Abstract
The COVID-19 pandemic has claimed numerous lives worldwide. Malaysia documented about 118 mortalities during the second wave of the outbreak. This study aims to assess associated risk factors of the COVID-19 mortalities from 18 March until 22 May 2020. The majority of patients were above 60 years old (69.0%), male (78.0%), and Malaysian citizens (98.0%). The mean age of the mortalities was 64.01 years old (±SD 14.91 years). The major risk factors consist of hypertension (52.0%), diabetes mellitus (43.0%), cardiovascular diseases (21.0%), extra-pulmonary solid malignancies (5.0%), cerebrovascular diseases (3.0%), pulmonary diseases (1.0%) and pulmonary malignancies (1.0%). About 23.0% of mortalities were related to established clusters while 5.0% had a history of travelling overseas. The mean survival time was 11.87 days (±SD 9.32 days). Approximately 50.0% of the patients survived until day 10 post-admission. The probability of the patients surviving beyond 30 days post-admission was less than 10.0%. There is a significant difference between groups for having a shorter duration to death for risk factors including age group, history of travelling overseas, attending mass gatherings, and having pulmonary malignancies. The hazard ratio (HR) for pulmonary malignancy is 5.512 (95% CI 0.662, 45.899), mass gathering; 3.434 (95% CI 1.375, 8.579), pulmonary disease is 2.442 (95% CI 0.314, 18.983), travelling overseas; 2.251 (95% CI 0.657, 7.711), extra-pulmonary solid malignancy; 2.165 (95% CI 0.767, 6.112), and despite the significant result only applied for mass gathering (p-value = 0.008). COVID-19 screening should be mandatory for those who attend mass gatherings as they are the main source of COVID-19 spread in the community during the second wave outbreak in Malaysia.
1. Introduction
COVID-19, a novel emerging infectious disease, was first identified in Wuhan City, Hubei Province, China in December 2019, following the diagnosis of a cluster of patients with pneumonia of unknown etiology [1]. It is caused by a newly discovered strain of coronavirus known to cause lower respiratory tract infections in humans, resulting in acute pulmonary complication, septic shock, multi-organ failure [2]. Fever, cough, dyspnea, myalgia, headache, diarrhoea, rhinorrhoea, and pharyngalgia are among the most typical clinical manifestation among COVID-19 patients [3,4]. The new official name of this disease, coronavirus disease (COVID-19) was announced by the World Health Organization (WHO) on 11 February 2020, to replace the previous name; “2019-nCov” [1]. COVID-19 is a major worldwide health concern that has spread rampantly, which cause the WHO to declare the coronavirus outbreak as a Public Health Emergency of International Concern (PHEIC) in March 2020. In April 2020, COVID-19 had spread internationally, affecting 210 countries, and infecting 1,948,617 patients [5]. Severe acute respiratory syndrome coronavirus (SARS-COV), Middle East respiratory syndrome coronavirus (MERS-COV), and COVID-19 are known to be highly pathogenic. They are proven to be lethal human coronaviruses which spread within two decades because of their dreadful impacts on humans. Fortunately, the documented case–fatality rate of COVID-19 is 4.4% which is lower than the other pandemics such as SARS-COV (9.4%) and the MERS-COV (34.3%) [2].
Despite having a lower case–fatality rate compared to the pandemics caused by other coronaviruses (SARS-COV and MERS-COV), COVID-19 has claimed more than one million lives globally since the first death reported in December 2019 until October 2020 [6]. At this moment, the large number of mortalities due to COVID-19 is observed predominantly in developed countries in North America, with 312,761 deaths, and Europe with 225,396 deaths [6]. Malaysia, an upper-middle-income country, was also not spared from having severe COVID-19 cases that ended in mortality and morbidity. In Malaysia, the overall number of deaths due to COVID-19 reported up until 5 October 2020, was 141, with a mortality rate of 1.1%, which was below the global mortality rate of 1.8% [6,7].
The first COVID-19 case in Malaysia was notified on 24 January 2020, which involved a 40-year-old tourist, who came on a group tour, from Wuhan, China who visited Johor, Malaysia [8]. Since then, the number of COVID-19 cases surged to 22 on 15 February 2020, and remained a plateau for almost two weeks afterward [9]. These 22 positive cases were declared by the Ministry of Health (MOH) Malaysia as the first wave of COVID-19 outbreak, with no mortality reported before the implementation of the Movement Control Order (MCO) on 18 March 2020 [10]. A sudden rise in new cases was related to the massive religious gathering organized from 27 February 2020 until 3 March 2020 in Sri Petaling, Malaysia, which later formed the second wave of the COVID-19 outbreak [10]. During this second wave outbreak, a vast number of mortality cases due to COVID-19 were reported [9]. During the first week of April, the COVID-19 case–mortality rate for Malaysia was documented at 1.6%, which was 3.8% lower compared to the global case–mortality rate of 6.3% [5,11].
Overall, common major risk factors of COVID-19 mortality cases identified among various studies are male gender, older age, smoking patient, and the comorbidities such as diabetes mellitus, hypertension, cardiovascular diseases, cerebrovascular diseases, and respiratory diseases [12,13,14,15]. Movement of people and mass gathering was closely related to the occurrence of COVID-19 cases [9,16,17]. It was observed that patients with malignancies had a higher COVID-19 mortality rate than the patient without malignancies [18,19,20]. Despite having a large volume of mortalities during the second wave of the COVID-19 outbreak, epidemiological and major risk factors of COVID-19 mortality cases are not well explored in Malaysia. Therefore, the primary aim of this study is to identify epidemiological and major risk factors of COVID-19 mortality cases during the second wave of the outbreak in Malaysia.
2. Methodology
Malaysia is a Southeast Asian nation that is also a member of the Western Pacific region. It consists of Peninsular Malaysia and the eastern islands of Borneo (4.2105° N, 101.9758° E). Malaysia has a total land area that covers up to 330,525 km2 and consists of 14 states; Perlis, Kedah, Penang, Perak, Selangor, Negeri Sembilan, Malacca, Johor, Pahang, Terengganu, Kelantan, Sabah, Sarawak, and three federal territories; Kuala Lumpur, Putrajaya, and Labuan. Malaysia has several neighboring countries; Singapore, Thailand, Brunei, and the Indonesian portion of the island of Borneo (Kalimantan), with established cross-border entry. Malaysia has a population density of 32.7 million (29.6 million Malaysian citizens and 3.1 million non-citizens) documented in the first quarter of 2020 who are prone to exposure to the COVID-19 pandemic [21]. Each state has a designated government hospital for COVID-19 treatment, gazette by the MOH Malaysia (during the pandemic period) to cater to the patients who are diagnosed with COVID-19 and the persons under investigation (PUI). Sungai Buloh General Hospital (HSB) was appointed as the first designated government hospital for COVID-19 treatment in Malaysia. To date, there are 34 allocated government hospitals and two non-government hospitals for COVID-19 treatment in Malaysia [22]. Public health action and management are fully organized at various levels; Crisis Preparedness and Response Centre (CPRC) MOH Malaysia at the national level, CPRC State Health Department (including federal territories) at the state level, and District Health Office at the district level. Until now, there are 17 state health departments and 167 district health offices in Malaysia working together to manage the outbreak [23].
This is a retrospective cohort study of adult inpatients (more than 18 years old) from all selected government and non-government hospitals for COVID-19 treatment in Malaysia. As shown in Figure 1, all adult patients (n = 118) who were diagnosed with COVID-19 according to Malaysia COVID-19 Guidelines 2020 [22], and passed away between 18 March 2020 and 22 May 2020 were identified. Among them, 18 patients were excluded due to the unavailability of information about the date of admission to the hospital (n = 16) and the patient who was diagnosed with COVID-19 during the post-mortem (n = 2) since the risk factors and status of underlying disease were unknown. For the management of COVID-19 patients, all positive cases in Malaysia were required to be admitted to the designated hospital for treatment and isolation. They will then be discharged after 72 h have passed since the recovery of symptoms (defined as resolution of fever without antipyretics and improvement in respiratory symptoms), and at least one sample of the naso-oropharyngeal swab is negative [22]. A COVID-19 mortality case is reported when the death was confirmed to be related to COVID-19.
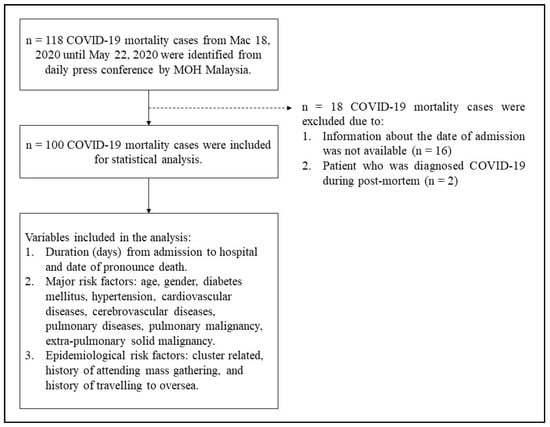
Figure 1.
Process flow of data collection and analysis involving 100 COVID-19 mortality cases in Malaysia.
The data regarding mortality cases were obtained from the daily official press conference statements organized by MOH Malaysia. The information about COVID-19 cases released during the press conference includes the sum of new cases, the final figure of cumulative cases, the number of the cases who recovered, and the number of mortality cases (if any). The official press statements including figures and tables were available for public reference on the MOH Malaysia official website; “From the Desk of the Director-General of Health Malaysia” [24]. Major risk factors were obtained from the COVID-19 updates; (1) age, (2) gender, (3) diabetes mellitus, (4) hypertension, (5) cardiovascular diseases, (6) cerebrovascular diseases, (7) pulmonary diseases, (8) pulmonary malignancy, (9) extra-pulmonary solid malignancy. Epidemiological risk factors were also included for data analysis; (1) cluster related, (2) mass gathering related, and (3) travelling oversea related.
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) version 22.0 for Windows (SPSS, Inc., Chicago, IL, USA). Detailed statistical analyses were presented in the form of text, tables, and figures. The descriptive statistics were in counts and percentages for categorical variables and mean ± standard deviation (SD) for continuous variables (age) since the data was normally distributed. Survival analysis was used to analyze the duration of time until the event that we are interested in occurs. The aims of the survival analysis were: (1) to estimate the probability of surviving to a certain time, (2) to compare the survival in the different patient groups, and (3) to determine the risk factors that affect the event. The definition of the event in the survival analysis is death due to COVID-19, while survival time is defined as the duration of time (days) from the date of admission to the hospital until the date of pronouncing dead due to COVID-19. There was no censored data since all patients reach the endpoint within the period of study and there was no loss to follow-up. The survival analysis tests used in this study were Kaplan–Meier Analysis, log rank Test, and Cox regression analysis.
Kaplan–Meier analysis is the univariate version of survival analysis and was used to analyze the survival-time data, in other words, to estimate the survival curve (S(t)). Using this technique, the mean and median survival time can be determined. Kaplan–Meier can be used to compare two groups on their survival times. The log-rank test was used in certain circumstances (equal weight to death throughout survival times) and aim to determine the equality of the survival distribution between the two groups. Cox regression analysis was used to identify the association between hazard function, survival time density distribution, and survival time. It is a specific analysis used if there are time-related covariates such as age, gender, underlying comorbidity, etc. The hazard ratio (HR) along with the 95% CI was also reported. The interpretation for HR is similar to the odds ratio. A value of one means there are no differences between the two groups in having a shorter time to death. HR > 1 means that the group of interest compared to the reference group likely has a shorter time to the event. HR < 1 means that the group of interest less likely to have a shorter time to death. A p-value of less than 0.05 was regarded as statistically significant in this study.
3. Results
Figure 2 shows the daily trend of COVID-19 new and mortality cases reported in Malaysia during the study period. It was observed that the mortality trend (Figure 2a) mirrors the cumulative trend of new COVID-19 cases (Figure 2b) throughout the second wave of infection. The mortality cases showed an increasing trend until 20 March 2020 and peaked on 29 March 2020, which was the highest number of mortality cases reported in Malaysia (n = 8). The mortality cases were found to be declining in the trend until the end of the MCO and maintained their lowest number (n = 1) since the beginning of the Conditional Movement Control Order (CMCO) until the end of the study period. Figure 3a shows the distribution of the survival times (duration from admission to hospital until the date of pronounced dead) with the mean survival times of 11.87 days ± SD 9.32 days. The minimum survival time was one day. The maximum survival time was 52 days, indicating that the patient will not be able to survive more than 52 days since the first day of admission to the hospital. Eight patients had a survival time of 11 days. Figure 3b shows the survival plots for non-censored scenario since all patients have achieved the event (death) at the end of the study. About 50.0% of the patients survived until day 10 of admission to the hospital. The probability of the patient surviving beyond 30 days after admission to the hospital was very minimal (less than 10.0%).
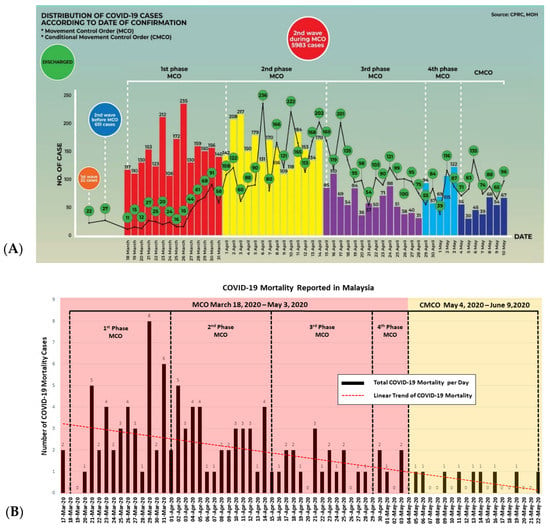
Figure 2.
The trend of COVID-19 mortality cases (A) (Source: CPRC, MOH Malaysia) as compared to the total number of COVID-19 cases (B) in Malaysia. MCO, Movement Control Order; CMCO, Conditional Movement Control Order.
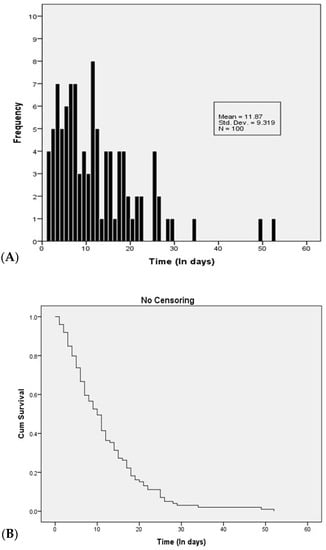
Figure 3.
(A) The distribution of the survival time among COVID-19 patients in Malaysia (from the date of admission to the hospital until the date of death). (B) Survival plots for COVID-19 among COVID-19 patients in Malaysia without censoring (n = 100).
A total of 100 COVID-19 patients were included in the study (Table 1). The majority of the patients were above 60 years old (69.0%), male (78.0%), and Malaysian citizens (98.0%). The mean age of the patients was 64.01 years old ± SD 14.91 years old. More than a quarter of total mortality cases were reported from Kuala Lumpur (27.0%), followed by Johor (17.0%), Sarawak (14.0%), Selangor (9.0%), and Negeri Sembilan (8.0%). As for major risk factors, about 43.0% had diabetes mellitus, 52.0% had hypertension, 21.0% had cardiovascular diseases, 3.0% had cerebrovascular diseases, 1.0% had pulmonary diseases, 1.0% had pulmonary malignancy, 5.0% had extra-pulmonary solid malignancy. About 23.0% of total patients were related to the established cluster in Malaysia, namely the Seri Petaling Tabligh cluster, Bali Cluster, Muar General Hospital Cluster, Sarawak Church Cluster, and Italy’s PUI Cluster. About 15.0% of total patients had a history of attending mass gatherings specifically to Sri Petaling tabligh gathering. About 5.0% of total patients had a history of travelling to Turkey, Saudi Arabia, India, Vietnam, and Indonesia.

Table 1.
Characteristics of the patients (n = 100).
Table 2 shows the mean and median survival times for two groups of each risk factor with the log-rank test result. It was observed that the group who had risk factors had a shorter time to death compared to the group who did not have the risk factors; pulmonary malignancy (mean survival time difference = 8.96 days, p-value = 0.037), mass gathering related (mean survival time difference = 4.94 days, p-value = 0.009) history of travelling overseas (mean survival time difference = 7.68 days, p-value = 0.007), except for age (mean survival time difference = 4.54 days, p-value = 0.007). The regression model in Table 3 shows a trend of risk for certain risk factors for COVID-19 mortality despite insignificant statistical results. The HR for pulmonary disease 2.442 (95% CI: 0.314, 18.983), pulmonary malignancy 5.512 (95% CI: 0.662, 45.899), extra-pulmonary solid malignancy 2.165 (95% CI: 0.767, 6.112), mass gathering related 3.434 (95% CI: 1.375, 8.579), and travelling overseas related 2.251 (95% CI: 0.657, 7.711) were more than one, indicating that the group of those who had pulmonary diseases, pulmonary malignancy, extra-pulmonary solid malignancy, mass gathering related, or history of travelling overseas were likely to have shorter time death due to COVID-19, despite the fact that the significant result was only applied for gathering-related cases (p-value = 0.008).
Table 2.
Kaplan–Meier analysis: Comparing Survival Between Two Groups (n = 100).
Table 3.
Estimates of Variables in Cox Regression (n = 100).
4. Discussion
Malaysia was recognized by WHO as one of the countries that are effectively fighting the pandemic through excellent public health intervention and good collaboration with both other government and non-government respective agencies. The mortality rate for COVID-19 in Malaysia was maintained between 1.4% and 1.7% during the second wave of the COVID-19 outbreak, better than the United Kingdom (mortality rate 7.2% to 15.4%), United States (mortality rate 2.2% to 5.9%) and the world (mortality rate 4.9% to 7.2%) [25]. Malaysia’s approach of isolating positive COVID-19-infected patients, regardless of the level of severity, even though they are asymptomatic or show mild symptoms, may have contributed to the low mortality rate and a high number of recovered cases. This approach is different from many other leading countries. The lower COVID-19 mortality rate in Malaysia indicates the excellent quality of public health action, good medical treatment, effective health enforcement, and public empowerment. Malaysia has taken immediate action in February 2020 and drastically upgraded health facilities and diagnostics capacity during this peak of COVID-19 including an 86.0% increment in diagnostics laboratory capacity, 89.0% increment in critical care bed capacity, and a 49.0% increase in the number of available ventilators [26]. However, Malaysia experienced challenges related to COVID-19 outbreak management during the early phase of the second wave of the COVID-19 outbreak from mid-March 2020 until mid-April 2020 due to a rapid increase in daily COVID-19 new cases (Figure 2a) and mortality cases (Figure 2b). As of 31 March 2020, 140 new cases were reported, adding up to the total number of 2766 positive cases, in which 94 patients were admitted to ICU and 60 patients needed ventilators to support [27]. In one week, the total number of positive cases raised to 3963 cases, in which 92 patients were admitted to ICU, and 50 patients needed ventilatory support [28].
Many studies revealed consistent findings regarding the age-related risk of death from COVID-19 where the elderly possess a higher risk of mortality compared to the younger age group [29,30]. COVID-19 is highly transmissible in humans in the elderly age group (median 47 to 59 years old), progresses fast probably due to weak immune systems, and subsequently develops rapidly into acute respiratory distress syndrome, septic shock, metabolic acidosis, and coagulation dysfunction, even leading to the death [4]. However, from current findings, younger people aged below 60 years old suffered short survival time to death compared to the older aged more than 60 years old. The probable reason for short survival time at a younger age could be due to obesity, although the impact of obesity on COVID-19 severity has not been thoroughly explored. Our assumption is relevant since the prevalence of overweight or obesity among adults in Malaysia as high as 50.1% [31]. In a previous study, obesity was found to be associated with increased severity and mortality in the H1N1 influenza pandemic and other respiratory viruses [32]. A recent retrospective study carried out in Singapore revealed a BMI of more or equal 25.0 kgm−2 among COVID-19 patients less than 60 years old was significantly associated with pneumonia on chest radiograph on admission (p-value = 0.017), requiring low flow supplemental oxygen (odds ratio (OR) 6.32; 95% CI: 1.23–32.34) and mechanical ventilation (OR, 1.16; 95% CI: 1.00–1.34), and higher serum lactate dehydrogenase levels (p-value = 0.011) [33]. Another retrospective study carried out in New York City revealed a similar association where patients aged less than 60 years with a BMI between 30 and 34 kgm−2 were 2.0 times (95% CI: 1.6–2.6; p-value < 0.0001) and 1.8 times (95% CI: 1.2–2.7; p-value = 0.006) more likely to be admitted to acute and critical care, respectively, compared to individuals with a BMI less than 30 kgm−2 [2,34].
Patients suffering from malignancy, particularly those with pulmonary malignancy, have been reported by multiple series to have disproportionally increased severity outcomes from COVID-19, including higher rates of hospitalization and death [35]. Pulmonary malignancy was shown to be the most frequent type of cancer among COVID-19 positive cases [18,36], and poses a higher risk of COVID-19 mortality [37]. Our results seem to mirror the typical prognosis of patients with pulmonary malignancy. A study revealed that among the four most common malignancies within the United States population (lung, breast, prostate, and colorectal), the mortality among COVID-19 patients with pulmonary malignancy was found to have the highest mortality 55.0%, followed by colorectal malignancy 38.0%, prostate malignancy 20.0%, and breast malignancy 14.0% [20]. Another study showed that COVID-19 patients with pulmonary malignancy had the second-highest risk levels after blood malignancy, with a mortality rate of 18.2%, with an average time to death of 16.75 ± 8.17 days [36]. COVID-19 patients with pulmonary malignancy are at risk for pulmonary complications not only from their malignancy but also from the potential of COVID-19 infection, and the interaction between these factors probably put this patient at risk for poor prognosis, despite optimal medical supports such as mechanical ventilation and intensive care [38].
The COVID-19 pandemic poses challenges for oncology services around the globe. The rate at which COVID-19 is going through, without treatment, malignancy could progressively worsen. Singh et al. suggested that pulmonary malignancy treatment should be continued without any delays, or otherwise, it could result in rapid cancer progression, and the principle of the treatment should continue to be individualized, with careful consideration of risks and benefits of continuing or altering pulmonary malignancy directed therapy [38]. An American College of Chest Physicians (CHEST) panel expert agreed that the risk of a delay in screening, in surveillance imaging, in avoidance of biopsy procedures, or delaying management of early cancer is low, and suggested that the patient’s care should be discussed in a multidisciplinary tumor board setting if available, and to consider the factors that may influence the decision; COVID-19 penetrance in the community and hospital, availability of rapid COVID-19 testing, availability of resources, the availability of other sites that could accommodate the patient, patient values, and comorbid conditions [39]. Patients with pulmonary malignancy who are undergoing active chemotherapy or radical radiotherapy are particularly vulnerable to serious illness if they become infected with COVID-19 [40]. With the spread of COVID-19, patients with pulmonary malignancy should be considered as the key targets for epidemic control as they will develop severe symptoms after infection with COVID-19, with a high mortality rate. Precise and individual management is crucial in lung cancer patients, and they should receive maximum protection to effectively prevent COVID-19 [41].
Mass gatherings occur as a result of proper human planning such as a religious event (the Hajj), cultural event (Olympics, musical concert, etc.), political event (election), economic event (exhibition, carnival, and expo), or it can occur spontaneously (unplanned) due to natural disasters such as mass evacuation [42]. Mass gatherings have no doubt contributed to the spread of infectious diseases. The mass gathering is not only about how people close to each other make physical contact, but it also highlights how people are connected. As such, the movement of people across these geographies would intensify the spread of COVID-19 [43]. The best example would be the situation and magnitude of the outbreak that happened in Iran, now considered the second epicenter of COVID-19. The epidemic in Iran began in Qom, a city with a population of 1.2 million, where it attracted 20.0 million annual pilgrims from neighboring countries with Shiite Muslim populations (Afghanistan, Iraq, Lebanon, Syria, and Pakistan), which contributed to 593 positive cases and 43 deaths as of 1 March 2020 [42]. The situation was similar to what had happened in Malaysia. The largest COVID-19 cluster in Malaysia, namely the Seri Petaling tabligh cluster was detected following a large religious gathering that was held at a mosque in Seri Petaling, Kuala Lumpur from 27 February 2020 to 3 March 2020, and was attended by 16,000 people (14,500 Malaysian citizens and 1500 non-citizens from various countries). As of 8 July 2020, a total of 42,023 individuals have been screened in this cluster. Of these, 3375 positive cases (38.9%) were reported, with 15 mortality cases [44].
The COVID-19 infection was growing exponentially and accelerating by human migration and movement, in which the exported cases have been reported in various regions of the world, including Europe, Asia, North America, and Oceania [45]. China was the first country to decide to suspend all modes of transportation to and from Wuhan in January 2020 including vehicles, trains, and flights [45]. Since then, the travel restriction, border control, and MCO have been implemented by various countries including Malaysia. These actions have a similar purpose, to cut off the chain of infection in the population. Studies have observed the efficacy of a travel ban on the incidences of COVID-19 importations. For example, the travel ban in Wuhan had a marked effect on the international scale, where case importations were reduced by nearly 80.0% until mid-February [46], which was consistent with the estimation from the statistical model, where 226 exported cases can be prevented by travel reduction to and from China in January–February 2020 [47]. Another study found that the magnitude of the early epidemic outside of Wuhan was very well predicted by the volume of human movement out of Wuhan, China alone (r2 = 0.89), in which cases exported from Wuhan before the cordon sanitaire appear to have contributed to initiating local chains of transmission in both neighboring provinces and more distant provinces [48]. The MCO implemented by the Malaysian government prohibits mass movements and mass gatherings at all places nationwide including religious services, and the closure of all business premises except manufacturers, suppliers, retailers, and food outlets. The MCO signifies a major step taken by the Malaysian Government to contain the COVID-19 pandemic, which has been deemed the main reason behind the decrease in new COVID-19 cases since mid-April [49]. A study carried out in Malaysia found that a reduction in peak active cases by 99.1%, where the implementation of the MCO measures in Malaysia has effectively controlled the outbreak [50].
The COVID-19 mortality rate could be due to the virological aspect. The ribonucleic acid (RNA) viruses are, in general, highly susceptible to mutations, and prone to have a high degree of changes [51]. The emergence of a more virulent COVID-19 virus was identified to infect certain countries. In a genetic study carried out in the United States, the virus mainly came from Asia through a small number of infected individuals in California, while in New York, more than 100 people initially brought the virus mainly from Europe, suggesting that the European type viruses are more virulent in their pathogenicity and infectivity than the Asian type [52]. Another genetic study also suggested that COVID-19 mutation as one of the important factors that might affect the susceptibility to COVID-19 infection or severity of COVID-19, in which mutation of COVID-19 happened most frequently in Europe (81.3%), followed by South America (73.2%) and Asia (14.7%), with an average fatality rate of 9.3%, 5.8%, and 3.0%, respectively [53]. In the current study, all mortality cases in Malaysia with a history of travelling to Turkey, Saudi Arabia, India, Vietnam, and Indonesia, there is a possibility that mutation of the virus happened and the emergence of the more virulent virus in those countries, but we were unable to retrieve the strain of COVID-19 viruses isolated from these patients. Additionally, MOH had detected a cluster in Sarawak, where the index case (case 1580) had a history of travelling to Italy and affected 37 people including five mortality cases, which supports the evidence as mention above [54].
5. Limitation
There are a few limitations to this study. Firstly, the data collected are taken from publicly announced information, hence it is incomplete. This is to preserve data confidentiality according to the Personal Data Protection Act 2010 [55] and Personal Data Protection Regulations 2013 [56]. Second, the collected data on risk factors were publicly announced in layman’s terms. Thereby the data were not based on the ICD-10 and made it difficult to classify the accurate risk factors. Thirdly, this is a short duration study. Data were collected throughout June 2020. Mortality cases were limited to 100 because of incomplete information, and ongoing pandemic and mortality. Despite this, we believe this study can provide thorough information on the COVID-19 mortality cases here in Malaysia as of now.
6. Conclusions
The COVID-19 mortality rate of Malaysia was among the lowest in the world during the second wave COVID-19 outbreak (March to May 2020). The highest comorbidity risk factor identified from the current study was hypertension, followed by diabetes mellitus, cardiovascular diseases, extra-pulmonary solid malignancy, pulmonary diseases, and pulmonary malignancy. Those who had pulmonary malignancy, history of attending a mass gathering, and history of travelling overseas were identified as associated factors of COVID-19 mortality cases during the huge second wave COVID-19 outbreak in Malaysia.
Author Contributions
This article is a requirement of M.S.A.W., S.P.C., C.J., M.F.M. and A.A.A.H. Doctorate of Public Health (DrPH) program. The research was conducted by M.S.A.W., S.P.C., C.J., R.S.S., M.F.M. and A.A.A.H. and supervised by M.H.J. and R.I. M.S.A.W., S.P.C., C.J., R.S.S., M.F.M. and A.A.A.H. conceived the conception and design of the study. S.P.C., C.J., R.S.S., M.F.M. and A.A.A.H. set up and organized the database. M.S.A.W. performed the data and statistical analysis. M.S.A.W. prepared the draft of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to express their gratitude and appreciation to the Department of Community Health, Faculty of Medicine, the National University of Malaysia for the assistance given for this research. The authors would also like to acknowledge the Director-General of Health, Malaysia for the data provided.
Conflicts of Interest
The authors declare no conflict of interest.
Ethics Approval and Consent to Participate
Ethical review and approval were not required for this study since the data obtained were sec-ondary data from the Ministry of Health (MOH) Malaysia open-access website and no confiden-tial information such as patient’s data was revealed in this study.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article. The da-tasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
| BMI | Body mass index |
| CHEST | American College of Chest Physicians |
| CMCO | Conditional Movement Control Order |
| COVID-19 | Coronavirus Disease 2019 |
| CPRC | Crisis Preparedness and Response Centre |
| HSB | Sungai Buloh General Hospital |
| MCO | Movement Control Order |
| MERS-CO | Middle East Respiratory Syndrome Coronavirus |
| MOH | Ministry of Health |
| HR | Hazard ratio |
| ICD | International Classification of Disease |
| OR | Odds ratio |
| PHEIC | Public Health Emergency of International Concern |
| PUI | Person under surveillance |
| RNA | Ribonucleic acid |
| SARS-COV | Severe acute respiratory syndrome coronavirus |
| SD | Standard deviation |
| SPSS | Statistical Package for the Social Sciences |
| WHO | World Health Organization |
| UKM | University Kebangsaan Malaysia (National University of Malaysia) |
References
- Centers for Disease Control and Prevention. Coronavirus Disease 2019 (COVID-19). Available online: https://www.cdc.gov/coronavirus/2019-ncov/cdcresponse/about-COVID-19.html (accessed on 6 October 2020).
- Zhu, Z.; Lian, X.; Su, X.; Wu, W.; Marraro, G.A.; Zeng, Y. From SARS and MERS to COVID-19: A brief summary and comparison of severe acute respiratory infections caused by three highly pathogenic human coronaviruses. Respir. Res. 2020, 21, 1–14. [Google Scholar] [CrossRef]
- Lai, C.-C.; Shih, T.-P.; Ko, W.-C.; Tang, H.-J.; Hsueh, P.-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.R.; Cao, Q.D.; Hong, Z.S.; Tan, Y.Y.; Chen, S.D.; Jin, H.J.; Tan, K.S.; Wang, D.Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Mil. Med. Res. 2020, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Abd El-Aziz, T.M.; Stockand, J.D. Recent progress and challenges in drug development against COVID-19 coronavirus (SARS-CoV-2)-an update on the status. Infect. Genet. Evol. 2020, 83, 104327. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Total Confirmed Deaths Due to COVID-19. 31 December 2019–6 October 2020. Available online: https://ourworldindata.org/grapher/total-COVID-deaths-region?tab=table&time=2020-01-11..2020-10-06 (accessed on 6 October 2020).
- Ministry of Health Malaysia. Director General of Health Press Statement 5 October 2020-Current Situation of Coronavirus Disease 2019 (COVID-19) in Malaysia. Available online: https://kpkesihatan.com/2020/10/05/kenyataan-akhbar-kpk-5-oktober-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-COVID-19-di-malaysia/ (accessed on 14 June 2020).
- Ministry of Health Malaysia. Director General of Health Press Statement 25 January 2020-Detection of New Cases Confirmed Infected 2019 Novel Coronavirus (2019-nCoV) in Malaysia. Available online: https://kpkesihatan.com/2020/01/25/kenyataan-akhbar-kpk-25-januari-2020-pengesanan-kes-baharu-yang-disahkan-dijangkiti-2019-novel-coronavirus-2019-ncov-di-malaysia/ (accessed on 6 October 2020).
- Mat, N.F.C.; Edinur, H.A.; Razab, M.K.A.A.; Safuan, S. A single mass gathering resulted in massive transmission of COVID-19 infections in Malaysia with further international spread. J. Travel Med. 2020, 27, 1–4. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia. Director General of Health Press Statement 13 March 2020-Current Situation of Coronavirus Disease 2019 (COVID-19) in Malaysia. Available online: https://kpkesihatan.com/2020/03/13/kenyataan-akhbar-kpk-13-mac-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-COVID-19-di-malaysia/ (accessed on 6 October 2020).
- Ministry of Health Malaysia. Directed General of Health Press Statement 7 April 2020-Current Situation of Coronavirus Disease 2019 (COVID-19) in Malaysia. Available online: https://kpkesihatan.com/2020/04/07/kenyataan-akhbar-kpk-7-april-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-COVID-19-di-malaysia/ (accessed on 6 October 2020).
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Wu, Y.-C.; Chen, C.-S.; Chan, Y.-J. The outbreak of COVID-19: An overview. J. Chin. Med. Assoc. 2020, 83, 217. [Google Scholar] [CrossRef]
- Chen, S.; Yang, J.; Yang, W.; Wang, C.; Bärnighausen, T. COVID-19 control in China during mass population movements at New Year. Lancet 2020, 395, 764–766. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Westblade, L.F.; Brar, G.; Pinh, L.C.; Paid, D.; Rajan, M.; Martin, P.; Goyal, P.; Sepulveda, J.L.; Zhang, L.; George, G.; et al. SARS-CoV-2 viral load predicts mortality in patients with and without cancer who are hospitalized with COVID-19. Cancer Cell 2020, 38, 661–671. [Google Scholar] [CrossRef]
- Mehta, V.; Goel, S.; Kabarriti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case fatality rate of cancer patients with COVID-19 in a New York hospital system. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Department of Statistics Malaysia. Demographic Statistics First Quarter 2020, Malaysia. Released by Dato’ Sri Dr. Mohd Uzir Mahidin, Chief Statistician Malaysia, Department of Statistics Malaysia. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=430&bul_id=aFYzVjJ3anNyQytHZGxzcUZxTG9Ydz09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09 (accessed on 14 June 2020).
- Ministry of Health Malaysia. Guidelines COVID-19 Management No. 5/2020 Update on 24 March 2020. Available online: http://www.umk.edu.my/covid19/doc/Garispanduan-COVID19-Edisi-5_2020.pdf (accessed on 14 June 2020).
- Ministry of Health Malaysia. The List of District Health Office in Malaysia. Available online: https://www.moh.gov.my/index.php/database_stores/store_view/5?items=25&page=1 (accessed on 14 June 2020).
- Ministry of Health Malaysia. From the Desk of the Director-General of Health Malaysia. Available online: https://kpkesihatan.com/ (accessed on 6 October 2020).
- European Centre for Disease Prevention and Control. Our World in Data. Case Fatality Rate of the Ongoing COVID-19 Pandemic. Available online: https://ourworldindata.org/coronavirus-data-explorer?zoomToSelection=true&time=2020-03-14..latest&country=OWID_WRL~BRN~MYS~THA~VNM~IDN~PHL~GBR~USA®ion=World&cfrMetric=true&interval=total&aligned=true&hideControls=true&smoothing=0&pickerMetric=location&pickerSort=asc (accessed on 6 October 2020).
- Ministry of Health Malaysia. From the Desk of the Director-General of Health Malaysia-The Malaysian Response to COVID-19: Building Preparedness for ‘Surge Capacity’, Testing Efficiency, and Containment. Available online: https://kpkesihatan.com/2020/06/16/the-malaysian-response-to-COVID-19-building-preparedness-for-surge-capacity-testing-efficiency-and-containment/ (accessed on 18 August 2020).
- Ministry of Health Malaysia. Press Release Ministry of Health Malaysia. Current Situation During Coronavirus Disease Infection 2019 (COVID-19) in Malaysia 31 March 2020. Available online: https://www.moh.gov.my/index.php/database_stores/attach_download/337/1410 (accessed on 18 August 2020).
- Ministry of Health Malaysia. Press Release Ministry of Health Malaysia. Current Situation During Coronavirus Disease Infection 2019 (COVID-19) in Malaysia 7 April 2020. Available online: https://www.moh.gov.my/index.php/database_stores/attach_download/337/1431 (accessed on 18 August 2020).
- Promislow, D.E.L. A Geroscience Perspective on COVID-19 Mortality. J. Gerontol. Ser. A 2020, 75, e30–e33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.; Chen, X.; Cai, Y.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; Zhang, Y.; et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute for Public Health Malaysia. National Health and Morbidity Survey (NHMS) 2019. Non-Communicable Diseases, Healthcare Demand, and Health Literacy: Key Findings. Available online: http://iku.moh.gov.my/images/IKU/Document/REPORT/NHMS2019/Infographic_Booklet_NHMS_2019-English.pdf (accessed on 6 October 2020).
- Moser, J.A.S.; Galindo-Fraga, A.; Ortiz-Hernández, A.A.; Gu, W.; Hunsberger, S.; Galán-Herrera, J.F.; Guerrero, M.L.; Ruiz-Palacios, G.M.; Beigel, J.H.; La Red ILI 002 Study Group; et al. Underweight, overweight, and obesity as independent risk factors for hospitalization in adults and children from influenza and other respiratory viruses. Influenza Other Respir. Viruses 2019, 13, 3–9. [Google Scholar] [CrossRef]
- Ong, S.W.X.; Young, B.E.; Leo, Y.-S.; Lye, D.C. Association of Higher Body Mass Index With Severe Coronavirus Disease 2019 (COVID-19) in Younger Patients. Clin. Infect. Dis. 2020, 71, 2300–2302. [Google Scholar] [CrossRef]
- Lighter, J.; Phillips, M.; Hochman, S.; Sterling, S.; Johnson, D.; Francois, F.; Stachel, A. Obesity in patients younger than 60 years is a risk factor for COVID-19 hospital admission. Clin. Infect. Dis. 2020, 71, 896–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, J.; Rizvi, H.; Preeshagul, I.R.; Egger, J.V.; Hoyos, D.; Bandlamudi, C.; McCarthy, C.G.; Falcon, C.J.; Schoenfeld, A.J.; Arbour, K.C.; et al. COVID-19 in patients with lung cancer. Ann. Oncol. 2020, 31, 1386–1396. [Google Scholar] [CrossRef]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-COV-2: A multicenter study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Kabarriti, R.; Brodin, N.P.; Maron, M.I.; Tomé, W.A.; Halmos, B.; Guha, C.; Kalnicki, S.; Garg, M.K.; Ohri, N. Extent of prior lung irradiation and mortality in COVID-19 patients with a cancer history. Adv. Radiat. Oncol. 2020, 5, 707–710. [Google Scholar] [CrossRef]
- Singh, A.P.; Berman, A.T.; Marmarelis, M.E.; Haas, A.R.; Feigenberg, S.J.; Braun, J.; Ciunci, C.A.; Bauml, J.M.; Cohen, R.B.; Kucharczuk, J.C.; et al. Management of lung cancer during the COVID-19 pandemic. JCO Oncol. Pract. 2020, 16, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, P.J.; Gould, M.K.; Arenberg, D.A.; Chen, A.C.; Choi, H.K.; Detterbeck, F.C.; Farjah, F.; Fong, K.M.; Iaccarino, J.M.; Janes, S.M.; et al. Management of lung nodules and lung cancer screening during the COVID-19 pandemic: CHEST expert panel report. Chest 2020, 158, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Burki, T.K. Cancer guidelines during the COVID-19 pandemic. Lancet Oncol. 2020, 21, 629–630. [Google Scholar] [CrossRef]
- Xu, Y.; Liu, H.; Hu, K.; Wang, M. Clinical recommendations on lung cancer management during the COVID-19 pandemic. Thorac. Cancer 2020, 11, 2067–2074. [Google Scholar] [CrossRef]
- Ebrahim, S.H.; Memish, Z.A. COVID-19–the role of mass gatherings. Travel Med. Infect. Dis. 2020, 34, 101617. [Google Scholar] [CrossRef]
- Parnell, D.; Widdop, P.; Bond, A.; Wilson, R. COVID-19, networks and sport. Manag. Sport Leis. 2020, 25, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health Malaysia. Director General of Health Press Statement 18 July 2020-Current Situation of Coronavirus Disease 2019 (COVID-19) in Malaysia. Available online: https://kpkesihatan.com/2020/07/08/kenyataan-akhbar-kpk-8-julai-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-COVID-19-di-malaysia/ (accessed on 16 August 2020).
- Studdert, D.M.; Hall, M.A.; Mello, M.M. Partitioning the Curve—Interstate Travel Restrictions During the COVID-19 Pandemic. N. Engl. J. Med. 2020, 383, e83. [Google Scholar] [CrossRef]
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; y Piontti, A.P.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Anzai, A.; Kobayashi, T.; Linton, N.M.; Kinoshita, R.; Hayashi, K.; Suzuki, A.; Yang, Y.; Jung, S.M.; Miyama, T.; Akhmetzhanov, A.R.; et al. Assessing the impact of reduced travel on exportation dynamics of novel coronavirus infection (COVID-19). J. Clin. Med. 2020, 9, 601. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, M.U.; Yang, C.H.; Gutierrez, B.; Wu, C.H.; Klein, B.; Pigott, D.M.; Du Plessis, L.; Faria, N.R.; Li, R.; Hanage, W.P.; et al. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 2020, 368, 493–497. [Google Scholar] [CrossRef] [Green Version]
- Tang, K.H.D. Movement control as an effective measure against COVID-19 spread in Malaysia: An overview. J. Public Health 2020, 28, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Gill, B.S.; Jayaraj, V.J.; Singh, S.; Mohd Ghazali, S.; Cheong, Y.L.; Md Iderus, N.H.; Sundram, B.M.; Aris, T.B.; Mohd Ibrahim, H.; Hong, B.H.; et al. Modelling the Effectiveness of Epidemic Control Measures in Preventing the Transmission of COVID-19 in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 5509. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Bauer, G. Apparent difference in fatalities between Central Europe and East Asia due to SARS-COV-2 and COVID-19: Four hypotheses for possible explanation. Med. Hypotheses 2020, 144, 110160. [Google Scholar] [CrossRef]
- Gonzalez-Reiche, A.S.; Hernandez, M.M.; Sullivan, M.J.; Ciferri, B.; Alshammary, H.; Obla, A.; Fabre, S.; Kleiner, G.; Polanco, J.; Khan, Z.; et al. Introductions and early spread of SARS-CoV-2 in the New York City area. Science 2020, 369, 297–301. [Google Scholar] [CrossRef]
- Toyoshima, Y.; Nemoto, K.; Matsumoto, S.; Nakamura, Y.; Kiyotani, K. SARS-CoV-2 genomic variations associated with mortality rate of COVID-19. J. Hum. Genet. 2020, 65, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Malaysia. Director General of Health Press Statement 5 April 2020-Current Situation of Coronavirus Disease 2019 (COVID-19) in Malaysia. Available online: https://kpkesihatan.com/2020/04/05/kenyataan-akhbar-kpk-5-april-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-COVID-19-di-malaysia/ (accessed on 6 October 2020).
- Department of Personal Data Protection Malaysia. Act 709, Personal Data Protection Act. Available online: https://www.pdp.gov.my/jpdpv2/assets/2019/09/Personal-Data-Protection-Act-2010.pdf (accessed on 6 October 2020).
- Department of Personal Data Protection Malaysia. Federal Government Gazette. P.U. (A) 335, Personal Data Protection Regulations 2013. Available online: https://www.pdp.gov.my/jpdpv2/assets/2019/09/Peraturan-peraturan_Perlindungan_Data_Peribadi.pdf (accessed on 6 October 2020).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).