1. Introduction
Since the first ocular echogram was performed in 1956, ultrasound has become a valuable tool for visualizing ocular structures. The anatomy of the eye facilitates insonation in several ways. Its superficial placement allows ultrasound waves to travel without obstruction, and the physical properties of its fluid-filled chambers allow facile ultrasound transmission to both the anterior and posterior segments. Moreover, ultrasound probes are mobile, which allows operators to approach the eye at different incident angles to capture high-quality images [
1]. These features make ocular ultrasound an indispensable diagnostic tool.
Although ultrasound is most often used at frequencies greater than 8 MHz as an imaging modality in the ophthalmology clinic, its therapeutic role is not fully defined [
2]. One recent development relevant to therapeutic ultrasound in the eye involves high-intensity focused ultrasound (HIFU) to treat glaucoma [
3]. HIFU coagulates the ciliary body to modulate aqueous humor production and subsequently reduces intraocular pressure [
3,
4,
5]. The use of ultrasound has also been studied in the context of ocular drug delivery. Methods of ultrasound-targeted drug delivery have included nano- and microparticles, including liposomes and micelles, phase-change agents, and thermally responsive materials [
6]. Notably, ultrasound-sensitive monodisperse microbubbles have been noted as optimal for ultrasound-mediated drug delivery, as their acoustic shadows allow ultrasound operators to selectively target tissues [
7]. Due to the complex anatomy and physiology of the eye, drugs are often absorbed in subtherapeutic doses due to physical obstruction [
8]. To achieve an adequate therapeutic window in ocular tissues, many compounds would need to be infused intravenously at such high concentrations as to cause significant systemic side effects. Ultrasound-assisted drug delivery in the eyes represents a potential solution to this challenge.
Few studies have assessed the relationship between pulsed ultrasound and antineoplastic agents in vitro. Prior studies have demonstrated that low-level ultrasound in combination with Adriamycin and diaziquone reduces uterine cervical squamous cell tumor size in vitro and in vivo [
9]. Ultrasound has also been demonstrated to enhance the delivery of dexamethasone sodium phosphate through the cornea in vivo [
10]. Yet, no reported studies have explored the impact of pulsed ultrasound on the cytotoxicity of antineoplastic drugs in cultured human retinal pigment epithelium (ARPE-19) cells. Due to its established cytotoxicity, doxorubicin, an anthracycline, was chosen as a model compound for our in vitro study. Cisplatin, a platinum analog and alkylating agent with known retinotoxic effects, including retinopathy, ischemia, and hemorrhage, was also evaluated [
11]. Moreover, doxorubicin and cisplatin are two drugs commonly used to treat ocular melanoma [
8]. These two drugs were chosen for our study because of this reason and also because they have well-defined toxicity profiles and dose–response effects in the ARPE-19 cell line, therefore serving as useful tools to interrogate the effect of pulsed ultrasound on their cytotoxicity.
The goal of the present study is to characterize the effects of pulsed ultrasound in the presence of doxorubicin and cisplatin as a method to modulate drug toxicity in ARPE-19 cells and expand upon its potential therapeutic role in ocular drug delivery.
2. Materials and Methods
2.1. ARPE-19 Cell Culture
ARPE-19 cells were cultured following the protocol established in the Hamid et al. study [
12]. It should be noted that this study utilized passages 5–7 of ARPE-19 cells.
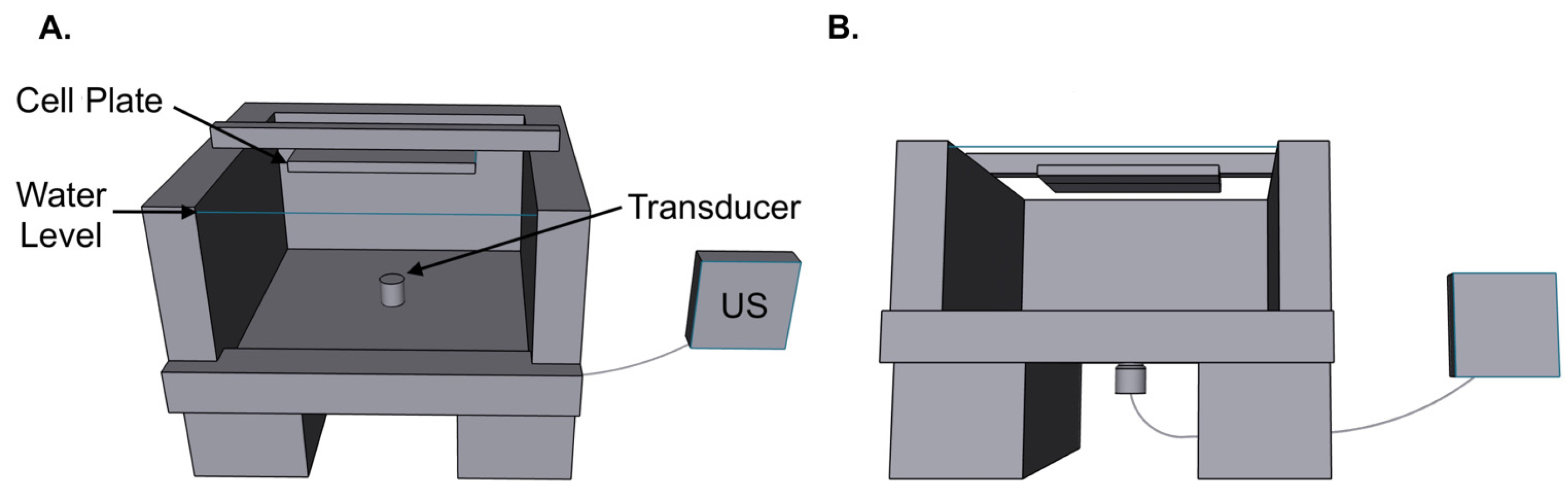
2.2. Pulsed Ultrasound Apparatus
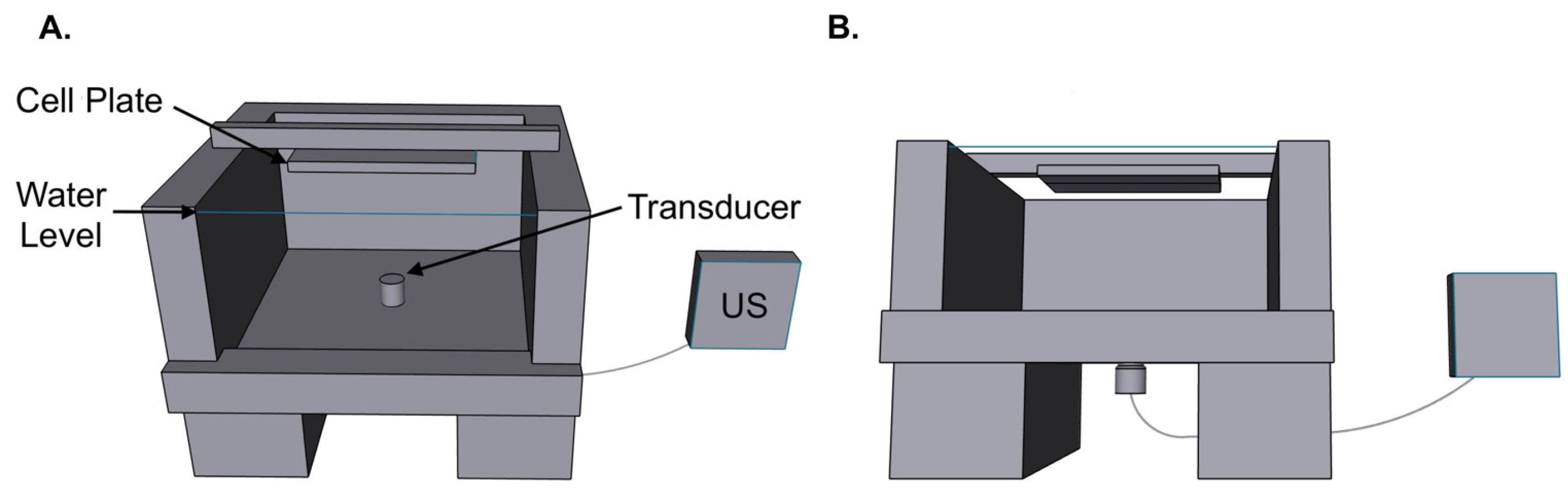
Our experimental ultrasound apparatus included a room-temperature water bath with a 0.5-inch inlet on its inferior surface for the ultrasound transducer to enter; a stand to elevate and stabilize the water bath and transducer, and a rig to fix the inverted cell plate at the focal point of the transducer (
Figure 1). ARPE-19 cells (ATCC
® CRL-2302
TM; American Type Culture Collection, Manassas, VA, USA) were plated on 96-well plates with 360 μL of media. Cell plates were saturated with culture media and sealed with MicroAmp
TM Optical Adhesive Film (Thermo Fisher Scientific, Austin, TX, USA), inverted, and submerged in the water bath to mitigate potential noise from the air–liquid interface and maximize ultrasound penetrance. After inversion, cell plates were fixed 1 inch from the transducer and displaced laterally in a controlled fashion for 5 min at a constant velocity to ensure uniform ultrasound exposure (
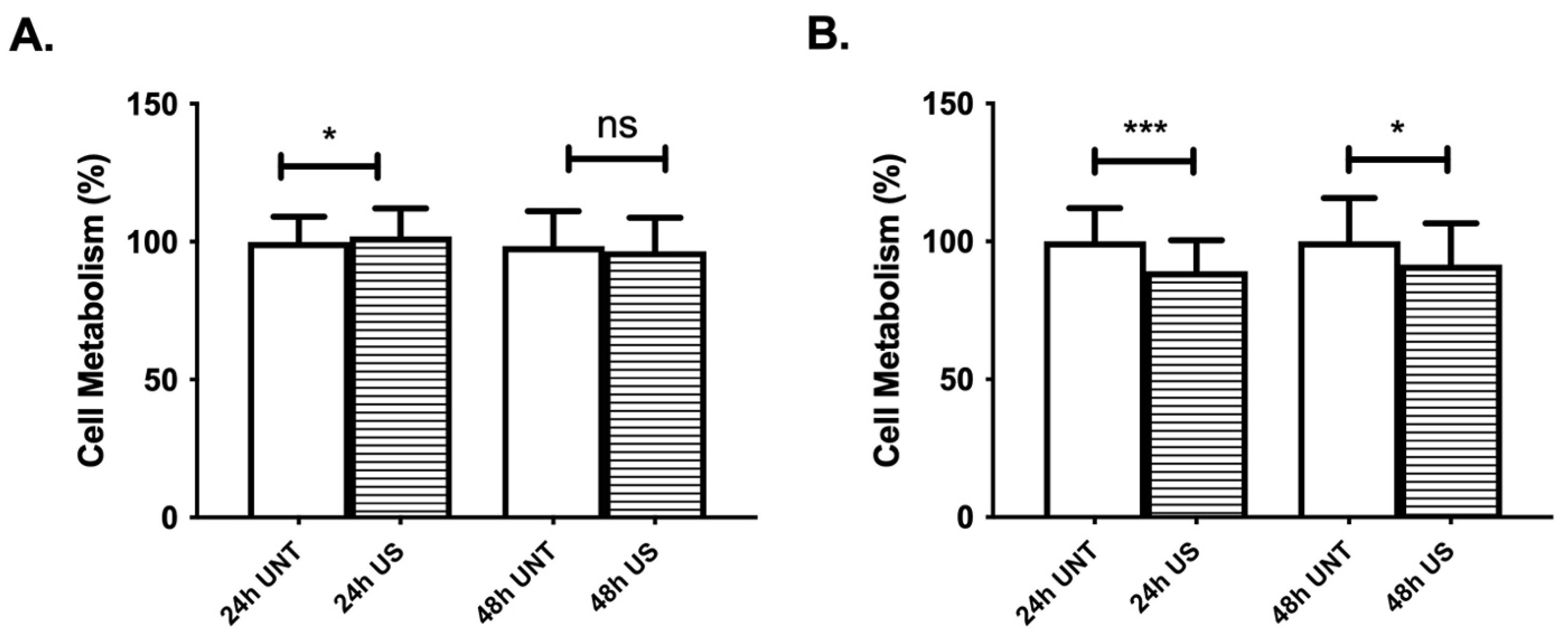
Figure 1). A portable Olympus EPOCH 650 system (Waltham, MA, USA) was used to generate ultrasound waves. ARPE-19 cells were initially subject to ultrasound at a frequency of 1 MHz, a power of 4.93 W/cm
2, and a pulse repetition frequency (PRF) of 100 Hz for 5 min based on prior ultrasound experiments on ARPE-19 cells reported in the existing literature [
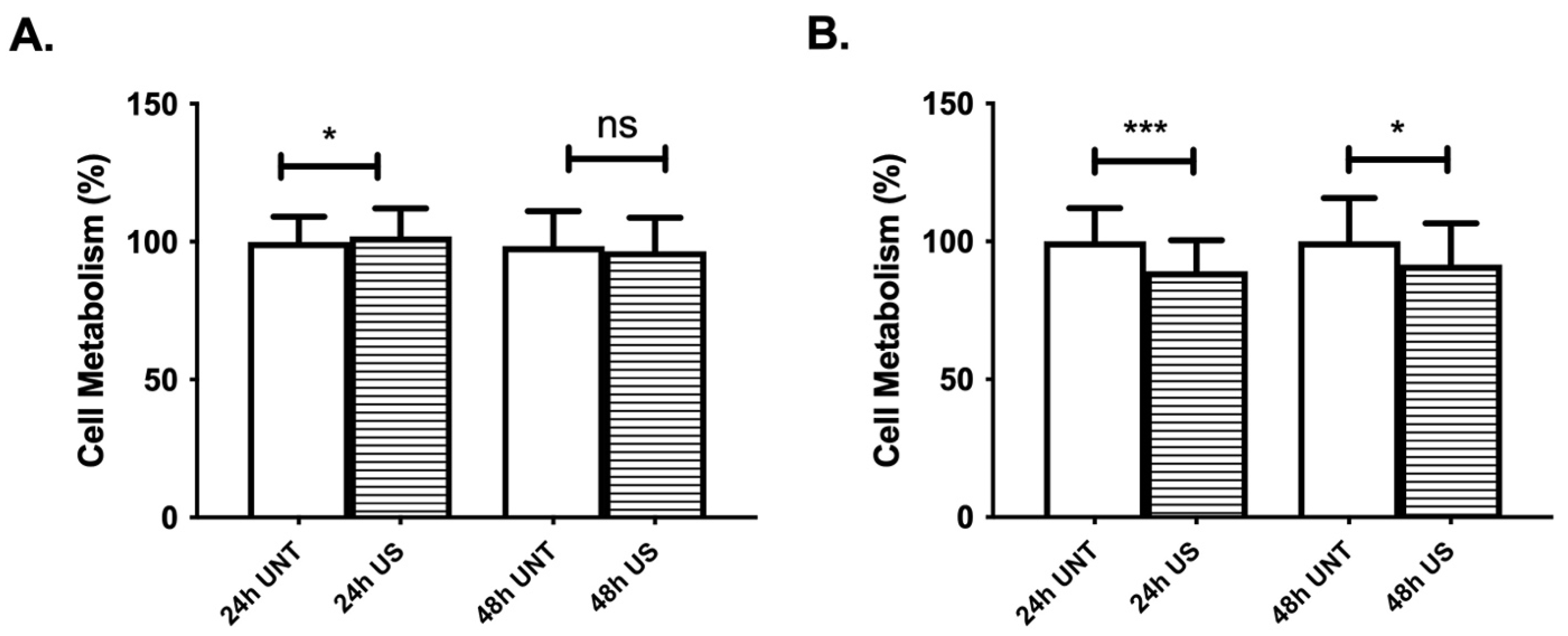
13]. Experiments were then repeated with the same parameters but at a PRF of 30 Hz, because ultrasound treatment at a PRF of 100 Hz exerted a significant decrease in cell metabolism at baseline (
Figure 2B). 3-[4,5-dimethylthiazol-2-yl]-2,5 diphenyltetrazolium bromide (MTT) assay was performed at 24 and 48 h to assess the effects of ultrasound on cell metabolism.
2.3. Doxorubicin-HCl and Cisplatin Toxicology
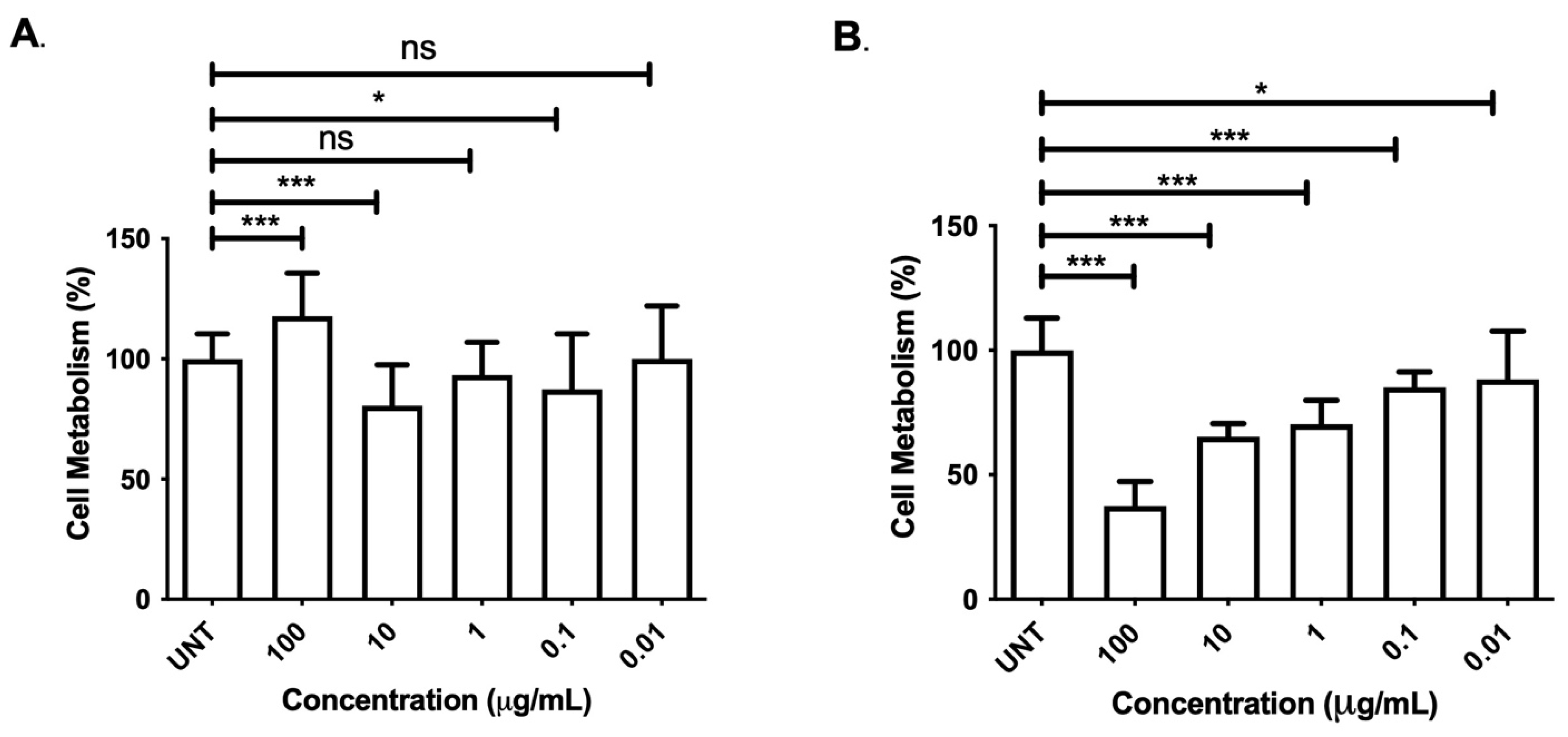
Doxorubicin-HCl toxicity in ARPE-19 cells was evaluated before pulsed ultrasound experiments. As working concentrations, 0.01, 0.1, 1, 10, and 100 μg/mL doxorubicin-HCl were chosen [
14]. A stock doxorubicin-HCl solution was initially created by dissolving doxorubicin-HCl (Fisher Scientific, Hanover Park, IL, USA) in DMSO; this solution was serially diluted in media to yield the working concentrations listed above. ARPE-19 cells were plated in 96-well plates containing 360 μL doxorubicin-HCl solution or media. Untreated cells were plated with media alone as experimental controls. After a 24 or 48 h incubation period, MTT assays were performed to establish the baseline toxicity of doxorubicin-HCl on ARPE-19 cells. All doxorubicin-HCl experiments were repeated three times. Cisplatin (BluePoint Laboratories, Little Island, Cork, Ireland) was used at working concentrations of 20 μM and 40 μM [
14].
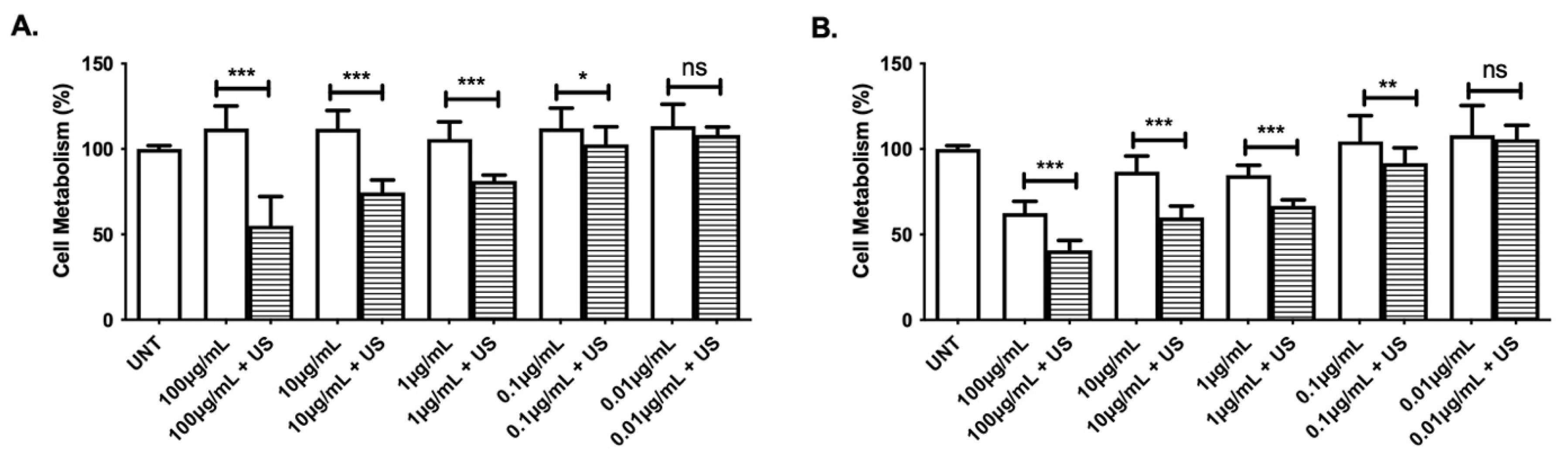
2.4. Doxorubicin-HCl, Cisplatin, and Pulsed Ultrasound Treatment
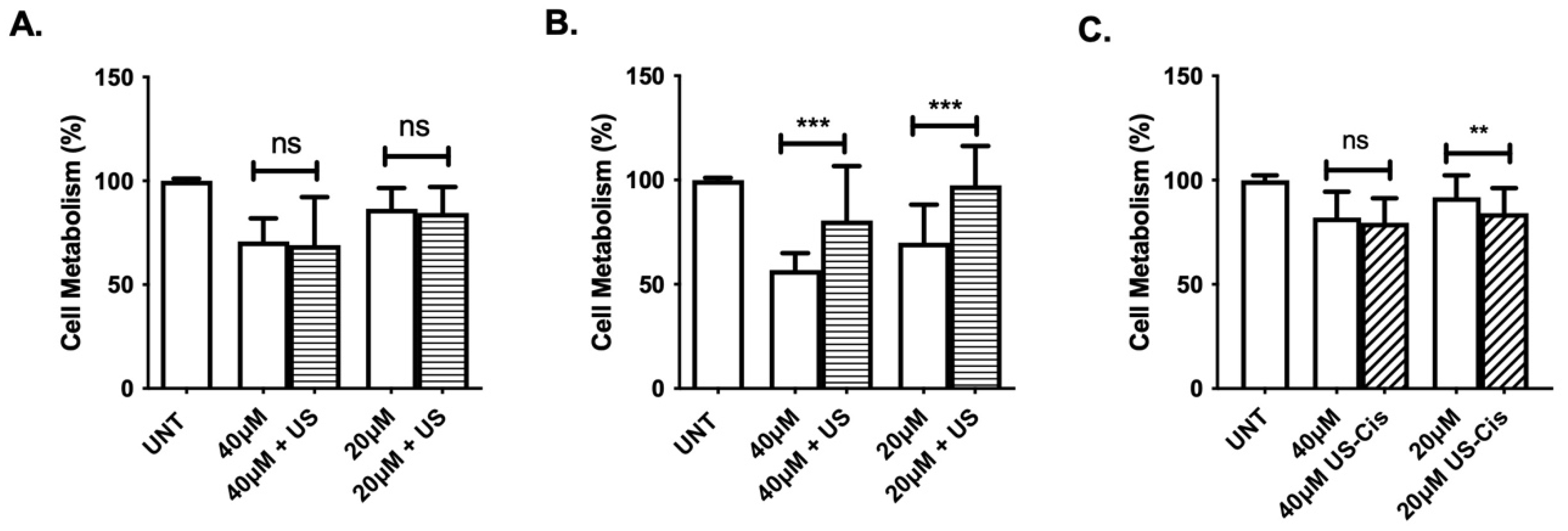
ARPE-19 cells were treated with doxorubicin-HCl or cisplatin with or without pulsed ultrasound exposure. ARPE-19 cells were initially plated in 96-well plates at a density of 1 × 105 cells/mL and treated with 360 μL doxorubicin-HCl or cisplatin solution. Doxorubicin-HCl was used at the concentrations described in Doxorubicin-HCl and Cisplatin Toxicology. After loading wells with doxorubicin-HCl or cisplatin, cell plates were treated with 1 MHz ultrasound at a power of 4.93 W/cm2 and PRF of 30 Hz. Pulsed ultrasound was not applied to control wells. Media were removed and wells were refreshed with doxorubicin-HCl or cisplatin solution. Plates were then incubated for 24 or 48 h at 37 degrees Celsius and 5% CO2 saturation. Following incubation, MTT assay was performed to assess metabolic activity as a proxy for cell viability. To determine if pulsed ultrasound treatment influences cisplatin toxicity, experiments were repeated utilizing pulsed ultrasound-treated cisplatin (US–Cis). First, cisplatin was treated with 1 MHz ultrasound at a power of 4.93 W/cm2 and PRF of 30 Hz. US–Cis was then added to the cultured cells. Plates were inverted and placed in the water bath, but no further pulsed ultrasound was applied to experimental groups. Plates were incubated for 48 h, and cell metabolism was assessed via the MTT assay described below.
2.5. Measurement of Cell Metabolism (MTT Assay)
The MTT (3-[4,5-dimethylthiazol-2-yl]-2,5 diphenyltetrazolium bromide) assay, based on the conversion of MTT to insoluble formazan crystals via NADPH-dependent oxidoreductases, was used to assess cellular metabolism as a proxy for cell viability, as described by T. Mosmann [
15]. MTT assay was primarily used to evaluate the in vitro cytotoxic effects of antineoplastic drugs. Assay outputs were quantified by a BioTek ELx808 spectrophotometer (Lonza Bioscience, Basel, Switzerland) at 570 nm and 630 nm. Results are expressed as percent of cell viability relative to untreated controls. Each experiment was independently repeated three times with three technical replicates per group per experiment.
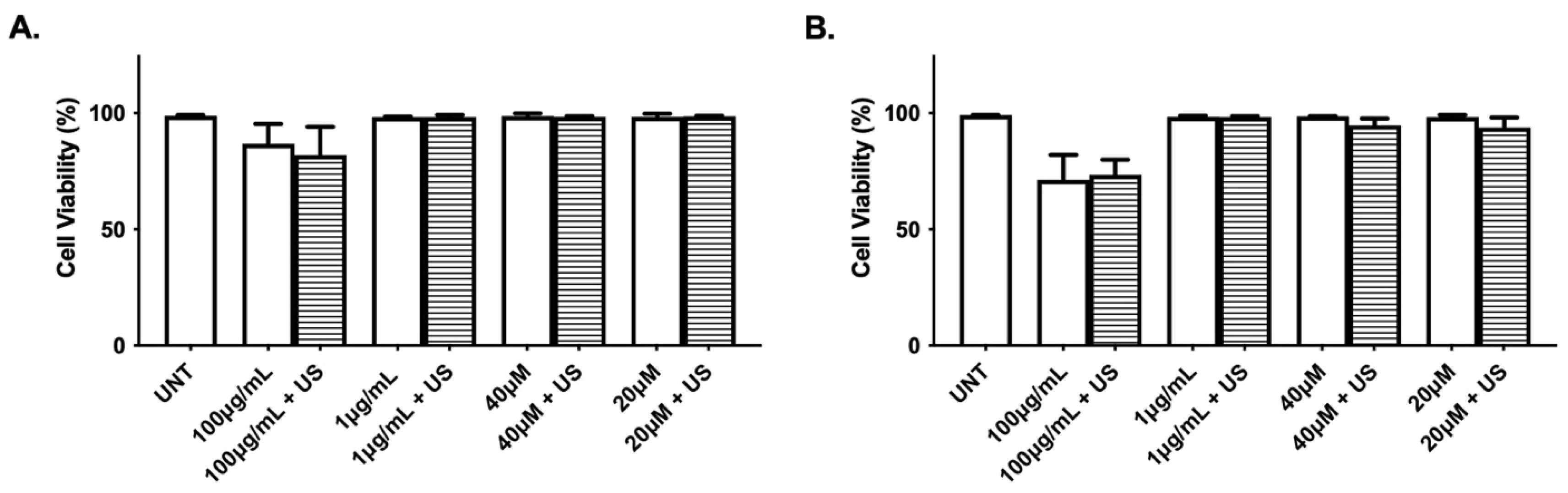
2.6. Measurement of Cell Death (Trypan Blue Assay)
Trypan blue exclusion assays were conducted to assess cell death. In total, 5 × 10
5 ARPE-19 cells were plated in 6-well plates. After a 24 h incubation period, media were replaced with either doxorubicin-HCl (100 μg/mL or 1 μg/mL) or cisplatin (40 μM or 20 μM). Half of the wells were treated with 90 s of 1 MHz ultrasound at a PRF of 30 Hz. The medium in each well was aspirated to a final volume of 2 mL. Trypan blue exclusion assay, as described by Strober [
16], was performed 24 and 48 h post treatment and read using a Vi-CELL XR Cell Viability Analyzer (Beckman Coulter).
2.7. Statistical Analysis
Unpaired two-tailed tests were used for statistical analysis via Prism 8 (GraphPad Software, San Diego, CA, USA). p-values < 0.05, <0.01, <0.001, <0.0001 are denoted as *, **, ***, and ****, respectively, and all denote statistical significance; nonsignificance is denoted as “ns”. All statistical tests were run on three independent repeats of three replicates. All values are expressed as average ± standard deviation.
4. Discussion
The salient findings of the present investigation are the (1) dose-dependent effects of doxorubicin-HCl and cisplatin on ARPE-19 cell metabolism, (2) the ultrasonic enhancement of doxorubicin-HCl toxicity, (3) the ultrasonic modulation of cisplatin toxicity, (4) a nonsignificant effect of pulsed ultrasound on cisplatin- and doxorubicin-treated cells on cell death, and (5) a viable pulsed ultrasound apparatus for use in vitro. These findings underscore the ability of ultrasound to regulate the cytotoxicity of antineoplastic agents in a drug-specific manner in cultured retinal epithelial cells and demonstrate its potential as a modulator of drug potency.
Because antineoplastic drugs such as doxorubicin-HCl and cisplatin are broadly used in clinical medicine, it is important to identify their secondary effects on tissues such as the eye. In our study, ARPE-19 cells demonstrated a dose-dependent decrease in metabolism after doxorubicin-HCl and cisplatin treatment alone, mimicking trends found in the literature [
14,
17]. Specifically, after a 48 h incubation period, the dose-dependent decrease caused by doxorubicin-HCl mirrored previously published results of retinal epithelium cells treated with liposomal doxorubicin [
14]. Interestingly, there was a deviation from this trend at the highest dose of doxorubicin-HCl; cells treated with 100 µg/mL doxorubicin-HCl exhibited a paradoxical increase in metabolic activity 24 h post treatment. Such findings were not seen in studies of NIH3T3 (mouse fibroblast) and MCF7 (breast adenocarcinoma) cell lines that were treated with 50 µg/mL doxorubicin for a 24 h incubation period [
18], and there are minimal to no published studies that identify such a trend. These data suggest that the cytotoxic effect of doxorubicin-HCl is dose-dependent at 48 h but not at 24 h post treatment in ARPE-19 cells. This distinction may be caused by a unique activating response in cell metabolism upon treatment with an overwhelming dose of toxin; therefore, our observations may provide insight into how ARPE-19 cells respond to stress. It is also important to note that cells subjected to the highest concentration of doxorubicin-HCl with ultrasound did not demonstrate the same paradoxical increase in metabolic activity seen at 24 h post treatment in the doxorubicin-HCl-only group. We suspect this response may have occurred prior to the 24 h time point or failed to occur at all. Further studies are necessary to explore and validate these claims.
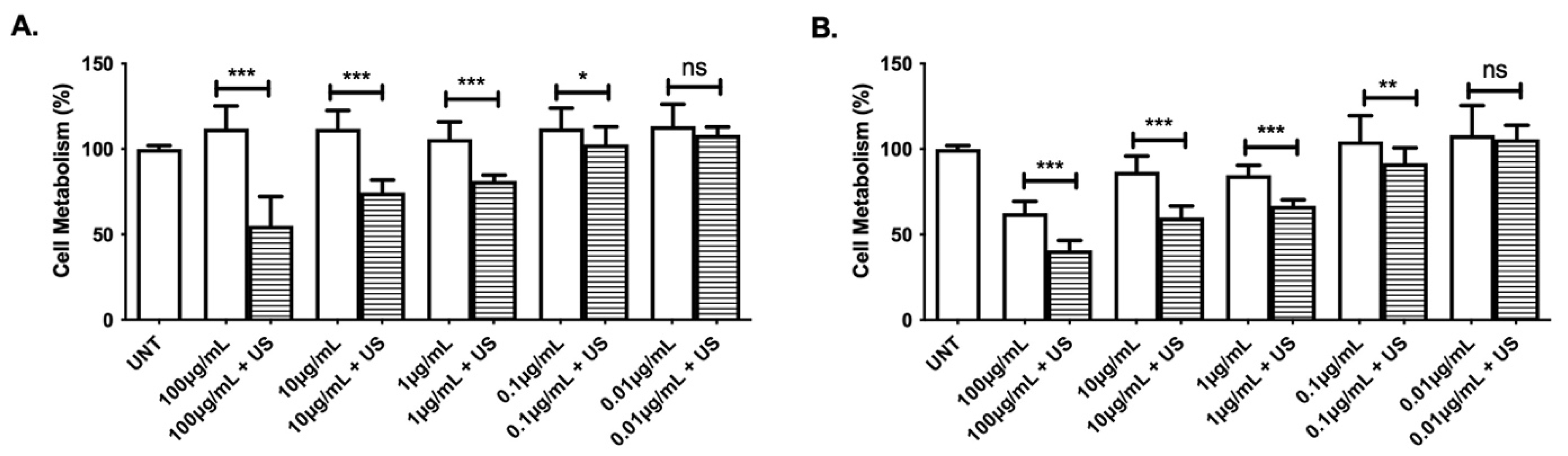
Cells treated with both ultrasound and doxorubicin-HCl displayed dose-dependent decreases in metabolic activity that were similar to those seen in cells treated with doxorubicin-HCl alone at 48 h post treatment. This toxicity was significantly amplified at both 24 and 48 h after dual treatment, suggesting that ultrasound magnifies the cytotoxic effects of doxorubicin-HCl. These findings corroborate reports in the literature demonstrating that ultrasound enhances the potency of Adriamycin on ovarian cancer in vivo [
19]. Because ultrasound treatment amplified the magnitude of doxorubicin-HCl toxicity rather than the pattern of effect, it can be concluded that ultrasound did not change doxorubicin-HCl’s functional structure.
One possible explanation for the increased cytotoxicity of doxorubicin-HCl in the presence of ultrasound involves enhanced cellular exposure to doxorubicin-HCl via ultrasound-induced cell cavitation. Similar findings have been observed in previously published work, in which ultrasound was shown to enhance the corneal permeability of dexamethasone sodium in vivo, a phenomenon theorized to be mediated by stable and inertial cavitation [
10]. This hypothesis of increased drug uptake has implications surrounding doxorubicin-HCl administration in several tissue types. Because cells subject to both ultrasound and doxorubicin-HCl exhibit a greater reduction in cell metabolism at all tested concentrations, we argue that a lower dose of doxorubicin-HCl could be combined with ultrasound to induce a cytotoxic effect comparable to that of a higher dose of doxorubicin-HCl alone. Lowering doxorubicin-HCl doses in conjunction with sonication to tissues of interest could minimize the adverse systemic side effects of doxorubicin-HCl while preserving its therapeutic effect.
In contrast to cells treated with doxorubicin-HCl, ARPE-19 cells treated with both cisplatin and ultrasound demonstrated a different response. Rather than amplifying cisplatin cytotoxicity and decreasing cell metabolism, ultrasound appeared to impart a cytoprotective effect. One theory regarding this increase in cell metabolism involves a physical modification of cisplatin’s molecular structure. To further explore this concept, we evaluated the ARPE-19 cell metabolic response to ultrasound-treated cisplatin (i.e., US–Cis). When cisplatin was pretreated with ultrasound before exposure to ARPE-19 cells, the previously described protective effect was lost. There may be a component of this apparent ultrasound-induced abrogation of cisplatin toxicity that relies on the timing and duration of ultrasound exposure. Work conducted by a different group found that low-intensity ultrasound increases the apoptotic rate of cisplatin-treated hepatocellular carcinoma cells [
20]. This finding suggests the type of sonication may also influence the cytotoxic effect of cisplatin. These findings also have important clinical implications. To minimize systemic side effects, ultrasound could conceivably be administered alongside cisplatin in ocular tissues that are particularly susceptible to cytotoxicity (e.g., retinal tissue) during cisplatin infusion.
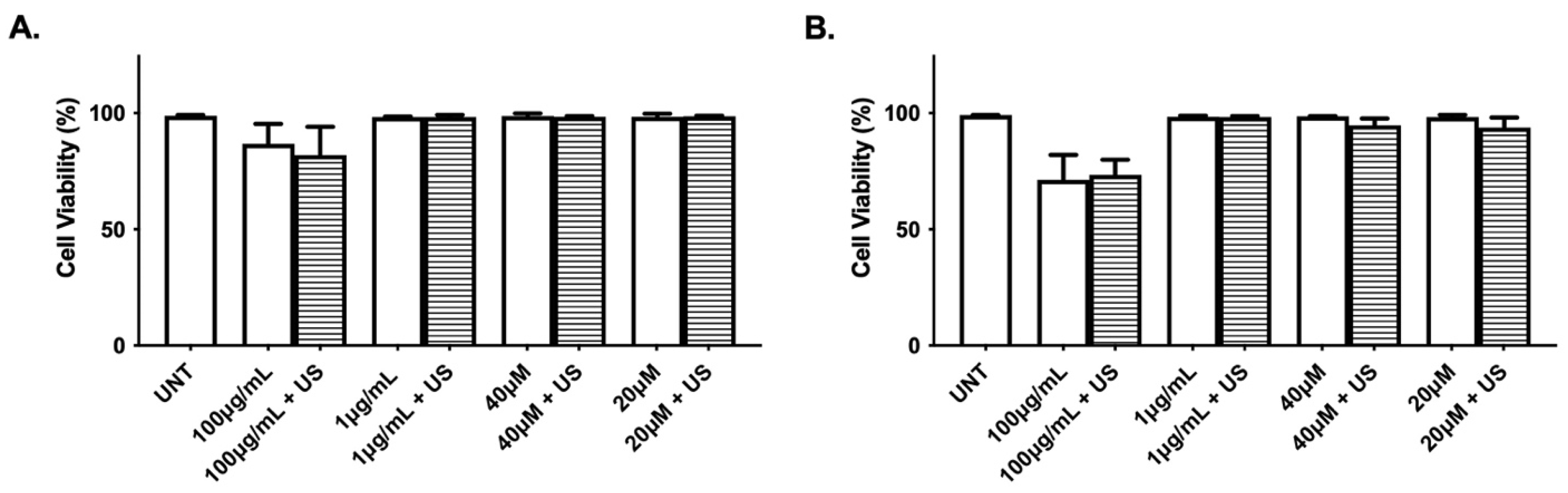
It is important to note that ultrasound did not have a significant effect on doxorubicin- and cisplatin-treated ARPE-19 cell death. This suggests ultrasonic waves may prompt a nonfatal cellular response that transiently halts metabolism when exposed to these antineoplastic agents. Additional studies are necessary to further understand why sonication in the presence of doxorubicin-HCl and cisplatin appears to modulate cell metabolic activity but spares cell death.
Our study also demonstrates a viable ultrasound apparatus for the application of pulsed ultrasound in vitro. The observed decrease in ARPE-19 cell metabolism with a 100 Hz ultrasound was suggestive of ultrasonic penetrance through the liquid–polystyrene–liquid interface, validating our pulsed ultrasound apparatus. Our sealed cell culture setup not only provides favorable parameters to test ultrasound penetration but also may have other applications in ocular drug delivery. Most notably, plate inversion allows for gas-filled particles, such as microbubbles, to rise to the cellular layer and facilitate optimal cell-particle contact. This minimizes the distance between drug and cells upon insonation.
Although there is growing interest in utilizing drug-filled microbubbles with insonation as a mechanism for targeted drug delivery, there remains a need to characterize the relationship between ultrasound and microbubble cargo in the absence of microbubbles [
21]. Our study reveals ultrasound variably influences the potency of cisplatin and doxorubicin-HCl in vitro. Future microbubble experiments should explore the effects of ultrasound on the loading medication prior to involving microbubbles, especially in the context of commonly administered intraocular drugs, such as those used in intravitreal injections to treat diabetic retinopathy. Such information is crucial to establishing our understanding of the therapeutic role of ultrasound, as well as augmenting ultrasound’s role as an ocular tool.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}