


Forecasting COVID-19 Cases, Hospital Admissions, and Deaths Based on Wastewater SARS-CoV-2 Surveillance Using Gaussian Copula Time Series Marginal Regression Model


 ,
, 
Abstract
1. Introduction
2. Methods
2.1. Wastewater SARS-CoV-2 Analyses
2.2. Clinical Data Source
2.3. Statistical Analysis
2.4. Copula-Based Time Series Modeling
3. Results
3.1. Relationships Among Wastewater SARS-CoV-2 Viral Load and Clinical Data
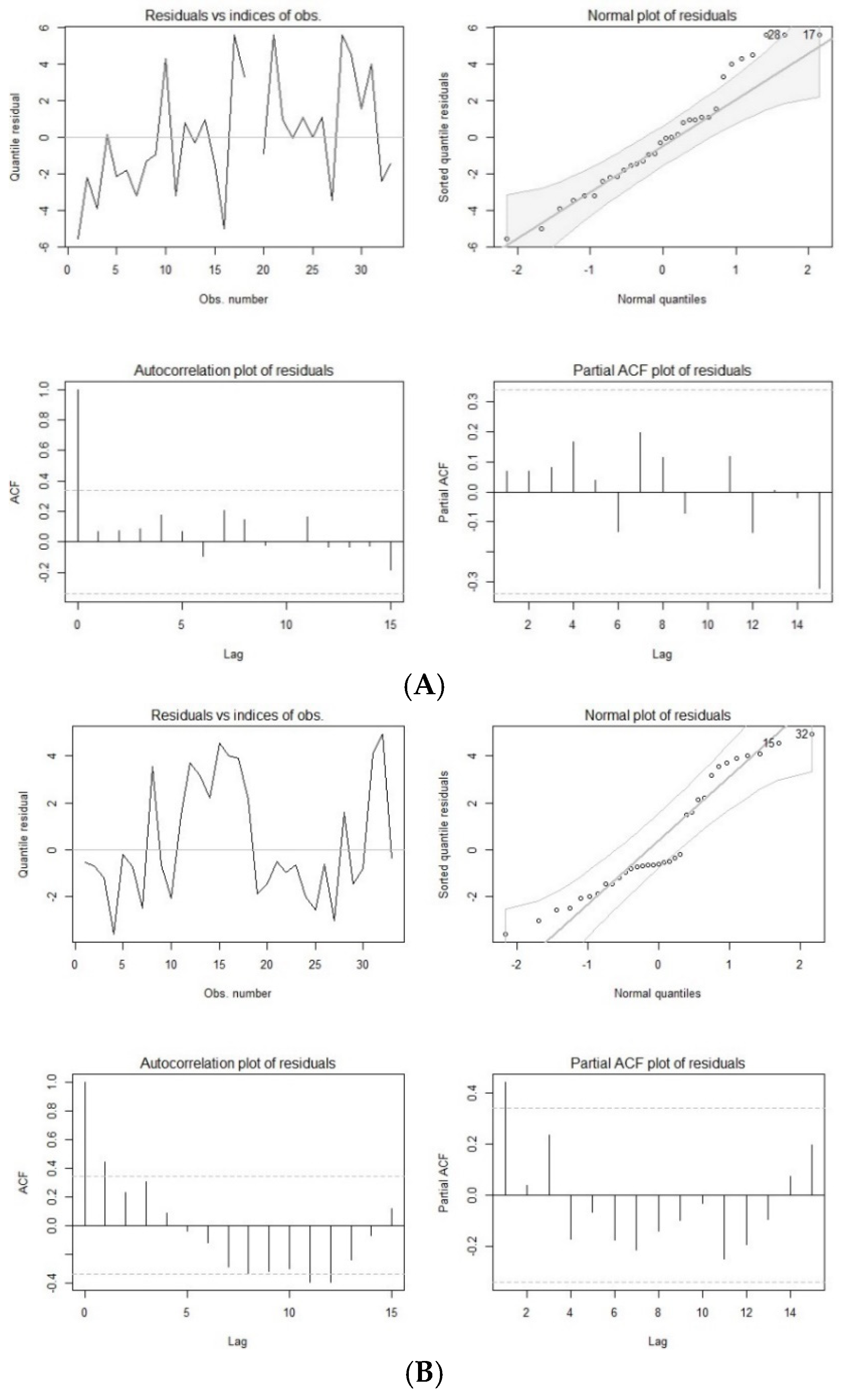
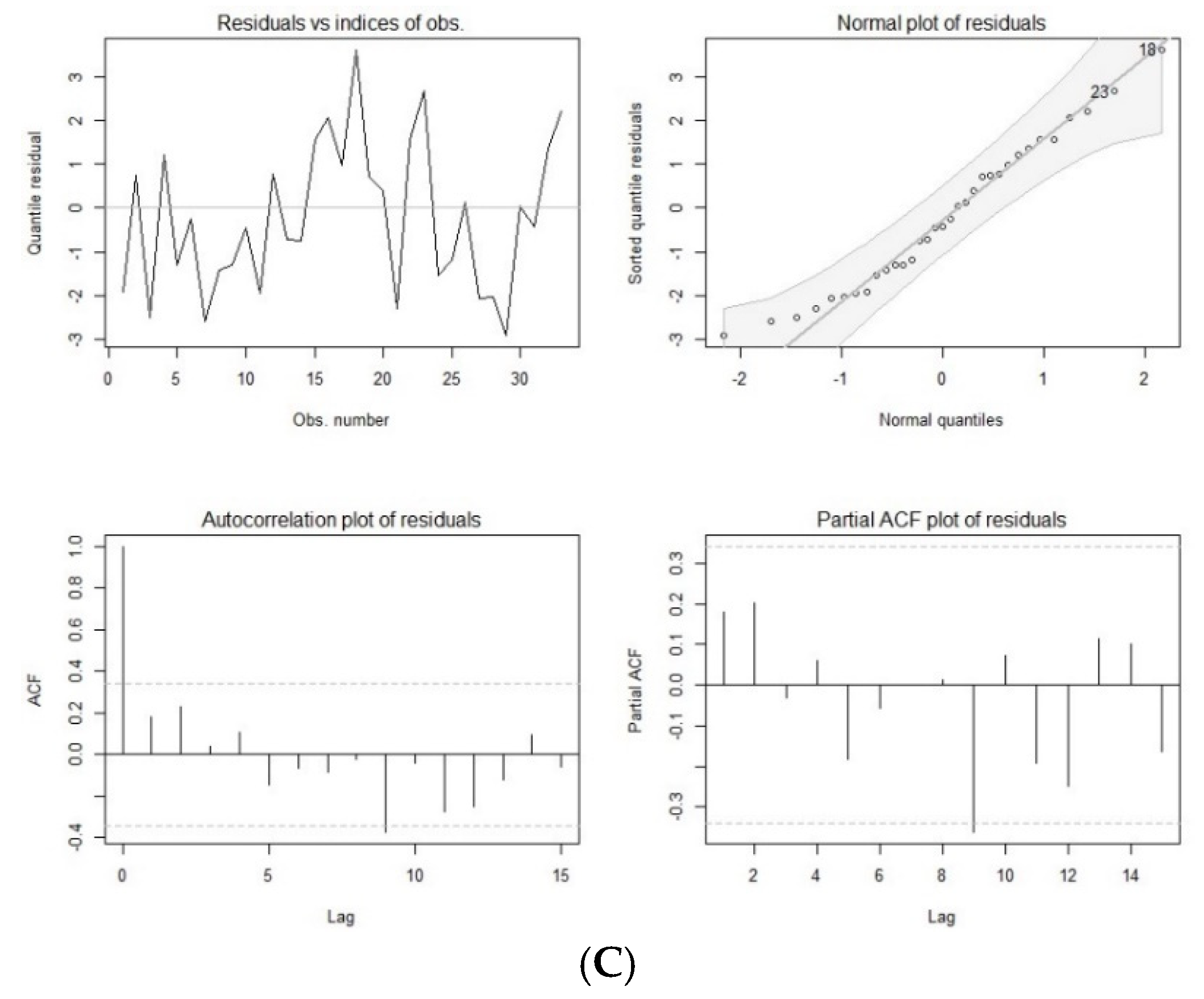
3.2. ARMA Time Series Analysis
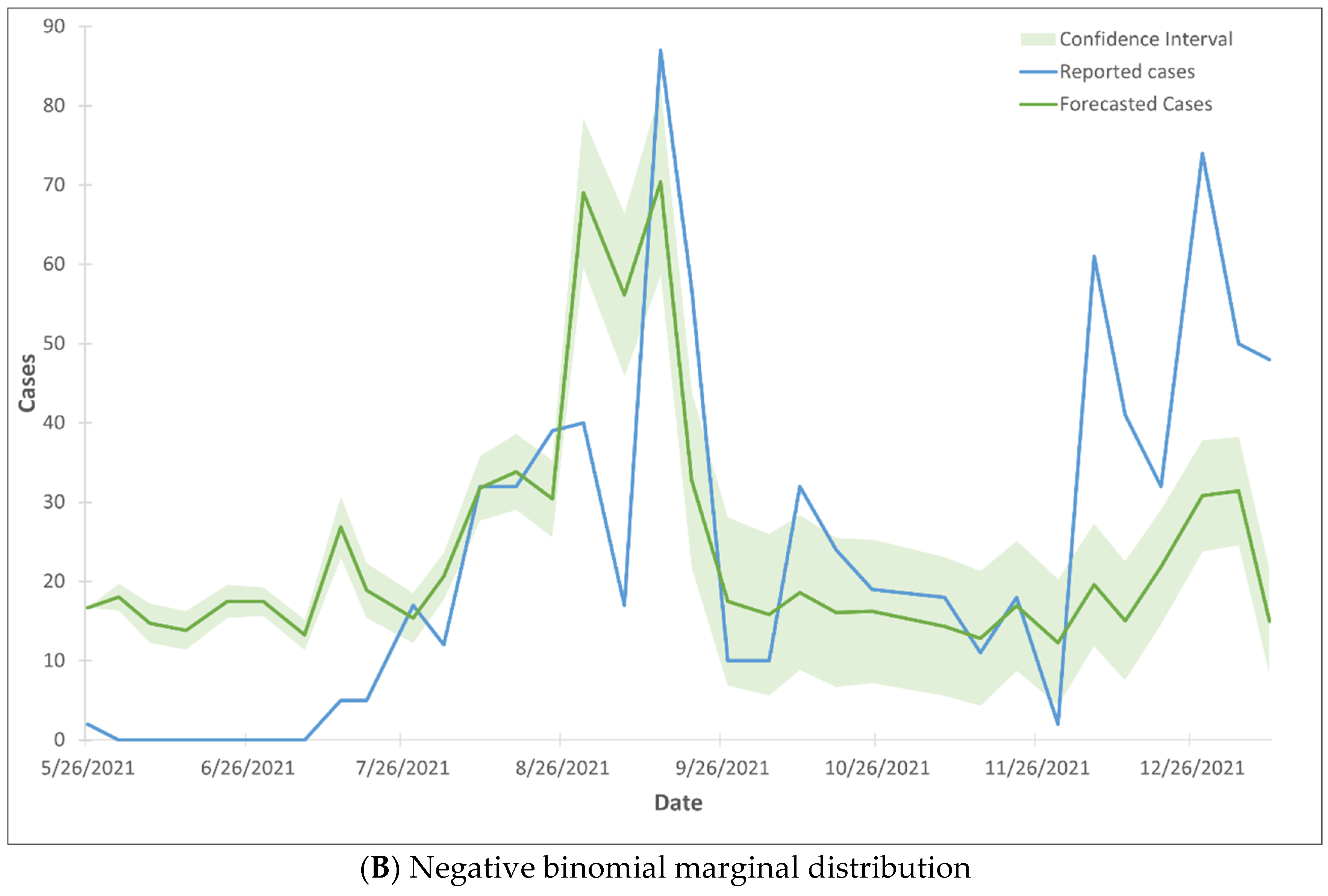
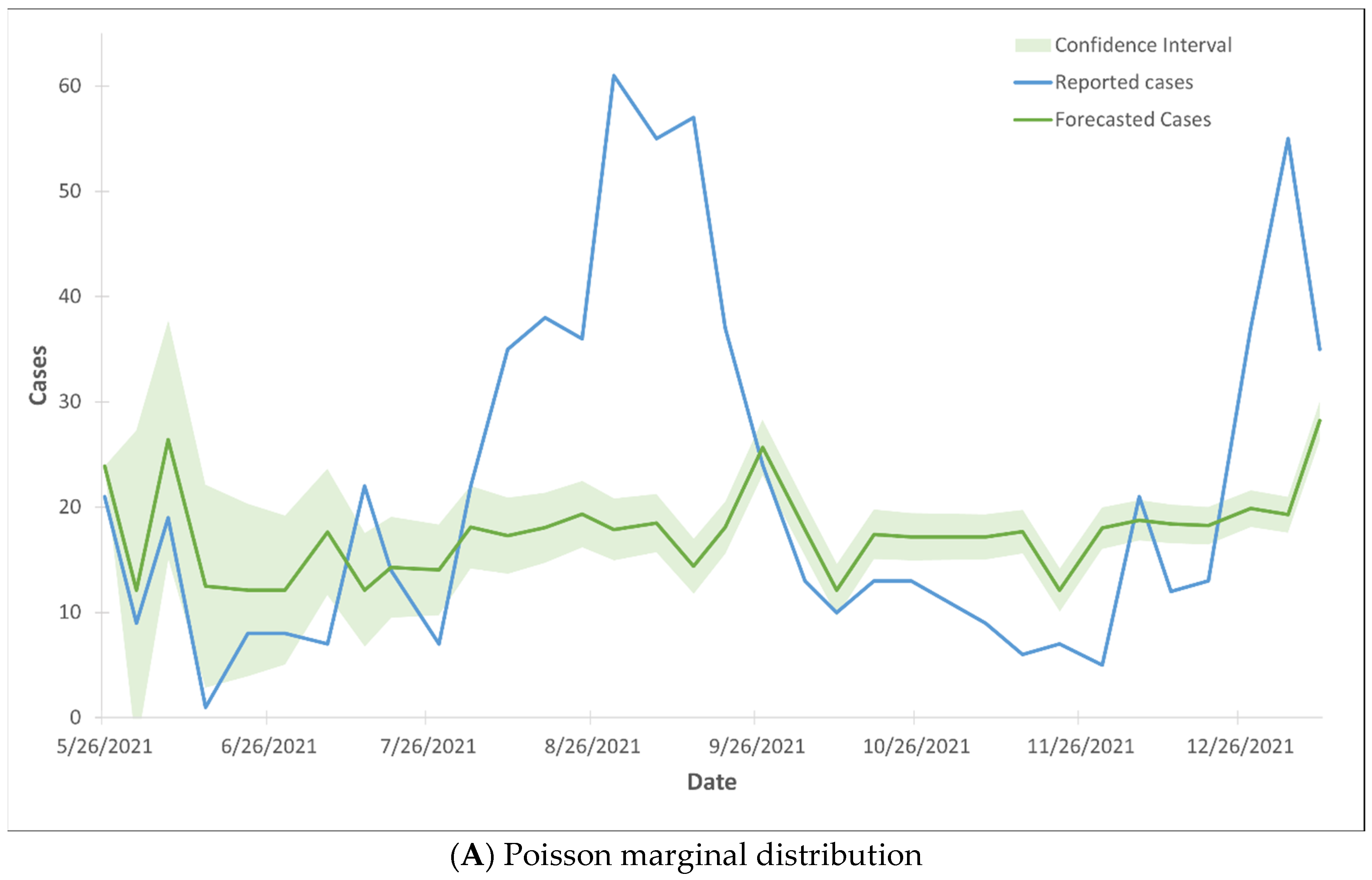
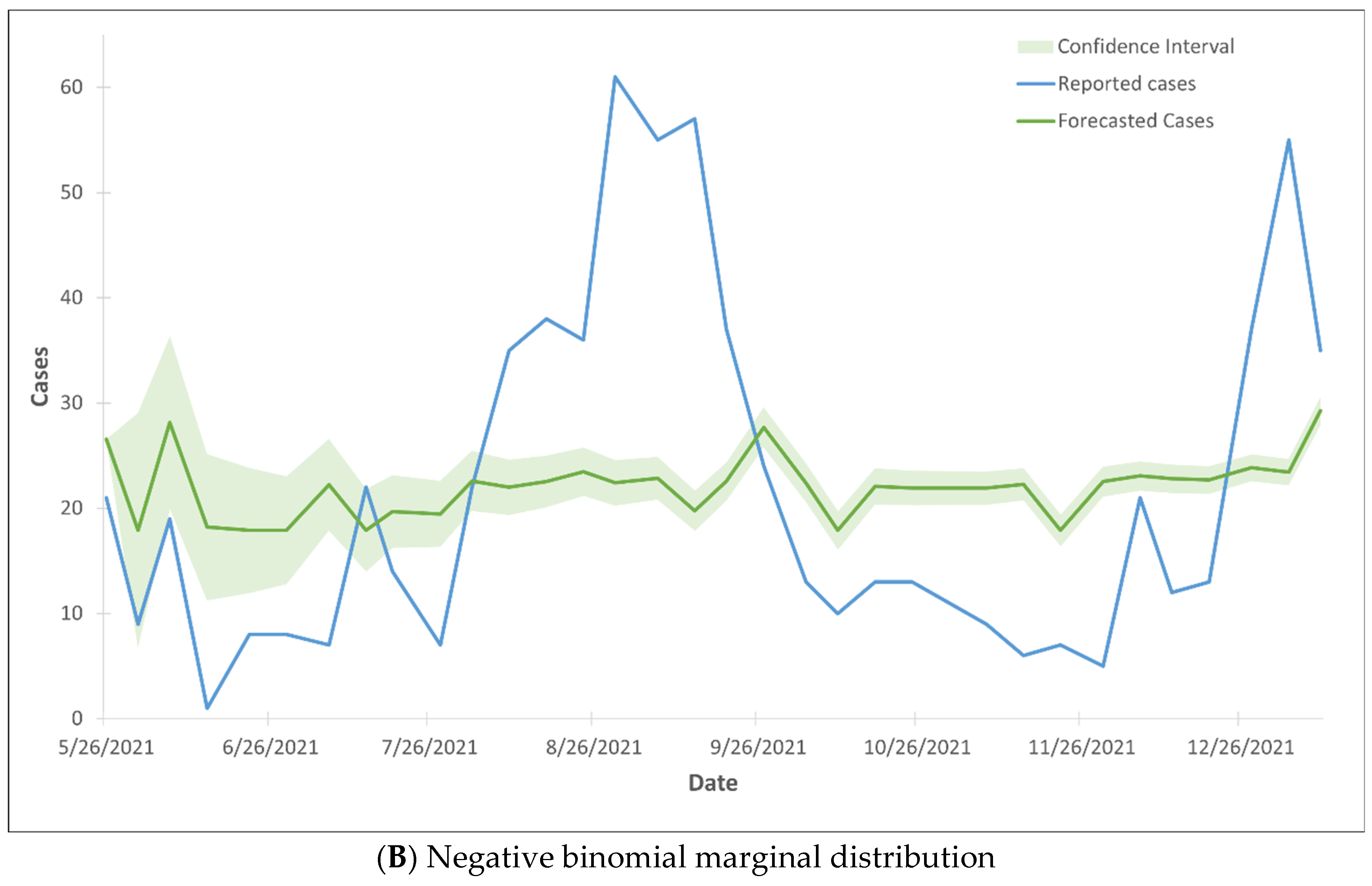
3.3. Modeling COVID-19 Cases
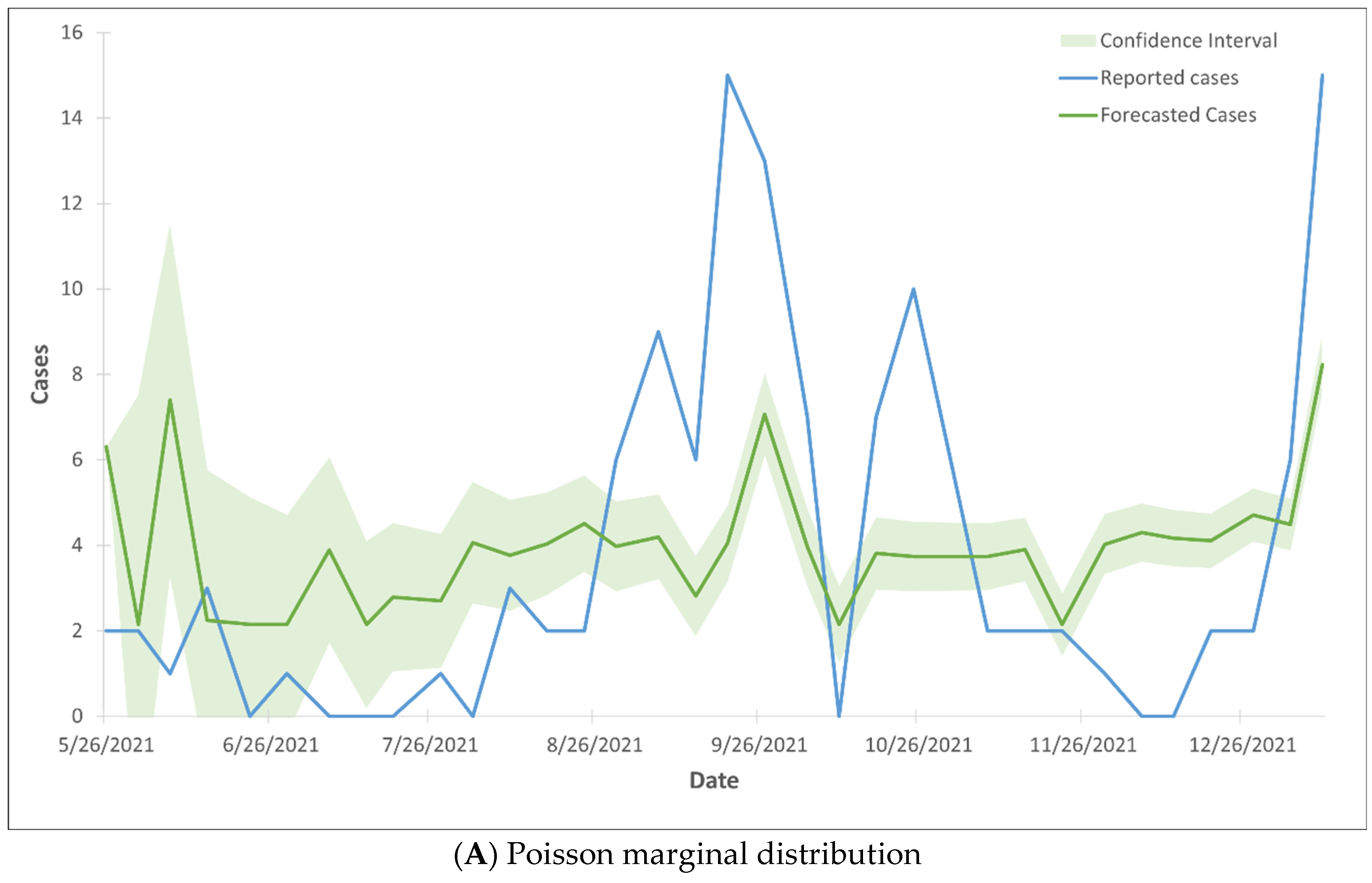
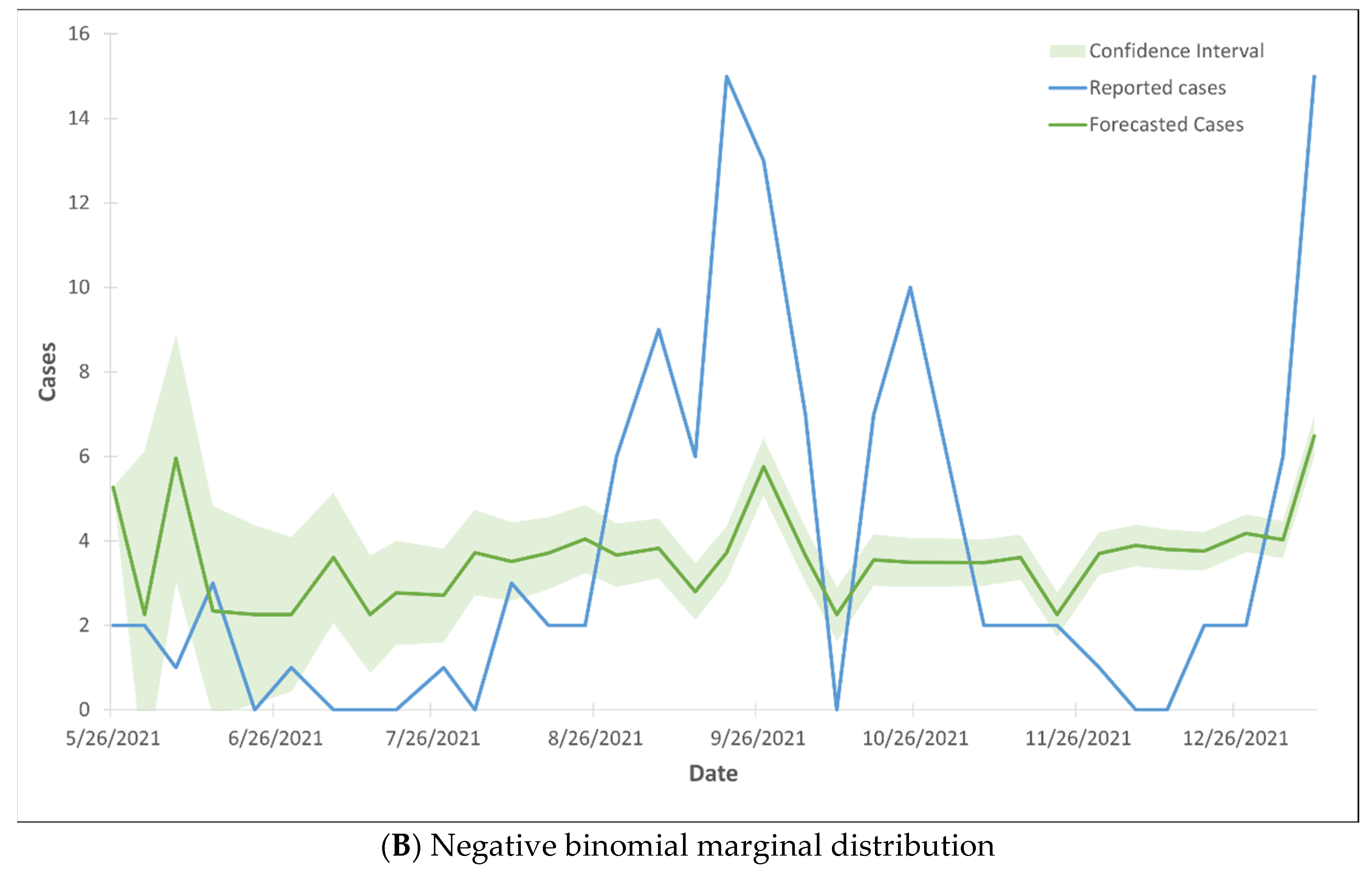
3.4. Modeling Hospital Admissions
3.5. Modeling Death Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
International Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Agrawal, S.; Orschler, L.; Lackner, S. Long-term monitoring of SARS-CoV-2 RNA in wastewater of the Frankfurt Metropolitan A in southern Germany. Sci. Rep. 2021, 11, 5372. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, R.; Curtis, K.; Bivins, A.; Bibby, K.; Weir, M.H.; Yetka, K. COVID-19 surveillance in southeastern Virginia using wastewater-based epidemiology. Water Res. 2020, 186, 116296. [Google Scholar] [CrossRef] [PubMed]
- Parasa, S.; Desai, M.; Thoguluva Chandrasekar, V.; Patel, H.K.; Kennedy, K.F.; Roesch, T.; Spadaccini, M.; Colombo, M.; Gabbiadini, R.; Artifon, E.L.A.; et al. Prevalence of gastrointestinal symptoms and fecal viral shedding in patients with coronavirus disease 2019: A systematic review and meta-analysis. JAMA Netw. Open 2020, 3, e2011335. [Google Scholar] [CrossRef]
- Peccia, J.; Zulli, A.; Brackney, D.E.; Grubaugh, N.D.; Kaplan, E.H.; Casanovas-Massana, A.I.; Ko, A.A.; Malik, D.; Wang, M.; Warren, J.L. Measurement of SARS-CoV-2 RNA in wastewater tracks community infection dynamics. Nat. Biotechnol. 2020, 38, 1164–1167. [Google Scholar] [CrossRef] [PubMed]
- Tang, A.; Tong, D.; Wang, H.L.; Dai, Y.X.; Li, K.F.; Liu, J.N.; Wu, W.J.; Yuan, C.Y.; Yu, M.L.; Li, P.; et al. Detection of novel coronavirus by RT-PCR in stool specimen from asymptomatic child, China. Emerg. Infect. Dis. 2020, 26, 1337–1339. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Zhang, J.; Xiao, A.; Gu, X.; Lee, W.L.; Armas, F.; Kauffman, K.; Hanage, W.; Matus, M.; Ghaeli, N.; et al. SARS-CoV-2 titers in wastewater are higher than expected from clinically confirmed cases. mSystems 2020, 5, e00614. [Google Scholar] [CrossRef]
- Markt, R.; Endler, L.; Amman, F.; Schedl, A.; Penz, T.; Büchel-Marxer, M.; Grünbacher, D.; Mayr, M.; Peer, E.; Pedrazzini, M.; et al. Detection and abundance of SARS-CoV-2 in wastewater in Liechtenstein, and the estimation of prevalence and impact of the B. 1.1.7 variant. J. Water Health 2022, 1, 114–125. [Google Scholar] [CrossRef]
- Trottier, J.; Darques, R.; Ait Mouheb, N.; Partiot, E.; Bakhache, W.; Deffieu, M.S.; Gaudin, R. Post-lockdown detection of SARS-CoV-2 RNA in the wastewater of Montpellier, France. One Health 2020, 10, 100157. [Google Scholar] [CrossRef] [PubMed]
- Jeng, H.A.; Singh, R.; Diawara, N.; Curtis, K.; Gonzalez, R.; Welch, N.; Jackson, C.; Jurgens, D.; Adikari, S. Application of wastewater-based surveillance and copula time-series model for COVID-19 forecasts. Sci. Total Environ. 2023, 885, 163655. [Google Scholar] [CrossRef]
- D’Aoust, P.M.; Mercier, E.; Montpetit, D.; Jia, J.J.; Alexandrov, I.; Neault, N.; Baig, A.T.; Mayne, J.; Zhang, X.; Alain, T.; et al. Quantitative analysis of SARS-CoV-2 RNA from wastewater solids in communities with low COVID-19 incidence and prevalence. Water Res. 2021, 188, 116560. [Google Scholar] [CrossRef]
- Róka, E.; Khayer, B.; Kis, Z.; Kovács, L.B.; Schuler, E.; Magyar, N.; Málnási, T.; Oravecz, O.; Pályi, B.; Pándics, T.; et al. Ahead of the second wave: Early warning for COVID-19 by wastewater surveillance in Hungary. Sci. Total Environ. 2021, 786, 147398. [Google Scholar] [CrossRef] [PubMed]
- Kisand, V.; Laas, P.; Palmik-Das, K.; Panksep, K.; Tammert, H.; Albreht, L.; Allemann, H.; Liepkalns, L.; Vooro, K.; Ritz, C.; et al. Prediction of COVID-19 positive cases, a nation-wide SARS-CoV-2 wastewater-based epidemiology study. Water Res. 2023, 231, 119617. [Google Scholar] [CrossRef] [PubMed]
- Wurtz, N.; Lacoste, A.; Jardot, P.; Delache, A.; Fontaine, X.; Verlande, M.; Annessi, A.; Giraud-Gatineau, A.; Chaudet, H.; Fournier, P.E.; et al. Viral RNA in city wastewater as a key indicator of COVID-19 recrudescence and containment measures effectiveness. Front. Microbiol. 2021, 12, 664477. [Google Scholar] [CrossRef]
- Daza-Torres, M.L.; Montesinos-López, J.C.; Kim, M.; Olson, R.; Bess, C.W.; Rueda, L.; Susa, M.; Tucker, L.; García, Y.E.; Schmidt, A.J.; et al. Model training periods impact estimation of COVID-19 incidence from wastewater viral loads. Sci. Total Environ. 2023, 858, 159680. [Google Scholar] [CrossRef]
- Taghia, J.; Kulyk, V.; Ickin, S.; Folkesson, M.; Nyström, C.; Ȧgren, K.; Brezicka, T.; Vingasre, T.; Karlsson, J.; Fritzell, I.; et al. Development of forecast models for COVID-19 hospital admissions using anonymized and aggregated mobile network data. Sci. Rep. 2022, 12, 17726. [Google Scholar] [CrossRef] [PubMed]
- Galani, A.; Aalizadeh, R.; Kostakis, M.; Markou, A.; Alygizakis, N.; Lytras, T.; Adamopoulos, P.G.; Peccia, J.; Thompson, D.C.; Kontou, A.; et al. SARS-CoV-2 wastewater surveillance data can predict hospitalizations and ICU admissions. Sci. Total Environ. 2022, 804, 150151. [Google Scholar] [CrossRef]
- Nelsen, R.B. An Introduction to Copulas; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Sen, S.; Diawara, N. Supervised Classification Using Finite Mixture Copula. J. Probab. Stat. Sci. 2017, 15, 189–201. [Google Scholar]
- Shahriari, S.; Sisson, S.A.; Rashidi, T. Copula ARMA-GARCH modeling of spatially and temporally correlated time series data for transportation planning use. Transp. Res. Part C Emerg. Technol. 2023, 146, 103969. [Google Scholar] [CrossRef]
- Ekinci, A. Modelling and forecasting of growth rate of new COVID-19 cases in top nine affected countries: Considering conditional variance and asymmetric effect. Chaos Solitons Fractals 2021, 151, 111227. [Google Scholar] [CrossRef] [PubMed]
- Wulff, J.N.; Jeppesen, L.E. Multiple imputation by chained equations in praxis: Guidelines and review. Electron. J. Bus. Res. Methods 2017, 15, 41–56. [Google Scholar]
- Alzahrani, S.I.; Aljamaan, I.A.; Al-Fakih, E.A. Forecasting the spread of the COVID-19 pandemic in Saudi Arabia using ARIMA prediction model under current public health interventions. J. Infect. Public Health 2020, 13, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Tounkara, F.; Lefebvre, G.; Greenwood, C.; Oualkacha, K. A flexible copula-based approach for the analysis of secondary phenotypes in ascertained samples. Stat. Med. 2020, 39, 517–543. [Google Scholar] [CrossRef] [PubMed]
- Aouissi, H.A.; Kechebar, M.S.A.; Ababsa, M.; Roufayel, R.; Neji, B.; Petrisor, A.I.; Hamimes, A.; Epelboin, L.; Ohmagari, N. The Importance of behavioral and native factors on COVID-19 infection and severity: Insights from a preliminary cross-sectional study. Healthcare 2022, 10, 1341. [Google Scholar] [CrossRef]
- Plescia, M.; Hannan, C.; Baggett, J. A pandemic success story: Distribution and administration of COVID-19 vaccines. J. Public Health Manag. Pract. 2022, 28, 749–750. [Google Scholar] [CrossRef]
- Suryawanshi, Y.; Biswas, D.A. Herd immunity to fight against COVID-19: A narrative review. Cureus 2023, 15, e33575. [Google Scholar] [CrossRef]
- Gasmi, A.; Peana, M.; Pivina, L.; Srinath, S.; Benahmed, G.A.; Semenova, Y.; Menzel, A.; Dadar, M.; Bjørklund, G. Interrelations between COVID-19 and other disorders. Clin. Immunol. 2021, 224, 108651. [Google Scholar] [CrossRef] [PubMed]
- Masarotto, G.; Varin, C. Gaussian copula regression in R. J. Stat. Softw. 2017, 77, 1–26. [Google Scholar] [CrossRef]
- Song, P.X.-K. Multivariate dispersion models generated from Gaussian copula. Scand. J. Stat. 2020, 27, 305–320. [Google Scholar] [CrossRef]
- Guolo, A.; Varin, C. Beta regression for time series analysis of bounded data, with application to Canada Google Flu Trends. Ann. Appl. Stat. 2014, 8, 74–88. [Google Scholar] [CrossRef]
- Henn, L.L. Limitations and performance of three approaches to Bayesian inference for Gaussian copula regression models of discrete data. Comput. Stat. 2022, 37, 909–946. [Google Scholar] [CrossRef]
- Suresh, K.; Taylor, J.M.G.; Tsodikov, A. A Gaussian copula approach for dynamic prediction of survival with a longitudinal biomarker. Biostatistics 2019, 22, 504–521. [Google Scholar] [CrossRef]
- Smith, M.; Abdesselem, H.B.; Mullins, M.; Tan, T.M.; Nel, A.J.M.; Al-Nesf, M.A.Y.; Bensmail, I.; Majbour, N.K.; Vaikath, N.N.; Naik, A.; et al. Age, disease severity and ethnicity influence humoral responses in a multi-ethnic COVID-19 cohort. Viruses 2021, 13, 786. [Google Scholar] [CrossRef] [PubMed]
- Akpinar, G.; Demir, M.C.; Sultanoglu, H.; Sonmez, F.T.; Karaman, K.; Keskin, B.H.; Ince, N.; Guclu, D. The demographic analysis of the probable COVID-19 cases in terms of RT-PCR results and age. Clin. Lab. 2021, 67, 1058. [Google Scholar] [CrossRef] [PubMed]
- Raine, S.; Liu, A.; Mintz, J.; Wahood, W.; Huntley, K.; Haffizulla, F. Racial and ethnic disparities in COVID-19 Outcomes: Social Determination of Health. Int. J. Environ. Res. Public Health 2020, 17, 8115. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, U.V.; Larkins-Pettigrew, M. Racial demographics and COVID-19 confirmed cases and deaths: A correlational analysis of 2886 US counties. J. Public Health 2020, 42, 445–447. [Google Scholar] [CrossRef]
- Xu, A.; Loch-Temzelides, T.; Adiole, C.; Botton, N.; Dee, S.G.; Masiello, C.A.; Osborn, M.; Torres, M.A.; Cohan, D.S. Race and ethnic minority, local pollution, and COVID-19 deaths in Texas. Sci. Rep. 2022, 12, 1002. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.B.; Charles, E.J.; Mehaffey, J.H. Socio-economic Status and COVID-19-Related Cases and Fatalities. Public Health 2020, 189, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Alqawba, M.; Diawara, N. Copula-based Markov zero-inflated count time series models with application. J. Appl. Stat. 2021, 48, 786–803. [Google Scholar] [CrossRef]
- Ashrafi, M.; Soltanian-Zadeh, H. Multivariate Gaussian copula mutual information to estimate functional connectivity with less random architecture. Entropy 2022, 24, 631. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COVID-19 Cases | Hospital Admissions | Deaths | |||||||
|---|---|---|---|---|---|---|---|---|---|
| AIC | Dispersion Parameters | Gaussian Copula Coefficients (AR, MA) with Significance | AIC | Dispersion Parameters | Gaussian Copula Coefficients (AR, MA) with Significance | AIC | Dispersion Parameters | Gaussian Copula Coefficients (AR, MA) with Significance | |
| Poisson ARMA (1,1) with missing data | 340.43 | (0.51 *, −0.21) | 165.11 | (0.67 *, −0.38 *) | |||||
| Negative Binomial ARMA (1,1) with missing data | 218.96 | 0.42 * | (0.76 *, −0.21) | 133.22 | 1.17 | (0.77 *, −0.33) | |||
| Poisson ARMA (1,1) with imputed data | 409.46 | (0.49 *, −0.23) | 188.75 | (0.64 *, −0.37 *) | |||||
| Negative Binomial ARMA (1,1) with imputed data | 253.99 | 0.42 * | (0.71 *, −0.14) | 155.80 | 0.85 * | (0.71 *, −0.29) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeng, H.A.; Diawara, N.; Welch, N.; Jackson, C.; Singh, R.; Curtis, K.; Gonzalez, R.; Jurgens, D.; Adikari, S. Forecasting COVID-19 Cases, Hospital Admissions, and Deaths Based on Wastewater SARS-CoV-2 Surveillance Using Gaussian Copula Time Series Marginal Regression Model. COVID 2025, 5, 25. https://doi.org/10.3390/covid5020025
Jeng HA, Diawara N, Welch N, Jackson C, Singh R, Curtis K, Gonzalez R, Jurgens D, Adikari S. Forecasting COVID-19 Cases, Hospital Admissions, and Deaths Based on Wastewater SARS-CoV-2 Surveillance Using Gaussian Copula Time Series Marginal Regression Model. COVID. 2025; 5(2):25. https://doi.org/10.3390/covid5020025
Chicago/Turabian StyleJeng, Hueiwang Anna, Norou Diawara, Nancy Welch, Cynthia Jackson, Rekha Singh, Kyle Curtis, Raul Gonzalez, David Jurgens, and Sasanka Adikari. 2025. "Forecasting COVID-19 Cases, Hospital Admissions, and Deaths Based on Wastewater SARS-CoV-2 Surveillance Using Gaussian Copula Time Series Marginal Regression Model" COVID 5, no. 2: 25. https://doi.org/10.3390/covid5020025
APA StyleJeng, H. A., Diawara, N., Welch, N., Jackson, C., Singh, R., Curtis, K., Gonzalez, R., Jurgens, D., & Adikari, S. (2025). Forecasting COVID-19 Cases, Hospital Admissions, and Deaths Based on Wastewater SARS-CoV-2 Surveillance Using Gaussian Copula Time Series Marginal Regression Model. COVID, 5(2), 25. https://doi.org/10.3390/covid5020025