Abstract
Together with the substantial role of genetic factors, serum urate levels and the occurrence of gout are also heavily driven by environmental and clinical factors, including adiposity, dietary patterns, alcohol, kidney function, and diuretic medication use. These are, in turn, greatly influenced by the social determinants of health, which encompass access to health care, availability of healthy foods, and opportunities for physical activity but also education, income, social norms, and racism, among other forces. Gout-related health disparities have been described for Māori and Pacific people in New Zealand, but racial disparities in gout prevalence and outcomes between Black and White Americans have been under-recognised, and particularly, sex-specific data are scarce. In this article we review evidence from prior cohort studies and contemporary national-level data which show the incidence and prevalence of gout and hyperuricemia in Black adults in the US have come to exceed that in White adults and are disproportionately greater in Black women. Importantly, this emerging disparity can be attributed entirely to social determinants of health, including higher levels of adiposity and poverty in Black women compared to White women and lower kidney function and poorer quality diet among Black men compared to White men. Furthermore, Black patients with gout have received poorer quality gout-related care and experienced higher levels of healthcare use, especially Black women. While identifying targets for culturally safe interventions for addressing risk factor disparities is essential, evidence gaps remain about potential disparities in longer-term outcomes of gout, including cardio-metabolic-kidney endpoints and premature mortality. Sociodemographically diverse, population-based longitudinal cohort studies, research on implementation strategies for improved gout care delivery models for underserved groups, and efforts to minimise structural racism and its effects are key to achieving health equity in gout.
1. Introduction
Gout is the most common inflammatory arthritis associated with acute episodes of excruciatingly painful flares, as well as an excess burden of cardiometabolic comorbidities [1] and premature mortality [2]. Together with the substantial role of genetic factors [3], serum urate levels and gout risk are heavily driven by environmental factors (and their genetic interactions), including adiposity, dietary patterns, alcohol, kidney function, and diuretic medication use [4,5,6]. For example, it was estimated that 77% of incident gout cases in a large prospective cohort of male health professionals could theoretically have been prevented had all men kept a normal body mass index (BMI) and adherence to a Dietary Approaches to Stop Hypertension (DASH)-style diet, with no alcohol or diuretic use. Furthermore, genetic interactions with BMI and DASH adherence accounted for 22% and 45% of their combined contributions, respectively, for incident female gout risk [7,8]. These established risk factors are, in turn, greatly influenced by and intertwined with the social determinants of health, which the US Centres for Disease Control and others describe as the economic and social conditions that influence health outcomes and inequities, such as poverty, access to health care, education, social norms and policies, and racism, among other forces and systems [9].
Health disparities in gout, being differences in gout prevalence and outcomes that adversely affect certain groups [10], have received particular attention in New Zealand where Maori and Pacific peoples experience a higher prevalence of gout than New Zealanders of European ancestry, as well as earlier age of onset, higher gout-related healthcare utilisation, and suboptimal pharmacologic management [11]. Gout-related health disparities have also been documented between men and women overall [11] and between Black and White adults living in the US. However, this racial disparity has been under-recognised, particularly with general population, sex-specific data lacking. By synthesising the available evidence on Black–White racial disparities in gout, we aim to articulate the associated burden and consequences for populations living with (or at risk) for gout, particularly at the national level, and identify targets for intervention at the individual, health system, and societal level for reducing these disparities.
2. Are Black Americans at Higher Risk of Gout Than White Americans?
Gout was rare among Black adults in the US until the 1940s and 1950s, similar to Black adults in Africa, especially in rural areas where traditional agricultural and dairy-based diets were common [12]. Subsequently, following worsening in diet quality and quantity, the frequency of metabolic conditions such as obesity, diabetes, and hypertension, as well as gout, rapidly rose overall, although disproportionately among Black Americans [12]. A similar increasing frequency was also noted in urban African communities, in association with an increasing frequency of hypertension and cardiovascular disease [13]. Several prospective cohort studies conducted after the 1950′s have quantified the excess risk of gout and hyperuricemia among Black individuals in the US versus their White counterparts. For example, in the Meharry-Hopkins Study, which prospectively followed Black and White male medical school graduates in Tennessee and Maryland from the late 1950′s and early 1960′s through 1992, the risk of incident gout was 70% greater among the Black men than White [14]. This excess risk was attributed to the excess risk of incident hypertension. Among a cohort of older US adults enrolled in the Multiethnic Cohort study based in California and Hawaii (aged 45–75 years at enrolment during 1993–1996), gout risk was 34% greater among Black individuals compared to White [15] (Table 1). Data from two younger cohorts, the Atherosclerosis Risk in Communities Study (ARIC, aged 45–64 years at enrolment during 1987–89) and the Coronary Artery Risk Development in Young Adults Study (CARDIA, aged 18–30 years at enrolment during 1985–86), further reported that these racial disparities in gout and hyperuricemia status are greater among younger women than younger men (Table 1). This is not surprising given the sex differences in gout risk factor profiles that have been observed (albeit among predominantly White cohorts), with higher frequencies of diuretic use [16,17,18] and obesity [18,19], in women than men, and data indicating higher obesity rates among Black women in the US general population than White [20,21]. Building on these prior findings, below we review national contemporary data on racial differences in gout and hyperuricemia prevalence of US adults across the age spectrum, and potential mediating factors, highlighting sex-specific data.

Table 1.
Black–White disparities in the incidence and prevalence of gout and hyperuricemia in the US, overall and by sex.
3. What Are the Contemporary National Level Black–White Disparity Figures?
For national-level estimates, McCormick et al. used data from the nationally representative National Health and Nutrition Examination Survey (NHANES) to investigate current racial differences in gout prevalence among women and men in the US general population. Participants self-reported their race and ethnicity, provided a blood sample for serum urate measurement, and were asked if a health professional had ever told them they had gout. Data collected from the 2007–08 through 2015–16 annual survey cycles were compared with the NHANES III (1988–1994); gout diagnoses were not ascertained in the intervening annual surveys (1999/00 through 2005/06).
The age-adjusted prevalence of gout over 2007–2016 was 3.5% in women self-reporting Black race and 2.0% in women self-reporting White race, respectively, and 7.0% and 5.4% in men self-reporting Black and White race, respectively [23]. This translated to 81% higher odds of gout among Black women during this contemporary period (vs. White), 26% higher odds of gout among Black men, and 46% higher odds overall [23]. In contrast, the respective age-adjusted odds ratios during NHANES III were null (Figure 1), confirming this disparity for excess gout frequency is a relatively new phenomenon at the national scale. As such, it is important to identify and understand the factors driving this newly emerged national level disparity.
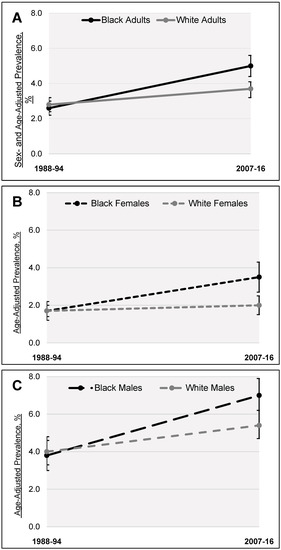
Figure 1.
Age-adjusted prevalence of gout among Black and White US adults between NHANES III (1988–1994) and NHANES 2006–2017. (A) Black and White adults overall; (B) Black and White women; (C) Black and White men.
4. What Drives the Contemporary Black–White Racial Disparities in the US?
Though gout and hyperuricaemia are driven by both environmental and genetic factors [28,29], this racial disparity is likely attributable to non-genetic, social determinants of health and resultant clinical factors [30].This notion is consistent with findings from the Multiple Risk Factor Intervention Trial, a study exclusively of men at high cardiovascular risk, wherein Black men had lower risks of incident gout and hyperuricemia than White men, 22% and 12% lower, respectively, after accounting for differences in gout risk factors between Black and White participants, including BMI, hypertension, alcohol use, and kidney function [24].
Furthermore, race is less of a biological framework and more of a social construct, and many individuals self-reporting Black race will have African and non-African genetic admixture [31]. As well, genetic liability to gout could not have increased over the two to three decades between NHANES III and 2016, and no systematic heterogeneity between genetic ancestry populations was detected in the latest genome-wide association study for serum urate levels [32]. As such, race should be considered as a social construct, with structural racism (i.e., macro-level conditions such as neighbourhood segregation and institutional policies [10]) likely at the core of the social and healthcare inequalities contributing to racial differences in gout frequency and outcomes [30].
McCormick and colleagues used the same nationally representative NHANES data to identify sex-specific factors potentially explaining these racial differences in contemporary gout prevalence. Two approaches were used to determine the impact of potential mediators, a conventional step-by-step approach [33], as well as sequential causal mediation analysis [34,35,36], following the causal flow using a directed acyclic graph (DAG) (Figure 2A). Seven potential mediators were assessed: low educational attainment (high school or less), living in poverty, level of alcohol consumption, non-adherence to a DASH-style diet, excess BMI, diuretic medication use, and chronic kidney disease (CKD). To mediate the racial disparity, a factor needed to be both associated with gout (or hyperuricaemia) and differ in levels or frequency between Black and White individuals. Risk factors associated with gout risk were more frequent (or levels were elevated) in Black women compared to White women, except for alcohol consumption, which was lower among Black women. In stepwise regression, the association between self-reported Black race and gout attenuated most after adjustment for poverty, diet, BMI, and CKD, finally nullifying the associations. Among men, the race–gout association changed little upon adjustment for poverty and BMI, whilst adjustment for CKD rendered the associations null.
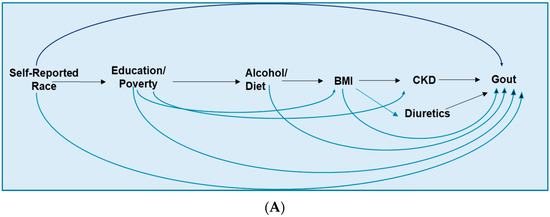
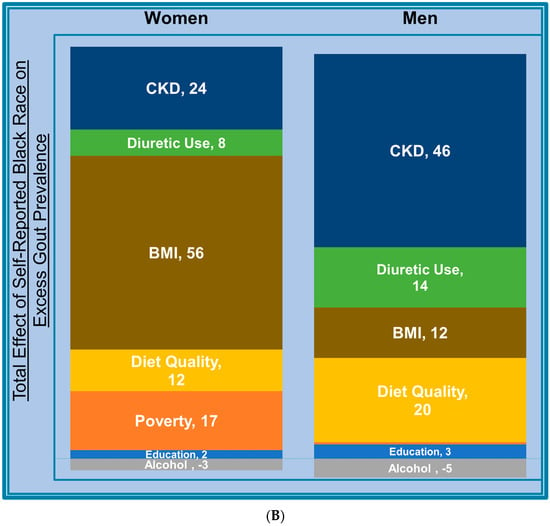
Figure 2.
Assumed causal diagram of the association between race and gout or hyperuricemia (A) and percentage of the total racial difference in gout prevalence mediated by each risk factor, by sex (B). BMI, body mass index; CKD, chronic kidney disease.
To quantify the specific proportion of the race–gout association mediated by each factor, independent of upstream mediators (see the directed acyclic graph (DAG) in Figure 2A), sequential causal mediation analysis was performed, which revealed that the largest mediating factor of excess gout cases among Black women was excess BMI, accounting for 56% of the racial difference (independent of education, poverty, diet, and alcohol), followed by CKD (24%), poverty (17%), and poor diet (12%) (Figure 2B) [23]. Among men, CKD was the largest mediator (46%) followed by diet (20%) and diuretic use (14%), while BMI (12%) and poverty (0.5%) mediated smaller proportions of the racial difference compared with women (Figure 2B) [23]. Mediators of the racial differences in hyperuricaemia were similar to those for female and male gout.
This mediation analysis showed that the excesses in gout and hyperuricemia prevalence among Black adults can be explained entirely by excess frequency or levels of the socio-clinical risk factors for gout, relative to White adults. These factors and their differential burden among Black Americans are described in further detail below.
4.1. Socioeconomic Status
Gout was historically portrayed as a disease of aristocrats [37], but contemporary data have shown different pictures on the relationship between socioeconomic factors and gout and hyperuricemia. For example, a recent meta-analysis reported a positive association between educational attainment and hyperuricemia (from nine studies) but a negative relationship between educational attainment and gout (from four studies) [38]. The authors suggested that differences in study setting may explain this discrepancy, with seven of the nine hyperuricemia studies originating from China, an emerging economy where more educated individuals may consume greater quantities of processed, pro-hyperuricemic foods, whilst the four gout studies were conducted in the US, UK, and Sweden [38]. An additional Swedish study found gout incidence and prevalence were lowest in those with white collar, highly skilled occupations and lowest in the middle-income group [39]. In their analysis of the US general population, McCormick et al. found that low education (no more than high school) was moderately associated with gout status, explaining less than 5% of the racial differences in both female and male gout. Poverty, however (defined as having a household income < 130% of the federal poverty guideline, a threshold often used to determine eligibility for federal benefit programs [40]), was associated with more than two-times greater odds of gout among women overall and explained 17% of racial difference among women but conferred no increased odds for male gout [23]. This low income–gout relationship is consistent with a UK study of primary care practices wherein perceived income inadequacy was associated with 44% greater odds of gout [41], though no sex- or race-stratified estimates were provided. Poverty likely impacts gout directly through its downstream effects on diet quality and BMI [42], with obese women experiencing greater risk of food insecurity than non-obese [43], and may also reflect the more limited healthcare and other health-promoting resources available in many low-income neighbourhoods.
4.2. Diet Quality and Alcohol
Isocaloric DASH adherence has been associated with lower serum urate levels in randomised trials [44,45] and with reduced risk of incident gout [8,46,47], likely by both improving insulin resistance (thereby enhancing urate excretion) [48,49,50] and modulating inflammatory pathways [51,52]. However, adherence to a DASH-style or other guideline-based healthy eating pattern is also associated with higher food costs [53,54]. US adults living in poverty have had lower DASH adherence than those with higher incomes [53,55], and Black adults have had lower DASH adherence than White adults [53,55]. (35, 37) Evidence suggests it costs more for Black adults to achieve DASH adherence than White adults [53]. Interventions aimed at promoting healthier eating patterns such as DASH or others described in the Dietary Guidelines for Americans [46], ensuring fresh produce and other appealing foods with documented benefits for serum urate levels and gout [30] are available for purchase in local neighbourhoods, and reducing financial barriers to adherence could reduce racial disparities in the prevalence of gout and hyperuricemia. Habitual consumption of alcoholic beverages, principally beer and spirits, has also been associated with increased serum urate levels [56] and risk of incident [5,57] and recurrent [58,59] gout. Ethanol has been shown to both increase urate production and reduce urate excretion, while the high purine content of beer may also raise serum urate levels, independently of alcohol levels [56,57]. However, data show the frequency of alcohol consumption is lower among Black Americans than White [23,60] on average, indicating this risk factor does not contribute to the excess prevalence of gout and hyperuricemia among Black Americans at the population level.
4.3. Adiposity
Excess adiposity is a key risk factor for gout [5,61] and hyperuricemia [4], but interestingly, McCormick et al. found excess BMI mediated a far greater proportion of the excess in gout cases among Black women (56%) than among Black men (12%) [23]. Correspondingly, age-adjusted mean BMI was higher in Black women than White women (by 3.2 kg/m2) but was similar between Black and White men [23]; recent NHANES analyses also report a higher mean waist circumference among Black women than White women (with the opposite phenomenon in men) and higher prevalence of general and central obesity [21]. Importantly, this 56% mediation reflects the isolated BMI proportion, independent of upstream factors, including poverty and poor-quality diet, purported to impact gout and hyperuricaemia partly through their impact on BMI (Figure 2A). Obesity rates have increased substantially among both Black and White members of the US general population since NHANES III [20,21] with a disproportionate increase among Black women through 1999–2000 [20]; as with gout itself, changes in genetics for obesity risk could not account for this rapid increase. Differences in neighbourhoods may contribute to excess adiposity in Black women, with evidence that Black Americans tend to live in neighbourhoods with a greater proportion of fast-food outlets and decreased access to resources influencing adiposity levels and overall health such as supermarkets and opportunities for physical activity [62]. Strategies tailed to promote the achievement of healthier body weights among Black women would be key in reducing the Black–White disparity in female gout.
4.4. Diuretic Medications
McCormick et al. found that significantly more Black women and men were currently using diuretics than White women and men. This is likely related to the higher frequency of hypertension among Black adults, particularly Black women [63], compared to White, although choice of anti-hypertensive drug class may also vary. Whilst Black patients with hypertension have been shown to respond better to diuretic or calcium channel blocker monotherapy, with White patients responding better to β-blockers and angiotensin-converting enzyme inhibitors, the variation within racial groups may actually exceed that between racial groups [64]. Thus, urate-lowering anti-hypertensives (e.g., calcium channel blockers or losartan) could be preferred to minimise gout risk [65,66], as could potassium-sparing diuretics [67].
4.5. Chronic Kidney Disease
CKD status was the largest mediator of the racial differences in male gout (46%) and hyperuricemia (37%) and the second-largest mediator among females (24% and 31%, respectively), independent of all upstream mediators. Notably, the emergence of the Black–White racial difference in gout prevalence parallels a disproportionate worsening in CKD prevalence among Black adults during a similar time period [68]. That CKD trends study also sourced NHANES data but, unlike McCormick et al., used the conventional CKD-Epi equation, which included a race coefficient that generates a larger value for estimated glomerular filtration rate for individuals of Black race than others. This can potentially overestimate kidney function in this population and under-ascertain CKD. While the higher prevalence of CKD in Black adults (compared to White) has been partly attributed to the APOL1 risk alleles present in African ancestry populations [69,70] evidence suggests that racial differences in social determinants and clinical factors play a greater role [71]. Sociodemographic and environmental factors together explained 44% [72] of the racial difference in CKD incidence in one study and 64% of the racial difference in another [73], where poorer access to healthcare among Black participants also contributed [73].
5. Are there Black–White Disparities in Gout Care and Outcomes in the US?
5.1. Gout Care Disparity
In addition to being more likely to carry a diagnosis of gout, evidence also suggests that Black individuals with gout receive a lower quality of care than White individuals with gout. As with incidence and prevalence, these disparities also appear worse among Black women than men. In a nationally representative sample of US ambulatory care data from 2002, Black gout patients were 82% less likely to receive an allopurinol prescription than White gout patients [74], with a similar phenomenon observed in the contemporary NHANES data [75] (Table 2). Additionally, Black race was associated with lower adherence among gout patients who were prescribed urate-lowering therapies [76,77,78], even in settings such as US Veterans Affairs healthcare system where out-of-pocket prescription medication costs are low [76,77] and lower odds of achieving a target serum urate level (<6 mg/dL) [78,79] (Table 2).
Table 2.
Black–White disparities in quality of care and healthcare utilisation for gout patients.
5.2. Gout Outcomes Disparity
While gout has been associated with a higher risk of myocardial infarction, stroke, and premature death among White individuals [1,49,85,86,87,88] almost no data on these critical outcomes exist specifically for Black adults. In a recent study of a predominantly Black urban population, gout was cross-sectionally associated with increased prevalence of cardiovascular disease and heart failure [89], although that study did not compare Black and White gout patients, and a worse impact is suspected among Black gout patients given their higher background risk. However, data are available for other key gout outcomes including recurrent flare rates, which were higher among Black individuals than those of other races [82]. Black race was associated with reduced physical function and walking speed among ARIC study participants with gout [81], as well as poorer generic mental and emotional health-related quality of life scores [80], and poorer scores on the Gout Impact Questionnaire, including those related to overall gout concern, unmet treatment need, and well-being and concern during gout flares [80].
5.3. More Frequent Gout-Primary ED Visits and Hospitalisation among the US Black Population
In a sample of US veterans with gout attending centres in Southern California and Alabama, Black patients had higher rates of both outpatient and urgent/overnight healthcare visits over the past year than White patients [84] (Table 2). Additionally, gout-related healthcare costs were higher for Black gout patients in a managed healthcare claims database than gout patients of other races [82]. However, it was not known at the national level how the aforementioned Black–White disparities in background gout risk and quality of care translated to the risk of frequently avoidable inpatient hospitalisations and emergency department (ED) visits for gout. Yokose et al. recently investigated this question using data from the 2019 US National Emergency Department Sample (NEDS) and National Inpatient Sample (NIS), which provide nationally representative samples of ED visits and inpatient admissions across all payers. Compared to White patients, Black patients had a five-times higher rate of gout-primary ED visits (per-capita analysis, with the entire White or Black US population as the denominator), adjusting for age and sex, and a four-times higher rate of gout-primary hospitalisations (Figure 3) [83]. The Black–White racial differences were more prominent for women, who had a nearly six-times higher rate of gout-primary ED visits compared to White women and nearly five-times higher rate of gout-primary hospitalisations (p for interaction < 0.001) (Table 2). Findings were similar in the per-visit analysis using all US ED visits or hospitalisations as the denominator.
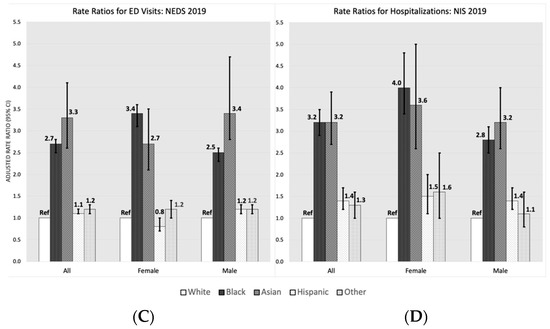
Figure 3.
Age- and sex-adjusted rate ratios for ED visits (A) and hospitalisations (B) for gout, per-capita (based on US Census population), and age-, sex-, and SDOH-adjusted rate ratios for ED visits (C) and hospitalisations (D), per total number of US visits or hospitalisations in 2019, according to race/ethnicity. SDOH, social determinants of health (payer, region, and household income).
Mean costs, a proxy for intensity of resource utilisation, were higher for gout-primary hospitalisations experienced by Black patients compared to White, with the mean excess cost for a gout-primary hospitalisation experienced by Black women (USD 1530 more than White women) being considerably higher than the excess costs experienced by Black men (USD 619 more than White men). When adjusting further for the available measures of social determinants of health (payer, geographic region, and household income level), there was a slight increase in the point estimates for inpatient hospitalisation rates and excess costs. However, these datasets lack data on individual level socioeconomic measures and clinical factors that may further mediate the relationship between Black race and acute healthcare utilisation for gout.
5.4. Role of Inherent Systematic Health Care Disparities
These racial disparities in gout-related care and utilisation suggest Black Americans have more difficulties accessing the primary care services needed to manage their disease and prevent flares and mirror those documented among the US population at-large, even among those receiving coverage from Medicare [90] and Medicaid programs [91]. For example, Black adults were observed to use fewer primary care services than White adults and fill fewer prescriptions for the treatment of asthma, diabetes, and cardiovascular disease, while experiencing higher rates of emergency department utilisation [91]. As such, interventions to improve the quality of care received by Black patients with gout will need to address logistical barriers as well as how racism and unconscious bias in healthcare have impacted the quality of care offered to Black patients and their trust in the system [92].
6. What Research Is Needed to Reduce Black–White Disparities?
Extending the identification of factors contributing to contemporary racial difference in gout prevalence cross-sectionally, prospective quantification of the potential impact of these modifiable risk factors on incident gout risk specifically among Black individuals, particularly Black women, would be valuable. Similarly, regarding the quality of care received by patients with gout, the aforementioned five-times higher risk of gout ED visits and hospitalisations for gout among Black adults could be explained by modifiable social determinants of health and suboptimal care, but no longitudinal cohort data are available. Quantifying their contributions with an expanded set of variables would be an essential step towards reducing these costly outcomes. Sociodemographically diverse population-based longitudinal cohort studies would also help in identifying and addressing potential disparities in gout-related cardio-metabolic-kidney endpoints and mortality. Investigating the impact of opioid and NSAID treatment on these outcomes among Black gout patients, another potential indicator of quality of care, would also be relevant. Implementation strategies of improved gout care delivery models for this underserved group, including enhanced cultural competency among gout providers who work with diverse populations, would be vital to help close the care gap [30].
Furthermore, while again acknowledging the incongruity between self-reported race/ethnicity and genetic ancestry, genetic research to-date has focussed heavily on European ancestry populations, and there is a critical need for genetic studies of gout and its comorbidities and treatments, including gene-environmental interactions, and pharmacogenetic research to guide personalised gout medication choices and doses [93], with more diverse populations and multi-ethnic genotyping arrays. For example, in the ARIC cohort [94,95] and others, it has been shown that genetic risk scores derived from European ancestry populations may be less accurate at predicting disease risk in people from other ancestral populations [96], especially African ancestry populations [97]. Additionally and more broadly, this review has focussed on gout disparities between Black and White adults living in the US, but these racial differences should be examined in other settings, such as Canada, Europe, and the African continent, where data on race/ethnic group-stratified gout prevalence and care are extremely scarce.
7. Conclusions
Over the last several decades, there have been significant advances in determining socio-lifestyle and genetic risk factors for gout [47,98,99,100,101,102,103,104] as well as important outcomes of gout. Still, these factors were ascertained nearly exclusively among White populations, while gout is now more prevalent in Black Americans, particularly women, than their White counterparts, in contrast with data from two decades earlier. A Black–White disparity in gout frequency has emerged over the past decades, heavily influenced by the social determinants of health, which encompasses inequities in access to health care, healthy foods, opportunities for physical activity, and education, and lower income and social resources. Furthermore, this disparity is even more prominent among Black women, attributed mainly to higher levels of adiposity and poverty compared to White women. These inequalities can and must be addressed, to reduce the impact of gout and associated chronic diseases, though this will likely require population- and health system-level changes. In the meantime, evidence also indicates that Black patients with gout, particularly Black women, receive a lower quality of care than White adults, are less likely to achieve a target serum urate, and experience higher rates of often avoidable gout-primary ED visits and hospitalisations. These findings together highlight the need for more race/ethnicity-specific research into the differential disease risk as well as improved management practices to address the health inequity in the care of this excruciatingly painful condition. In particular, purposeful implementation of culturally safe interventions to address this disparity among members of underserved racial/ethnic groups is needed.
Author Contributions
Conceptualization, H.K.C.; Data curation, N.M.; Writing-original draft preparation, H.K.C. and N.M.; Writing-review and editing, N.M., C.Y. and H.K.C.; Supervision, H.K.C.; Funding acquisition, H.K.C.; All authors have read and agreed to the published version of the manuscript.
Funding
P50-AR-060772 (H.K.C.) and R01 AR065944 (H.K.C.), K99-AR080243 (N.M.), and Scientist Development Award, Rheumatology Research Foundation (C.Y.).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
H.K.C. reports research support from Horizon, and consulting fees from Ani, LG, Horizon, Shanton, and Protalix. N.M. and C.Y. have no competing interests to declare.
References
- Choi, H.K.; McCormick, N.; Yokose, C. Excess comorbidities in gout: The causal paradigm and pleiotropic approaches to care. Nat. Rev. Rheumatol. 2022, 18, 97–111. [Google Scholar] [CrossRef]
- Fisher, M.C.; Rai, S.K.; Lu, N.; Zhang, Y.; Choi, H.K. The unclosing premature mortality gap in gout: A general population-based study. Ann. Rheum. Dis. 2017, 76, 1289–1294. [Google Scholar] [CrossRef]
- Major, T.J.; Dalbeth, N.; Stahl, E.A.; Merriman, T.R. An update on the genetics of hyperuricaemia and gout. Nat. Rev. Rheumatol. 2018, 14, 341–353. [Google Scholar] [CrossRef]
- Choi, H.K.; McCormick, N.; Lu, N.; Rai, S.K.; Yokose, C.; Zhang, Y. Population Impact Attributable to Modifiable Risk Factors for Hyperuricemia. Arthritis Rheumatol. 2020, 72, 157–165. [Google Scholar] [CrossRef] [PubMed]
- McCormick, N.; Rai, S.K.; Lu, N.; Yokose, C.; Curhan, G.C.; Choi, H.K. Estimation of Primary Prevention of Gout in Men Through Modification of Obesity and Other Key Lifestyle Factors. JAMA Netw. Open 2020, 3, e2027421. [Google Scholar] [CrossRef] [PubMed]
- MacFarlane, L.A.; Kim, S.C. Gout: A review of nonmodifiable and modifiable risk factors. Rheum. Dis. Clin. N. Am. 2014, 40, 581–604. [Google Scholar] [CrossRef]
- McCormick, N.; Yokose, C.; Lu, N.; Joshi, A.D.; Curhan, G.C.; Choi, H.K. Impact of adiposity on risk of female gout among those genetically predisposed: Sex-specific prospective cohort study findings over >32 years. Ann. Rheum. Dis. 2022, 81, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.; McCormick, N.; Yokose, C.; Joshi, A.D.; Lu, N.; Curhan, G.C.; Merriman, T.R.; Saag, K.G.; Ridker, P.M.; Buring, J.E.; et al. Interactions Between Genetic Risk and Diet Influencing Risk of Incident Female Gout: Discovery and Replication Analysis of Four Prospective Cohorts. Arthritis Rheumatol. 2022, 75, 1028–1038. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. NCHHSTP Social Determinants of Health. 2023. Available online: https://www.cdc.gov/nchhstp/socialdeterminants/faq.html (accessed on 4 February 2023).
- U.S. Department of Health & Human Services. Minority Health and Health Disparities Research. Available online: https://www.nih.gov/ending-structural-racism/minority-health-health-disparities-research (accessed on 4 February 2023).
- Guillen, A.G.; Te Karu, L.; Singh, J.A.; Dalbeth, N. Gender and Ethnic Inequities in Gout Burden and Management. Rheum. Dis. Clin. N. Am. 2020, 46, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J.; Rideout, B.A. Uric acid and diet—Insights into the epidemic of cardiovascular disease. N. Engl. J. Med. 2004, 350, 1071–1073. [Google Scholar] [CrossRef]
- Cassim, B.; Mody, G.M.; Deenadayalu, V.K.; Hammond, M.G. Gout in black South Africans: A clinical and genetic study. Ann. Rheum. Dis. 1994, 53, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C.; Thomas, J.; Thomas, D.J.; Mead, L.; Levine, D.M.; Klag, M.J. Racial differences in the incidence of gout. The role of hypertension. Arthritis Rheum. 1995, 38, 628–632. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.D.; Wu, Y.Y.; Cooney, R.V.; Wilkens, L.R.; Haiman, C.A.; Pirkle, C.M. Modifiable Factors and Incident Gout across Ethnicity within a Large Multiethnic Cohort of Older Adults. J. Rheumatol. 2022, 49, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Puig, J.G.; Michan, A.D.; Jimenez, M.L.; Perez de Ayala, C.; Mateos, F.A.; Capitan, C.F.; de Miguel, E.; Gijon, J.B. Female gout. Clinical spectrum and uric acid metabolism. Arch. Intern. Med. 1991, 151, 726–732. [Google Scholar] [CrossRef]
- Harrold, L.R.; Yood, R.A.; Mikuls, T.R.; Andrade, S.E.; Davis, J.; Fuller, J.; Chan, K.A.; Roblin, D.; Raebel, M.A.; Von Worley, A.; et al. Sex differences in gout epidemiology: Evaluation and treatment. Ann. Rheum. Dis. 2006, 65, 1368–1372. [Google Scholar] [CrossRef]
- Harrold, L.R.; Etzel, C.J.; Gibofsky, A.; Kremer, J.M.; Pillinger, M.H.; Saag, K.G.; Schlesinger, N.; Terkeltaub, R.; Cox, V.; Greenberg, J.D. Sex differences in gout characteristics: Tailoring care for women and men. BMC Musculoskelet. Disord. 2017, 18, 108. [Google Scholar] [CrossRef]
- Te Kampe, R.; Janssen, M.; van Durme, C.; Jansen, T.L.; Boonen, A. Sex Differences in the Clinical Profile Among Patients With Gout: Cross-sectional Analyses of an Observational Study. J. Rheumatol. 2021, 48, 286–292. [Google Scholar] [CrossRef]
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Johnson, C.L. Prevalence and trends in obesity among US adults, 1999–2000. JAMA 2002, 288, 1723–1727. [Google Scholar] [CrossRef]
- Liu, B.; Du, Y.; Wu, Y.; Snetselaar, L.G.; Wallace, R.B.; Bao, W. Trends in obesity and adiposity measures by race or ethnicity among adults in the United States 2011-18: Population based study. BMJ 2021, 372, n365. [Google Scholar] [CrossRef]
- Helget, L.N.; England, B.R.; Roul, P.; Sayles, H.; Petro, A.D.; Michaud, K.; Mikuls, T.R. Incidence, Prevalence, and Burden of Gout in the Veterans Health Administration. Arthritis Care Res. 2021, 73, 1363–1371. [Google Scholar] [CrossRef]
- McCormick, N.; Lu, N.; Yokose, C.; Joshi, A.D.; Sheehy, S.; Rosenberg, L.; Warner, E.T.; Dalbeth, N.; Merriman, T.R.; Saag, K.G.; et al. Racial and Sex Disparities in Gout in US Adults. JAMA Netw. Open 2022, 5, e2226804. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, E. Gout in African Americans. Am. J. Med. 2014, 127, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Maynard, J.W.; McAdams-DeMarco, M.A.; Law, A.; Kao, L.; Gelber, A.C.; Coresh, J.; Baer, A.N. Racial differences in gout incidence in a population-based cohort: Atherosclerosis Risk in Communities Study. Am. J. Epidemiol. 2014, 179, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Gaffo, A.L.; Jacobs, D.R., Jr.; Lewis, C.E.; Mikuls, T.R.; Saag, K.G. Association between being African-American, serum urate levels and the risk of developing hyperuricemia: Findings from the Coronary Artery Risk Development in Young Adults cohort. Arthritis Res. Ther. 2012, 14, R4. [Google Scholar] [CrossRef] [PubMed]
- McAdams-DeMarco, M.A.; Law, A.; Maynard, J.W.; Coresh, J.; Baer, A.N. Risk factors for incident hyperuricemia during mid-adulthood in African American and white men and women enrolled in the ARIC cohort study. BMC Musculoskelet. Disord. 2013, 14, 347. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Guo, C.Y.; Cupples, L.A.; Levy, D.; Wilson, P.W.; Fox, C.S. Genome-wide search for genes affecting serum uric acid levels: The Framingham Heart Study. Metabolism 2005, 54, 1435–1441. [Google Scholar] [CrossRef]
- Krishnan, E.; Lessov-Schlaggar, C.N.; Krasnow, R.E.; Swan, G.E. Nature versus nurture in gout: A twin study. Am. J. Med. 2012, 125, 499–504. [Google Scholar] [CrossRef]
- Roman, Y.M. Moving the Needle in Gout Management: The Role of Culture, Diet, Genetics, and Personalized Patient Care Practices. Nutrients 2022, 14, 3590. [Google Scholar] [CrossRef]
- Banda, Y.; Kvale, M.N.; Hoffmann, T.J.; Hesselson, S.E.; Ranatunga, D.; Tang, H.; Sabatti, C.; Croen, L.A.; Dispensa, B.P.; Henderson, M.; et al. Characterizing Race/Ethnicity and Genetic Ancestry for 100,000 Subjects in the Genetic Epidemiology Research on Adult Health and Aging (GERA) Cohort. Genetics 2015, 200, 1285–1295. [Google Scholar] [CrossRef]
- Tin, A.; Marten, J.; Halperin Kuhns, V.L.; Li, Y.; Wuttke, M.; Kirsten, H.; Sieber, K.B.; Qiu, C.; Gorski, M.; Yu, Z.; et al. Target genes, variants, tissues and transcriptional pathways influencing human serum urate levels. Nat. Genet. 2019, 51, 1459–1474. [Google Scholar] [CrossRef]
- Howard, G.; Cushman, M.; Moy, C.S.; Oparil, S.; Muntner, P.; Lackland, D.T.; Manly, J.J.; Flaherty, M.L.; Judd, S.E.; Wadley, V.G.; et al. Association of Clinical and Social Factors With Excess Hypertension Risk in Black Compared With White US Adults. JAMA 2018, 320, 1338–1348. [Google Scholar] [CrossRef]
- McCormick, N.; Lu, N.; Yokose, C.; Joshi, A.D.; Merriman, T.R.; Saag, K.; Zhang, Y.; Choi, H.K. What drives racial disparities in gout in the US?—Population-based, sex-specific, casual mediation analysis. Ann. Rheum. Dis. 2022, 81, 305–306. [Google Scholar] [CrossRef]
- Valeri, L.; Vanderweele, T.J. Mediation analysis allowing for exposure-mediator interactions and causal interpretation: Theoretical assumptions and implementation with SAS and SPSS macros. Psychol. Methods 2013, 18, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Steen, J.; Loeys, T.; Moerkerke, B.; Vansteelandt, S. Flexible Mediation Analysis With Multiple Mediators. Am. J. Epidemiol. 2017, 186, 184–193. [Google Scholar] [CrossRef]
- Derksen, C.; Murdoch, R.; Petrie, K.J.; Dalbeth, N. “An apple pie a day does not keep the doctor away”: Fictional depictions of gout in contemporary film and television. BMC Rheumatol. 2021, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Pan, Z.; Huang, M.; Fang, M.; Xie, X.; Huang, Z. Socioeconomic differences in hyperuricemia and gout: A systematic review and meta-analysis. Endocrine 2020, 69, 286–293. [Google Scholar] [CrossRef]
- Kapetanovic, M.C.; Hameed, M.; Turkiewicz, A.; Neogi, T.; Saxne, T.; Jacobsson, L.; Englund, M. Prevalence and incidence of gout in southern Sweden from the socioeconomic perspective. RMD Open 2016, 2, e000326. [Google Scholar] [CrossRef]
- US Department of Agriculture. SNAP Eligibility. Available online: https://www.fns.usda.gov/snap/recipient/eligibility (accessed on 4 February 2023).
- Hayward, R.A.; Rathod, T.; Roddy, E.; Muller, S.; Hider, S.L.; Mallen, C.D. The association of gout with socioeconomic status in primary care: A cross-sectional observational study. Rheumatology 2013, 52, 2004–2008. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Fakhouri, T.H.; Carroll, M.D.; Hales, C.M.; Fryar, C.D.; Li, X.; Freedman, D.S. Prevalence of Obesity Among Adults, by Household Income and Education—United States, 2011–2014. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 1369–1373. [Google Scholar] [CrossRef]
- Myers, C.A.; Mire, E.F.; Katzmarzyk, P.T. Trends in Adiposity and Food Insecurity Among US Adults. JAMA Netw. Open 2020, 3, e2012767. [Google Scholar] [CrossRef]
- Juraschek, S.P.; Gelber, A.C.; Choi, H.K.; Appel, L.J.; Miller, E.R., 3rd. Effects of the Dietary Approaches To Stop Hypertension (DASH) Diet and Sodium Intake on Serum Uric Acid. Arthritis Rheumatol. 2016, 68, 3002–3009. [Google Scholar] [CrossRef] [PubMed]
- Juraschek, S.P.; Yokose, C.; McCormick, N.; Miller, E.R., 3rd; Appel, L.J.; Choi, H.K. Effects of Dietary Patterns on Serum Urate: Results From a Randomized Trial of the Effects of Diet on Hypertension. Arthritis Rheumatol. 2021, 73, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Yokose, C.; McCormick, N.; Lu, N.; Joshi, A.D.; Curhan, G.; Choi, H.K. Adherence to 2020 to 2025 Dietary Guidelines for Americans and the Risk of New-Onset Female Gout. JAMA Intern. Med. 2022, 182, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.K.; Fung, T.T.; Lu, N.; Keller, S.F.; Curhan, G.C.; Choi, H.K. The Dietary Approaches to Stop Hypertension (DASH) diet, Western diet, and risk of gout in men: Prospective cohort study. BMJ 2017, 357, j1794. [Google Scholar] [CrossRef] [PubMed]
- Emmerson, B. Hyperlipidaemia in hyperuricaemia and gout. Ann. Rheum. Dis. 1998, 57, 509–510. [Google Scholar] [CrossRef] [PubMed]
- Fam, A.G. Gout, diet, and the insulin resistance syndrome. J. Rheumatol. 2002, 29, 1350–1355. [Google Scholar]
- Quinones Galvan, A.; Natali, A.; Baldi, S.; Frascerra, S.; Sanna, G.; Ciociaro, D.; Ferrannini, E. Effect of insulin on uric acid excretion in humans. Am. J. Physiol. 1995, 268, E1–E5. [Google Scholar] [CrossRef]
- Solomon, D.H.; Glynn, R.J.; MacFadyen, J.G.; Libby, P.; Thuren, T.; Everett, B.M.; Ridker, P.M. Relationship of Interleukin-1beta Blockade With Incident Gout and Serum Uric Acid Levels: Exploratory Analysis of a Randomized Controlled Trial. Ann. Intern. Med. 2018, 169, 535–542. [Google Scholar] [CrossRef]
- Hart, M.J.; Torres, S.J.; McNaughton, S.A.; Milte, C.M. Dietary patterns and associations with biomarkers of inflammation in adults: A systematic review of observational studies. Nutr. J. 2021, 20, 24. [Google Scholar] [CrossRef]
- Monsivais, P.; Rehm, C.D.; Drewnowski, A. The DASH diet and diet costs among ethnic and racial groups in the United States. JAMA Intern. Med. 2013, 173, 1922–1924. [Google Scholar] [CrossRef]
- Mackenbach, J.D.; Burgoine, T.; Lakerveld, J.; Forouhi, N.G.; Griffin, S.J.; Wareham, N.J.; Monsivais, P. Accessibility and Affordability of Supermarkets: Associations With the DASH Diet. Am. J. Prev. Med. 2017, 53, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Crews, D.C.; Kuczmarski, M.F.; Miller, E.R., 3rd; Zonderman, A.B.; Evans, M.K.; Powe, N.R. Dietary habits, poverty, and chronic kidney disease in an urban population. J. Ren. Nutr. 2015, 25, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Curhan, G. Beer, Liquor, Wine, and Serum Uric Acid Level—The Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2004, 51, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Willett, W.C.; Curhan, G. Alcohol Intake and Risk of Incident Gout in Men—A Prospective Study. Lancet 2004, 363, 1277–1281. [Google Scholar] [CrossRef]
- Neogi, T.; Chen, C.; Niu, J.; Chaisson, C.; Hunter, D.J.; Zhang, Y. Alcohol quantity and type on risk of recurrent gout attacks: An internet-based case-crossover study. Am. J. Med. 2014, 127, 311–318. [Google Scholar] [CrossRef]
- Zhang, Y.; Woods, R.; Chaisson, C.E.; Neogi, T.; Niu, J.; McAlindon, T.E.; Hunter, D. Alcohol consumption as a trigger of recurrent gout attacks. Am. J. Med. 2006, 119, 800.e11–800.e16. [Google Scholar] [CrossRef]
- Sa, J.; Russell, M.; Weintruab, M.R.; Seo, D.C.; Chaput, J.P.; Habib, M. Gender and Racial/Ethnic Differences in the Association Between Alcohol Drinking Patterns and Body Mass Index-the National Health and Nutrition Examination Survey, 1999–2010. J. Racial Ethn. Health Disparit. 2019, 6, 301–311. [Google Scholar] [CrossRef]
- Aune, D.; Norat, T.; Vatten, L.J. Body mass index and the risk of gout: A systematic review and dose-response meta-analysis of prospective studies. Eur. J. Nutr. 2014, 53, 1591–1601. [Google Scholar] [CrossRef]
- Phelan, J.C.; Link, B.G. Is racism a fundamental cause of inequalities in health? Annu. Rev. Sociol. 2015, 41, 311–330. [Google Scholar] [CrossRef]
- Aggarwal, R.; Chiu, N.; Wadhera, R.K.; Moran, A.E.; Raber, I.; Shen, C.; Yeh, R.W.; Kazi, D.S. Racial/Ethnic Disparities in Hypertension Prevalence, Awareness, Treatment, and Control in the United States, 2013 to 2018. Hypertension 2021, 78, 1719–1726. [Google Scholar] [CrossRef]
- Sehgal, A.R. Overlap between whites and blacks in response to antihypertensive drugs. Hypertension 2004, 43, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Soriano, L.C.; Zhang, Y.; Rodriguez, L.A. Antihypertensive drugs and risk of incident gout among patients with hypertension: Population based case-control study. BMJ 2012, 344, d8190. [Google Scholar] [CrossRef] [PubMed]
- Juraschek, S.P.; Simpson, L.M.; Davis, B.R.; Shmerling, R.H.; Beach, J.L.; Ishak, A.; Mukamal, K.J. The effects of antihypertensive class on gout in older adults: Secondary analysis of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. J. Hypertens. 2020, 38, 954–960. [Google Scholar] [CrossRef]
- Bruderer, S.; Bodmer, M.; Jick, S.S.; Meier, C.R. Use of diuretics and risk of incident gout: A population-based case-control study. Arthritis Rheumatol. 2014, 66, 185–196. [Google Scholar] [CrossRef]
- Murphy, D.; McCulloch, C.E.; Lin, F.; Banerjee, T.; Bragg-Gresham, J.L.; Eberhardt, M.S.; Morgenstern, H.; Pavkov, M.E.; Saran, R.; Powe, N.R.; et al. Trends in Prevalence of Chronic Kidney Disease in the United States. Ann. Intern. Med. 2016, 165, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.C.; Coresh, J.; Fornage, M.; Astor, B.C.; Grams, M.; Franceschini, N.; Boerwinkle, E.; Parekh, R.S.; Kao, W.H. APOL1 variants associate with increased risk of CKD among African Americans. J. Am. Soc. Nephrol. 2013, 24, 1484–1491. [Google Scholar] [CrossRef]
- Chen, T.K.; Coresh, J.; Daya, N.; Ballew, S.H.; Tin, A.; Crews, D.C.; Grams, M.E. Race, APOL1 Risk Variants, and Clinical Outcomes among Older Adults: The ARIC Study. J. Am. Geriatr. Soc. 2021, 69, 155–163. [Google Scholar] [CrossRef]
- Norton, J.M.; Moxey-Mims, M.M.; Eggers, P.W.; Narva, A.S.; Star, R.A.; Kimmel, P.L.; Rodgers, G.P. Social Determinants of Racial Disparities in CKD. J. Am. Soc. Nephrol. 2016, 27, 2576–2595. [Google Scholar] [CrossRef]
- Tarver-Carr, M.E.; Powe, N.R.; Eberhardt, M.S.; LaVeist, T.A.; Kington, R.S.; Coresh, J.; Brancati, F.L. Excess risk of chronic kidney disease among African-American versus white subjects in the United States: A population-based study of potential explanatory factors. J. Am. Soc. Nephrol. 2002, 13, 2363–2370. [Google Scholar] [CrossRef]
- Evans, K.; Coresh, J.; Bash, L.D.; Gary-Webb, T.; Kottgen, A.; Carson, K.; Boulware, L.E. Race differences in access to health care and disparities in incident chronic kidney disease in the US. Nephrol. Dial. Transplant. 2011, 26, 899–908. [Google Scholar] [CrossRef]
- Krishnan, E.; Lienesch, D.; Kwoh, C.K. Gout in ambulatory care settings in the United States. J. Rheumatol. 2008, 35, 498–501. [Google Scholar] [PubMed]
- Chen-Xu, M.; Yokose, C.; Rai, S.K.; Pillinger, M.H.; Choi, H.K. Contemporary Prevalence of Gout and Hyperuricemia in the United States and Decadal Trends: The National Health and Nutrition Examination Survey, 2007–2016. Arthritis Rheumatol. 2019, 71, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Solomon, D.H.; Avorn, J.; Levin, R.; Brookhart, M.A. Uric acid lowering therapy: Prescribing patterns in a large cohort of older adults. Ann. Rheum. Dis. 2008, 67, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.A.; Richman, J.; Yang, S.; Bridges, S.L.; Saag, K. Allopurinol adherence and its predictors in gout: A national cohort study in US veterans. Lancet Rheumatol. 2020, 2, e281–e291. [Google Scholar] [CrossRef] [PubMed]
- Rashid, N.; Coburn, B.W.; Wu, Y.L.; Cheetham, T.C.; Curtis, J.R.; Saag, K.G.; Mikuls, T.R. Modifiable factors associated with allopurinol adherence and outcomes among patients with gout in an integrated healthcare system. J. Rheumatol. 2015, 42, 504–512. [Google Scholar] [CrossRef]
- Singh, J.A.; Yang, S.; Saag, K.G. Factors Influencing the Effectiveness of Allopurinol in Achieving and Sustaining Target Serum Urate in a US Veterans Affairs Gout Cohort. J. Rheumatol. 2020, 47, 449–460. [Google Scholar] [CrossRef]
- Singh, J.A.; Bharat, A.; Khanna, D.; Aquino-Beaton, C.; Persselin, J.E.; Duffy, E.; Elashoff, D.; Khanna, P.P. Racial differences in health-related quality of life and functional ability in patients with gout. Rheumatology 2017, 56, 103–112. [Google Scholar] [CrossRef]
- Burke, B.T.; Kottgen, A.; Law, A.; Windham, B.G.; Segev, D.; Baer, A.N.; Coresh, J.; McAdams-DeMarco, M.A. Physical Function, Hyperuricemia, and Gout in Older Adults. Arthritis Care Res. 2015, 67, 1730–1738. [Google Scholar] [CrossRef]
- Jackson, R.; Shiozawa, A.; Buysman, E.K.; Altan, A.; Korrer, S.; Choi, H. Flare frequency, healthcare resource utilisation and costs among patients with gout in a managed care setting: A retrospective medical claims-based analysis. BMJ Open 2015, 5, e007214. [Google Scholar] [CrossRef]
- Yokose, C.; McCormick, N.; Lu, N.; Joshi, A.D.; Jackson, L.; Kohler, M.J.; Yinh, J.; Zhang, Y.; Hsu, J.; Dalbeth, N.; et al. Nationwide racial/ethnic disparities in US emergency department visits and hospitalizations for gout. Rheumatology 2022, 62, 2247–2251. [Google Scholar] [CrossRef]
- Singh, J.A.; Bharat, A.; Khanna, D.; Aquino-Beaton, C.; Persselin, J.E.; Duffy, E.; Elashoff, D.; Khanna, P.P. Health care utilization in patients with gout: A prospective multicenter cohort study. BMC Musculoskelet. Disord. 2017, 18, 233. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Mount, D.B.; Reginato, A.M. Pathogenesis of gout. Ann. Intern. Med. 2005, 143, 499–516. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am. J. Med. 2012, 125, 679–687. [Google Scholar] [CrossRef]
- Choi, H.K.; Curhan, G. Independent impact of gout on mortality and risk for coronary heart disease. Circulation 2007, 116, 894–900. [Google Scholar] [CrossRef]
- Krishnan, E.; Svendsen, K.; Neaton, J.D.; Grandits, G.; Kuller, L.H. Long-term cardiovascular mortality among middle-aged men with gout. Arch. Intern. Med. 2008, 168, 1104–1110. [Google Scholar] [CrossRef] [PubMed]
- Chandrakumar, H.P.; Puskoor, A.V.; Chillumuntala, S.; Sharif, S.; Mora, D.C.; Gupta, T.; Tadayoni, A.; Zonnoor, S.L.; Celiker, P.; Yakoubovitch, S.; et al. Assessment of Cardiovascular Disease Among Predominantly Black Gout Patients. J. Clin. Rheumatol. 2023, 29, 202–206. [Google Scholar] [CrossRef]
- Johnston, K.J.; Hammond, G.; Meyers, D.J.; Joynt Maddox, K.E. Association of Race and Ethnicity and Medicare Program Type With Ambulatory Care Access and Quality Measures. JAMA 2021, 326, 628–636. [Google Scholar] [CrossRef]
- Wallace, J.; Lollo, A.; Duchowny, K.A.; Lavallee, M.; Ndumele, C.D. Disparities in Health Care Spending and Utilization Among Black and White Medicaid Enrollees. JAMA Health Forum 2022, 3, e221398. [Google Scholar] [CrossRef]
- Bailey, Z.D.; Krieger, N.; Agenor, M.; Graves, J.; Linos, N.; Bassett, M.T. Structural racism and health inequities in the USA: Evidence and interventions. Lancet 2017, 389, 1453–1463. [Google Scholar] [CrossRef]
- Alrajeh, K.; Roman, Y. Pharmacogenetic Perspective for Optimal Gout Management. Future Pharmacol. 2022, 2, 135–152. [Google Scholar] [CrossRef]
- Thomas, E.A.; Enduru, N.; Tin, A.; Boerwinkle, E.; Griswold, M.E.; Mosley, T.H.; Gottesman, R.F.; Fornage, M. Polygenic Risk, Midlife Life’s Simple 7, and Lifetime Risk of Stroke. J. Am. Heart Assoc. 2022, 11, e025703. [Google Scholar] [CrossRef] [PubMed]
- Hasbani, N.R.; Ligthart, S.; Brown, M.R.; Heath, A.S.; Bebo, A.; Ashley, K.E.; Boerwinkle, E.; Morrison, A.C.; Folsom, A.R.; Aguilar, D.; et al. American Heart Association’s Life’s Simple 7: Lifestyle Recommendations, Polygenic Risk, and Lifetime Risk of Coronary Heart Disease. Circulation 2022, 145, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Rhodes, L.; Young, K.L.; Lilly, A.G.; Raffield, L.M.; Highland, H.M.; Wojcik, G.L.; Agler, C.; Love, S.M.; Okello, S.; Petty, L.E.; et al. Importance of Genetic Studies of Cardiometabolic Disease in Diverse Populations. Circ. Res. 2020, 126, 1816–1840. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.R.; Kanai, M.; Kamatani, Y.; Okada, Y.; Neale, B.M.; Daly, M.J. Clinical use of current polygenic risk scores may exacerbate health disparities. Nat. Genet. 2019, 51, 584–591. [Google Scholar] [CrossRef]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Curhan, G. Obesity, weight change, hypertension, diuretic use, and risk of gout in men: The health professionals follow-up study. Arch. Intern. Med. 2005, 165, 742–748. [Google Scholar] [CrossRef]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Willett, W.C.; Curhan, G. Purine-Rich Foods, Dairy and Protein Intake, and the Risk of Gout in Men. New. Eng. J. Med. 2004, 350, 1093–1103. [Google Scholar] [CrossRef]
- Choi, H.K.; Curhan, G. Soft drinks, fructose consumption, and the risk of gout in men: Prospective cohort study. BMJ 2008, 336, 309–312. [Google Scholar] [CrossRef]
- Choi, H.K.; Willett, W.; Curhan, G. Fructose-rich beverages and risk of gout in women. JAMA 2010, 304, 2270–2278. [Google Scholar] [CrossRef]
- Choi, H.K.; Willett, W.; Curhan, G. Coffee consumption and risk of incident gout in men: A prospective study. Arthritis Rheum. 2007, 56, 2049–2055. [Google Scholar] [CrossRef]
- Choi, H.K.; Curhan, G. Coffee consumption and risk of incident gout in women: The Nurses’ Health Study. Am. J. Clin. Nutr. 2010, 92, 922–927. [Google Scholar] [CrossRef]
- Choi, H.K.; Gao, X.; Curhan, G. Vitamin C intake and the risk of gout in men: A prospective study. Arch. Intern. Med. 2009, 169, 502–507. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).