
Supplementation with Crocus sativus L. (Saffron) against Placebo in Multiple Sclerosis: A Systematic Review and Synthesis without Meta-Analysis of Randomized Controlled Trials

 , , , , ,
, , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Review Protocol and PICO
2.2. Search Strategy, Inclusion and Exclusion Criteria
2.3. Outcomes of Interest
2.4. Risk of Bias
2.5. Data Extraction
2.6. Data Synthesis
3. Results
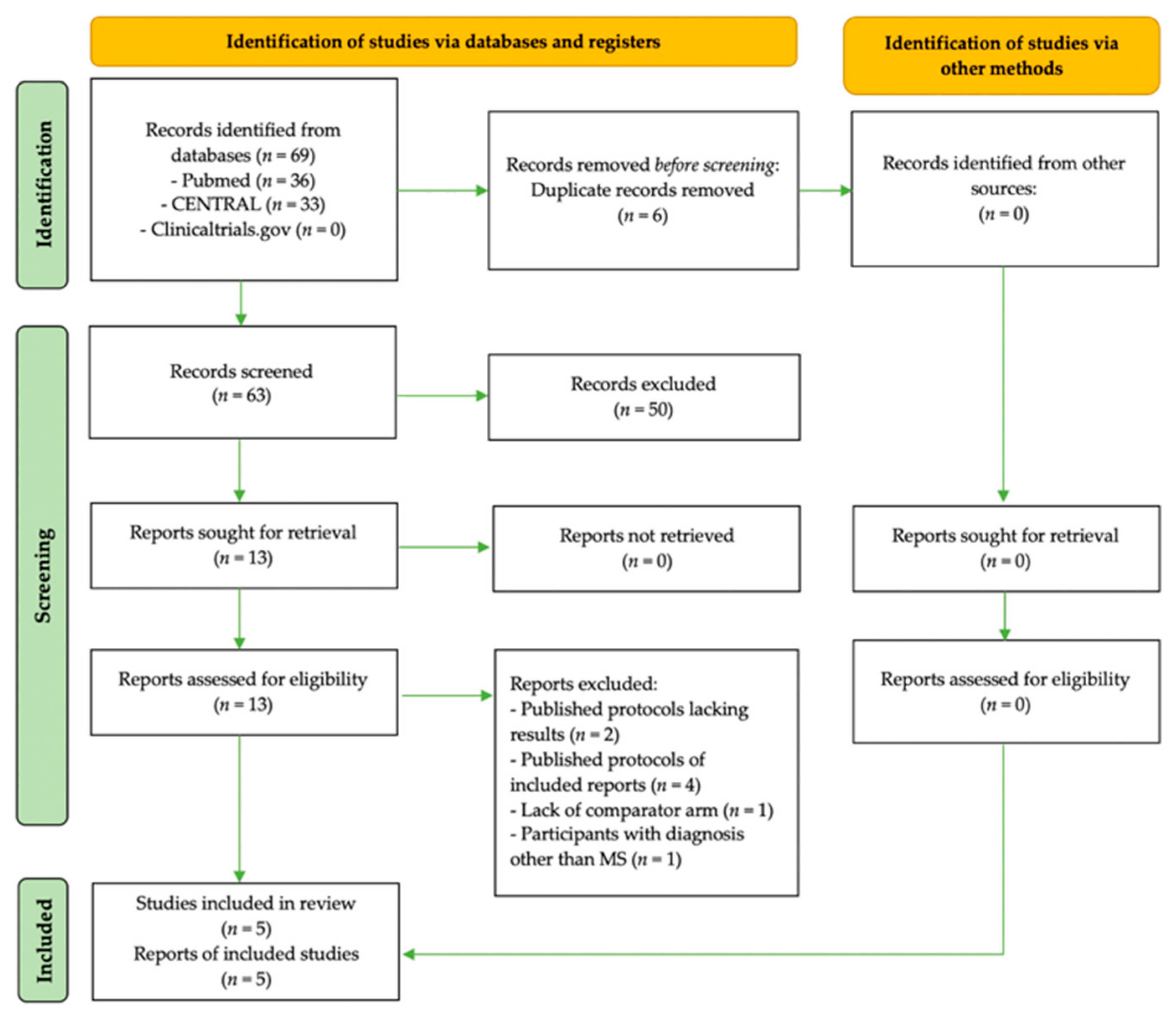
3.1. Search Results
3.2. Characteristics of RCTs with Saffron Interventions in Patients with ΜS
3.2.1. Trial Design, Origin, and MS Diagnosis
3.2.2. Intervention and Comparator Particularities
3.2.3. Sample Size

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Adalat [44] | Ahmadi [45] | Doosti [43] | Ghasemi Sakha [42] | Ghiasian [41] |
|---|---|---|---|---|---|
| Publication | Full-text | Full-text | Abstract | Full-text | Full-text |
| Journal | Galen. Med. J., 2019 | Biomedicine, 2020 | Mult. Scler J., 2019 | Iran J. Allergy Asthma Immunol., 2020 | J. Biochem. Mol. Toxicol., 2019 |
| Origin | Iran | Iran | Iran | Iran | Iran |
| Registry | IRCT2016012916369N3 | IRCT2016122013194N3 | NR | IRCT138802091859N1 | IRCT2016092713194N2 |
| Design | Parallel | Parallel | Parallel | Parallel | Parallel |
| Funding | NR | NR | NR | NR | Neurophysiology Center |
| Masking | Double blind | Double blind | Triple blind | Triple blind | Double blind |
| Randomization | Blocked, PC-generated random numbers (1:1 ratio) | “Randomly” NOD | NR | “Randomly” NOD | PC-generated sequence |
| Recruitment | Sina Hospital, Tabriz | Farshchian Hospital, Hamadan University of Medical Sciences | NR | Sina Hospital, Emam Khomeni Hospital | Farshchian Hospital, Hamadan University |
| Study duration | NR | 2017 | NR | NR | NR |
| Participants | N = 52 adult patients with MS (EDDS ≤ 6) on SSRIs | N = 40 patients with RRMS and low disability (EDSS < 4) | N = 50 adult patients with RRMS (EDSS: 0–5.5) | N = 43 adult patients with RRMS (EDSS: 0–5.5) | N = 40 patients with RRMS |
| Participant age (years) | 20–50 R | 20–40 R | 18–50 R | 18–50 R | 29 ± 5 M (intervention); 31.5 ± 5.3 M (placebo) |
| Men/women (n) | 14/38 | 5/35 | NR | 4/39 | 5/35 |
| MS diagnostic criteria | McDonald et al. [46] criteria | NR | NR | McDonald et al. [46] | McDonald et al. [46] and MRI |
| Intervention | ONS with herbal syrup (2 × 10 mL/day) with C. sativus, V. vinifera, C. verum, H. perforatum (n = 26) | ONS with crocin (2 × 15 mg caps/day) (n = 20) | ONS with saffron NOD (n NR) | ONS with saffron (3 × 500 mg pill/day) (n = 21) | ONS with crocin (2 × 15 mg caps/day) (n = 20) |
| Comparator | Placebo syrup (n = 26) | Placebo (n = 20) | Placebo (n NR) | Placebo (n = 22) | Placebo (n = 20) |
| Intervention duration | 4 weeks | 4 weeks | NR | 12 months | 4 weeks |
| Standard therapy | SSRIs were only reported; MS medications were NR | NR | NR | Vitamin D3, vitamin B1, Ca, tolterodine, gabapentin, citalopram, amantadine | NR |
| Treatment adherence | By periodic phone follow-ups | NR | NR | NR | NR |
| Ban of other antioxidants | Discontinuation at trial start (including herbal medicines) | NR | NR | NR | NR |
| Main hypothesis | Δ in fatigue and sleep disorders (depression was presented instead) | Δ in oxidative stress | Δ in cognition and functional ability | Δ in proxy markers of disease severity | Δ in inflammation and oxidative and DNA damage |
| Outcomes | BDI | TAC, CAT, TTG, LPO from saliva and urine samples | EDSS, BDI, MACFIMS (PASAT, BWMT, DKEFS-ST, CO-WAT, CVLT, NAART), 9HPT | Serum levels of MMP-9 and TIMP-1 (its inhibitor) | LPO, TAC, TTG, IL-17, TNF-α, DNA damage |
| Assays | N/A | Absorbance (CAT), FRAP assay (TAC) | N/A | ELISA | Absorbance (TTG), FRAP (TAC), SP, ELISA (IL-17, TNF-a, DNA damage) |
| Dietary assessment | NR | NR | NR | NR | NR |
| PE assessment | NR | NR | NR | NR | NR |
| AEs | None | NR | NR | NR | NR |
| Drop outs | Few relapsed (n = 2) or were dissatisfied (n = 4) (all on placebo) | NR | NR | NR | NR |
| n included in final analysis | n = 26 active arm n = 20 placebo | n = 20 active arm n = 20 placebo | NR | n = 21 active arm n = 22 placebo | n = 20 active arm n = 20 placebo |
| Analysis | PP | ITT | NR | ITT | ITT |
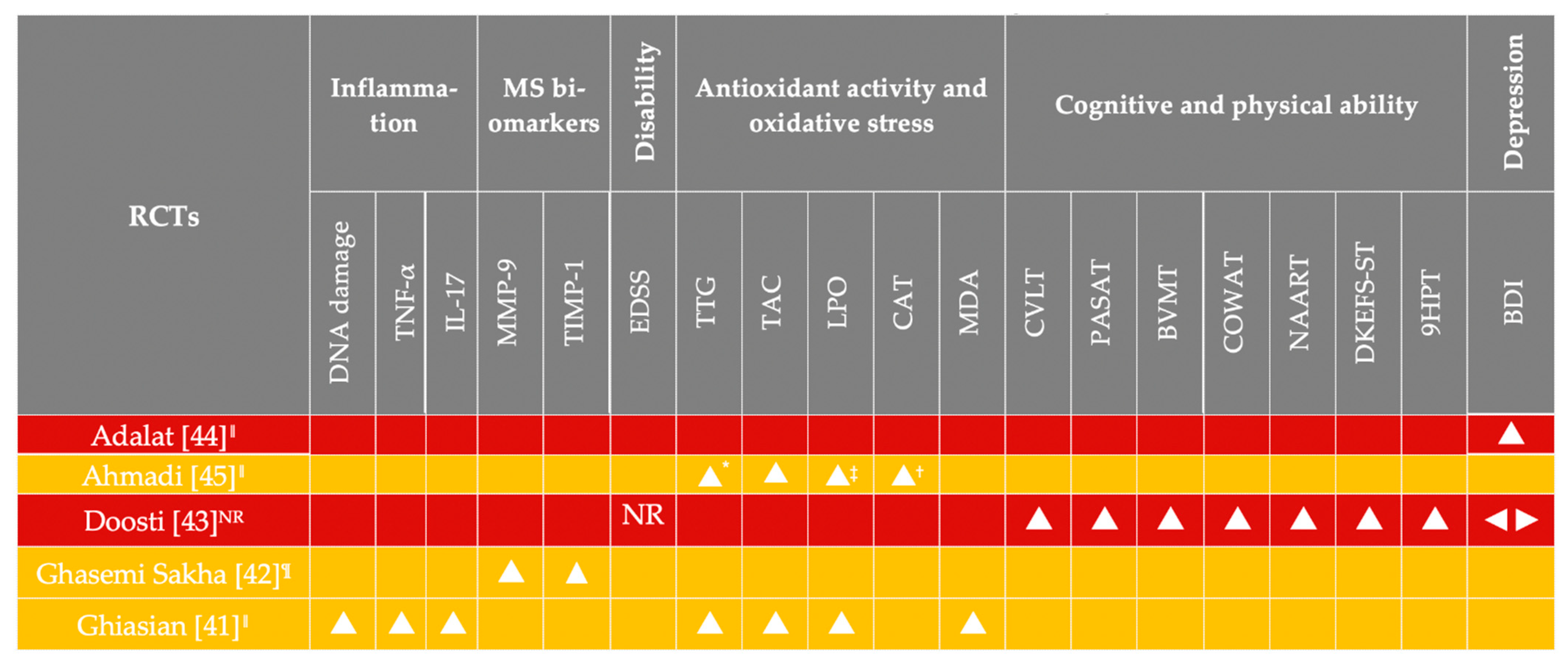
| Results | Those treated with the herbal extract demonstrated reduced BDI scores compared to participants in the placebo arm. | A difference in TTG, TAC, and LPO, except for CAT activity, was noted in the crocin arm. Crocin increased saliva TTG, TAC levels, and CAT, and lowered LPO. | Saffron improved MAC-FIMS subdomains (total learning-CVLT, PASAT, total and delay-BWMT, COWAT, DKEFS-ST, NAART). Dominant hand 9HPT differed between arms. | The level of MMP-9 was decreased, and that of TIMP-1 was increased in the saffron arm. | A decrease in the level of LPO, DNA damage, TNF-α, and IL-17, as well as an increase in the TAC of patients treated with crocin. |
3.3. Outcomes Assessed in the Included Interventions
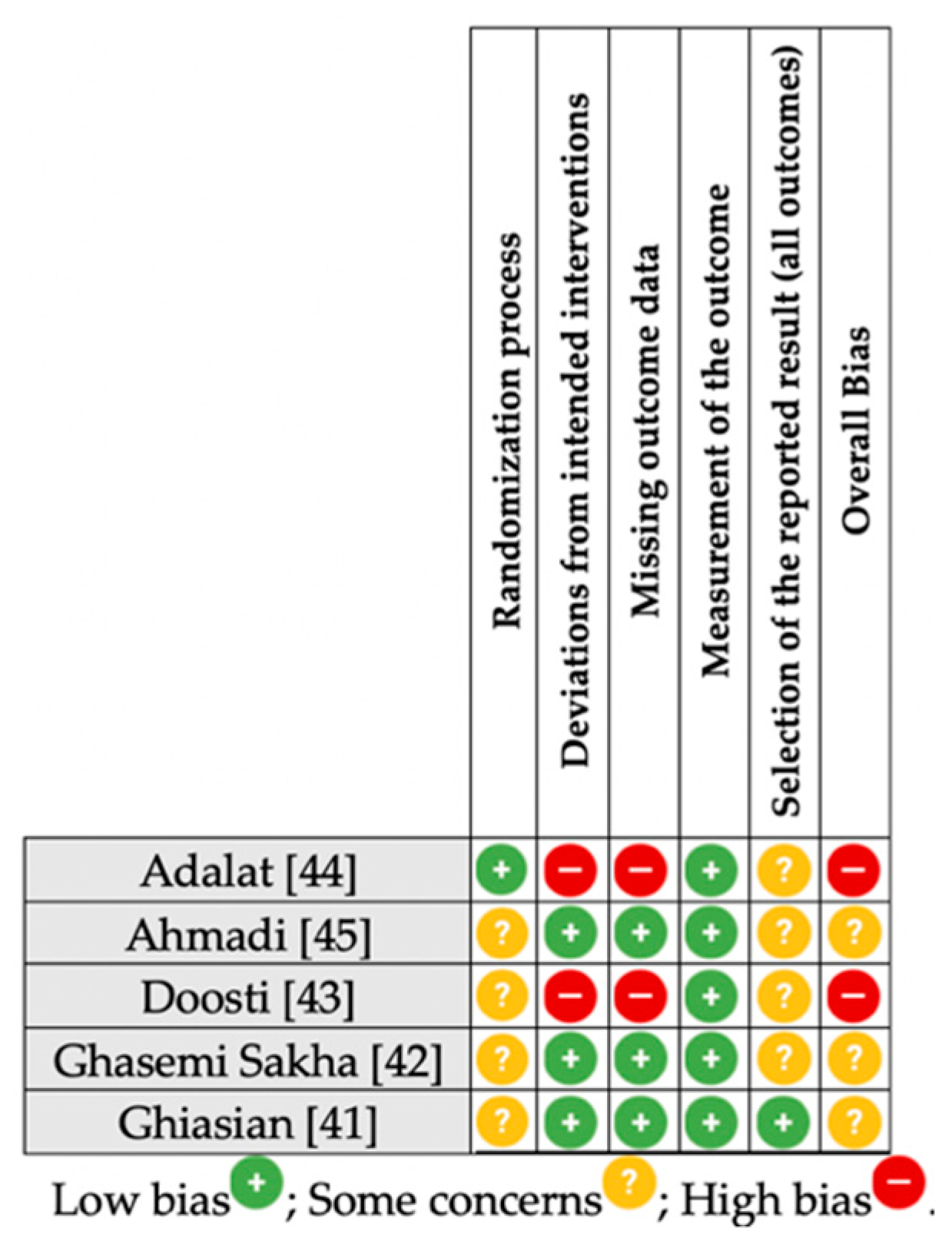
3.4. Risk of Bias Summary
3.5. AEs, Treament Adherence, and Other Biases
3.6. Synthesis without Meta-Analysis (SwiM)
4. Discussion
4.1. Heterogeneity in the Examined Outcome Measures
4.2. RCTs in the Pipeline
4.3. Limitations of the Present SWiM
4.4. Advice for Future Trials Administering Saffron in Patients with MS
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef]
- Koch-Henriksen, N.; Sørensen, P.S. The changing demographic pattern of multiple sclerosis epidemiology. Lancet. Neurol. 2010, 9, 520–532. [Google Scholar] [CrossRef]
- Zhang, S.Y.; Gui, L.N.; Liu, Y.Y.; Shi, S.; Cheng, Y. Oxidative Stress Marker Aberrations in Multiple Sclerosis: A Meta-Analysis Study. Front. Neurosci. 2020, 14, 823. [Google Scholar] [CrossRef]
- Gelfand, J.M. Multiple sclerosis: Diagnosis, differential diagnosis, and clinical presentation. Handb. Clin. Neurol. 2014, 122, 269–290. [Google Scholar] [CrossRef]
- Huang, W.J.; Chen, W.W.; Zhang, X. Multiple sclerosis: Pathology, diagnosis and treatments. Exp. Ther. Med. 2017, 13, 3163. [Google Scholar] [CrossRef]
- Aboud, T.; Schuster, N.M. Pain Management in Multiple Sclerosis: A Review of Available Treatment Options. Curr. Treat. Options Neurol. 2019, 21, 62. [Google Scholar] [CrossRef]
- Andravizou, A.; Dardiotis, E.; Artemiadis, A.; Sokratous, M.; Siokas, V.; Tsouris, Z.; Aloizou, A.-M.; Nikolaidis, I.; Bakirtzis, C.; Tsivgoulis, G.; et al. Brain atrophy in multiple sclerosis: Mechanisms, clinical relevance and treatment options. Autoimmun. Highlights 2019, 10, 7. [Google Scholar] [CrossRef]
- Chastain, E.M.L.; Miller, S.D. Molecular mimicry as an inducing trigger for CNS autoimmune demyelinating disease. Immunol. Rev. 2012, 245, 227–238. [Google Scholar] [CrossRef]
- Schreiner, T.G.; Genes, T.M. Obesity and Multiple Sclerosis—A Multifaceted Association. J. Clin. Med. 2021, 10, 2689. [Google Scholar] [CrossRef]
- Manouchehrinia, A.; Huang, J.; Hillert, J.; Alfredsson, L.; Olsson, T.; Kockum, I.; Constantinescu, C.S. Smoking Attributable Risk in Multiple Sclerosis. Front. Immunol. 2022, 13, 845. [Google Scholar] [CrossRef]
- Gombash, S.E.; Lee, P.W.; Sawdai, E.; Lovett-Racke, A.E. Vitamin D as a Risk Factor for Multiple Sclerosis: Immunoregulatory or Neuroprotective? Front. Neurol. 2022, 13, 796933. [Google Scholar] [CrossRef]
- Bjornevik, K.; Cortese, M.; Healy, B.C.; Kuhle, J.; Mina, M.J.; Leng, Y.; Elledge, S.J.; Niebuhr, D.W.; Scher, A.I.; Munger, K.L.; et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science 2022, 375, 296–301. [Google Scholar] [CrossRef]
- Zuliani, C.; Baroni, L. Antioxidants for the Prevention and Treatment of Multiple Sclerosis: An Overview. In Bioactive Nutraceuticals and Dietary Supplements in Neurological and Brain Disease: Prevention and Therapy; Watson, R.R., Preedy, V.R., Eds.; Academic Press: Cambridge, MA, USA, 2015; pp. 341–353. ISBN 9780124115293. [Google Scholar]
- Bast, A.; Haenen, G.R.M.M.; Doelman, C.J.A. Oxidants and antioxidants: State of the art. Am. J. Med. 1991, 91, S2. [Google Scholar] [CrossRef]
- Bongarzone, E.R.; Pasquini, J.M.; Soto, E.F. Oxidative damage to proteins and lipids of CNS myelin produced by in vitro generated reactive oxygen species. J. Neurosci. Res. 1995, 41, 213–221. [Google Scholar] [CrossRef]
- Armon-Omer, A.; Waldman, C.; Simaan, N.; Neuman, H.; Tamir, S.; Shahien, R. New Insights on the Nutrition Status and Antioxidant Capacity in Multiple Sclerosis Patients. Nutrients 2019, 11, 427. [Google Scholar] [CrossRef]
- Ohl, K.; Tenbrock, K.; Kipp, M. Oxidative stress in multiple sclerosis: Central and peripheral mode of action. Exp. Neurol. 2016, 277, 58–67. [Google Scholar] [CrossRef]
- Moravejolahkami, A.R.; Paknahad, Z.; Chitsaz, A.; Hojjati Kermani, M.A.; Borzoo-Isfahani, M. Potential of modified Mediterranean diet to improve quality of life and fatigue severity in multiple sclerosis patients: A single-center randomized controlled trial. Int. J. Food Prop. 2020, 23, 1993–2004. [Google Scholar] [CrossRef]
- Papandreou, P.; Gioxari, A.; Daskalou, E.; Vasilopoulou, A.; Skouroliakou, M. Personalized Nutritional Intervention to Improve Mediterranean Diet Adherence in Female Patients with Multiple Sclerosis: A Randomized Controlled Study. Dietetics 2022, 1, 25–38. [Google Scholar] [CrossRef]
- Katz Sand, I. The Role of Diet in Multiple Sclerosis: Mechanistic Connections and Current Evidence. Curr. Nutr. Rep. 2018, 7, 150. [Google Scholar] [CrossRef]
- Bagur, M.J.; Antonia Murcia, M.; Jiménez-Monreal, A.M.; Tur, J.A.; Mar Bibiloni, M.; Alonso, G.L.; Martínez-Tomé, M. Influence of Diet in Multiple Sclerosis: A Systematic Review. Adv. Nutr. 2017, 8, 463–472. [Google Scholar] [CrossRef]
- Aristotelous, P.; Stefanakis, M.; Pantzaris, M.; Pattichis, C.S.; Calder, P.C.; Patrikios, I.S.; Sakkas, G.K.; Giannaki, C.D. The Effects of Specific Omega-3 and Omega-6 Polyunsaturated Fatty Acids and Antioxidant Vitamins on Gait and Functional Capacity Parameters in Patients with Relapsing-Remitting Multiple Sclerosis. Nutrients 2021, 13, 3661. [Google Scholar] [CrossRef]
- Ferorelli, P.; Antonelli, F.; Shevchenko, A.; Mischiati, C.; Doepp, M.; Lenzi, S.; Borromeo, I.; Feriotto, G.; Beninati, S. Reduction in Fatigue Symptoms Following the Administration of Nutritional Supplements in Patients with Multiple Sclerosis. Med. Sci. 2021, 9, 52. [Google Scholar] [CrossRef]
- Holton, K.F.; Kirkland, A.E. Moving past antioxidant supplementation for the dietary treatment of multiple sclerosis. Mult. Scler. 2020, 26, 1012–1023. [Google Scholar] [CrossRef]
- Tsiogkas, S.G.; Grammatikopoulou, M.G.; Gkiouras, K.; Zafiriou, E.; Papadopoulos, I.; Liaskos, C.; Dardiotis, E.; Sakkas, L.I.; Bogdanos, D.P. Effect of Crocus sativus (Saffron) Intake on Top of Standard Treatment, on Disease Outcomes and Comorbidities in Patients with Rheumatic Diseases: Synthesis without Meta-Analysis (SWiM) and Level of Adherence to the CONSORT Statement for Randomized Controlled Trials Delivering Herbal Medicine Interventions. Nutrients 2021, 13, 4274. [Google Scholar] [CrossRef]
- Hosseini, A.; Razavi, B.M.; Hosseinzadeh, H. Pharmacokinetic Properties of Saffron and its Active Components. Eur. J. Drug Metab. Pharmacokinet. 2018, 43, 383–390. [Google Scholar] [CrossRef]
- Musazadeh, V.; Zarezadeh, M.; Faghfouri, A.H.; Keramati, M.; Ghoreishi, Z.; Farnam, A. Saffron, as an adjunct therapy, contributes to relieve depression symptoms: An umbrella meta-analysis. Pharmacol. Res. 2022, 175, 105963. [Google Scholar] [CrossRef]
- Setayesh, L.; Ashtary-Larky, D.; Clark, C.C.T.; Rezaei Kelishadi, M.; Khalili, P.; Bagheri, R.; Asbaghi, O.; Suzuki, K. The Effect of Saffron Supplementation on Blood Pressure in Adults: A Systematic Review and Dose-Response Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 2736. [Google Scholar] [CrossRef]
- Bian, Y.; Zhao, C.; Lee, S.M.Y. Neuroprotective Potency of Saffron Against Neuropsychiatric Diseases, Neurodegenerative Diseases, and Other Brain Disorders: From Bench to Bedside. Front. Pharmacol. 2020, 11, 579052. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Vrysis, C.; Chaitidis, N.; Kolotsiou, K.; Myserlis, P.G.; Kapogiannis, D. Effects of saffron (Crocus Sativus L.) on cognitive function. A systematic review of RCTs. Neurol. Sci. 2020, 41, 2747. [Google Scholar] [CrossRef]
- Jackson, P.A.; Forster, J.; Khan, J.; Pouchieu, C.; Dubreuil, S.; Gaudout, D.; Moras, B.; Pourtau, L.; Joffre, F.; Vaysse, C.; et al. Effects of Saffron Extract Supplementation on Mood, Well-Being, and Response to a Psychosocial Stressor in Healthy Adults: A Randomized, Double-Blind, Parallel Group, Clinical Trial. Front. Nutr. 2021, 7, 365. [Google Scholar] [CrossRef]
- Bagur, M.J.; Alonso Salinas, G.L.; Jiménez-Monreal, A.M.; Serrano-Heras, G.; Martínez-Tome., M.; Alonso, G.L. Effect of Daily Intake of a Saffron Infusion on Blood Cholesterol Levels. Appl. Sci. 2020, 10, 4763. [Google Scholar] [CrossRef]
- Ashtiani, A.R.; Seied Amirhossein, L.; Jadidi, A.; Ghasami, K.; Khanmohamadi Hezave, A.; Aghae Pour, S.M.; Malekhosseni, S.; Kamalinejad, M.; Alimoradian, A.; Salehi, M. The effect of novel simple saffron syrup on fatigue reduction in patients with multiple sclerosis. J. Basic Clin. Physiol. Pharmacol. 2020, 31. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, I6890. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Goel, A.; Aggarwal, B.B. Curcumin, the golden spice from Indian saffron, is a chemosensitizer and radiosensitizer for tumors and chemoprotector and radioprotector for normal organs. Nutr. Cancer 2010, 62, 919–930. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.; Elbers, R.; Blencowe, N.; Boutron, I.; Cates, C.; Cheng, H.-Y.; Corbett, M.; Eldridge, S.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. Br. Med. J. 2019, 366, l4898. [Google Scholar] [CrossRef]
- Thomson, H.J.; Thomas, S. The effect direction plot: Visual display of non-standardised effects across multiple outcome domains. Res. Synth. Methods 2013, 4, 95. [Google Scholar] [CrossRef]
- McKenzie, J.E.; Brennan, S.E. Synthesizing and presenting findings using other methods. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2019; pp. 321–347. [Google Scholar]
- Ghiasian, M.; Khamisabadi, F.; Kheiripour, N.; Karami, M.; Haddadi, R.; Ghaleiha, A.; Taghvaei, B.; Oliaie, S.S.; Salehi, M.; Samadi, P.; et al. Effects of crocin in reducing DNA damage, inflammation, and oxidative stress in multiple sclerosis patients: A double-blind, randomized, and placebo-controlled trial. J. Biochem. Mol. Toxicol. 2019, 33, e22410. [Google Scholar] [CrossRef]
- Ghasemi Sakha, F.; Azimi Saeen, A.; Moazzeni, S.M.; Etesam, F.; Vaezi, A. Randomized, Triple-blind Placebo-controlled Trial to Determine the Effect of Saffron on the Serum Levels of MMP-9 and TIMP-1 in Patients with Multiple Sclerosis. Iran. J. Allergy. Asthma. Immunol. 2020, 19, 297–304. [Google Scholar] [CrossRef]
- Doosti, R.; Ghasemi-Sakha, F.; Saeedi, R.; Almasi-Hashiani, A.; Naser Moghadasi, A.; Sahraian, M.A.; Madah Movahedi, M.; Toliyat, T.; Azimi, A.R. EP1592. A triple-blind, randomized controlled trial of Saffron in cognitive function of multiple sclerosis patients. Mult. Scler. J. 2019, 25, 884. [Google Scholar]
- Adalat, M.; Khalili, M.; Ayromlou, H.; Haririan, S.; Fazljou, S.M.B.; Rezaeizadeh, H.; Safari, A.A.; Zargaran, A. Antidepressant Effects of a Persian Medicine Remedy on Multiple Sclerosis Patients: A Double-Blinded Randomized Clinical Trial. Galen Med. J. 2019, 8, e1212. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, S.A.; Kazemi, A.; Sabahi, M.; Razipour, S.; Salehipour, A.; Ghiasian, M.; Ghasemi, H.; Ranjbar, A. Probable antioxidant therapy of Saffron Crocin in patients with multiple sclerosis: A randomized controlled trial. Biomedicine 2020, 40, 516–521. [Google Scholar] [CrossRef]
- McDonald, W.I.; Compston, A.; Edan, G.; Goodkin, D.; Hartung, H.-P.; Lublin, F.D.; McFarland, H.F.; Paty, D.W.; Polman, C.H.; Reingold, S.C.; et al. Recommended diagnostic criteria for multiple sclerosis: Guidelines from the international panel on the diagnosis of multiple sclerosis. Ann. Neurol. 2001, 50, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.; Steer, R.; Brown, G. Beck Depression Inventory, 2nd ed.; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Benedict, R.H.B.; Cookfair, D.; Gavett, R.; Gunther, M.; Munschauer, F.; Garg, N.; Weinstock-Guttman, B. Validity of the minimal assessment of cognitive function in multiple sclerosis (MACFIMS). J. Int. Neuropsychol. Soc. 2006, 12, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Uttl, B. North American Adult Reading Test: Age norms, reliability, and validity. J. Clin. Exp. Neuropsychol. 2002, 24, 1123–1137. [Google Scholar] [CrossRef]
- Trojano, M.; Avolio, C.; Liuzzi, G.M.; Ruggieri, M.; Defazio, G.; Liguori, M.; Santacroce, M.P.; Paolicelli, D.; Giuliani, F.; Riccio, P.; et al. Changes of serum sICAM-1 and MMP-9 induced by rIFNβ-1b treatment in relapsing-remitting MS. Neurology 1999, 53, 1402. [Google Scholar] [CrossRef]
- Rahaiee, S.; Moini, S.; Hashemi, M.; Shojaosadati, S.A. Evaluation of antioxidant activities of bioactive compounds and various extracts obtained from saffron (Crocus sativus L.): A review. J. Food Sci. Technol. 2015, 52, 1881. [Google Scholar] [CrossRef]
- Asbaghi, O.; Sadeghian, M.; Sadeghi, O.; Rigi, S.; Tan, S.C.; Shokri, A.; Mousavi, S.M. Effects of saffron (Crocus sativus L.) supplementation on inflammatory biomarkers: A systematic review and meta-analysis. Phyther. Res. 2021, 35, 20–32. [Google Scholar] [CrossRef]
- Thushara, R.M.; Hemshekhar, M.; Paul, M.; Shanmuga Sundaram, M.; Shankar, R.L.; Kemparaju, K.; Girish, K.S. Crocin prevents sesamol-induced oxidative stress and apoptosis in human platelets. J. Thromb. Thrombolysis 2014, 38, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Morvaridzadeh, M.; Agah, S.; Estêvão, M.D.; Hosseini, A.S.; Heydari, H.; Toupchian, O.; Abdollahi, S.; Persad, E.; Abu-Zaid, A.; Rezamand, G.; et al. Effect of saffron supplementation on oxidative stress parameters: A systematic review and meta-analysis of randomized placebo-controlled trials. Food Sci. Nutr. 2021, 9, 5819. [Google Scholar] [CrossRef] [PubMed]
- Gilgun-Sherki, Y.; Melamed, E.; Offen, D. The role of oxidative stress in the pathogenesis of multiple sclerosis: The need for effective antioxidant therapy. J. Neurol. 2004, 251, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, G.G.; Pacheco-Moisés, F.P.; Bitzer-Quintero, O.K.; Ramírez-Anguiano, A.C.; Flores-Alvarado, L.J.; Ramírez-Ramírez, V.; Macias-Islas, M.A.; Torres-Sánchez, E.D. Immunology and Oxidative Stress in Multiple Sclerosis: Clinical and Basic Approach. Clin. Dev. Immunol. 2013, 2013, 14. [Google Scholar] [CrossRef] [PubMed]
- Boeschoten, R.E.; Braamse, A.M.J.; Beekman, A.T.F.; Cuijpers, P.; van Oppen, P.; Dekker, J.; Uitdehaag, B.M.J. Prevalence of depression and anxiety in Multiple Sclerosis: A systematic review and meta-analysis. J. Neurol. Sci. 2017, 372, 331–341. [Google Scholar] [CrossRef]
- Fahy, A.; Maguire, R. Potentially modifiable associates of anxiety in people with multiple sclerosis: A systematic review. Disabil. Rehabil. 2021, 31. [Google Scholar] [CrossRef]
- Morrow, S.A. Anxiety is more important than depression in MS—Yes. Mult. Scler. J. 2018, 24, 440–441. [Google Scholar] [CrossRef]
- Marx, W.; Lane, M.; Rocks, T.; Ruusunen, A.; Loughman, A.; Lopresti, A.; Marshall, S.; Berk, M.; Jacka, F.; Dean, O.M. Effect of saffron supplementation on symptoms of depression and anxiety: A systematic review and meta-analysis. Nutr. Rev. 2019, 77, 557–571. [Google Scholar] [CrossRef]
- Lu, C.; Ke, L.; Li, J.; Zhao, H.; Lu, T.; Mentis, A.F.A.; Wang, Y.; Wang, Z.; Polissiou, M.G.; Tang, L.; et al. Saffron (Crocus sativus L.) and health outcomes: A meta-research review of meta-analyses and an evidence mapping study. Phytomedicine 2021, 91, 153699. [Google Scholar] [CrossRef]
- Dai, L.; Chen, L.; Wang, W. Safety and Efficacy of Saffron (Crocus sativus L.) for Treating Mild to Moderate Depression: A Systematic Review and Meta-analysis. J. Nerv. Ment. Dis. 2020, 208, 269–276. [Google Scholar] [CrossRef]
- Khaksarian, M.; Behzadifar, M.; Behzadifar, M.; Alipour, M.; Jahanpanah, F.; Re, T.S.; Firenzuoli, F.; Zerbetto, R.; Bragazzi, N.L. The efficacy of Crocus sativus (Saffron) versus placebo and Fluoxetine in treating depression: A systematic review and meta-analysis. Psychol. Res. Behav. Manag. 2019, 12, 305. [Google Scholar] [CrossRef]
- Fanara, S.; Aprile, M.; Iacono, S.; Schirò, G.; Bianchi, A.; Brighina, F.; Dominguez, L.J.; Ragonese, P.; Salemi, G. The Role of Nutritional Lifestyle and Physical Activity in Multiple Sclerosis Pathogenesis and Management: A Narrative Review. Nutrients 2021, 13, 3774. [Google Scholar] [CrossRef]
- Guo, R.; Canter, P.H.; Ernst, E. A systematic review of randomised clinical trials of individualised herbal medicine in any indication. Postgrad. Med. J. 2007, 83, 637. [Google Scholar] [CrossRef]
- Singletary, K. Saffron: Potential Health Benefits. Nutr. Today 2020, 55, 294–303. [Google Scholar] [CrossRef]
- Inojosa, H.; Schriefer, D.; Ziemssen, T. Clinical outcome measures in multiple sclerosis: A review. Autoimmun. Rev. 2020, 19, 102512. [Google Scholar] [CrossRef]
- Dwan, K.; Altman, D.G.; Arnaiz, J.A.; Bloom, J.; Chan, A.W.; Cronin, E.; Decullier, E.; Easterbrook, P.J.; Von Elm, E.; Gamble, C.; et al. Systematic review of the empirical evidence of study publication bias and outcome reporting bias. PLoS ONE 2008, 3, e3081. [Google Scholar] [CrossRef]
- Williamson, P.R.; Altman, D.G.; Bagley, H.; Barnes, K.L.; Blazeby, J.M.; Brookes, S.T.; Clarke, M.; Gargon, E.; Gorst, S.; Harman, N.; et al. The COMET Handbook: Version 1.0. Trials 2017, 18, 280. [Google Scholar] [CrossRef]
- Clarke, M.; Williamson, P.R. Core outcome sets and systematic reviews. Syst. Rev. 2016, 5, 11. [Google Scholar] [CrossRef]
- Gargon, E.; Gurung, B.; Medley, N.; Altman, D.G.; Blazeby, J.M.; Clarke, M.; Williamson, P.R. Choosing important health outcomes for comparative effectiveness research: A systematic review. PLoS ONE 2014, 9, e99111. [Google Scholar] [CrossRef]
- Prinsen, C.A.C.; Vohra, S.; Rose, M.R.; King-Jones, S.; Ishaque, S.; Bhaloo, Z.; Adams, D.; Terwee, C.B. Core Outcome Measures in Effectiveness Trials (COMET) initiative: Protocol for an international Delphi study to achieve consensus on how to select outcome measurement instruments for outcomes included in a “core outcome set. ” Trials 2014, 15, 247. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Evans, S.J.W.; Gøtzsche, P.C.; O’Neill, R.T.; Altman, D.G.; Schulz, K.; Moher, D. Better reporting of harms in randomized trials: An extension of the CONSORT statement. Ann. Intern. Med. 2004, 141, 781–788. [Google Scholar] [CrossRef]
- Riccio, P.; Rossano, R. Nutrition Facts in Multiple Sclerosis. ASN Neuro 2015, 7, 1–20. [Google Scholar] [CrossRef]
- Stoiloudis, P.; Kesidou, E.; Bakirtzis, C.; Sintila, S.A.; Konstantinidou, N.; Boziki, M.; Grigoriadis, N. The Role of Diet and Interventions on Multiple Sclerosis: A Review. Nutrients 2022, 14, 1150. [Google Scholar] [CrossRef]




| Population | Patients with an MS diagnosis |
| Intervention | Saffron (tabs, sachets, pills, tea, etc.) |
| Comparison | Placebo, or any other intervention |
| Outcomes | Any disease-specific (immediate/intermediate) or comorbidity-related outcome |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| (1) Having an RCT design, parallel, or cross-over | (1) All other study designs, including those lacking a comparator arm |
| (2) In a sample of patients with MS | |
| (3) Of any age group | (2) Not including patients with MS |
| (4) Using an active per os intervention with saffron in any form (tablets, capsules, powder, syrup, tea) | (3) Using interventions lacking saffron |
| (4) Using interventions with curcumin | |
| (5) Compared against placebo or any other intervention (comparative effectiveness studies) | (5) Published protocols without results |
| (6) Animal or preclinical studies |
| CTI | Sample | Affiliation | Intervention Duration | Arms | Outcomes | ||
|---|---|---|---|---|---|---|---|
| Intervention (s) | Comparator (s) | Primary | Secondary | ||||
| IRCT201202 27009157N7DB | Patients with MS | Tehran University of Medical Sciences | 12 weeks | ONS with nanocrocin caps (2 × 0.27 mg of nanocrocin/day) | 2 × placebo caps with the same smell and taste as nanocrocin | MACFIMS total score | BDI |
| IRCT201705 14033961N4OL | Women with MS (N = 100) | Khoram-Abad University of Medical Sciences | 12 weeks | (1) Performing corrective movements thrice/week and ONS with saffron (15 mg) caps twice/day (2) Performing corrective movements thrice/week (3) ONS with saffron caps (15 mg) twice/day | Not receiving any intervention | Depression (BDI) QoL (SF-36) | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grammatikopoulou, M.G.; Tsiogkas, S.G.; Gkiouras, K.; Gioxari, A.; Daskalou, E.; Maraki, M.I.; Dardiotis, E.; Bogdanos, D.P. Supplementation with Crocus sativus L. (Saffron) against Placebo in Multiple Sclerosis: A Systematic Review and Synthesis without Meta-Analysis of Randomized Controlled Trials. Dietetics 2022, 1, 227-241. https://doi.org/10.3390/dietetics1030020
Grammatikopoulou MG, Tsiogkas SG, Gkiouras K, Gioxari A, Daskalou E, Maraki MI, Dardiotis E, Bogdanos DP. Supplementation with Crocus sativus L. (Saffron) against Placebo in Multiple Sclerosis: A Systematic Review and Synthesis without Meta-Analysis of Randomized Controlled Trials. Dietetics. 2022; 1(3):227-241. https://doi.org/10.3390/dietetics1030020
Chicago/Turabian StyleGrammatikopoulou, Maria G., Sotirios G. Tsiogkas, Konstantinos Gkiouras, Aristea Gioxari, Efstratia Daskalou, Maria I. Maraki, Efthimios Dardiotis, and Dimitrios P. Bogdanos. 2022. "Supplementation with Crocus sativus L. (Saffron) against Placebo in Multiple Sclerosis: A Systematic Review and Synthesis without Meta-Analysis of Randomized Controlled Trials" Dietetics 1, no. 3: 227-241. https://doi.org/10.3390/dietetics1030020
APA StyleGrammatikopoulou, M. G., Tsiogkas, S. G., Gkiouras, K., Gioxari, A., Daskalou, E., Maraki, M. I., Dardiotis, E., & Bogdanos, D. P. (2022). Supplementation with Crocus sativus L. (Saffron) against Placebo in Multiple Sclerosis: A Systematic Review and Synthesis without Meta-Analysis of Randomized Controlled Trials. Dietetics, 1(3), 227-241. https://doi.org/10.3390/dietetics1030020