.
Table 2.
Summary of baseline characteristics.
Table 3.
Summary of study outcomes.
4. Diagnostic Implications
PTA of peripheral arteries is associated with vascular wall injury followed by repair processes, including endothelialization and neointimal formation [51]. This process is more expressed after stent implantation. The damage to the vascular wall caused by angioplasty and/or stenting causes inflammatory activation. This mechanism leads to the activation of the proliferative process, which consists of the proliferation, migration and differentiation of vascular smooth muscle cells (VSMC). Therefore, this inflammatory process leads to the release of various blood markers.
Beyond the classic inflammatory indices, microRNAs are assuming a considerable importance. Many scientific papers examine mRNAs as markers of disease or as markers of disease progression (Figure 2). In the case of ISR, we have noted and assumed from the literature that these markers can evaluate the longevity of a stent based on the degree of expression at the plasma level.
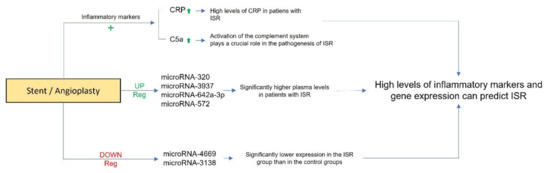
Figure 2.
Schematic representation of diagnostic implications of inflammatory markers and microRNAs in in-stent restenosis. “+” indicates an increase.
4.1. Inflammatory Markers
Numerous studies have reported the probable correlation between inflammatory markers and the restenosis process. In particular, some studies have previously reported that high levels of C-Reactive Protein (CRP) could predict the ISR after the BMS implantation [52,53]. Furthermore, Zhu et al., [54], conducted a meta-analysis of six prospective observational trials, which confirmed that the higher level of hs-CRP is associated with a significantly increased risk of ISR (OR 1.16, 95% CI 1.01–1.30; p < 0.05) in patients who underwent percutaneous transluminal coronary angioplasty. Finally, Jakubiak et al. [55], reported in a review that processes such as inflammation, neointimal hyperplasia and neoatherosclerosis, allergy, resistance to antimitotic drugs used for coating stents and balloons, genetic factors, and technical and mechanical factors, could be implicated in restenosis complications. The authors concluded that every effort should be made to develop knowledge about the pathogenesis of ISR after endovascular treatment of PAD, leading to the availability of more and more perfect therapeutic tools in clinical practice. Some studies reported that the activation of the complement system could play a crucial role in the pathogenesis of restenosis [56,57]. Speidl et al. [56] reported that a higher C5a plasma level is associated with an increased risk of restenosis in patients with PAD who underwent peripheral PTA. In this study C5a concentration was measured at baseline and eight hours after the procedure. Median C5a levels increased significantly from 39.7 ng/mL (IQR 27.8 to 55.0) at baseline to 53.8 ng/mL (IQR 35.6 to 85.1, p < 0.001) 8 h post intervention. During follow-up period, 53% of patients developed restenosis, and elevated levels of C5a at baseline were significantly associated with an increased risk for restenosis (p = 0.0092). Furthermore, the authors specified that this effect was independent of nonspecific inflammation as reflected by the plasma levels of CRP in their patients.
From these experiences, it comes to light that the inflammatory mechanisms play a major role in the development of restenosis after PTA and stent implantation. Therefore, the value of inflammatory biomarkers should be more investigated to improve patency rates.
4.2. microRNA
Recently, studies have reported that elevated levels of microRNA in patients after stenting could be predictive of ISR. Yuan et al. [58] reported that circulating microRNA-320a and microRNA-572 have promising value in diagnosing ISR in patients with PAD. The authors compared 78 patients with ISR, 68 non-ISR patients and 62 healthy volunteers. The microarray analysis showed significant changes in microRNAs, which were up-regulated or down-regulated in ISR groups compared with non-ISR and healthy volunteers. In fact, the analysis revealed that the expression of plasma microRNA-320a, microRNA-3937, microRNA-642a-3p and microRNA-572 were significantly higher in ISR patients than in the control groups. On the other hand, microRNA-4669 and microRNA-3138 showed significantly lower expression in the ISR group than that in the control groups. In addition, from the entire sample set, testing with quantitative reverse transcriptase-polymerase chain reaction (qRT-PCR) and receiver operating characteristic (ROC) analysis, the patients with ISR showed significantly higher expression levels of microRNA-320a and microRNA-572, suggesting their high potential diagnostic value for ISR detection.
Furthermore, Stojkovic et al. [59] recently reported a study on 62 consecutive PAD patients after infrainguinal PTA with stent implantation. The authors investigated the predictive value of 11 microRNAs for the composite endpoint of restenosis and atherothrombotic events (primary endpoint) and target lesion revascularization (TLR, secondary endpoint), demonstrating that the circulating microRNA-195 could predict restenosis, atherothrombotic events and TLR after PTA with stent implantation in FP district.
5. Discussion
The new treatments for PAD have considerably simplified the post-operative course compared to the open surgery approach, but a significant increase in ISR has been observed in recent years and is forecasted in the next years considering the number of procedures performed in each center [2,4,5,26,60,61]. Despite reducing the impact for the patient, PTA is giving very poor results in terms of long-term patency and TLR, and DCB is a new technique which is performing adequately in ISR.
As anticipated in the introduction, this manuscript has the intention of providing a narrative review on the current knowledge on the value of circulating biomarkers as predictors of ISR and to foster the scientific debate on the advantages of using DCB in the treatment of ISR in the FP district. In fact, the use of the stent in the FP district will become an increasingly pursued practice in the field of vascular surgery, making it increasingly necessary to study this knowledge in depth.
There is a focus on more complex and combined techniques for the treatment of ISRs which are producing more encouraging results such as DES, again with major limitations such as a stent length which excludes treating long stenosis. DCB shows superior results compared to traditional re-PTA with a stent and is becoming the technique of choice for ISRs [12,13,14,15,62]. Combined techniques such as laser atherectomy and DCB are also being developed and appear to be candidates to become the reference technique, but adequate studies are warranted [1,11,18,19]. In all the studies included in this review, the treatment with DCB demonstrated a higher rate of patency and minor rate of restenosis during the follow-up. Furthermore, Tepe et al. [24] in the COPACABANA trial reported that at the 12-month follow-up, TLR was performed in 18 (49%) of 37 patients in the uncoated group and in 6 (14%) of 43 patients in the single-dose DCB group (p = 0.001). At ~2 years after treatment, a remarkable number (14/27, 52%) of TLRs were recorded in the single-dose DCB group. The authors concluded that treatment with DCBs resulted in significantly less 6-month restenosis rate and fewer TLRs up to 24 months than the treatment with uncoated balloons.
In the recent metanalysis performed by Xi et al. [12], despite not considering the most recently published articles, 18 studies (9 RCTs and 9 OSs) have been included with a follow-up extended to 3 years. The data analysis showed how the treatment of ISR with DCB and DES was comparable, concluding that the treatment with DCB has a proven efficacy and certainly is not inferior to DES. The current guidelines confirm that DCB is a valid treatment for ISR, which obviates various problems brought about by the placement of traditional stents such as the reduction, in terms of time, of the double antiplatelet therapy, required in the placement of stent-in-stent. Another finding was that the restenosis has drastically decreased after the advent of DES and DCB. However, data have emerged that show that PAD patients treated with DCB (paclitaxel) have an increased risk of death, and it is hypothesized that paclitaxel toxicity is the cause of this increased risk. The mechanism of this increase remains unknown, and new studies are needed to investigate this issue. By comparing the DCBs used for the treatment of PAD and the DCBs used for coronary heart disease, it is hypothesized that the problem is the size and therefore the quantity of paclitaxel released. At the coronary level the DCB is very small, and consequently, the quantity of drug released is significantly lower than the DCB used for peripheral arteries (about 10 times greater). Another hypothesis, in addition to the intrinsic quantity of the drug present on the DCB, is the washing of the drug due to the blood circulation, obviously greater in the peripheral arteries than in the coronary circulation. Less circulating paclitaxel may be the reason for the diverging data between coronary and peripheral DCB. An alternative to PCB or Sirolimus-coated balloon (SCB) is being studied, which seems to give encouraging results. The mechanism of SCB is different from paclitaxel: the first falls into the class of cytostatics, the second into the class of cytotoxics, reversibly binding to the FKBP12 receptor forming a complex with rapamycin blocking the cell cycle in the G1 and S phase. Furthermore, Sirolimus has anti-inflammatory properties compared to paclitaxel, which appears to be the target treatment of patients with ISR. This new technology was approved by the European community and obtained the CE mark in 2016, and numerous centers are experimenting with this new method with Sirolimus. Sirolimus might be the alternative to paclitaxel in peripheral and coronary treatment, provided that the mortality data will be confirmed with scientific evidence.
In addition to all the data collected on the efficacy of the specific drug, the anatomy of the stenosis should also be carefully considered. Feng et al. [14] specifically evaluated the length of the stenosis by dividing the patients into two main categories. CTO (chronic total occlusion) >10 cm, in the reported analysis. Those treated with DCB had a 1-year patency free from other treatments, significantly lower compared to chronic total occlusion, with a length less than 10 cm. The measure of stenosis thus became a 1-year predictor of patency. In addition to the length of the stenosis, the degree of calcification was taken into consideration, considered a limiting factor for treatment with DCB13. It was noted that calcification in the arterial vessel reduces the diffusion capacity of the cytostatic/cytotoxic drug to the arterial wall. Another problem for which we are turning to combined procedures, as described above, is the degree of stenosis or calcification that does not allow for the passage of devices. For this reason, many stenoses or ISRs must be pretreated with traditional balloons to fragment the stenosing plaque, bringing the vessel back to an adequate caliber and allowing the absorption of drugs in situ [12,13,14,15].
6. Conclusions
ISR has been increasingly acknowledged as a daunting complication after percutaneous treatment of PAD. Poor long-term patency and the risk of stent failure in the case of inadequate pharmacological management expose the patient to a risk of limb injury. Multiple studies have shown that proinflammatory markers and high plasma levels of micro-RNA can influence the outcomes after peripheral stenting. This aspect could hold promise for early recognition of ISR, paving the way for future therapeutic tools. The DCB device has been recently introduced to perform target vessel and TLR. DCB have been shown to have promising results and will rapidly be the first line indication for ISR. In particular, DCB showed a significantly lower rate of restenosis and TLR in all the analyzed reports compared to conventional PTA. However, studies with dedicated long-term follow-up are warranted to verify the true efficiency of a technique. DCB gives excellent results in the short-term outcomes, and therefore it might be reliably speculated that it will become the best practice in complex and complicated PAD treatment.
Author Contributions
Conceptualization, N.M., V.C. and A.N.; methodology, N.M., V.C., A.N., M.J. and E.V.; software, F.L., F.N., M.L., C.M., P.M., G.F.S. and F.J.; validation, F.A.C., M.C., F.S. (Francesco Spinelli) and F.S. (Francesco Stilo); formal analysis, A.N., M.J. and E.V.; investigation, V.C. and A.N.; resources, V.C. and A.N.; data curation, V.C. and A.N.; writing—original draft preparation, N.M. and V.C.; writing—review and editing, N.M., V.C. and A.N.; visualization, M.C., F.S. (Francesco Spinelli) and F.S. (Francesco Stilo); supervision, F.S. (Francesco Spinelli) and F.S. (Francesco Stilo). All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| BMS | bare metal stent |
| CLI | critical limb ischemia |
| CSD | covered stent deployment |
| DA | directional atherectomy |
| DCB | drug-coated balloon |
| DCBA | drug-coated balloon angioplasty |
| DES | drug-eluting stent |
| EES | everolimus eluting stent |
| LA | laser atherectomy |
| LD | laser debulking |
| MATH | percutaneous mechanical atherectomy plus thrombectomy |
| MPRT | multicenter prospective randomized controlled trial |
| NRSO | not randomized observational studies |
| PEB | paclitaxel eluting balloon |
| PES | paclitaxel eluting stent |
| PMT | prospective multicenter trial |
| POBA | plain old balloon angioplasty |
| PSMs | propensity score matched study |
| PTA | percutaneous transluminal angioplasty |
| RA | rotational atherectomy |
| RCT | randomized control trial |
| RS | retrospective study |
| TLR | target lesion revascularization |
| VSG | Viabahn Stent-Graft |
References
- Kokkinidis, D.G.; Armstrong, E.J. Current developments in endovascular therapy of peripheral vascular disease. J. Thorac. Dis. 2020, 12, 1681–1694. [Google Scholar] [CrossRef] [PubMed]
- Kayssi, A.; Al-Jundi, W.; Papia, G.; Kucey, D.S.; Forbes, T.; Rajan, D.K.; Neville, R.; Dueck, A.D. Drug-eluting balloon angioplasty versus uncoated balloon angioplasty for the treatment of in-stent restenosis of the femoropopliteal arteries. Cochrane Database Syst. Rev. 2019, 1, CD012510. [Google Scholar] [CrossRef] [PubMed]
- Stilo, F.; Montelione, N.; Calandrelli, R.; Distefano, M.; Spinelli, F.; Di Lazzaro, V.; Pilato, F. The management of carotid restenosis: A comprehensive review. Ann. Transl. Med. 2020, 8, 1272. [Google Scholar] [CrossRef] [PubMed]
- Varela, D.L.; Armstrong, E.J. Endovascular Management of Femoropopliteal In-Stent Restenosis: A Systematic Review. Cardiovasc. Revasc. Med. 2019, 20, 915–925. [Google Scholar] [CrossRef]
- Anantha-Narayanan, M.; Love, K.; Nagpal, S.; Sheikh, A.B.; Regan, C.J.; Mena-Hurtado, C. Safety and efficacy of paclitaxel drug-coated balloon in femoropopliteal in-stent restenosis. Expert Rev. Med Devices 2020, 17, 533–539. [Google Scholar] [CrossRef]
- Spadaccio, C.; Nenna, A.; Rose, D.; Piccirillo, F.; Nusca, A.; Grigioni, F.; Chello, M.; Vlahakes, G.J. The Role of Angiogenesis and Arteriogenesis in Myocardial Infarction and Coronary Revascularization. J. Cardiovasc. Transl. Res. 2022. [Google Scholar] [CrossRef]
- Nusca, A.; Patti, G. Platelet Function and Inhibition in Ischemic Heart Disease. Curr. Cardiol. Rep. 2012, 14, 457–467. [Google Scholar] [CrossRef]
- Nusca, A.; Tuccinardi, D.; Pieralice, S.; Giannone, S.; Carpenito, M.; Monte, L.; Watanabe, M.; Cavallari, I.; Maddaloni, E.; Ussia, G.P.; et al. Platelet Effects of Anti-diabetic Therapies: New Perspectives in the Management of Patients with Diabetes and Cardiovascular Disease. Front. Pharmacol. 2021, 12, 670155. [Google Scholar] [CrossRef]
- Nusca, A.; Viscusi, M.M.; Piccirillo, F.; De Filippis, A.; Nenna, A.; Spadaccio, C.; Nappi, F.; Chello, C.; Mangiacapra, F.; Grigioni, F.; et al. In Stent Neo-Atherosclerosis: Pathophysiology, Clinical Implications, Prevention, and Therapeutic Approaches. Life 2022, 12, 393. [Google Scholar] [CrossRef]
- Sirignano, P.; Citone, M.; Menna, D.; Mansour, W.; Montelione, N.; Capoccia, L.; Speziale, F. Superficial Femoral Artery Stent Disruption Treated by Peripheral Endograft. Ann. Vasc. Surg. 2015, 29, 1661.e5–1661.e8. [Google Scholar] [CrossRef]
- Doshi, R.; Kumar, A.; Adalja, D.; Vaz, I.; Shariff, M. Meta-analysis of Usefulness of Drug Coated Balloon Versus Standard Balloon in the Treatment of Femoropopliteal In-Stent-Restenosis. Am. J. Cardiol. 2020, 133, 170–171. [Google Scholar] [CrossRef] [PubMed]
- Xi, Y.; Chen, J.; Bi, Y.; Xie, S.; Liao, T.; Zhang, Y.; Kislauskis, E.; Wu, T.; Laham, R.; Xiao, J. Long-term clinical safety and efficacy of drug-coated balloon in the treatment of in-stent restenosis: A meta-analysis and systematic review. Catheter. Cardiovasc. Interv. 2020, 96, E129–E141. [Google Scholar] [CrossRef] [PubMed]
- Tong, Z.; Guo, L.; Qi, L.; Cui, S.; Gao, X.; Li, Y.; Guo, J.; Gu, Y. Drug-Coated Balloon Angioplasty and Debulking for the Treatment of Femoropopliteal In-Stent Restenosis: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2020, 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Yang, S.; Sang, H.; Xue, G.; Ni, Q.; Zhang, L.; Zhang, W.; Fang, X.; Ye, M. One-Year Clinical Outcome and Risk Factor Analysis of Directional Atherectomy Followed with Drug-Coated Balloon for Femoropopliteal Artery Disease. J. Endovasc. Ther. 2021, 28, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Cao, S.; He, T.; Xie, J.; Feng, H.; Liu, K.; Qu, B.; Wu, X. Drug-coated balloon angioplasty versus balloon angioplasty for treating patients with in-stent restenosis in the femoropopliteal artery: A meta-analysis. Medicine 2021, 100, e25599. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Nenna, A.; Larobina, D.; Martuscelli, G.; Singh, S.S.A.; Chello, M.; Ambrosio, L. The Use of Bioactive Polymers for Intervention and Tissue Engineering: The New Frontier for Cardiovascular Therapy. Polymers 2021, 13, 446. [Google Scholar] [CrossRef] [PubMed]
- Nenna, A.; Nappi, F.; Larobina, D.; Verghi, E.; Chello, M.; Ambrosio, L. Polymers and Nanoparticles for Statin Delivery: Current Use and Future Perspectives in Cardiovascular Disease. Polymers 2021, 13, 711. [Google Scholar] [CrossRef]
- Kokkinidis, D.G.; Behan, S.; Jawaid, O.; Hossain, P.; Giannopoulos, S.; Singh, G.D.; Laird, J.R.; Valle, J.A.; Waldo, S.W.; Armstrong, E.J. Laser atherectomy and drug-coated balloons for the treatment of femoropopliteal in-stent restenosis: 2-Year outcomes. Catheter. Cardiovasc. Interv. 2020, 95, 439–446. [Google Scholar] [CrossRef]
- Kokkinidis, D.G.; Hossain, P.; Jawaid, O.; Alvandi, B.; Foley, T.R.; Singh, G.D.; Waldo, S.W.; Laird, J.R.; Armstrong, E.J. Laser Atherectomy Combined with Drug-Coated Balloon Angioplasty Is Associated with Improved 1-Year Outcomes for Treatment of Femoropopliteal In-Stent Restenosis. J. Endovasc. Ther. 2018, 25, 81–88. [Google Scholar] [CrossRef]
- Schmidt, A.; Zeller, T.; Sievert, H.; Krankenberg, H.; Torsello, G.; Stark, M.A.; Scheinert, D. Photoablation Using theTurbo-Booster andExcimer Laser for In-Stent RestenosisTreatment: Twelve-Month Results from the PATENT Study. J. Endovasc. Ther. 2014, 21, 52–60. [Google Scholar] [CrossRef]
- Brodmann, M.; Keirse, K.; Scheinert, D.; Spak, L.; Jaff, M.R.; Schmahl, R.; Li, P.; Zeller, T. Drug-Coated Balloon Treatment for Femoropopliteal Artery Disease: The IN.PACT Global Study De Novo In-Stent Restenosis Imaging Cohort. JACC: Cardiovasc. Interv. 2017, 10, 2113–2123. [Google Scholar] [CrossRef]
- Horie, K.; Tanaka, A.; Suzuki, K.; Taguri, M.; Inoue, N. Long-term clinical effectiveness of a drug-coated balloon for in-stent restenosis in Femoropopliteal lesions. CVIR Endovasc. 2021, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- Liistro, F.; Angioli, P.; Porto, I.; Ricci, L.; Ducci, K.; Grotti, S.; Falsini, G.; Ventoruzzo, G.; Turini, F.; Bellandi, G.; et al. Paclitaxel-Eluting Balloon vs. Standard Angioplasty to Reduce Recurrent Restenosis in Diabetic Patients with In-Stent Restenosis of the Superficial Femoral and Proximal Popliteal Arteries: The DEBATE-ISR Study. J. Endovasc. Ther. 2014, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Tepe, G.; Schroeder, H.; Albrecht, T.; Reimer, P.; Diehm, N.; Baeriswyl, J.-L.; Brechtel, K.; Speck, U.; Zeller, T. Paclitaxel-Coated Balloon vs Uncoated Balloon Angioplasty for Treatment of In-Stent Restenosis in the Superficial Femoral and Popliteal Arteries: The COPA CABANA Trial. J. Endovasc. Ther. 2020, 27, 276–286. [Google Scholar] [CrossRef]
- Tepe, G.; Zeller, T.; Moscovic, M.; Corpataux, J.-M.; Christensen, J.K.; Keirse, K.; Nano, G.; Schroeder, H.; Binkert, C.A.; Brodmann, M. Paclitaxel-Coated Balloon Angioplasty for the Treatment of Infrainguinal Arteries: 24-Month Outcomes in the Full Cohort of BIOLUX P-III Global Registry. Cardiovasc. Interv. Radiol. 2021, 44, 207–217. [Google Scholar] [CrossRef]
- Liao, C.-J.; Song, S.-H.; Li, T.; Zhang, Y.; Zhang, W.-D. Randomized controlled trial of orchid drug-coated balloon versus standard percutaneous transluminal angioplasty for treatment of femoropopliteal artery in-stent restenosis. Int. Angiol. 2019, 38, 365–371. [Google Scholar] [CrossRef]
- Liao, C.-J.; Song, S.-H.; Li, T.; Zhang, Y.; Zhang, W.-D. Combination of Rotarex Thrombectomy and Drug-Coated Balloon for the Treatment of Femoropopliteal Artery In-Stent Restenosis. Ann. Vasc. Surg. 2019, 60, 301–307. [Google Scholar] [CrossRef]
- Ott, I.; Cassese, S.; Groha, P.; Steppich, B.; Voll, F.; Hadamitzky, M.; Ibrahim, T.; Kufner, S.; Dewitz, K.; Wittmann, T.; et al. ISAR-PEBIS (Paclitaxel-Eluting Balloon Versus Conventional Balloon Angioplasty for In-Stent Restenosis of Superficial Femoral Artery): A Randomized Trial. J. Am. Heart Assoc. 2017, 6, 006321. [Google Scholar] [CrossRef]
- Krankenberg, H.; Tübler, T.; Ingwersen, M.; Schlüter, M.; Scheinert, D.; Blessing, E.; Sixt, S.; Kieback, A.; Beschorner, U.; Zeller, T. Drug-Coated Balloon Versus Standard Balloon for Superficial Femoral Artery In-Stent Restenosis: The Randomized Femoral Artery In-Stent Restenosis (FAIR) Trial. Circulation 2015, 132, 2230–2236. [Google Scholar] [CrossRef]
- Kinstner, C.M.; Lammer, J.; Willfort-Ehringer, A.; Matzek, W.K.; Gschwandtner, M.; Javor, D.; Funovics, M.; Schoder, M.; Koppensteiner, R.; Loewe, C.; et al. Paclitaxel-Eluting Balloon Versus Standard Balloon Angioplasty in In-Stent Restenosis of the Superficial Femoral and Proximal Popliteal Artery: 1-Year Results of the PACUBA Trial. JACC Cardiovasc. Interv. 2016, 9, 1386–1392. [Google Scholar] [CrossRef]
- Armstrong, E.J.; Thiruvoipati, T.; Tanganyika, K.; Singh, G.D.; Laird, J.R. Laser Atherectomy for Treatment of Femoropopliteal In-Stent Restenosis. J. Endovasc. Ther. 2015, 22, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Laird, J.R., Jr.; Yeo, K.K.; Rocha-Singh, K.; Das, T.; Joye, J.; Dippel, E.; Reddy, B.; Botti, C.; Jaff, M.R. Excimer laser with adjunctive balloon angioplasty and heparin-coated self-expanding stent grafts for the treatment of femoropopliteal artery in-stent restenosis: Twelve-month results from the SALVAGE study. Catheter. Cardiovasc. Interv. 2012, 80, 852–859. [Google Scholar] [CrossRef]
- Gandini, R.; Del Giudice, C.; Merolla, S.; Morosetti, D.; Pampana, E.; Simonetti, G. Treatment of Chronic SFA In-Stent Occlusion with Combined Laser Atherectomy and Drug-Eluting Balloon Angioplasty in Patients with Critical Limb Ischemia: A Single-Center, Prospective, Randomized Study. J. Endovasc. Ther. 2013, 20, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Shammas, N.W.; Shammas, G.A.; Banerjee, S.; Popma, J.J.; Mohammad, A.; Jerin, M. JetStream Rotational and Aspiration Atherectomy in Treating In-Stent Restenosis of the Femoropopliteal Arteries: Results of the JETSTREAM-ISR Feasibility Study. J. Endovasc. Ther. 2016, 23, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Sixt, S.; Cancino, O.G.C.; Treszl, A.; Beschorner, U.; Macharzina, R.; Rastan, A.; Krankenberg, H.; Neumann, F.-J.; Zeller, T. Drug-coated balloon angioplasty after directional atherectomy improves outcome in restenotic femoropopliteal arteries. J. Vasc. Surg. 2013, 58, 682–686. [Google Scholar] [CrossRef][Green Version]
- Bague, N.; Julia, P.; Sauguet, A.; Pernès, J.; Chatelard, P.; Garbé, J.; Penillon, S.; Cardon, J.; Commeau, P.; Planché, O.; et al. Femoropopliteal In-stent Restenosis Repair: Midterm Outcomes After Paclitaxel Eluting Balloon Use (PLAISIR Trial). Eur. J. Vasc. Endovasc. Surg. 2017, 53, 106–113. [Google Scholar] [CrossRef]
- Stabile, E.; Virga, V.; Salemme, L.; Cioppa, A.; Ambrosini, V.; Sorropago, G.; Tesorio, T.; Cota, L.; Popusoi, G.; Pucciarelli, A.; et al. Drug-Eluting Balloon for Treatment of Superficial Femoral Artery In-Stent Restenosis. J. Am. Coll. Cardiol. 2012, 60, 1739–1742. [Google Scholar] [CrossRef]
- Virga, V.; Stabile, E.; Biamino, G.; Salemme, L.; Cioppa, A.; Giugliano, G.; Tesorio, T.; Cota, L.; Popusoi, G.; Pucciarelli, A.; et al. Drug-Eluting Balloons for the Treatment of the Superficial Femoral Artery In-Stent Restenosis: 2-year follow-up. JACC Cardiovasc. Interv. 2014, 7, 411–415. [Google Scholar] [CrossRef]
- Milnerowicz, A.; Milnerowicz, A.; Kuliczkowski, W.; Protasiewicz, M. Rotational Atherectomy Plus Drug-Coated Balloon Angioplasty for the Treatment of Total In-Stent Occlusions in Iliac and Infrainguinal Arteries. J. Endovasc. Ther. 2019, 26, 316–321. [Google Scholar] [CrossRef]
- Giannopoulos, S.; Kokkinidis, D.G.; Jawaid, O.; Behan, S.; Hossain, P.; Alvandi, B.; Foley, T.R.; Singh, G.D.; Waldo, S.W.; Armstrong, E.J. Turbo-Power™ Laser Atherectomy Combined with Drug-coated Balloon Angioplasty is Associated with Improved One-Year Outcomes for the Treatment of Tosaka II and III Femoropopliteal In-stent Restenosis. Cardiovasc. Revasc. Med. 2020, 21, 771–778. [Google Scholar] [CrossRef]
- Thieme, M.; Von Bilderling, P.; Paetzel, C.; Karnabatidis, D.; Delgado, J.P.; Lichtenberg, M. The 24-Month Results of the Lutonix Global SFA Registry: Worldwide Experience with Lutonix Drug-Coated Balloon. JACC Cardiovasc. Interv. 2017, 10, 1682–1690. [Google Scholar] [CrossRef] [PubMed]
- Al Shammeri, O.; Bitar, F.; Ghitelman, J.; Soukas, P.A. Viabahn for femoropopliteal in-stent restenosis. Ann. Saudi Med. 2012, 32, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Bosiers, M.; Deloose, K.; Callaert, J.; Verbist, J.; Hendriks, J.; Lauwers, P.; Schroë, H.; Lansink, W.; Scheinert, D.; Schmidt, A.; et al. Superiority of Stent-Grafts for In-Stent Restenosis in the Superficial Femoral Artery: Twelve-month results from a multicenter randomized trial. J. Endovasc. Ther. 2015, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Zeller, T.; Dake, M.D.; Tepe, G.; Brechtel, K.; Noory, E.; Beschorner, U.; Kultgen, P.L.; Rastan, A. Treatment of Femoropopliteal In-Stent Restenosis with Paclitaxel-Eluting Stents. JACC Cardiovasc. Interv. 2013, 6, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Murata, N.; Takahara, M.; Soga, Y.; Nakano, M.; Yamauchi, Y.; Zen, K.; Kawasaki, D.; Yokoi, H.; Tosaka, A.; Tanaka, N.; et al. Drug-Eluting Stent vs. Percutaneous Transluminal Angioplasty for Treatment of Femoropopliteal In-Stent Restenosis: Results from a Retrospective 1-Year Multicenter Study. J. Endovasc. Ther. 2016, 23, 642–647. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, J.C.; Pedrotti, M.; Canevascini, R.; Chimchila Chevili, S.; Giovannacci, L.; Rosso, R. In-stent restenosis: Mid-term results of debulking using excimer laser and drug-eluting balloons: Sustained benefit? J. Invasive Cardiol. 2014, 26, 333–337. [Google Scholar] [PubMed]
- Liu, M.-Y.; Li, W.; Guo, X.; Zhang, Z.; Liu, B.; Yu, H.; Zhang, Z.; Chen, X.; Feng, H. Percutaneous Mechanical Atherectomy Plus Thrombectomy Using the Rotarex(R)S Device Followed by a Drug-Coated Balloon for the Treatment of Femoropopliteal Artery In-stent Restenosis: A Prospective Single-Center, Single-Arm Efficacy Trial (PERMIT-ISR Trial). Front. Surg. 2021, 8, 671849. [Google Scholar] [CrossRef] [PubMed]
- Tomoi, Y.; Soga, Y.; Okazaki, J.; Iida, O.; Shiraki, T.; Hiramori, S.; Ando, K. Drug-coated stent implantation vs. bypass surgery for in-stent occlusion after femoropopliteal stenting. Heart Vessel. 2021, 36, 646–653. [Google Scholar] [CrossRef]
- Zhang, B.; Niu, G.; Yan, Z.; Zou, Y.; Tong, X.; Yang, M. Drug-Coated Balloon for the Treatment of Femoropopliteal Tosaka Class III In-stent Restenosis Lesions. Front. Surg. 2020, 7, 616414. [Google Scholar] [CrossRef]
- Bosiers, M.; Deloose, K.; Callaert, J.; Verbist, J.; Hendriks, J.; Lauwers, P.; Schroë, H.; Lansink, W.; Scheinert, D.; Schmidt, A.; et al. Stent-grafts are the best way to treat complex in-stent restenosis lesions in the superficial femoral artery: 24-month results from a multicenter randomized trial. J. Cardiovasc. Surg. 2020, 61, 617–625. [Google Scholar] [CrossRef]
- Lee, S.-Y.; Hong, M.-K.; Jang, Y. Formation and Transformation of Neointima after Drug-eluting Stent Implantation: Insights from Optical Coherence Tomographic Studies. Korean Circ. J. 2017, 47, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Walter, D.H.; Fichtlscherer, S.; Sellwig, M.; Auch-Schwelk, W.; Schächinger, V.; Zeiher, A.M. Preprocedural C-reactive protein levels and cardiovascular events after coronary stent implantation. J. Am. Coll. Cardiol. 2001, 37, 839–846. [Google Scholar] [CrossRef]
- Ferrante, G.; Niccoli, G.; Biasucci, L.M.; Liuzzo, G.; Burzotta, F.; Galiuto, L.; Trani, C.; Rebuzzi, A.G.; Crea, F. Association between C-reactive protein and angiographic restenosis after bare metal stents: An updated and comprehensive meta-analysis of 2747 patients. Cardiovasc. Revasc. Med. 2008, 9, 156–165. [Google Scholar] [CrossRef]
- Zhu, X.; Chen, Y.; Xiang, L.; You, T.; Jiao, Y.; Xu, W.; Chen, J. The long-term prognostic significance of high-sensitive C-reactive protein to in-stent restenosis. Medicine 2018, 97, e10679. [Google Scholar] [CrossRef]
- Jakubiak, G.K.; Pawlas, N.; Cies’lar, G.; Stanek, A. Pathogenesis and Clinical Significance of In-Stent Restenosis in Patients with Diabetes. Int. J. Environ. Res. Public Health 2021, 18, 11970. [Google Scholar] [CrossRef]
- Speidl, W.S.; Exner, M.; Amighi, J.; Mlekusch, W.; Sabeti, S.; Kastl, S.P.; Zorn, G.; Maurer, G.; Wagner, O.; Huber, K.; et al. Complement Component C5a Predicts Restenosis After Superficial Femoral Artery Balloon Angioplasty. J. Endovasc. Ther. 2007, 14, 62–69. [Google Scholar] [CrossRef]
- Speidl, W.S.; Exner, M.; Amighi, J.; Kastl, S.P.; Zorn, G.; Maurer, G.; Wagner, O.; Huber, K.; Minar, E.; Wojta, J.; et al. Complement component C5a predicts future cardiovascular events in patients with advanced atherosclerosis. Eur. Heart J. 2005, 26, 2294–2299. [Google Scholar] [CrossRef]
- Yuan, L.; Dong, J.; Zhu, G.; Bao, J.; Lu, Q.; Zhou, J.; Jing, Z. Diagnostic Value of Circulating microRNAs for In-Stent Restenosis in Patients with Lower Extremity Arterial Occlusive Disease. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef]
- Stojkovic, S.; Jurisic, M.; Kopp, C.W.; Koppensteiner, R.; Huber, K.; Wojta, J.; Gremmel, T. Circulating microRNAs identify patients at increased risk of in-stent restenosis after peripheral angioplasty with stent implantation. Atherosclerosis 2018, 269, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Li, B.H.; Chan, Y.C.; Cheng, S.W. Evidence for treatment of lower limb in-stent restenosis with drug eluting balloons. J. Cardiovasc. Surg. 2020, 61, 626–631. [Google Scholar] [CrossRef]
- Li, X.; Zhou, M.; Ding, Y.; Wang, Y.; Cai, L.; Shi, Z. A systematic review and meta-analysis of the efficacy of debulking devices for in-stent restenosis of the femoropopliteal artery. J. Vasc. Surg. 2020, 72, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Spadaccio, C.; Antoniades, C.; Nenna, A.; Chung, C.; Will, R.; Chello, M.; Gaudino, M.F.L. Preventing treatment failures in coronary artery disease: What can we learn from the biology of in-stent restenosis, vein graft failure, and internal thoracic arteries? Cardiovasc. Res. 2020, 116, 505–519. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).