
A Case Series of Transscleral Cyclophotocoagulation Nd:YAG Laser in Refractory Glaucoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AGM | antiglaucoma medications |
| CPC | cyclophotocoagulation |
| GAT | Goldmann applanation tonometry |
| IOP | intraocular pressure |
| OCT | Optical coherence tomography |
| TSCPC | transscleral cyclophotocoagulation |
References
- Jonas, J.B.; Aung, T.; Bourne, R.R.; Bron, A.M.; Ritch, R.; Panda-Jonas, S. Glaucoma. Lancet 2017, 11, 2183–2193. [Google Scholar] [CrossRef]
- Quigley, H.A.; Broman, A.T. The number of people with glaucoma worldwide in 2010 and 2020. Br. J. Ophthalmol. 2006, 90, 262–267. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The Pathophysiology and Treatment of Glaucoma. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Boland, M.V.; Ervin, A.M.; Friedman, D.S.; Jampel, H.D.; Hawkins, B.S.; Vollenweider, D.; Chelladurai, Y.; Ward, D.; Suarez-Cuervo, C.; Robinson, K.A. Comparative effectiveness of treatments for open-angle glaucoma: A systematic review for the US Preventive Services Task Force. Ann. Intern. Med. 2013, 158, 271–279. [Google Scholar] [CrossRef]
- Nassiri, N.; Kamali, G.; Rahnavardi, M.; Mohammadi, B.; Nassiri, S.; Rahmani, L.; Nassiri, N. Ahmed glaucoma valve and single-plate Molteno implants in treatment of refractory glaucoma: A comparative study. Am. J. Ophthalmol. 2010, 149, 893–902. [Google Scholar] [CrossRef]
- Mahmood, K.; Baig, R.A.; Jameel, M.; Waseem, A.; Khan, M.T.; Qazi, Z.A. Transscleral Diode Laser Cyclophotocoagulation for the Treatment of Refractory Glaucoma. Pak. J. Ophthalmol. 2007, 23, 204–208. [Google Scholar]
- Ho, C.L.; Wong, E.Y.; Chew, P.T. Effect of diode laser contact transscleral pars plana photocoagulation on intraocular pressure in glaucoma. Clin. Exp. Ophthalmol. 2002, 30, 343–347. [Google Scholar] [CrossRef]
- Pantcheva, M.B.; Kahook, M.Y.; Schuman, J.S.; Noecker, R.J. Comparison of acute structural and histopathological changes of the porcine ciliary processes after endoscopic cyclophotocoagulation and transscleral cyclophotocoagulation. Clin. Exp. Ophthalmol. 2007, 35, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R.M.; El-Harazi, S.M.; LoRusso, F.J.; McCash, C.; Lloyd, W.C., III; Warner, P.A. Histopathologic findings following contact transscleral semiconductor diode laser cyclophotocoagulation in a human eye. J. Glaucoma 1997, 6, 139–140. [Google Scholar] [CrossRef] [PubMed]
- Subrata, M.; Ritu, G.; Jatin, A. Diode laser cyclophotocoagulation. J. Curr. Glaucoma Pract. 2009, 3, 47–59. [Google Scholar]
- Ishida, K. Update on results and complications of cyclophotocoagulation. Curr. Opin. Ophthalmol. 2013, 24, 102–110. [Google Scholar] [CrossRef]
- Vernon, S.A.; Koppens, J.M.; Menon, G.J.; Negi, A.K. Diode laser cycloablation in adult glaucoma: Long-term results of a standard protocol and review of current literature. Clin. Exp. Ophthalmol. 2006, 34, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Pastor, S.A.; Singh, K.; Lee, D.A.; Juzych, M.S.; Lin, S.C.; Netland, P.A.; Nguyen, N.T. Cyclophotocoagulation: A report by the American Academy of Ophthalmology. Ophthalmology 2001, 108, 2130–2138. [Google Scholar] [CrossRef]
- Cheung, J.J.; Li, K.K.; Tang, S.W. Retrospective review on the outcome and safety of transscleral diode laser cyclophotocoagulation in refractory glaucoma in Chinese patients. Int. Ophthalmol. 2019, 39, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Souissi, S.; Le Mer, Y.; Metge, F.; Portmann, A.; Baudouin, C.; Labbé, A.; Hamard, P. An update on continuous-wave cyclophotocoagulation (CW-CPC) and micropulse transscleral laser treatment (MP-TLT) for adult and paediatric refractory glaucoma. Acta Ophthalmol. 2021, 99, e621–e653. [Google Scholar] [CrossRef]
- Anderson, A.P.; Douglas, R. MD Collaborative Normal Tension Glaucoma Study. Curr. Opin. Ophthalmol. 2003, 14, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Frezzotti, P.; Mittica, V.; Martone, G.; Motolese, I.; Lomurno, L.; Peruzzi, S.; Motolese, E. Longterm follow-up of diode laser transscleral cyclophotocoagulation in the treatment of refractory glaucoma. Acta Ophthalmol. 2010, 88, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Simmons, R.B.; Prum, B.E., Jr.; Shields, S.R.; Echelman, D.A.; Shields, M.B. Videographic and histologic comparison of Nd:YAG and diode laser contact transscleral cyclophotocoagulation. Am. J. Ophthalmol. 1994, 117, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Kosoko, O.; Gaasterland, D.E.; Pollack, I.P.; Enger, C.L. Long-term outcome of initial ciliary ablation with contact diode laser transscleral cyclophotocoagulation for severe glaucoma. The Diode Laser Ciliary Ablation Study Group. Ophthalmology 1996, 103, 1294–1302. [Google Scholar] [CrossRef]
- Bloom, P.A.; Tsai, J.C.; Sharma, K.; Miller, M.H.; Rice, N.S.; Hitchings, R.A.; Khaw, P.T. “Cyclodiode”. Trans- scleral diode laser cyclophotocoagulation in the treatment of advanced refractory glaucoma. Ophthalmology 1997, 104, 1508–1519, discussion 1519–1520. [Google Scholar] [CrossRef]
- Brancato, R.; Carassa, R.G.; Bettin, P.; Fiori, M.; Trabucchi, G. Contact transscleral cyclophotocoagulation with diode laser in refractory glau-coma. Eur. J. Ophthalmol. 1995, 5, 32–39. [Google Scholar] [CrossRef]
- Farraovà, P.; Ondrejkovà, M.; Demianova, D. Transscleral Diode Cyclophotocoagulation in Treatment Of Glaucoma. Ceska Slov. Oftalmol. 2020, 76, 236–242. (In English) [Google Scholar] [CrossRef] [PubMed]
- Kuchar, S.; Moster, M.R.; Reamer, C.B.; Waisbourd, M. Treatment outcomes of micropulse transscleral cyclophotocoagulation in advanced glaucoma. Lasers Med. Sci. 2016, 31, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Amoozgar, B.; Phan, E.N.; Lin, S.C.; Han, Y. Update on ciliary body laser procedures. Curr. Opin. Ophthalmol. 2017, 28, 181–186. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic data | ||
| No. of patients | 134 | |
| Age | 67.00 ± 17.00 | |
| No. of eyes | 134 | |
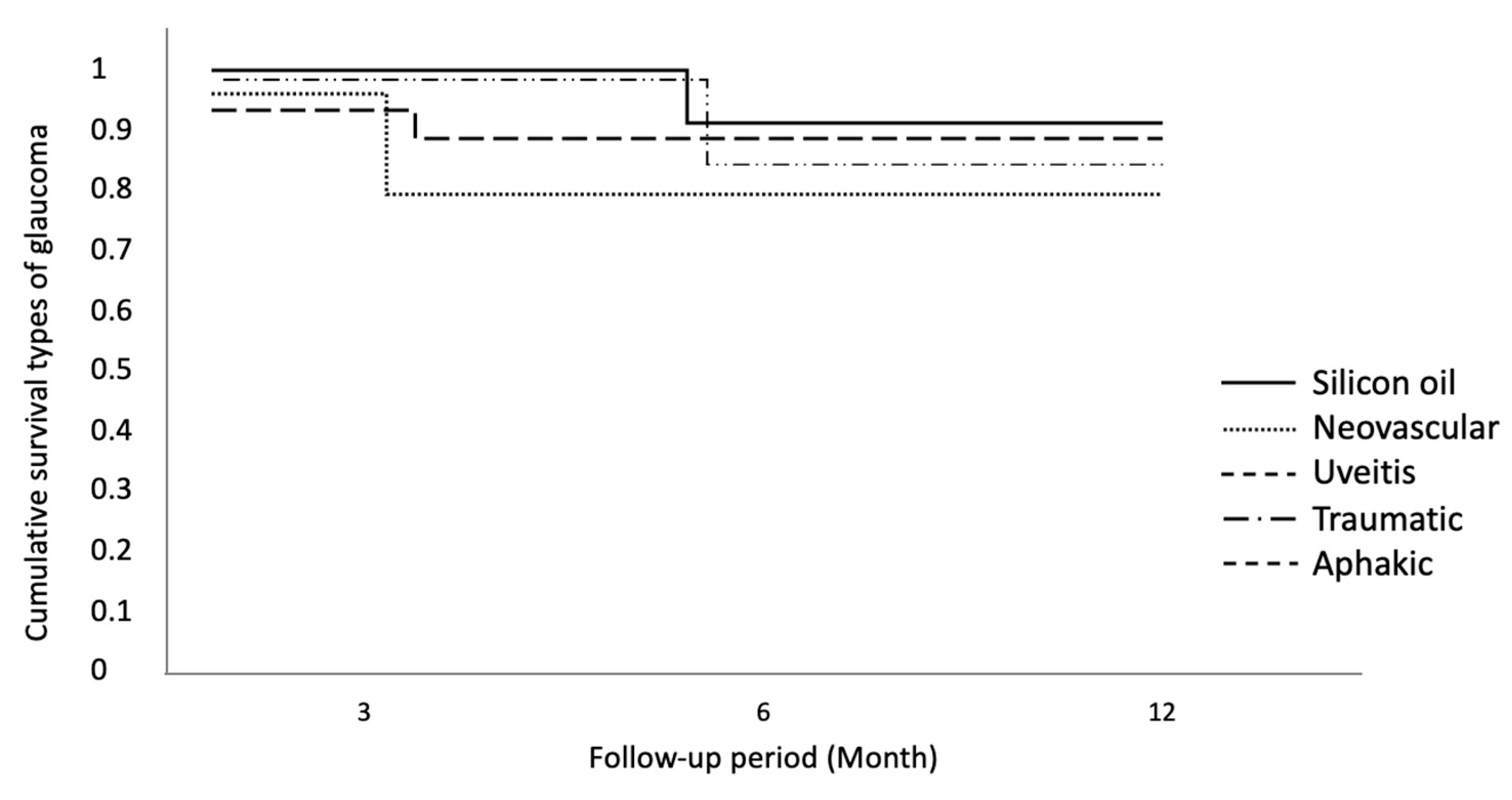
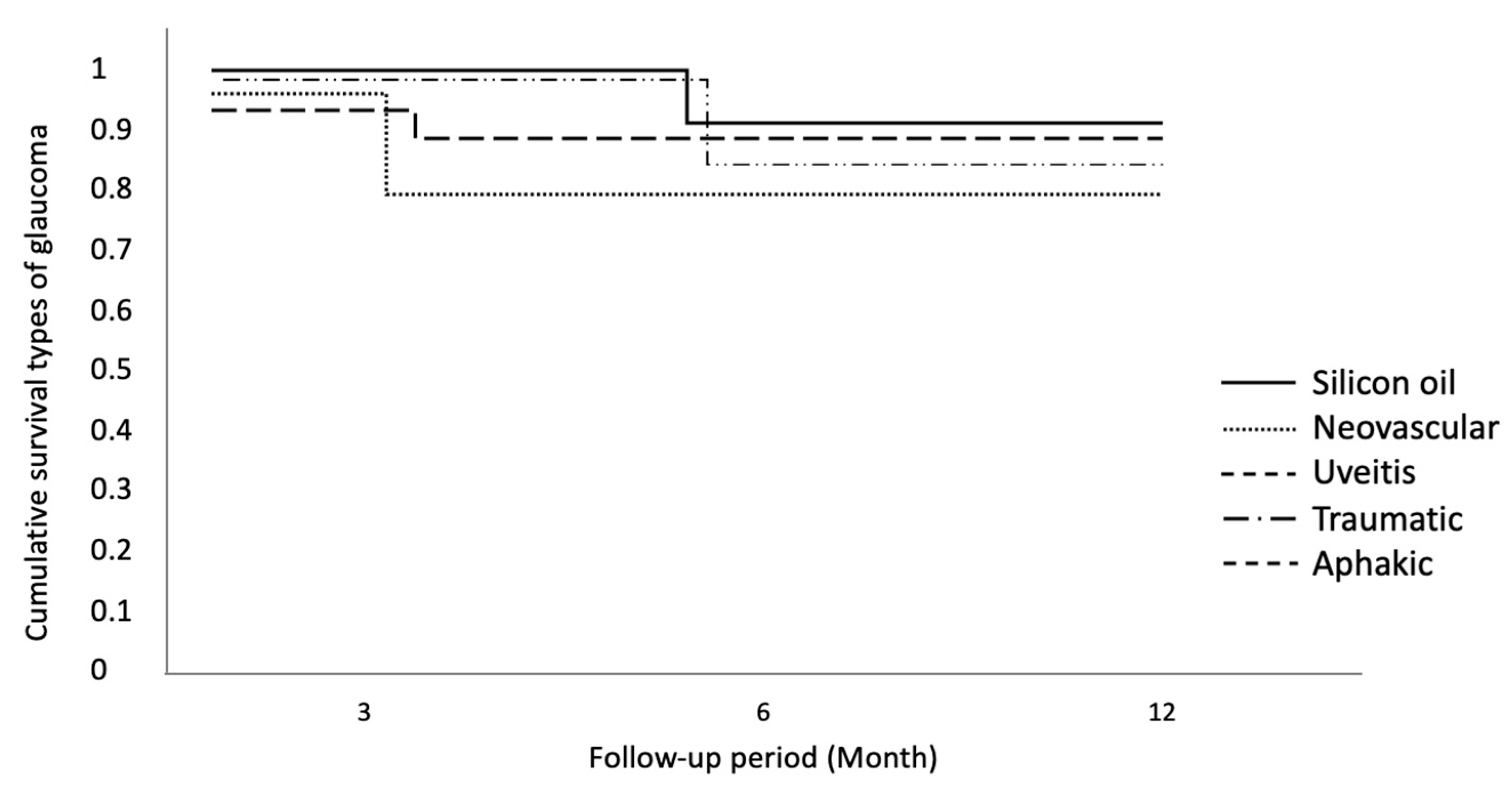
| Type of glaucoma | ||
| Silicon oil | 42 | 31.34% |
| Neovascular | 28 | 20.90% |
| Uveitis | 19 | 14.18% |
| Traumatic | 33 | 24.63% |
| Aphakic | 12 | 8.96% |
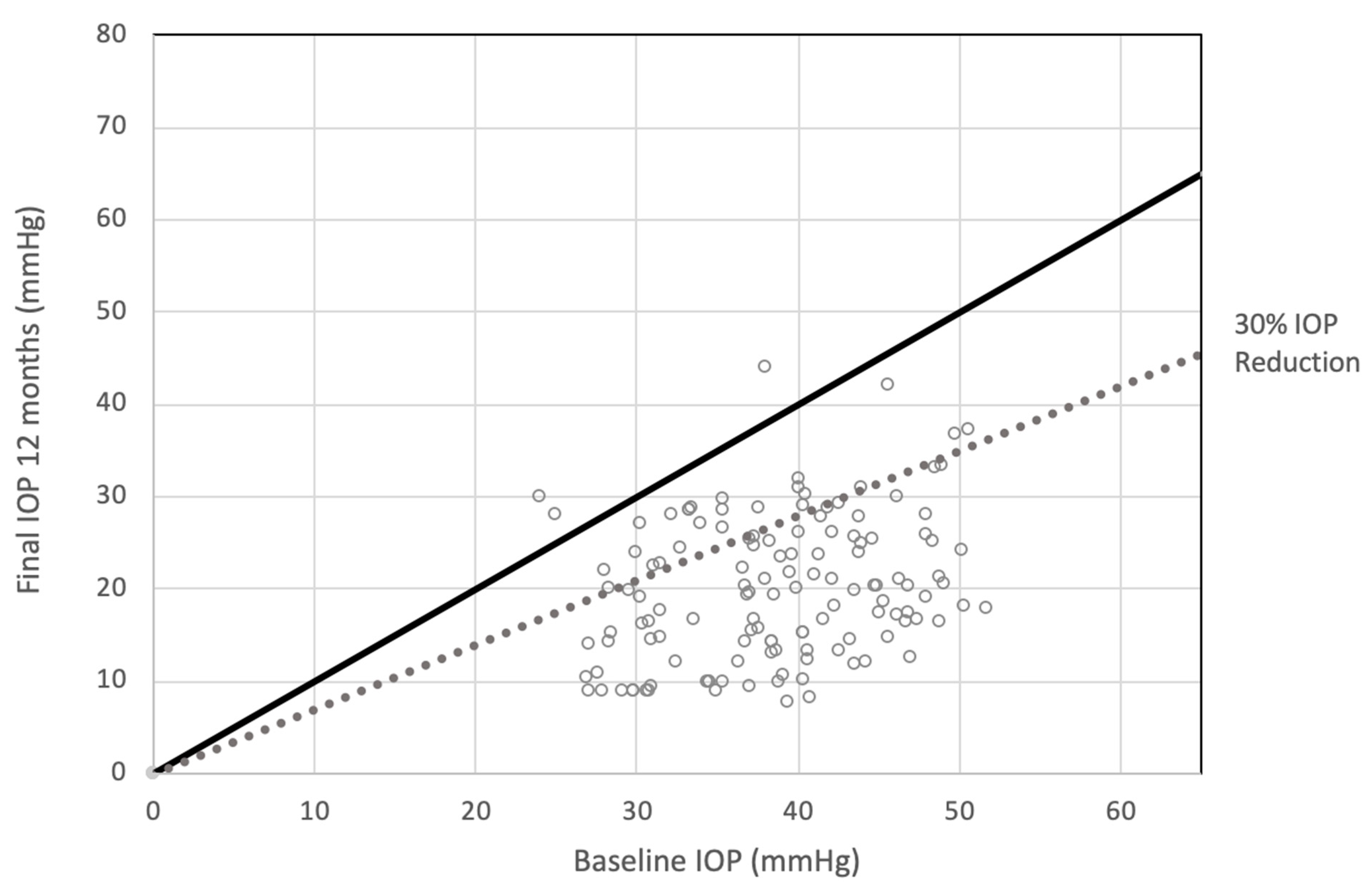
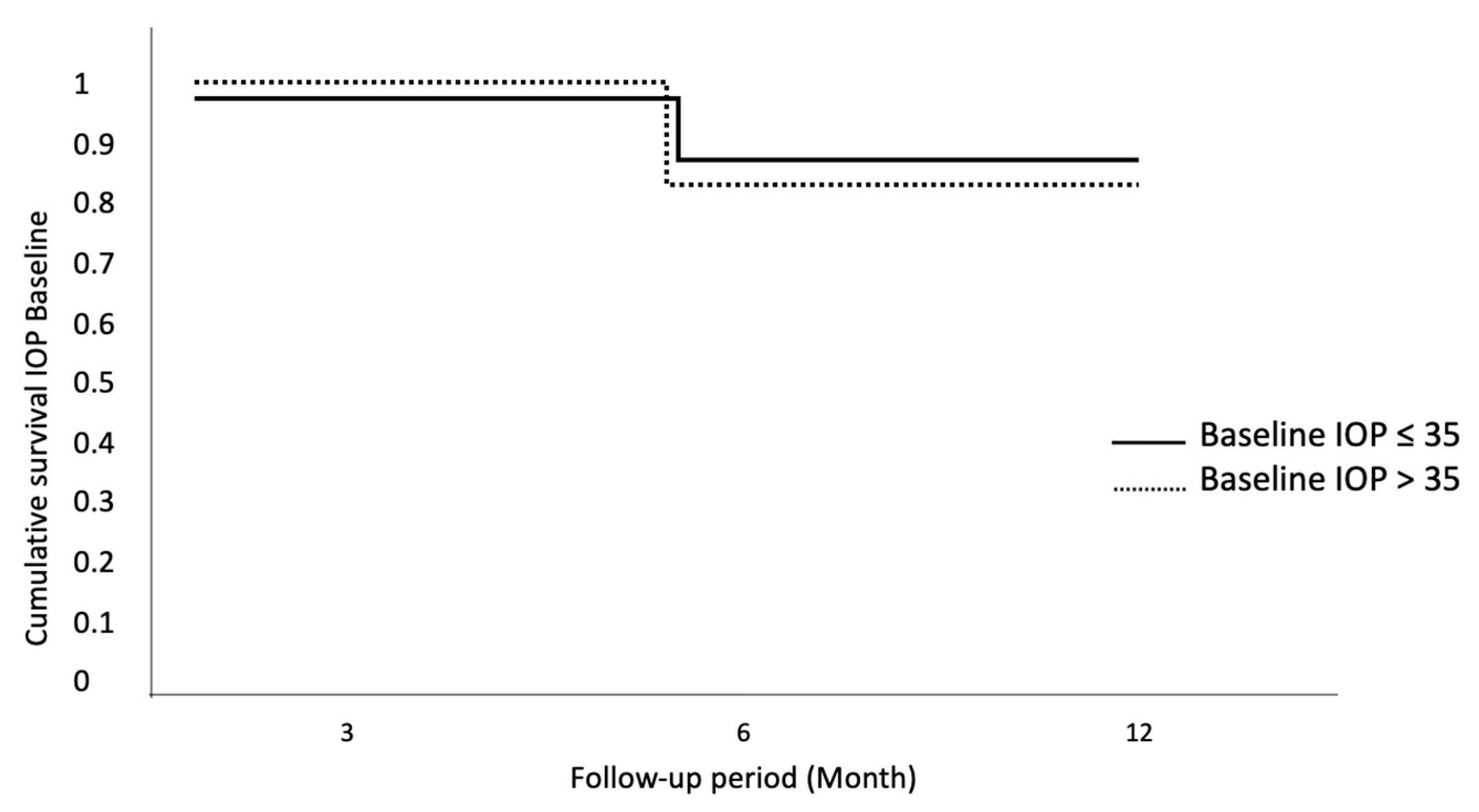
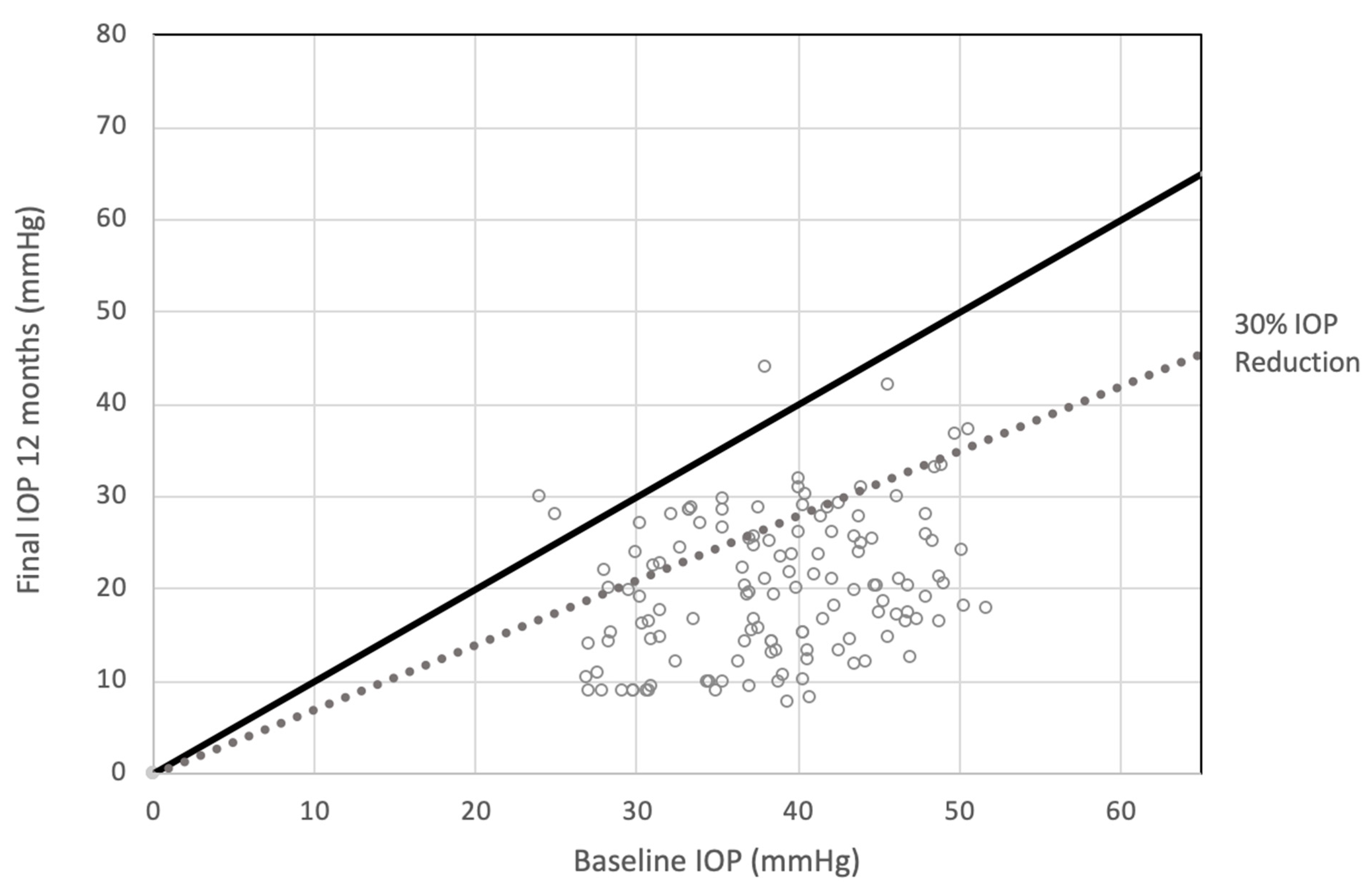
| Baseline IOP * in mmHg. mean ± SD (range) | 38.87 ± 6.93 (27–60) | |
| Number of AGM ǂ. mean ± SD | 4.57 ± 0.75 | |
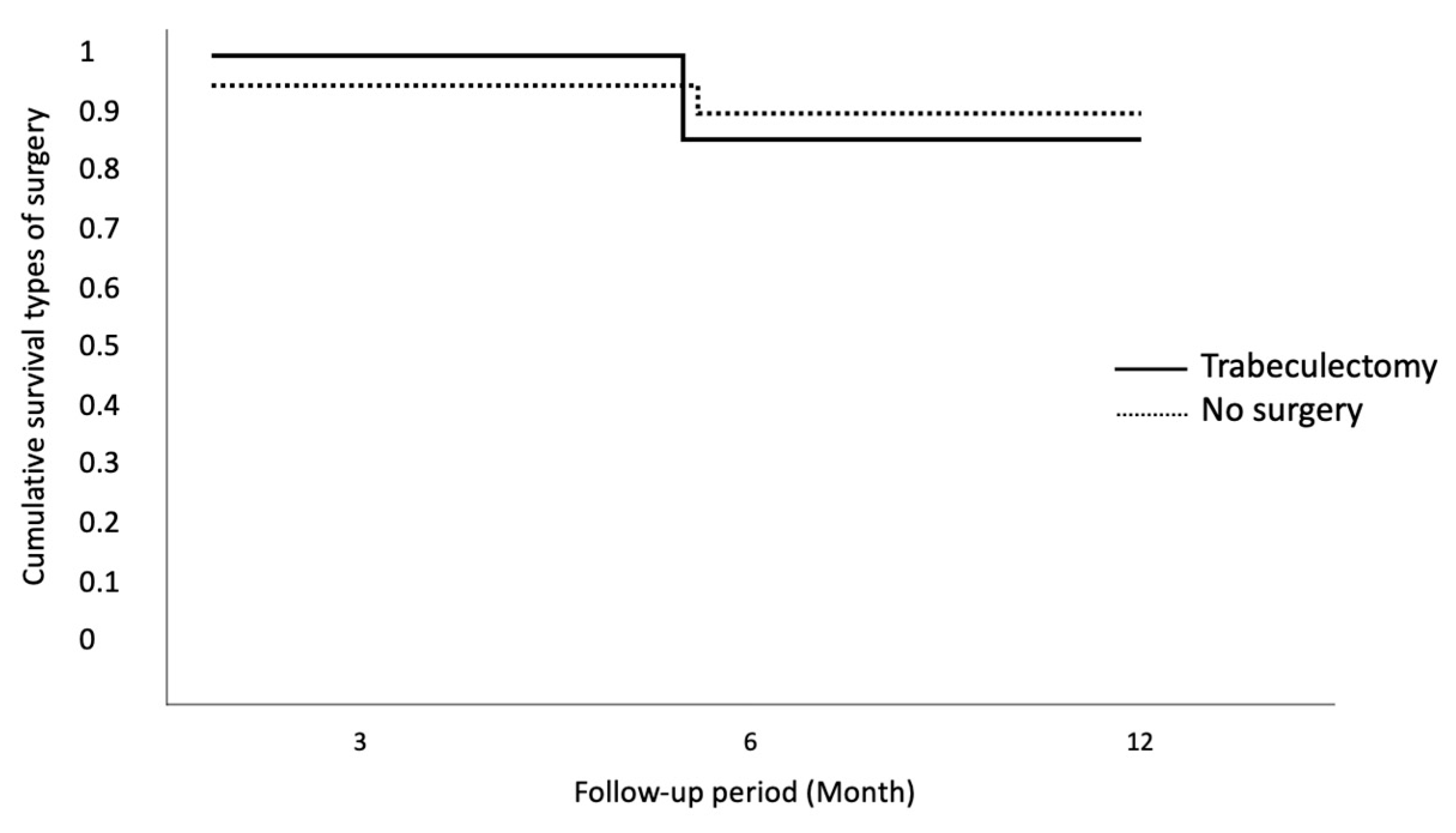
| Type of surgery | ||
| Trabeculectomy | 110 | 82% |
| No surgery | 24 | 18% |
| Pretreatment | 3 Months | 6 Months | 12 Months | |
|---|---|---|---|---|
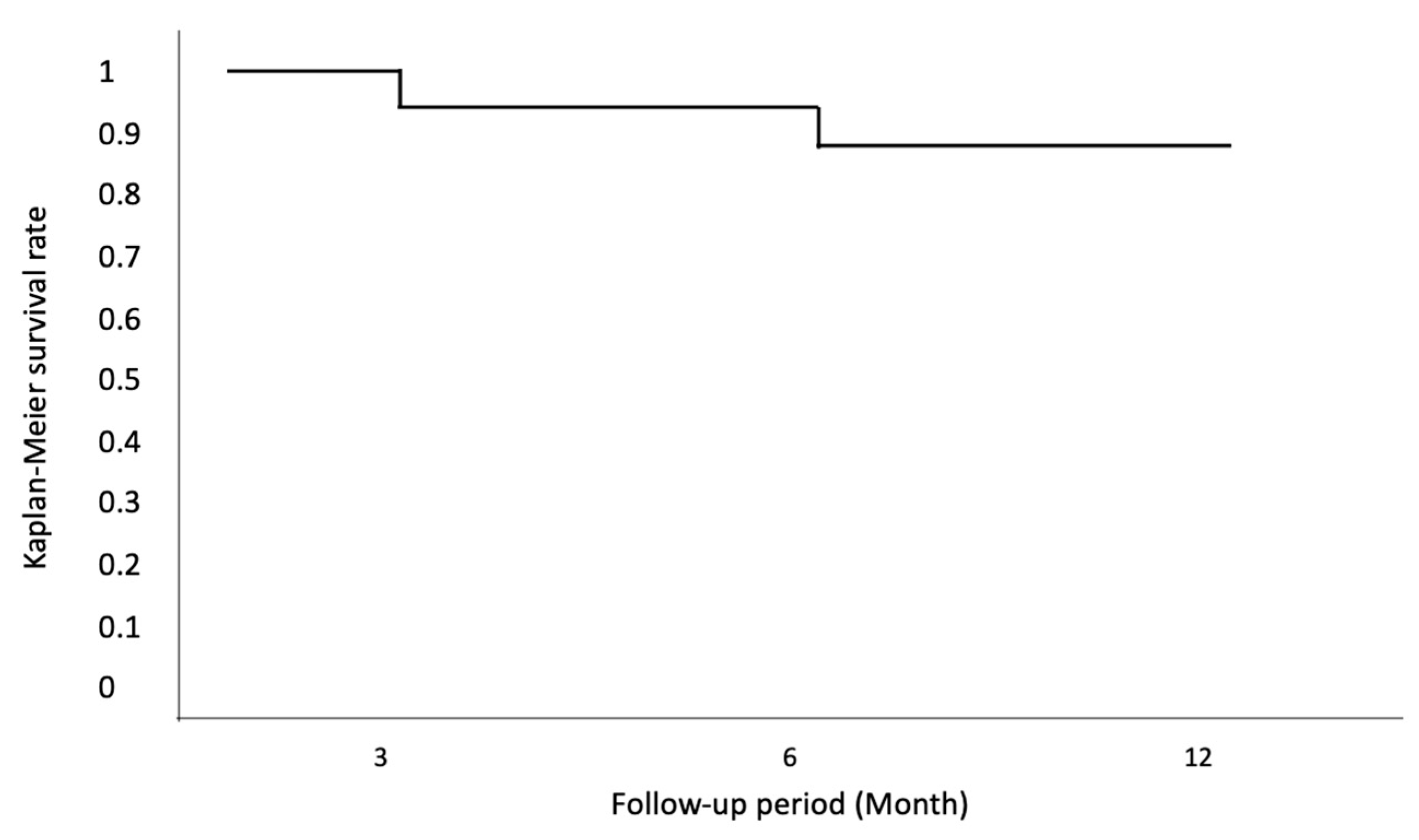
| Eyes. n | 134 | 134 | 134 | 132 |
| Eyes with an IOP decrease. n | - | 134 | 132 | 129 |
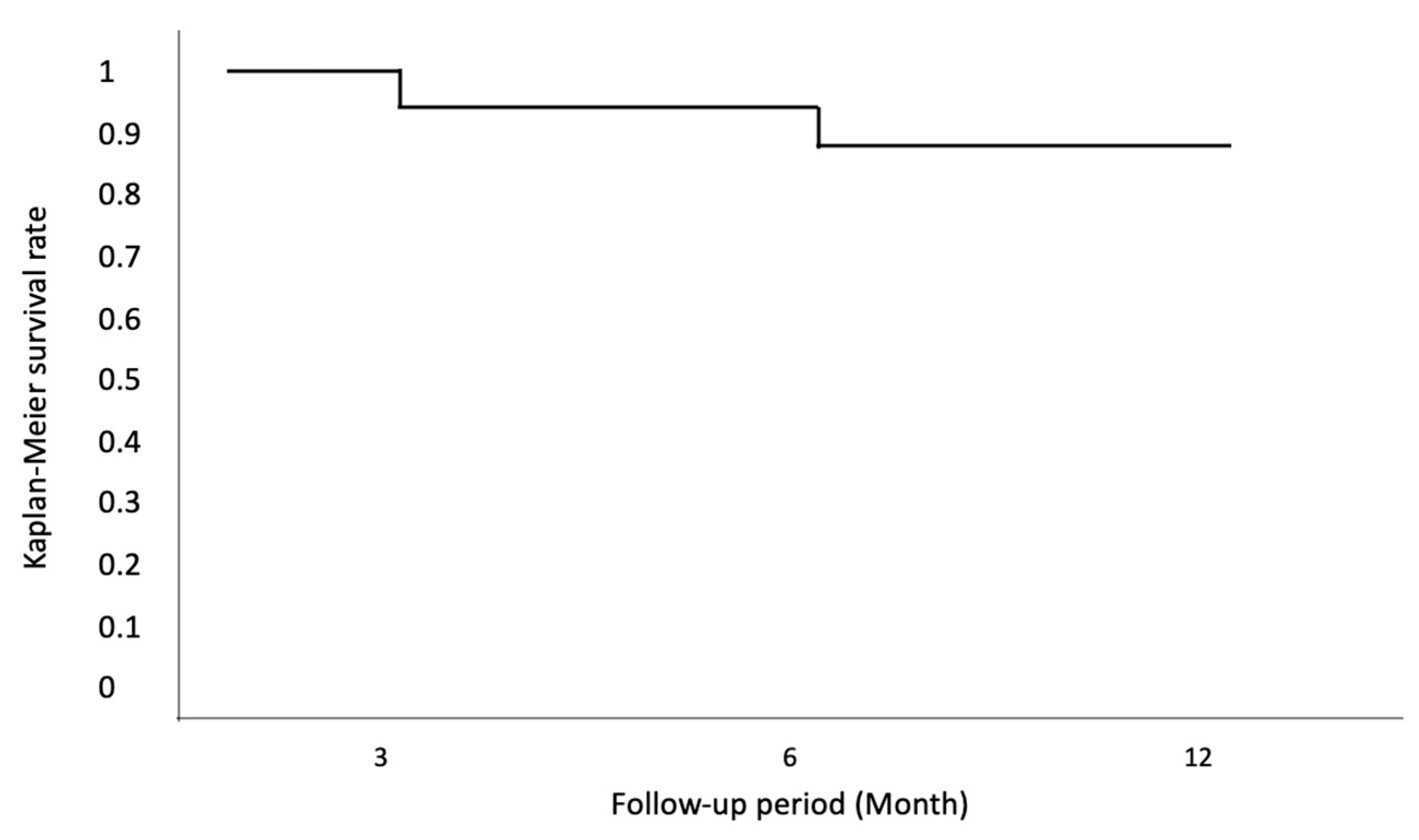
| % eyes with a decrease in IOP | - | 100 | 98.51 | 97.73 |
| Eyes with IOP < 21 mmHg. n | - | 78 | 76 | 75 |
| % Eyes with IOP < 21 mmHg (%) | - | 58.21 | 56.72 | 55.97 |
| Eyes with a decrease in IOP > 30%. n | - | 129 | 113 | 106 |
| % eyes with a decrease in IOP > 30% | - | 96.27 | 85.61 | 82.17 |
| Pretreatment | 3 Months | 6 Months | 12 Months | |
|---|---|---|---|---|
| Eyes. n Mean IOP. mmHg | 134 | 134 | 132 | 132 |
| 38.87 ± 6.93 | 14.99 ± 3.88 | 16.78 ± 8.25 | 19.89 ± 8.6 | |
| Dev Std (+/−) | 6.93 | 3.88 | 8.25 | 8.6 |
| Range (min–Max) | 27–60 | 9–29 | 10–45 | 8–44 |
| Mean IOP reduction. mmHg | - | 23.88 | 22.09 | 18.98 |
| % reduction | - | 61.44 | 56.83 | 48.83 |
| p-value for IOP change (vs. baseline) | - | p < 0.001 | p < 0.001 | p < 0.001 |
| Mean visual acuity (LogMAR) | 1.3 | 1.2 | 1.3 | 1.3 |
| Dev Std (+/−) | 0.1 | 0.1 | 0.3 | 0.2 |
| p-value for visual acuity (vs. baseline) | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| Pretreatment | 6 Months | 12 Months | |
|---|---|---|---|
| AGM. n | 4.57 | 2.25 | 2.36 |
| Dev Std (+/−) | 0.75 | 1.6 | 1.7 |
| Range (min–Max) | 3–6 | 0–6 | 1–6 |
| No. of Patients | 134 | 114 | 117 |
| % Patients | - | 85.07 | 87.31 |
| p-value for AGM change (vs. baseline) | - | p < 0.001 | p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Giudice, G.; Miceli, G.; Tumminello, G.; Trapani, A.; Pioppo, A. A Case Series of Transscleral Cyclophotocoagulation Nd:YAG Laser in Refractory Glaucoma. J. Clin. Transl. Ophthalmol. 2023, 1, 97-106. https://doi.org/10.3390/jcto1040012
Lo Giudice G, Miceli G, Tumminello G, Trapani A, Pioppo A. A Case Series of Transscleral Cyclophotocoagulation Nd:YAG Laser in Refractory Glaucoma. Journal of Clinical & Translational Ophthalmology. 2023; 1(4):97-106. https://doi.org/10.3390/jcto1040012
Chicago/Turabian StyleLo Giudice, Gregorio, Giuseppe Miceli, Giuseppe Tumminello, Alessandro Trapani, and Antonino Pioppo. 2023. "A Case Series of Transscleral Cyclophotocoagulation Nd:YAG Laser in Refractory Glaucoma" Journal of Clinical & Translational Ophthalmology 1, no. 4: 97-106. https://doi.org/10.3390/jcto1040012
APA StyleLo Giudice, G., Miceli, G., Tumminello, G., Trapani, A., & Pioppo, A. (2023). A Case Series of Transscleral Cyclophotocoagulation Nd:YAG Laser in Refractory Glaucoma. Journal of Clinical & Translational Ophthalmology, 1(4), 97-106. https://doi.org/10.3390/jcto1040012