
The Role of Lactic Acid in the Management of Bacterial Vaginosis: A Systematic Literature Review


Abstract
1. Introduction
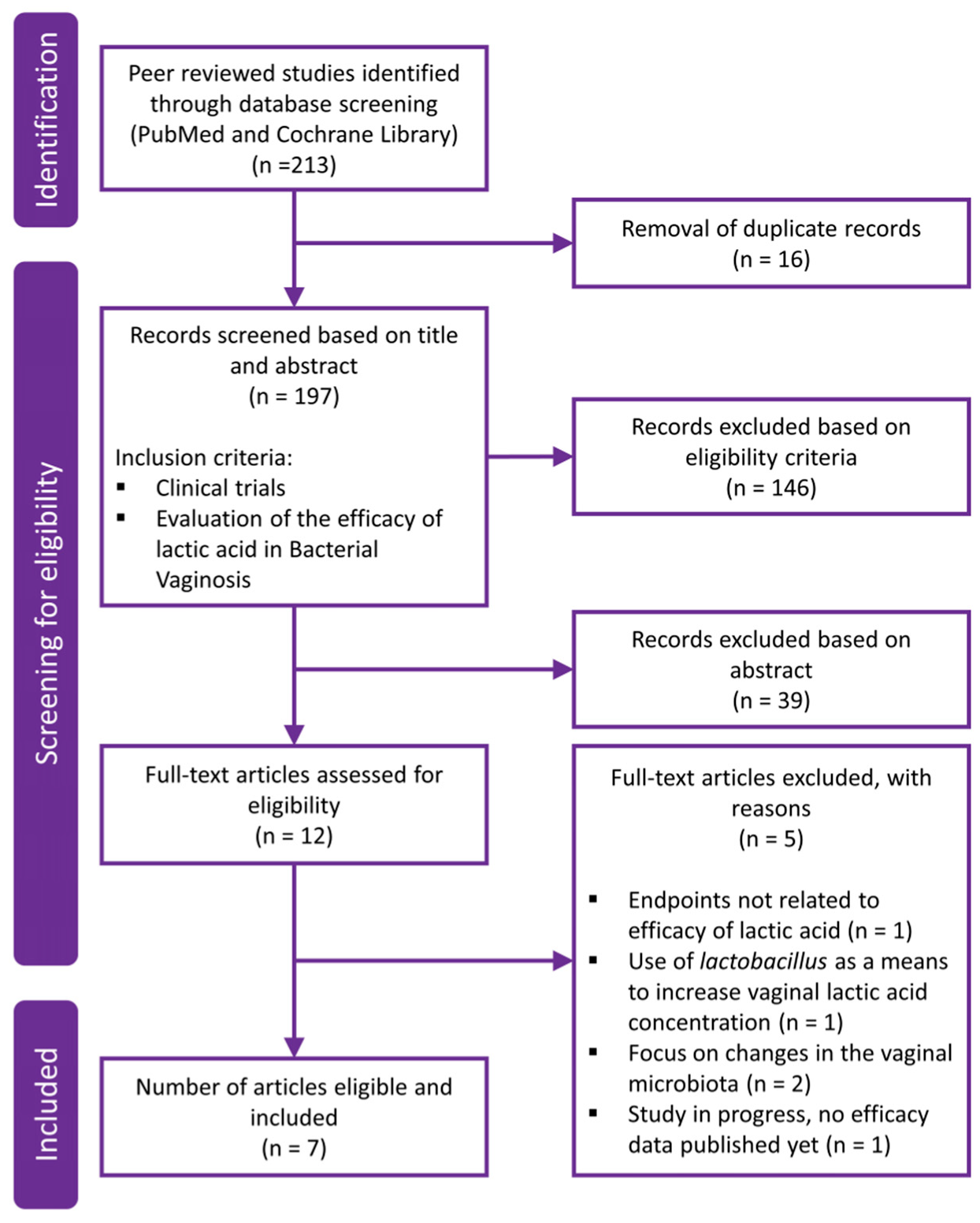
2. Methods
3. Results
3.1. Clinical Evaluation of Lactic Acid in Symptomatic BV
3.2. Clinical Evaluation of Lactic Acid in Recurrent BV
3.3. Clinical Evaluation of Lactic Acid in Symptomatic BV during Pregnancy
4. Discussion
4.1. BV in Nonpregnancy
4.1.1. First Time BV
4.1.2. Recurrent BV
4.2. BV in Pregnancy
4.2.1. Pregnant with BV
4.2.2. Planning Pregnancy with Mild BV
4.3. Mixed Infections
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Li, J.; McCormick, J.; Bocking, A.; Reid, G. Importance of vaginal microbes in reproductive health. Reprod. Sci. 2012, 19, 235–242. [Google Scholar] [CrossRef]
- Diop, K.; Dufour, J.C.; Levasseur, A.; Fenollar, F. Exhaustive repertoire of human vaginal microbiota. Hum. Microbiome J. 2019, 11, 100051. [Google Scholar] [CrossRef]
- Mendling, W. Vaginal microbiota. Adv. Exp. Med. Biol. 2016, 902, 83–93. [Google Scholar] [PubMed]
- Saraf, V.S.; Sheikh, S.A.; Ahmad, A.; Gillevet, P.M.; Bokhari, H.; Javed, S. Vaginal microbiome: Normalcy vs dysbiosis. Arch. Microbiol. 2021, 203, 3793–3802. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Lu, Y.; Chen, T.; Li, R. The Female Vaginal Microbiome in Health and Bacterial Vaginosis. Front. Cell. Infect. Microbiol. 2021, 11, 631972. [Google Scholar] [CrossRef]
- Buchta, V. Vaginal microbiome. Ces. Gynekol. 2018, 83, 371–379. [Google Scholar]
- Amabebe, E.; Anumba, D.O.C. The Vaginal Microenvironment: The Physiologic Role of Lactobacilli. Front. Med. 2018, 5, 181. [Google Scholar] [CrossRef]
- Klebanoff, M.A.; Schwebke, J.R.; Zhang, J.; Nansel, T.R.; Yu, K.F.; Andrews, W.W. Vulvovaginal symptoms in women with bacterial vaginosis. Obstet. Gynecol. 2004, 104, 267–272. [Google Scholar] [CrossRef]
- Reiter, S.; Spadt, S.K. Bacterial vaginosis: A primer for clinicians. Postgrad. Med. 2019, 131, 8–18. [Google Scholar] [CrossRef]
- Javed, A.; Parvaiz, F.; Manzoor, S. Bacterial Vaginosis: An insight into the prevalence, alternative regimen treatments and its associated resistance patterns. Microb. Pathog. 2019, 127, 21–30. [Google Scholar] [CrossRef]
- Joseph, R.J.; Ser, H.L.; Kuai, Y.H.; Tan, L.T.-H.; Arasoo, V.J.T.; Letchumanan, V.; Wang, L.; Pusparajah, P.; Goh, B.-H.; Ab Mutalib, N.-S.; et al. Finding a Balance in the Vaginal Microbiome: How Do We Treat and Prevent the Occurrence of Bacterial Vaginosis? Antibiotics 2021, 10, 719. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, C.S.; Sobel, J.D. Current Treatment of Bacterial Vaginosis-Limitations and Need for Innovation. J. Infect. Dis. 2016, 214, S14–S20. [Google Scholar] [CrossRef] [PubMed]
- Hill, G.B. The microbiology of bacterial vaginosis. Am. J. Obstet. Gynecol. 1993, 169, 450–454. [Google Scholar] [CrossRef]
- Kalia, N.; Singh, J.; Kaur, M. Microbiota in vaginal health and pathogenesis of recurrent vulvovaginal infections: A critical review. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 5. [Google Scholar] [CrossRef]
- Muzny, C.A.; Taylor, C.M.; Swords, W.E.; Tamhane, A.; Chattopadhyay, D.; Cerca, N.; Schwebke, J.R. An Updated Conceptual Model on the Pathogenesis of Bacterial Vaginosis. J. Infect. Dis. 2019, 220, 1399–1405. [Google Scholar] [CrossRef]
- Lamont, R.F.; Sobel, J.D.; Akins, R.A.; Hassan, S.S.; Chaiworapongsa, T.; Kusanovic, J.P.; Romeroa, R. The vaginal microbiome: New information about genital tract flora using molecular based techniques. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 533–549. [Google Scholar] [CrossRef]
- Swidsinski, A.; Mendling, W.; Loening-Baucke, V.; Ladhoff, A.; Swidsinski, S.; Hale, L.P.; Lochs, H. Adherent biofilms in bacterial vaginosis. Obstet. Gynecol. 2005, 106, 1013–1023. [Google Scholar] [CrossRef]
- Allsworth, J.E.; Peipert, J.F. Prevalence of bacterial vaginosis: 2001–2004 National Health and Nutrition Examination Survey data. Obstet. Gynecol. 2007, 109, 114–120. [Google Scholar] [CrossRef]
- Marrazzo, J.M. Interpreting the epidemiology and natural history of bacterial vaginosis: Are we still confused? Anaerobe 2011, 17, 186–190. [Google Scholar] [CrossRef]
- Peebles, K.; Velloza, V.; Balkus, J.E.; McClelland, R.S.; Barnabas, R.V. High Global Burden and Costs of Bacterial Vaginosis: A Systematic Review and Meta-Analysis. Sex. Transm. Dis. 2019, 46, 304–311. [Google Scholar] [CrossRef]
- Yalew, G.T.; Muthupandian, S.; Hagos, K.; Negash, L.; Venkatraman, G.; Hagos, Y.M.; Meles, H.N.; Weldehaweriat, H.H.; Al-Dahmoshi, H.O.M.; Saki, M. Prevalence of bacterial vaginosis and aerobic vaginitis and their associated risk factors among pregnant women from northern Ethiopia: A cross-sectional study. PLoS ONE 2022, 17, e0262692. [Google Scholar] [CrossRef] [PubMed]
- Mulinganya, G.; de Vulder, A.; Bisimwa, G.; Boelens, J.; Claeys, G.; De Keyser, K.; De Vos, D.; Hendwa, E.; Kampara, F.; Kujirakwinja, Y.; et al. Prevalence, risk factors and adverse pregnancy outcomes of second trimester bacterial vaginosis among pregnant women in Bukavu, Democratic Republic of the Congo. PLoS ONE 2021, 16, e0257939. [Google Scholar] [CrossRef]
- Amsel, R.; Totten, P.A.; Spiegel, C.A.; Chen, K.C.S.; Eschenbach, D.; Holmes, K.K. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am. J. Med. 1983, 74, 14–22. [Google Scholar] [CrossRef]
- Koumans, E.H.; Sternberg, M.; Bruce, C.; McQuillan, G.; Kendrick, J.; Sutton, M.; Markowitz, L.E. The prevalence of bacterial vaginosis in the United States, 2001–2004; associations with symptoms, sexual behaviors, and reproductive health. Sex. Transm. Dis. 2007, 34, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Coudray, M.S.; Madhivanan, P. Bacterial vaginosis-A brief synopsis of the literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 245, 143–148. [Google Scholar] [CrossRef]
- Kairys, N.; Garg, M. Bacterial Vaginosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020; pp. 1–6. [Google Scholar]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef]
- Singh, R.; Ramsuran, V.; Mitchev, N.; Niehaus, A.J.; Han, K.S.S.; Osman, F.; Ngcapu, S.; Karim, S.A.; Rompalo, A.; Garrett, N.; et al. Assessing a diagnosis tool for bacterial vaginosis. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1481–1485. [Google Scholar] [CrossRef] [PubMed]
- Watkins, J.A.; Ross, J.D.C.; Thandi, S.; Brittain, C.; Kai, J.; Griffiths, F. Acceptability of and treatment preferences for recurrent bacterial vaginosis—Topical lactic acid gel or oral metronidazole antibiotic: Qualitative findings from the VITA trial. PLoS ONE 2019, 14, e0224964. [Google Scholar] [CrossRef]
- Colonna, C.; Steelman, M. Amsel Criteria. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Donders, G.G.G. Definition and classification of abnormal vaginal flora. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 355–373. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, L.; Zhao, M.; Wang, Y.; Bai, H.; Wang, Y.; Rui, C.; Fan, C.; Li, J.; Li, N.; et al. Deep Neural Networks Offer Morphologic Classification and Diagnosis of Bacterial Vaginosis. J. Clin. Microbiol. 2021, 59, e02236-20. [Google Scholar] [CrossRef] [PubMed]
- Cherpes, T.L.; Meyn, L.A.; Krohn, M.A.; Lurie, J.G.; Hillier, S.L. Association between acquisition of herpes simplex virus type 2 in women and bacterial vaginosis. Clin. Infect. Dis. 2003, 37, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Abbai, N.S.; Reddy, T.; Ramjee, G. Prevalent bacterial vaginosis infection—a risk factor for incident sexually transmitted infections in women in Durban, South Africa. Int. J. STD AIDS 2016, 27, 1283–1288. [Google Scholar] [CrossRef]
- Balkus, J.E.; Richardson, B.A.; Rabe, L.K.; Taha, T.E.; Mgodi, N.; Kasaro, M.P.; Ramjee, G.; Hoffman, I.F.; Karim, S.S.A. Bacterial vaginosis and the risk of trichomonas vaginalis acquisition among HIV-1-negative women. Sex. Transm. Dis. 2014, 41, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Sewankambo, N.; Gray, R.H.; Wawer, M.J.; Paxton, L.; McNairn, D.; Wabwire-Mangen, F.; Serwadda, D.; Li, C.; Kiwanuka, N.; Hillier, S.L. HIV-1 infection associated with abnormal vaginal flora morphology and bacterial vaginosis. Lancet 1997, 350, 546–550. [Google Scholar] [CrossRef]
- Redelinghuys, M.J.; Geldenhuys, J.; Jung, H.; Kock, M.M. Bacterial Vaginosis: Current Diagnostic Avenues and Future Opportunities. Front. Cell. Infect. Microbiol. 2020, 10, 354. [Google Scholar] [CrossRef] [PubMed]
- Ellington, K.; Saccomano, S.J. Recurrent bacterial vaginosis. Nursing 2021, 51, 48–52. [Google Scholar] [CrossRef]
- Armstrong, E.; Kaul, R. Beyond bacterial vaginosis: Vaginal lactobacilli and HIV risk. Microbiome 2021, 9, 239. [Google Scholar] [CrossRef]
- Workowski, K.A.; Bolan, G.A. Sexually transmitted diseases treatment guidelines, 2015. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 1–138. [Google Scholar]
- Sherrard, J.; Wilson, J.; Donders, G.; Mendling, W.; Jensen, J.S. 2018 European (IUSTI/WHO) International Union against sexually transmitted infections (IUSTI) World Health Organisation (WHO) guideline on the management of vaginal discharge. Int. J. STD AIDS 2018, 29, 1258–1272. [Google Scholar] [CrossRef]
- Larsson, P.G.; Forsum, U. Bacterial vaginosis—A disturbed bacterial flora and treatment enigma. APMIS 2005, 113, 305–316. [Google Scholar] [CrossRef]
- Vodstrcil, L.A.; Muzny, C.A.; Plummer, E.L.; Sobel, J.; Bradshaw, C.S. Bacterial vaginosis: Drivers of recurrence and challenges and opportunities in partner treatment. BMC Med. 2021, 19, 194. [Google Scholar] [CrossRef] [PubMed]
- Swidsinski, A.; Mendling, W.; Loening-Baucke, V.; Swidsinski, S.; Dörffel, Y.; Scholze, J.; Lochs, H.; Verstraelen, H. An adherent Gardnerella vaginalis biofilm persists on the vaginal epithelium after standard therapy with oral metronidazole. Am. J. Obstet. Gynecol. 2008, 198, 97.e1–97.e6. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, C.; Rolo, J.; Cerca, N.; Palmeira-de-Oliveira, R.; Martinez-de-Oliveira, J.; Palmeira-de-Oliveira, A. Dequalinium Chloride Effectively Disrupts Bacterial Vaginosis (BV) Gardnerella spp. Biofilms. Pathogens 2021, 10, 261. [Google Scholar] [CrossRef] [PubMed]
- Deng, Z.-L.; Gottschick, C.; Bhuju, S.; Masur, C.; Abels, C.; Wagner-Döbler, I. Metatranscriptome Analysis of the Vaginal Microbiota Reveals Potential Mechanisms for Protection against Metronidazole in Bacterial Vaginosis. mSphere 2018, 3, e00262-18. [Google Scholar] [CrossRef]
- Baldacci, F.; Baldacci, M.; Bertini, M. Lactobacillus rhamnosus BMX 54 + Lactose, A Symbiotic Long-Lasting Vaginal Approach to Improve Women’s Health. Int. J. Womens Health 2020, 12, 1099. [Google Scholar] [CrossRef] [PubMed]
- Tomás, M.; Palmeira-de-Oliveira, A.; Simões, S.; Martinez-de-Oliveira, J.; Palmeira-de-Oliveira, R. Bacterial vaginosis: Standard treatments and alternative strategies. Int. J. Pharm. 2020, 587, 119659. [Google Scholar] [CrossRef] [PubMed]
- van de Wijgert, J.H.H.M.; Verwijs, M.C.; Agaba, S.K.; Bronows, C.; Mwambarangwe, L.; Uwineza, M.; Lievens, E.; Nivoliez, A.; Ravel, J.; Darby, A.C. Intermittent Lactobacilli-containing Vaginal Probiotic or Metronidazole Use to Prevent Bacterial Vaginosis Recurrence: A Pilot Study Incorporating Microscopy and Sequencing. Sci. Rep. 2020, 10, 3884. [Google Scholar] [CrossRef] [PubMed]
- Laue, C.; Papazova, E.; Liesegang, A.; Pannenbeckers, A.; Arendarski, P.; Linnerth, B.; Domig, K.J.; Kneifel, W.; Petricevic, L.; Schrezenmeir, J. Effect of a yoghurt drink containing Lactobacillus strains on bacterial vaginosis in women—A double-blind, randomised, controlled clinical pilot trial. Benef. Microbes 2018, 9, 35–50. [Google Scholar] [CrossRef]
- Jeng, H.; Yan, T.; Chen, J. Treating vaginitis with probiotics in non-pregnant females: A systematic review and meta-analysis. Exp. Ther. Med. 2020, 20, 3749–3765. [Google Scholar] [CrossRef]
- Liu, H.F.; Yi, N. A systematic review and meta-analysis on the efficacy of probiotics for bacterial vaginosis. Eur. Rev. Med. Pharmacol. Sci. 2020, 26, 90–98. [Google Scholar]
- dos Santos, A.M.; Carvalho, S.G.; Araujo, V.H.S.; Carvalho, G.C.; Gremião, M.P.D.; Chorilli, M. Recent advances in hydrogels as strategy for drug delivery intended to vaginal infections. Int. J. Pharm. 2020, 590, 119867. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, P.M.; Mohan, M.K.; Konje, J. Bacterial vaginosis in pregnancy—A storm in the cup of tea. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 253, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Chappell, B.T.; Mena, L.A.; Maximos, B.; Mollan, S.; Culwell, K.; Howard, B. EVO100 prevents chlamydia and gonorrhea in women at high risk of infection. Am. J. Obstet. Gynecol. 2021, 225, 162.e1–162.e14. [Google Scholar] [CrossRef] [PubMed]
- O’Hanlon, D.E.; Moench, T.R.; Cone, R.A. Vaginal pH and microbicidal lactic acid when lactobacilli dominate the microbiota. PLoS ONE 2013, 8, e80074. [Google Scholar] [CrossRef] [PubMed]
- Tachedjian, G.; O’Hanlon, D.E.; Ravel, J. The implausible “in vivo” role of hydrogen peroxide as an antimicrobial factor produced by vaginal microbiota. Microbiome 2018, 6, 29. [Google Scholar] [CrossRef]
- Reid, G. Probiotic agents to protect the urogenital tract against infection. Am. J. Clin. Nutr. 2001, 73 (Suppl. S2), 437S–443S. [Google Scholar] [CrossRef]
- O’Hanlon, D.E.; Come, R.A.; Moench, T.R. Vaginal pH measured in vivo: Lactobacilli determine pH and lactic acid concentration. BMC Microbiol. 2019, 191, 13. [Google Scholar] [CrossRef]
- Aldunate, M.; Srbinovski, D.; Hearps, A.C.; Latham, C.F.; Ramsland, P.A.; Gugasyan, R.; Cone, R.A.; Tachedjian, G. Antimicrobial and immune modulatory effects of lactic acid and short chain fatty acids produced by vaginal microbiota associated with eubiosis and bacterial vaginosis. Front. Physiol. 2015, 6, 164. [Google Scholar] [CrossRef]
- Gong, Z.; Luna, Y.; Yu, P.; Fan, H. Lactobacilli Inactivate Chlamydia trachomatis through Lactic Acid but Not H2O2. PLoS ONE 2014, 9, e107758. [Google Scholar]
- Tyssen, D.; Wang, Y.-Y.; Hayward, J.A.; Agius, P.A.; DeLong, K.; Aldunate, M.; Ravel, J.; Moench, T.R.; Cone, R.A.; Tachedjian, G. Anti-HIV-1 Activity of Lactic Acid in Human Cervicovaginal Fluid. mSphere 2018, 3, e00055-18. [Google Scholar] [CrossRef]
- Biliavska, L.; Pankivska, Y.; Povnitsa, O.; Zagorodnya, S. Antiviral Activity of Exopolysaccharides Produced by Lactic Acid Bacteria of the Genera Pediococcus, Leuconostoc and Lactobacillus against Human Adenovirus Type 5. Medicina 2019, 55, 519. [Google Scholar] [CrossRef] [PubMed]
- Keller, M.J.; Carpenter, C.A.; Lo, Y.; Einstein, M.H.; Liu, C.; Fredricks, D.N.; Herold, B.C. Phase I Randomized Safety Study of Twice Daily Dosing of Acidform Vaginal Gel: Candidate Antimicrobial Contraceptive. PLoS ONE 2012, 7, e46901. [Google Scholar] [CrossRef] [PubMed]
- Ehrström, S.; Daroczy, K.; Rylander, E.; Samuelsson, C.; Johannesson, U.; Anzén, B.; Påhlson, C. Lactic acid bacteria colonization and clinical outcome after probiotic supplementation in conventionally treated bacterial vaginosis and vulvovaginal candidiasis. Microbes Infect. 2010, 12, 691–699. [Google Scholar] [CrossRef] [PubMed]
- van der Veer, C.; Bruisten, S.M.; van Houdt, R.; Matser, A.A.; Tachedjian, G.; van de Wijgert, J.H.H.M.; de Vries, H.J.C.; van der Helm, J.J. Effects of an over-the-counter lactic-acid containing intra-vaginal douching product on the vaginal microbiota. BMC Microbiol. 2019, 19, 168. [Google Scholar] [CrossRef]
- Gottschick, C.; Deng, Z.L.; Vital, M.; Masur, C.; Abels, C.; Pieper, D.H.; Rohde, M.; Mendling, W.; Wagner-Döbler, I. Treatment of biofilms in bacterial vaginosis by an amphoteric tenside pessary-clinical study and microbiota analysis. Microbiome 2017, 5, 119. [Google Scholar] [CrossRef]
- Boeke, A.J.P.; Dekker, J.H.; Van Eijk, J.T.M.; Kostense, P.J.; Bezemer, P.D. Effect of lactic acid suppositories compared with oral metronidazole and placebo in bacterial vaginosis: A randomised clincial trial. Genitourin Med. 1993, 69, 388–392. [Google Scholar] [CrossRef][Green Version]
- Decena, D.C.D.; Co, J.T.; Manalastas, R.M.; Palaypayon, E.P.; Padolina, C.S.; Sison, J.M.; Dancel, L.A.; Lelis, M.A. Metronidazole with Lactacyd vaginal gel in bacterial vaginosis. J. Obstet. Gynaecol. Res. 2006, 32, 243–251. [Google Scholar] [CrossRef]
- Fredstorp, M.; Jonasson, A.F.; Barth, A.; Robertsson, J. A New Effective, User-friendly Bacterial Vaginosis Treatment: A Randomized Multicenter Open-label Parallel-group Two-part Study with a Novel Sustained-release Pessary Containing Oligomeric Lactic Acid. J. Infect. Non Infect. Dis. 2015, 1, 006. [Google Scholar]
- Simoes, J.A.; Bahamondes, L.G.; Camargo, R.P.S.; Alves, V.M.N.; Zaneveld, L.J.D.; Waller, D.P.; Schwartz, J.; Callahan, M.M.; Mauck, C.K. A pilot clinical trial comparing an acid-buffering formulation (ACIDFORM gel) with metronidazole gel for the treatment of symptomatic bacterial vaginosis. Br. J. Clin. Pharmacol. 2006, 61, 211–217. [Google Scholar] [CrossRef]
- Andersch, B.; Lindell, D.; Dahlen, I.; Brandberg, Å. Bacterial vaginosis and the effect of intermittent prophylactic treatment with an acid lactate gel. Gynecol. Obstet. Investig. 1990, 30, 114–119. [Google Scholar] [CrossRef]
- Holst, E.; Brandberg, Å. Treatment of bacterial vaginosis in pregnancy with a lactate gel. Scand. J. Infect. Dis. 1990, 22, 625–626. [Google Scholar] [CrossRef] [PubMed]
- Andersch, B.; Forssman, L.; Lincoln, K.; Torstensson, P. Treatment of bacterial vaginosis with an acid cream: A comparison between the effect of lactate-gel and metronidazole. Gynecol. Obstet. Investig. 1986, 21, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Mendling, W.; Martius, J.; Hoyme, U.B. S1-guideline on bacterial vaginosis in gynecology and obstetrics. Geburtshilfe Frauenheilkd. 2015, 74, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Muzny, C.A.; Schwebke, J.R. Asymptomatic Bacterial Vaginosis: To Treat or Not to Treat? Curr. Infect. Dis. Rep. 2020, 22, 32. [Google Scholar] [CrossRef] [PubMed]
- Crowley, T.; Low, N.; Turner, A.; Harvey, I.; Bidgood, K.; Horner, P. Antibiotic prophylaxis to prevent post-abortal upper genital tract infection in women with bacterial vaginosis: Randomised controlled trial. BJOG An. Int. J. Obstet. Gynaecol. 2001, 108, 396–402. [Google Scholar] [CrossRef]
- Larsson, P.G.; Carlsson, B. Does pre- and postoperative metronidazole treatment lower vaginal cuff infection rate after abdominal hysterectomy among women with bacterial vaginosis? Infect. Dis. Obstet. Gynecol. 2002, 10, 133–140. [Google Scholar] [CrossRef]
- Miller, L.; Thomas, K.; Hughes, J.P.; Holmes, K.K.; Stout, S.; Eschenbach, D.A. Randomised treatment trial of bacterial vaginosis to prevent post-abortion complication. BJOG Int. J. Obstet. Gynaecol. 2004, 111, 982–988. [Google Scholar] [CrossRef]
- Qian, Z.; Zhu, H.; Zhao, D.; Yang, P.; Gao, F.; Lu, C.; Yin, Y.; Kan, S.; Chen, D. Probiotic lactobacillus Sp. Strains inhibit growth, adhesion, biofilm formation, and gene expression of bacterial vaginosis-inducing Gardnerella vaginalis. Microorganisms 2021, 9, 728. [Google Scholar] [CrossRef]
- Mendling, W. Milchsäure und Milchsäurebakterien bei rezidivierenden Scheideninfektion. Frauenarzt 2010, 5, 453–466. [Google Scholar]
- Sobel, J.D.; Sobel, R. Current and emerging pharmacotherapy for recurrent bacterial vaginosis. Expert Opin. Pharmacother. 2021, 22, 1593–1600. [Google Scholar] [CrossRef]
- Turner, E.; Sobel, J.D.; Akins, R.A. Prognosis of recurrent bacterial vaginosis based on longitudinal changes in abundance of Lactobacillus and specific species of Gardnerella. PLoS ONE 2021, 16, e0256445. [Google Scholar] [CrossRef] [PubMed]
- Faught, B.M.; Reyes, S. Characterization and Treatment of Recurrent Bacterial Vaginosis. J. Women’s Health 2019, 28, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- Sobel, J.D.; Ferris, D.; Schwebke, J.; Nyirjesy, P.; Wiesenfeld, H.C.; Peipert, J.; Soper, D.; Ohmit, S.E.; Hillier, S.L. Suppressive antibacterial therapy with 0.75% metronidazole vaginal gel to prevent recurrent bacterial vaginosis. Am. J. Obstet. Gynecol. 2006, 194, 1283–1289. [Google Scholar] [CrossRef] [PubMed]
- Yudin, M.H.; Money, D.M.; Boucher, M.; Cormier, B.; Gruslin, A.; Ogilvie, G.; Paquet, C.; Steenbeek, A.; Van Eyk, N.; van Schalkwyk, J.; et al. Screening and Management of Bacterial Vaginosis in Pregnancy. J. Obstet. Gynaecol. Canada 2008, 30, 702–708. [Google Scholar] [CrossRef]
- Nyemba, D.C.; Haddison, E.C.; Wang, C.; Johnson, L.F.; Myer, L.; Davey, D.J. Prevalence of curable STIs and bacterial vaginosis during pregnancy in sub-Saharan Africa: A systematic review and meta-analysis. Sex. Transm. Infect. 2021, 2021, 055057. [Google Scholar] [CrossRef] [PubMed]
- Bonneton, M.; Huynh, B.T.; Seck, A.; Bercion, R.; Sarr, F.D.; Delarocque-Astagneau, E.; Vray, M. Bacterial vaginosis and other infections in pregnant women in Senegal. BMC Infect. Dis. 2021, 21, 1090. [Google Scholar] [CrossRef]
- Joyisa, N.; Moodley, D.; Nkosi, T.; Talakgale, R.; Sebitloane, M.; Naidoo, M.; Karim, Q.A. Asymptomatic bacterial vaginosis in pregnancy and missed opportunities for treatment: A cross-sectional observational study. Infect. Dis. Obstet. Gynecol. 2019, 2019, 7808179. [Google Scholar] [CrossRef]
- Hillier, S.L.; Nugent, R.P.; Eschenbach, D.A.; Krohn, M.A.; Gibbs, R.S.; Martin, D.H.; Cotch, M.F.; Edelman, R.; Pastorek, J.G.; Rao, A.V.; et al. Association between Bacterial Vaginosis and Preterm Delivery of a Low-Birth-Weight Infant. N. Engl. J. Med. 1995, 333, 1737–1742. [Google Scholar] [CrossRef]
- Tabatabaei, N.; Eren, A.M.; Barreiro, L.B.; Yotova, V.; Dumaine, A.; Allard, C.; Fraser, W.D. Vaginal microbiome in early pregnancy and subsequent risk of spontaneous preterm birth: A case–control study. BJOG Int. J. Obstet. Gynaecol. 2019, 126, 349–358. [Google Scholar] [CrossRef]
- Mullick, S.; Watson-Jones, D.; Beksinska, M.; Mabey, D. Sexually transmitted infections in pregnancy: Prevalence, impact on pregnancy outcomes, and approach to treatment in developing countries. Sex. Transm. Infect. 2005, 81, 294–302. [Google Scholar] [CrossRef]
- Leitich, H.; Kiss, H. Asymptomatic bacterial vaginosis and intermediate flora as risk factors for adverse pregnancy outcome. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 375–390. [Google Scholar] [CrossRef]
- Klebanoff, M.A.; Hillier, S.L.; Nugent, R.P.; MacPherson, C.A.; Hauth, J.C.; Carey, J.C.; Harper, M.; Wapner, R.J.; Trout, W.; Moawad, A. Is bacterial vaginosis a stronger risk factor for preterm birth when it is diagnosed earlier in gestation? Am. J. Obstet. Gynecol. 2005, 192, 470–477. [Google Scholar] [CrossRef]
- Guise, J.M.; Mahon, S.M.; Aickin, M.; Helfand, M.; Peipert, J.F.; Westhoff, C. Screening for bacterial vaginosis in pregnancy. Am. J. Prev. Med. 2001, 20, 62–72. [Google Scholar] [CrossRef]
- Bhakta, V.; Aslam, S.; Aljaghwani, A. Bacterial vaginosis in pregnancy: Prevalence and outcomes in a tertiary care hospital. Afr. J. Reprod. Health 2021, 25, 49–55. [Google Scholar] [PubMed]
- Subtil, D.; Brabant, G.; Tilloy, E.; Devos, P.; Canis, F.; Fruchart, A.; Bissinger, M.-C.; Dugimont, J.-C.; Nolf, C.; Hacot, C.; et al. Early clindamycin for bacterial vaginosis in pregnancy (PREMEVA): A multicentre, double-blind, randomised controlled trial. Lancet 2018, 392, 2171–2179. [Google Scholar] [CrossRef]
- Moodley, T.; Moodley, D.; Sebitloane, M.; Maharaj, N.; Sartorius, B. Improved pregnancy outcomes with increasing antiretroviral coverage in South Africa. BMC Pregnancy Childbirth 2016, 16, 35. [Google Scholar] [CrossRef]
- Moodley, D.; Sartorius, B.; Madurai, S.; Chetty, V.; Maman, S. Pregnancy Outcomes in Association with STDs including genital HSV-2 shedding in a South African Cohort Study. Sex. Transm. Infect. 2017, 93, 460–466. [Google Scholar] [CrossRef]
- Brocklehurst, P.; Gordon, A.; Heatley, E.; Milan, S.J. Antibiotics for treating bacterial vaginosis in pregnancy. Cochrane Database Syst. Rev. 2013, 2013, 1–96. [Google Scholar] [CrossRef]
- Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Donahue, K.; Doubeni, C.A.; Epling, J.W.; Kubik, M. Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery: US Preventive Services Task Force Recommendation Statement. JAMA J. Am. Med. Assoc. 2020, 323, 1286–1292. [Google Scholar]
- Carey, J.C.; Klebanoff, M.A.; Hauth, J.C.; Hillier, S.L.; Thom, E.A.; Ernest, J.M.; Heine, R.P.; Nugent, R.P.; Fischer, M.L.; Leveno, K.J. Metronidazole to Prevent Preterm Delivery in Pregnant Women with Asymptomatic Bacterial Vaginosis. N. Engl. J. Med. 2000, 342, 534–540. [Google Scholar] [CrossRef]
- Nygren, P.; Fu, R.; Freeman, M.; Bougatsos, C.; Klebanoff, M.; Guise, J.M. Evidence on the benefits and harms of screening and treating pregnant women who are asymptomatic for bacterial vaginosis: An update review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2008, 148, 220–233. [Google Scholar] [CrossRef]
- Hoyme, U.B.; Hesse, M. Reduced incidence of early preterm birth in the State of Thuringia following an intravaginal pH-self-monitoring screening program. Arch. Gynecol. Obstet. 2020, 302, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Lewis, A.L.; Laurent, L.C. USPSTF 2020 Recommendations on Screening for Asymptomatic Bacterial Vaginosis in Pregnancy. JAMA 2020, 323, 1253–1255. [Google Scholar] [CrossRef]
- Sobel, J.D.; Subramanian, C.; Foxman, B.; Fairfax, M.; Gygax, S.E. Mixed vaginitis—More than coinfection and with therapeutic implications. Curr. Infect. Dis. Rep. 2013, 15, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Qi, W.; Li, H.; Wang, C.; Li, H.; Zhang, B.; Dong, M.; Fan, A.; Han, C.; Xue, F. Recent Advances in Presentation, Diagnosis and Treatment for Mixed Vaginitis. Front. Cell. Infect. Microbiol. 2021, 11, 759795. [Google Scholar] [CrossRef]
- Benyas, D.; Sobel, J.D. Mixed Vaginitis Due to Bacterial Vaginosis and Candidiasis. J. Low Genit. Tract. Dis. 2022, 26, 68–70. [Google Scholar] [CrossRef]
- Sobel, J.D. Vulvovaginal candidosis. Lancet 2007, 369, 1961–1971. [Google Scholar] [CrossRef]
- Sustr, V.; Foessleitner, P.; Kiss, H.; Farr, A. Vulvovaginal candidosis: Current concepts, challenges and perspectives. J. Fungi 2020, 6, 267. [Google Scholar] [CrossRef]
- Denning, D.W.; Kneale, M.; Sobel, J.D.; Rautemaa-Richardson, R. Global burden of recurrent vulvovaginal candidiasis: A systematic review. Lancet Infect. Dis. 2018, 18, e339–e347. [Google Scholar] [CrossRef]
- Mendling, W.; El Shazly, M.A.; Zhang, L. Clotrimazole for vulvovaginal candidosis: More than 45 years of clinical experience. Pharmaceuticals 2020, 13, 274. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.; Bellen, G.; Ausma, J.; Verguts, L.; Vaneldere, J.; Hinoul, P.; Borgers, M.; Janssens, D. The effect of antifungal treatment on the vaginal flora of women with vulvo-vaginal yeast infection with or without bacterial vaginosis. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Rivers, C.A.; Adaramola, O.O.; Schwebke, J.R. Prevalence of bacterial vaginosis and vulvovaginal candidiasis mixed infection in a southeastern American STD clinic. Sex. Transm. Dis. 2011, 38, 672–674. [Google Scholar] [CrossRef] [PubMed]
- Edwards, T.; Burke, P.; Smalley, H.; Hobbs, G. Trichomonas vaginalis: Clinical relevance, pathogenicity and diagnosis. Crit. Rev. Microbiol. 2016, 42, 406–417. [Google Scholar] [CrossRef]
- Elkins, J.M.; Cantillo-Campos, S.; Sheele, J.M. Frequency of Coinfection on the Vaginal Wet Preparation in the Emergency Department. Cureus 2020, 12, e11566. [Google Scholar] [CrossRef]
- Franklin, T.L.; Monif, G.R.G. Trichomonas vaginalis and bacterial vaginosis: Coexistence in vaginal wet mount preparations from pregnant women. J. Reprod. Med. Obstet. Gynecol. 2000, 45, 131–134. [Google Scholar]
- Kim, J.-M.; Park, Y.J. Probiotics in the Prevention and Treatment of Postmenopausal Vaginal Infections: Review Article. J. Menopausal. Med. 2017, 23, 139. [Google Scholar] [CrossRef]
- Borges, S.; Silva, J.; Teixeira, P. The role of lactobacilli and probiotics in maintaining vaginal health. Arch. Gynecol. Obstet. 2014, 289, 479–489. [Google Scholar] [CrossRef]
- Jones, C.P.; Carter, B.; Thomas, W.L. The treatment of resistant or recurrent vaginal trichomoniasis with lactic acid jelly and lactic acid douches. Gynecol. Obstet. Investig. 1960, 149, 128–138. [Google Scholar] [CrossRef]
- Mendling, W.; Plempel, M. Vaginal secretion levels after 6 days, 3 days and 1 day of treatment with 100, 200 and 500 mg vaginal tablets of clotrimazole and their therapeutic efficacy. Chemotherapy 1982, 28, 43–47. [Google Scholar] [CrossRef]
- Li, T.; Liu, Z.; Zhang, Z.; Bai, H.; Zong, X.; Wang, F.; Fan, L. Comparative analysis of the vaginal microbiome of Chinese women with Trichomonas vaginalis and mixed infection. Microb. Pathog. 2021, 154, 104790. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Barreno, A.; Cabezas-Mera, F.; Tejera, E.; Machado, A. Comparative Effectiveness of Treatments for Bacterial Vaginosis: A Network Meta-Analysis. Antibiotics 2021, 10, 978. [Google Scholar] [CrossRef] [PubMed]
- Armstrong-Buisseret, L.; Brittain, C.; Kai, J.; David, M.; Watkins, J.A.; Ozolins, M.; Jackson, L.; Abdali, Z.; Hepburn, T.; Griffiths, F.; et al. Lactic acid gel versus metronidazole for recurrent bacterial vaginosis in women aged 16 years and over: The VITA RCT. Health Technol. Assess. 2022, 26, 1–170. [Google Scholar] [CrossRef]
- Plummer, E.; Bradshaw, C.; Doyle, M.; Fairley, C.; Murray, G.; Bateson, D.; Masson, L.; Slifirski, J.; Tachedjian, G.; Vodstrcil, L. Lactic acid-containing products for bacterial vaginosis and their impact on the vaginal microbiota: A systematic review. PLoS ONE 2021, 16, e0246953. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Ref | Author | Year | Population | Design | Diagnosis | Drug and Formulation | Comparator | Outcomes |
|---|---|---|---|---|---|---|---|---|
| [68] | Boeke | 1993 | Symptomatic BV | RCT a |
| Lactic acid vaginal suppository/night × 7 days |
| ≤2 of 4 Amsel criteria
|
| [69] | Decena | 2006 | Symptomatic BV | RCT |
| Vaginal lactal gel 5 g/night × 7 nights |
|
|
| [70] | Fredstorp | 2015 | Symptomatic BV | RCT |
| Oligomeric lactic acid pessary once or twice a week |
|
|
| [71] | Simoes | 2006 | Symptomatic BV | RCT, db |
| Vaginal Acidform gel 5 g/day × 5 days |
|
|
| [72] | Andersch | 1990 | Recurrent BV | RCT, db |
| Initial treatment with vaginal lactate gel 5 mL/night × 7 nights + prophylactic treatment for 6 months with 5 mL vaginal lactate gel/night × 3 nights immediately after menstruation |
|
|
| [73] | Holst | 1990 | Pregnant with symptomatic BV | ND |
| Vaginal lactal gel 5 mL/night × 7 nights + 4 treatments for 2 days with an interim period of 7 days or 5 treatments for 2 days with an interim period of 5 days |
|
|
| [74] | Andersch | 1986 | Symptomatic BV | RCT, db |
| Vaginal lactal gel 5 mL/night × 7 nights |
|
|
| Patient Group | Lactic Acid | Antibiotics | Antifungal | |
|---|---|---|---|---|
| First time BV | Mild BV | Vaginal lactic acid, 5 mL, 7 days | No | No |
| Moderate/Severe BV | Vaginal lactic acid, 5 mL, 7 days | Oral metronidazole, 7 days, or Vaginal metronidazole or clindamycin, 5–7 days | No | |
| Recurrent BV | Vaginal lactic acid, 5 mL, 7 days | Vaginal metronidazole, 4–6 months, or Oral metronidazole or tinidazole, 7 days | No | |
| Pregnant with BV | Symptomatic | Vaginal lactic acid, 5 mL, 7 days | Oral metronidazole or clindamycin, 7 days, or Vaginal dequalinium, metronidazole, or clindamycin | No |
| Asymptomatic and at high risk of preterm birth | Vaginal lactic acid, 5 mL, 7 days | No | No | |
| Planning pregnancy | Asymptomatic mild BV | Vaginal lactic acid, 5 mL, 7 days | No | No |
| Mixed infection | BV and VVC | Vaginal lactic acid, 5 mL, 7 days, only if BV symptoms persist after VVC treatment | Only if BV symptoms persist after VVC treatment, and depending on the patient group | Vaginal clotrimazole, single dose |
| BV and trichomoniasis | Vaginal lactic acid, 5 mL, 7 days | Oral metronidazole or tinidazole, single dose | No | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendling, W.; Shazly, M.A.E.; Zhang, L. The Role of Lactic Acid in the Management of Bacterial Vaginosis: A Systematic Literature Review. Future Pharmacol. 2022, 2, 198-213. https://doi.org/10.3390/futurepharmacol2030014
Mendling W, Shazly MAE, Zhang L. The Role of Lactic Acid in the Management of Bacterial Vaginosis: A Systematic Literature Review. Future Pharmacology. 2022; 2(3):198-213. https://doi.org/10.3390/futurepharmacol2030014
Chicago/Turabian StyleMendling, Werner, Maged Atef El Shazly, and Lei Zhang. 2022. "The Role of Lactic Acid in the Management of Bacterial Vaginosis: A Systematic Literature Review" Future Pharmacology 2, no. 3: 198-213. https://doi.org/10.3390/futurepharmacol2030014
APA StyleMendling, W., Shazly, M. A. E., & Zhang, L. (2022). The Role of Lactic Acid in the Management of Bacterial Vaginosis: A Systematic Literature Review. Future Pharmacology, 2(3), 198-213. https://doi.org/10.3390/futurepharmacol2030014