
A Multi-Well Method for the CD138 and AML/MDS FISH Testing of Multiple Biomarkers on a Single Slide in Multiple Myeloma and AML/MDS Patients

 , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
2.1. The Patient Cohort in This Study
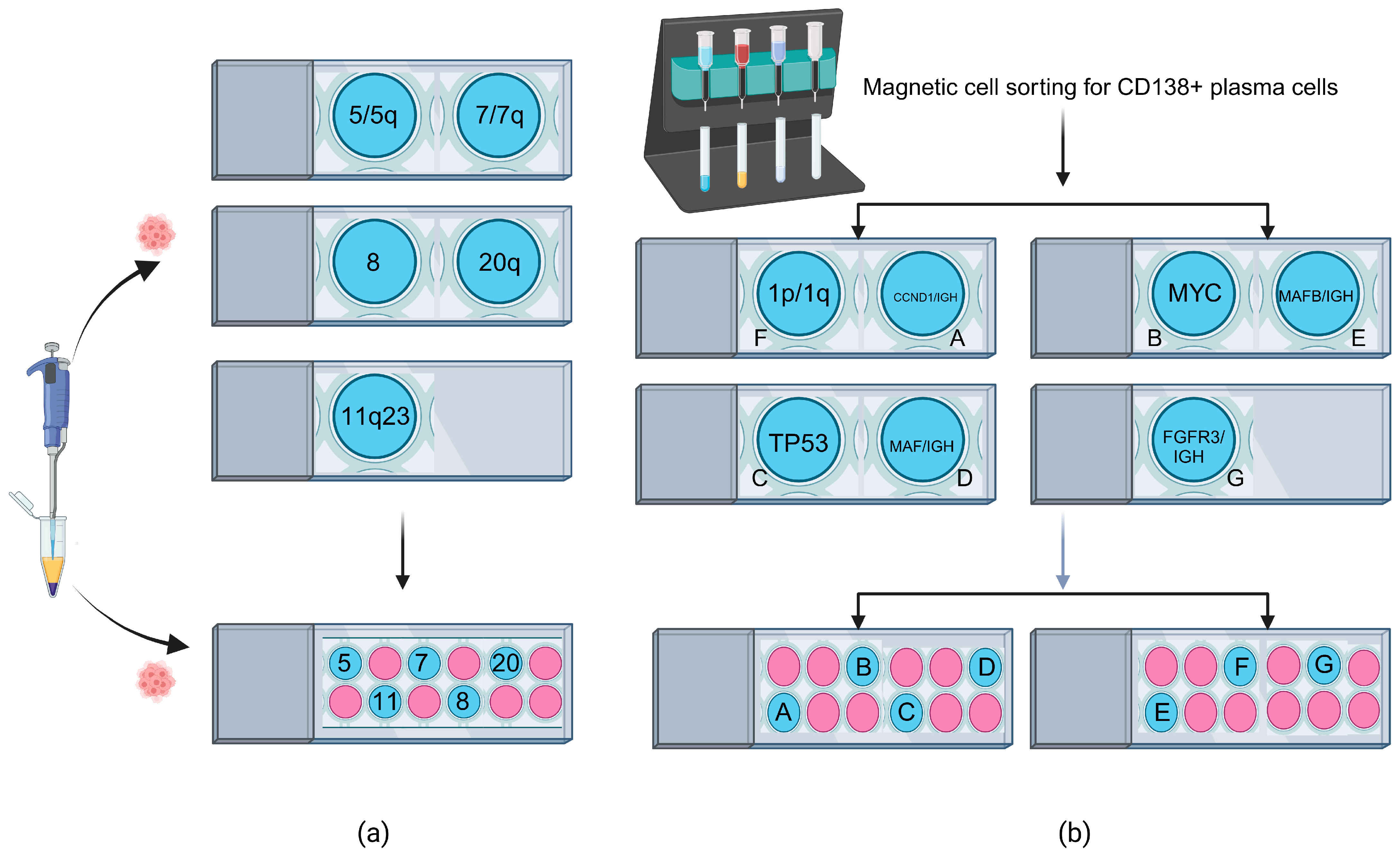
2.2. AML/MDS FISH Testing on Multi-Well Slides
2.3. CD138 MM FISH Testing on Multi-Well Slides
2.4. Statistical Calculations
3. Results
3.1. AML/MDS FISH Testing on Multi-Well Slides
3.2. CD138 MM FISH Testing on Multi-Well Slides
4. Discussion
4.1. Advantages of Performing FISH on Multi-Well Slides for Leukemia Patients
4.1.1. Enhanced Cell Concentration and Technologist Time Savings
4.1.2. Reduced Probe Volume (Cost Savings) and Optimized Resource Utilization
4.2. Potential Pitfalls of Performing FISH on Multi-Well Slides and Future Improvements
4.2.1. Potential for Cross-Contamination
4.2.2. Learning Curve, Limited Well Size, and Cell Capacity
4.3. The Adoption of FISH on Multi-Well Slides in a Clinical Diagnostic Setting
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AML | Acute myeloid leukemia |
| CD38+ | CD38 enrichment |
| CNV | Copy number variant |
| del | Deletion |
| FISH | Fluorescence in situ hybridization |
| MDS | Myelodysplastic syndrome |
| MM | Multiple myeloma |
| SV | Structural variant |
| t | Translocation |
References
- Abdallah, N.H.; Binder, M.; Rajkumar, S.V.; Greipp, P.T.; Kapoor, P.; Dispenzieri, A.; Gertz, M.A.; Baughn, L.B.; Lacy, M.Q.; Hayman, S.R.; et al. A simple additive staging system for newly diagnosed multiple myeloma. Blood Cancer J. 2022, 12, 21. [Google Scholar] [CrossRef] [PubMed]
- Cardona-Benavides, I.J.; de Ramon, C.; Gutierrez, N.C. Genetic Abnormalities in Multiple Myeloma: Prognostic and Therapeutic Implications. Cells 2021, 10, 336. [Google Scholar] [CrossRef]
- Clarke, S.E.; Fuller, K.A.; Erber, W.N. Chromosomal defects in multiple myeloma. Blood Rev. 2024, 64, 101168. [Google Scholar] [CrossRef]
- Rajkumar, S.V. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am. J. Hematol. 2022, 97, 1086–1107. [Google Scholar] [CrossRef] [PubMed]
- Zou, Y.S.; Klausner, M.; Ghabrial, J.; Stinnett, V.; Long, P.; Morsberger, L.; Murry, J.B.; Beierl, K.; Gocke, C.D.; Xian, R.R.; et al. A comprehensive approach to evaluate genetic abnormalities in multiple myeloma using optical genome mapping. Blood Cancer J. 2024, 14, 78. [Google Scholar] [CrossRef]
- Saxe, D.; Seo, E.J.; Bergeron, M.B.; Han, J.Y. Recent advances in cytogenetic characterization of multiple myeloma. Int. J. Lab. Hematol. 2019, 41, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Rustad, E.H.; Yellapantula, V.D.; Glodzik, D.; Maclachlan, K.H.; Diamond, B.; Boyle, E.M.; Ashby, C.; Blaney, P.; Gundem, G.; Hultcrantz, M.; et al. Revealing the impact of structural variants in multiple myeloma. Blood Cancer Discov. 2020, 1, 258–273. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.P.; Borowitz, M.J.; Calvo, K.R.; Kvasnicka, H.M.; Wang, S.A.; Bagg, A.; Barbui, T.; Branford, S.; et al. International Consensus Classification of Myeloid Neoplasms and Acute Leukemias: Integrating morphologic, clinical, and genomic data. Blood 2022, 140, 1200–1228. [Google Scholar] [CrossRef]
- Garcia-Manero, G. Myelodysplastic syndromes: 2023 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2023, 98, 1307–1325. [Google Scholar] [CrossRef]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef]
- Jiang, L.; Pallavajjala, A.; Huang, J.; Haley, L.; Morsberger, L.; Stinnett, V.; Hardy, M.; Park, R.; Ament, C.; Finch, A.; et al. Clinical Utility of Targeted Next-Generation Sequencing Assay to Detect Copy Number Variants Associated with Myelodysplastic Syndrome in Myeloid Malignancies. J. Mol. Diagn. 2021, 23, 467–483. [Google Scholar] [CrossRef]
- Halper-Stromberg, E.; Stinnett, V.; Morsberger, L.; Pallavajjala, A.; Levis, M.J.; DeZern, A.E.; Lei, M.; Phan, B.; Xian, R.R.; Gocke, C.D.; et al. 1q jumping translocation as a biomarker in myeloid malignancy: Frequently mutated genes associated with bad prognosis and low survival. Exp. Hematol. Oncol. 2024, 13, 73. [Google Scholar] [CrossRef] [PubMed]
- Boyd, R.J.; Murry, J.B.; Morsberger, L.A.; Klausner, M.; Chen, S.; Gocke, C.D.; McCallion, A.S.; Zou, Y.S. Ring Chromosomes in Hematological Malignancies Are Associated with TP53 Gene Mutations and Characteristic Copy Number Variants. Cancers 2023, 15, 5439. [Google Scholar] [CrossRef]
- Snaith, O.; Poveda-Rogers, C.; Laczko, D.; Yang, G.; Morrissette, J.J.D. Cytogenetics and genomics of acute myeloid leukemia. Best Pract. Res. Clin. Haematol. 2024, 37, 101533. [Google Scholar] [CrossRef]
- Palumbo, A.; Anderson, K. Multiple myeloma. N. Engl. J. Med. 2011, 364, 1046–1060. [Google Scholar] [CrossRef] [PubMed]
- Cowan, A.J.; Green, D.J.; Kwok, M.; Lee, S.; Coffey, D.G.; Holmberg, L.A.; Tuazon, S.; Gopal, A.K.; Libby, E.N. Diagnosis and Management of Multiple Myeloma: A Review. JAMA 2022, 327, 464–477. [Google Scholar] [CrossRef]
- Palumbo, A.; Avet-Loiseau, H.; Oliva, S.; Lokhorst, H.M.; Goldschmidt, H.; Rosinol, L.; Richardson, P.; Caltagirone, S.; Lahuerta, J.J.; Facon, T.; et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J. Clin. Oncol. 2015, 33, 2863–2869. [Google Scholar] [CrossRef]
- D’Agostino, M.; Cairns, D.A.; Lahuerta, J.J.; Wester, R.; Bertsch, U.; Waage, A.; Zamagni, E.; Mateos, M.V.; Dall’Olio, D.; van de Donk, N.; et al. Second Revision of the International Staging System (R2-ISS) for Overall Survival in Multiple Myeloma: A European Myeloma Network (EMN) Report Within the HARMONY Project. J. Clin. Oncol. 2022, 40, 3406–3418. [Google Scholar] [CrossRef] [PubMed]
- Venugopal, S.; Mascarenhas, J.; Steensma, D.P. Loss of 5q in myeloid malignancies—A gain in understanding of biological and clinical consequences. Blood Rev. 2021, 46, 100735. [Google Scholar] [CrossRef]
- Mori, M.; Kubota, Y.; Durmaz, A.; Gurnari, C.; Goodings, C.; Adema, V.; Ponvilawan, B.; Bahaj, W.S.; Kewan, T.; LaFramboise, T.; et al. Genomics of deletion 7 and 7q in myeloid neoplasm: From pathogenic culprits to potential synthetic lethal therapeutic targets. Leukemia 2023, 37, 2082–2093. [Google Scholar] [CrossRef]
- Hemsing, A.L.; Hovland, R.; Tsykunova, G.; Reikvam, H. Trisomy 8 in acute myeloid leukemia. Expert. Rev. Hematol. 2019, 12, 947–958. [Google Scholar] [CrossRef]
- Hernandez-Sanchez, A.; Gonzalez, T.; Sobas, M.; Strang, E.; Castellani, G.; Abaigar, M.; Valk, P.J.M.; Villaverde Ramiro, A.; Benner, A.; Metzeler, K.H.; et al. Rearrangements involving 11q23.3/KMT2A in adult AML: Mutational landscape and prognostic implications—A HARMONY study. Leukemia 2024, 38, 1929–1937. [Google Scholar] [CrossRef]
- Kokate, P.; Dalvi, R.; Koppaka, N.; Mandava, S. Prognostic classification of MDS is improved by the inclusion of FISH panel testing with conventional cytogenetics. Cancer Genet. 2017, 216–217, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Lu, G.; Muddasani, R.; Orlowski, R.Z.; Abruzzo, L.V.; Qazilbash, M.H.; You, M.J.; Wang, Y.; Zhao, M.; Chen, S.; Glitza, I.C.; et al. Plasma cell enrichment enhances detection of high-risk cytogenomic abnormalities by fluorescence in situ hybridization and improves risk stratification of patients with plasma cell neoplasms. Arch. Pathol. Lab. Med. 2013, 137, 625–631. [Google Scholar] [CrossRef]
- Ross, F.M.; Avet-Loiseau, H.; Ameye, G.; Gutierrez, N.C.; Liebisch, P.; O’Connor, S.; Dalva, K.; Fabris, S.; Testi, A.M.; Jarosova, M.; et al. Report from the European Myeloma Network on interphase FISH in multiple myeloma and related disorders. Haematologica 2012, 97, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, L.; Biggerstaff, J.S.; Chapman, D.B.; Scott, J.M.; Johnson, K.R.; Ghirardelli, K.M.; Fritschle, W.K.; Martinez, D.L.; Bennington, R.K.; de Baca, M.E.; et al. Detection of genomic abnormalities in multiple myeloma: The application of FISH analysis in combination with various plasma cell enrichment techniques. Am. J. Clin. Pathol. 2011, 136, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Panakkal, V.; Rana, S.; Rathore, S.; Anshu, A.; Balakrishnan, A.; Singh, C.; Jandial, A.; Sachdeva, M.U.S.; Varma, N.; Lad, D.; et al. The success rate of interphase fluorescence in situ hybridization in plasma cell disorders can be improved using unconventional sources of plasma cells. Int. J. Lab. Hematol. 2022, 44, 157–162. [Google Scholar] [CrossRef]
- Gagnon, M.F.; Midthun, S.M.; Fangel, J.A.; Schuh, C.M.; Luoma, I.M.; Pearce, K.E.; Meyer, R.G.; Ailawadhi, S.; Arribas, M.J.; Braggio, E.; et al. Superior detection rate of plasma cell FISH using FACS-FISH. Am. J. Clin. Pathol. 2024, 161, 60–70. [Google Scholar] [CrossRef]
- Ha, J.; Cho, H.; Lee, T.G.; Shin, S.; Chung, H.; Jang, J.E.; Kim, S.J.; Cheong, J.W.; Lee, S.T.; Kim, J.S.; et al. Cytogenetic testing by fluorescence in situ hybridization is improved by plasma cell sorting in multiple myeloma. Sci. Rep. 2022, 12, 8287. [Google Scholar] [CrossRef]
- Christensen, T.; Deng, W.; McMahill, B.; Schappert, J.; Liu, W.; Saleki, R.; Zou, Y.S. Utilization of magnetic-activated cell sorting and high-density single nucleotide polymorphism microarrays improves diagnostic yield and prognostic value in clinical testing for patients with multiple myeloma and normal routine chromosome study. Acta Haematol. 2014, 132, 233–236. [Google Scholar] [CrossRef]
- Smith, D.; Stephenson, C.; Percy, L.; Lach, A.; Chatters, S.; Kempski, H.; Yong, K. Cohort analysis of FISH testing of CD138(+) cells in relapsed multiple myeloma: Implications for prognosis and choice of therapy. Br. J. Haematol. 2015, 171, 881–883. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board (Ed.) Haematolymphoid Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2024; Volume 11, Available online: https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours/Haematolymphoid-Tumours-2024 (accessed on 23 April 2025).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specimen Types | # AML/MDS Cases (FISH Probes) | # MM Cases (FISH Probes) |
|---|---|---|
| Peripheral Blood | 23 (115) | 0 (0) |
| Bone Marrow | 106 (530) | 53 (371) |
| Total | 129 (645) | 53 (371) |
| AML/MDS FISH Panel | MM FISH Panel |
|---|---|
| 5p15.2/5q31 (EGR1) | 1p32 (CDKN2C)/1q21 (CKS1B) |
| 7cen/7q31 | MYC break-apart probe |
| 8cen | 17p13 (TP53)/17cen |
| KMT2A break-apart probe | IGH::FGFR3 dual fusion |
| 20q12/20q13.12 | IGH::CCND1 dual fusion |
| IGH::MAF dual fusion | |
| IGH::MAFB dual fusion |
| Results | Karyotyping | FISH Results | |||||
|---|---|---|---|---|---|---|---|
| 5q−/−5 | 7q−/−7 | +8 | 20q− | KMT2A Gene Rearrangement | Others * | ||
| Normal | 104 | 121 | 119 | 123 | 121 | 127 | 122 |
| Abnormal | 25 ** | 8 | 10 | 6 | 8 | 2 | 7 |
| Results | FISH Results | |||||||
|---|---|---|---|---|---|---|---|---|
| 1p (Loss) | 1q (Gain) | MYC Gene Rearrangement | TP53 (Loss) | IGH:: CCND1 Fusion | IGH::FGFR3/ NSD2 Fusion | IGH::MAF Fusion | IGH:: MAFB Fusion | |
| Normal | 51 | 42 | 51 | 49 | 46 | 48 | 52 | 51 |
| Abnormal | 2 | 11 | 2 | 4 | 7 | 5 | 1 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tambini, F.; Klausner, M.; Stinnett, V.; Ghabrial, J.; Nozari, A.; Middlezong, W.; Phan, B.; Phan, M.; Morsberger, L.; Long, P.; et al. A Multi-Well Method for the CD138 and AML/MDS FISH Testing of Multiple Biomarkers on a Single Slide in Multiple Myeloma and AML/MDS Patients. DNA 2025, 5, 31. https://doi.org/10.3390/dna5020031
Tambini F, Klausner M, Stinnett V, Ghabrial J, Nozari A, Middlezong W, Phan B, Phan M, Morsberger L, Long P, et al. A Multi-Well Method for the CD138 and AML/MDS FISH Testing of Multiple Biomarkers on a Single Slide in Multiple Myeloma and AML/MDS Patients. DNA. 2025; 5(2):31. https://doi.org/10.3390/dna5020031
Chicago/Turabian StyleTambini, Frank, Melanie Klausner, Victoria Stinnett, Jen Ghabrial, Azin Nozari, William Middlezong, Brian Phan, Micheal Phan, Laura Morsberger, Patty Long, and et al. 2025. "A Multi-Well Method for the CD138 and AML/MDS FISH Testing of Multiple Biomarkers on a Single Slide in Multiple Myeloma and AML/MDS Patients" DNA 5, no. 2: 31. https://doi.org/10.3390/dna5020031
APA StyleTambini, F., Klausner, M., Stinnett, V., Ghabrial, J., Nozari, A., Middlezong, W., Phan, B., Phan, M., Morsberger, L., Long, P., & Zou, Y. S. (2025). A Multi-Well Method for the CD138 and AML/MDS FISH Testing of Multiple Biomarkers on a Single Slide in Multiple Myeloma and AML/MDS Patients. DNA, 5(2), 31. https://doi.org/10.3390/dna5020031