
Better COVID-19 Outcomes in Children with Good Asthma Control

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Study Design
2.3. Methods
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barber, A.T.; Loughlin, C.E. Pediatric Pulmonology 2020 year in review: Asthma. Pediatr. Pulmonol. 2021, 56, 2455–2459. [Google Scholar] [CrossRef]
- Graff, K.; Smith, C.; Silveira, L.; Jung, S.; Curran-Hays, S.; Jarjour, J.; Carpenter, L.; Pickard, K.; Mattiucci, M.; Fresia, J.; et al. Risk Factors for Severe COVID-19 in Children. Pediatr. Infect. Dis. J. 2021, 40, e137–e145. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- Zhang, J.J.; Cao, Y.Y.; Dong, X.; Wang, B.C.; Liao, M.Y.; Lin, J.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Distinct characteristics of COVID-19 patients with initial rRT-PCR-positive and rRT-PCR-negative results for SARS-CoV-2. Allergy 2020, 75, 1809–1812. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef]
- Garg, S.; Kim, L.; Whitaker, M.; O’Halloran, A.; Cummings, C.; Holstein, R.; Prill, M.; Chai, S.J.; Kirley, P.D.; Alden, N.B.; et al. Hospitalization Rates and Characteristics of Patients Hospitalized with Laboratory-Confirmed Coronavirus Disease 2019—COVID-NET, 14 States, March 1–30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 458–464. [Google Scholar] [CrossRef]
- Halpin, D.M.G.; Faner, R.; Sibila, O.; Badia, J.R.; Agusti, A. Do chronic respiratory diseases or their treatment affect the risk of SARS-CoV-2 infection? Lancet Respir. Med. 2020, 8, 436–438. [Google Scholar] [CrossRef]
- Papadopoulos, N.G.; Custovic, A.; Deschildre, A.; Mathioudakis, A.G.; Phipatanakul, W.; Wong, G.; Xepapadaki, P.; Agache, I.; Bacharier, L.; Bonini, M.; et al. Impact of COVID-19 on Pediatric Asthma: Practice Adjustments and Disease Burden. J. Allergy Clin. Immunol. Pract. 2020, 8, 2592–2599.e3. [Google Scholar] [CrossRef]
- Moeller, A.; Thanikkel, L.; Duijts, L.; Gaillard, E.A.; Garcia-Marcos, L.; Kantar, A.; Tabin, N.; Turner, S.; Zacharasiewicz, A.; Pijnenburg, M.W.H. COVID-19 in children with underlying chronic respiratory diseases: Survey results from 174 centres. ERJ Open Res. 2020, 6, 00409–02020. [Google Scholar] [CrossRef]
- Papadopoulos, N.G.; Mathioudakis, A.G.; Custovic, A.; Deschildre, A.; Phipatanakul, W.; Wong, G.; Xepapadaki, P.; Abou-Taam, R.; Agache, I.; Castro-Rodriguez, J.A.; et al. Childhood asthma outcomes during the COVID-19 pandemic: Findings from the PeARL multi-national cohort. Allergy 2021, 76, 1765–1775. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team. Coronavirus Disease 2019 in Children—United States, February 12-April 2, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 422–426. [Google Scholar] [CrossRef]
- Parri, N.; Lenge, M.; Buonsenso, D. Children with Covid-19 in pediatric emergency departments in Italy. N. Engl. J. Med. 2020, 383, 187–190. [Google Scholar] [CrossRef]
- Banasiak, N.C. Implementation of the Asthma Control Test in Primary Care to Improve Patient Outcomes. J. Pediatr. Health Care 2018, 32, 591–599. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention. GINA 2023. Available online: http://www.ginasthma.org (accessed on 20 August 2023).
- COVID-19 Situation in Slovenia. Available online: https://covid-19.sledilnik.org/en/stats (accessed on 28 August 2023).
- Zheng, F.; Liao, C.; Fan, Q.H.; Chen, H.B.; Zhao, X.G.; Xie, Z.G.; Li, X.L.; Chen, C.X.; Lu, X.X.; Liu, Z.S.; et al. Clinical Characteristics of Children with Coronavirus Disease 2019 in Hubei, China. Curr. Med. Sci. 2020, 40, 275–280. [Google Scholar] [CrossRef]
- Dong, X.; Cao, Y.Y.; Lu, X.X.; Zhang, J.J.; Du, H.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Eleven faces of coronavirus disease 2019. Allergy 2020, 75, 1699–1709. [Google Scholar] [CrossRef]
- Shi, T.; Pan, J.; Katikireddi, S.V.; McCowan, C.; Kerr, S.; Agrawal, U.; Shah, S.A.; Simpson, C.R.; Ritchie, L.D.; Robertson, C.; et al. Risk of COVID-19 hospital admission among children aged 5-17 years with asthma in Scotland: A national incident cohort study. Lancet Respir. Med. 2022, 10, 191–198. [Google Scholar] [CrossRef]
- Dolby, T.; Nafilyan, V.; Morgan, A.; Kallis, C.; Sheikh, A.; Quint, J.K. Relationship between asthma and severe COVID-19: A national cohort study. Thorax 2023, 78, 120–127. [Google Scholar] [CrossRef]
- Bateman, E.D.; Reddel, H.K.; Eriksson, G.; Peterson, S.; Ostlund, O.; Sears, M.R.; Jenkins, C.; Humbert, M.; Buhl, R.; Harrison, T.W.; et al. Overall asthma control: The relationship between current control and future risk. J. Allergy Clin. Immunol. 2010, 125, 600–608, 608.e1–608.e6. [Google Scholar] [CrossRef]
- Bateman, E.D.; Bousquet, J.; Busse, W.W.; Clark, T.J.; Gul, N.; Gibbs, M.; Pedersen, S.; on behalf of the GOAL Steering Committee and Investigators. Stability of asthma control with regular treatment: An analysis of the Gaining Optimal Asthma controL (GOAL) study. Allergy 2008, 63, 932–938. [Google Scholar] [CrossRef]
- Message, S.D.; Laza-Stanca, V.; Mallia, P.; Parker, H.L.; Zhu, J.; Kebadze, T.; Contoli, M.; Sanderson, G.; Kon, O.M.; Papi, A.; et al. Rhinovirus-induced lower respiratory illness is increased in asthma and related to virus load and Th1/2 cytokine and IL-10 production. Proc. Natl. Acad. Sci. USA 2008, 105, 13562–13567. [Google Scholar] [CrossRef]
- Holley, A.B. Does asthma lead to worse COVID-19 otcomes? Medscape 2020, 10223, 514–523. [Google Scholar]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef]
- Zhang, H.P.; Sun, Y.L.; Wang, Y.F.; Yazici, D.; Azkur, D.; Ogulur, I.; Azkur, A.K.; Yang, Z.W.; Chen, X.X.; Zhang, A.Z.; et al. Recent developments in the immunopathology of COVID-19. Allergy 2023, 78, 369–388. [Google Scholar] [CrossRef]
- Krivec, U.; Kofol Seliger, A.; Tursic, J. COVID-19 lockdown dropped the rate of paediatric asthma admissions. Arch. Dis. Child. 2020, 105, 809–810. [Google Scholar] [CrossRef]
- Taquechel, K.; Diwadkar, A.R.; Sayed, S.; Dudley, J.W.; Grundmeier, R.W.; Kenyon, C.C.; Henrickson, S.E.; Himes, B.E.; Hill, D.A. Pediatric Asthma Health Care Utilization, Viral Testing, and Air Pollution Changes During the COVID-19 Pandemic. J. Allergy Clin. Immunol. Pract. 2020, 8, 3378–3387.e11. [Google Scholar] [CrossRef]
- Yang, Z.; Wang, X.; Wan, X.G.; Wang, M.L.; Qiu, Z.H.; Chen, J.L.; Shi, M.H.; Zhang, S.Y.; Xia, Y.L. Pediatric asthma control during the COVID-19 pandemic: A systematic review and meta-analysis. Pediatr. Pulmonol. 2022, 57, 20–25. [Google Scholar] [CrossRef]
- Jackson, D.J.; Busse, W.W.; Bacharier, L.B.; Kattan, M.; O’Connor, G.T.; Wood, R.A.; Visness, C.M.; Durham, S.R.; Larson, D.; Esnault, S.; et al. Association of respiratory allergy, asthma, and expression of the SARS-CoV-2 receptor ACE2. J. Allergy Clin. Immunol. 2020, 146, 203–206.e3. [Google Scholar] [CrossRef]
- Pakkasela, J.; Ilmarinen, P.; Honkamäki, J.; Tuomisto, L.E.; Andersén, H.; Piirilä, P.; Hisinger-Mölkänen, H.; Sovijärvi, A.; Backman, H.; Lundbäck, B.; et al. Age-specific incidence of allergic and non-allergic asthma. BMC Pulm. Med. 2020, 20, 9. [Google Scholar] [CrossRef]
- Shaw, B.; Daskareh, M.; Gholamrezanezhad, A. The lingering manifestations of COVID-19 during and after convalescence: Update on long-term pulmonary consequences of coronavirus disease 2019 (COVID-19). Radiol. Med. 2020, 126, 40–46. [Google Scholar] [CrossRef]
- Patel, J.M. Multisystem Inflammatory Syndrome in Children (MIS-C). Curr. Allergy Asthma Rep. 2022, 22, 53–60. [Google Scholar] [CrossRef]
- Tosca, M.A.; Crocco, M.; Girosi, D.; Olcese, R.; Schiavetti, I.; Ciprandi, G. Unaffected asthma control in children with mild asthma after COVID-19. Pediatr. Pulmonol. 2021, 56, 3068–3070. [Google Scholar] [CrossRef]
- Gaietto, K.; Bergum, N.; Acevedo-Torres, N.; Snyder, O.; DiCicco, L.A.; Butler, G.; Rauenswinter, S.; Iagnemma, J.; Wolfson, D.; Kazmerski, T.M.; et al. The Impact of SARS-CoV-2 Infection on Symptom Control and Lung Function in Children with Asthma. Ann. Am. Thorac. Soc. 2023; (submitted; accepted; in press). [Google Scholar] [CrossRef]
- Lee, S.; Zhang, A.; Liu, L.; Salvo, D.; Wang, L. Changes in physical activity and sedentary time among children with asthma during the COVID-19 pandemic and influencing factors. J. Asthma 2023, 60, 525–533. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | SARS-CoV-2 URTI (n = 27) | SARS-CoV-2 LRTI (n = 15) | Test Statistic, p-Value |
|---|---|---|---|
| Age (y), mean (SD) | 12.0 (SD 4.1) | 14.6 (SD 3.2) | t = 2.10, 0.042 |
| Male, no. (%) | 20 (74%) | 6 (40%) | χ2 = 4.75, 0.029 |
| BMI Z-score, median (IQR) | 0.40 (IQR −0.40–1.01) | −0.24 (IQR −0.91–1.13) | U = 124.00, 0.431 |
| Atopy, no. (%) | 24 (89%) | 8 (53%) | χ2 = 5.42, 0.020 |
| Regular ICS, no. (%) | 18 (67%) | 7 (47%) | χ2 = 1.60, 0.206 |
| Daily ICS dose (budesonide/equivalent) (μg), median (IQR) | 200 (IQR 0–400) | 160 (IQR 0–200) | U = 147.50, 0.131 |
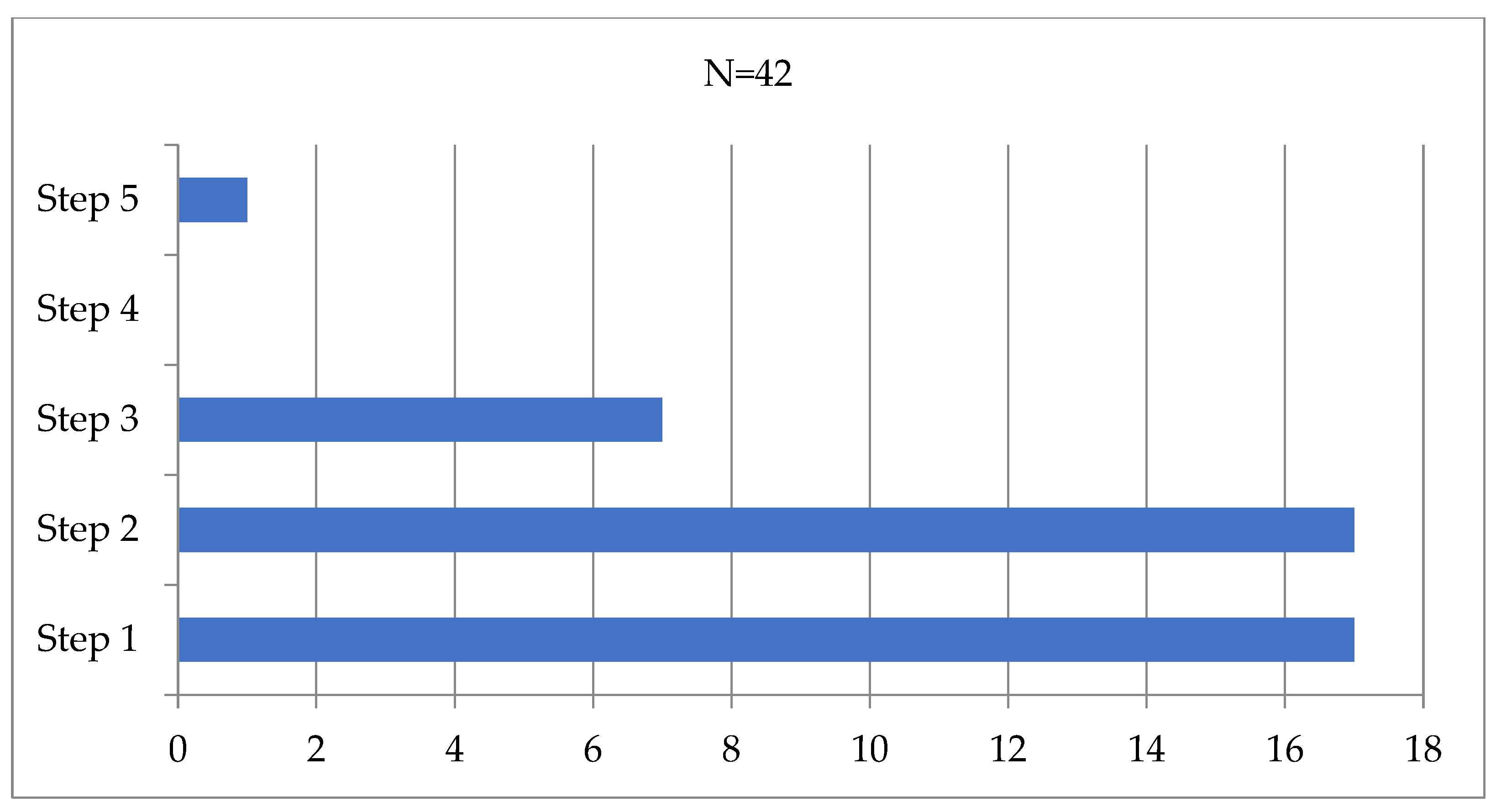
| GINA treatment step Step 1, no. (%) Step 2, no. (%) Step 3, no. (%) Step 5, no (%) | 9 (33%) 13 (48%) 4 (15%) 1 (4%) | 8 (53%) 4 (27%) 3 (20%) 0 (0%) | χ2 = 2.76, 0.430 |
| Well-controlled asthma, no. (%) | 25 (93%) | 3 (20%) | χ2 = 22.87, <0.001 |
| ACT score, points, mean (SD) | 23.6 (SD 1.9) | 19.7 (SD 1.7) | t = 6.39, <0.001 |
| New referrals, no. (%) | 4 (15%) | 2 (14%) | χ2 = 0.02, 0.895 |
| Therapy step-up, no. (%) | 3 (11%) | 7 (47%) | χ2 = 6.72, 0.010 |
| p Value | Odds Ratio (OR) | 95% CI for OR | |
|---|---|---|---|
| Age Gender | 0.214 0.298 | 1.22 0.28 | 0.89–1.67 0.03–3.08 |
| Atopy Daily ICS dose | 0.120 0.242 | 9.20 1.01 | 0.56–150.21 1.00–1.01 |
| ACT score | 0.003 | 0.39 | 0.21–0.73 |
| All Patients (n = 37) | p Value | SARS-CoV-2 URTI (n = 27) | p Value | SARS-CoV-2 LRTI (n = 10) | p Value | |
|---|---|---|---|---|---|---|
| FVC, % of predicted pre-COVID-19 | 96 (12) | 0.30 | 94 (11) | 0.36 | 100 (12) | 0.62 |
| FVC, % of predicted post-COVID-19 | 94 (14) | 92 (13) | 99 (16) | |||
| FEV1, % of predicted pre-COVID-19 | 103 (11) | 0.32 | 102 (11) | 0.62 | 104 (13) | 0.17 |
| FEV1, % of predicted post-COVID-19 | 101 (12) | 101 (13) | 101 (13) | |||
| FEV1/FVC, % pre-COVID-19 | 88 (7) | 0.95 | 89 (8) | 0.72 | 87 (5) | 0.42 |
| FEV1/FVC, % post-COVID-19 | 88 (5) | 89 (5) | 86 (3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodman Berlot, J.; Aldeco, M.; Lepej, D.; Praprotnik, M.; Šetina Šmid, S.; Zver, A.; Krivec, U. Better COVID-19 Outcomes in Children with Good Asthma Control. Appl. Microbiol. 2023, 3, 1204-1213. https://doi.org/10.3390/applmicrobiol3040083
Rodman Berlot J, Aldeco M, Lepej D, Praprotnik M, Šetina Šmid S, Zver A, Krivec U. Better COVID-19 Outcomes in Children with Good Asthma Control. Applied Microbiology. 2023; 3(4):1204-1213. https://doi.org/10.3390/applmicrobiol3040083
Chicago/Turabian StyleRodman Berlot, Jasna, Malena Aldeco, Dušanka Lepej, Marina Praprotnik, Saša Šetina Šmid, Aleksandra Zver, and Uroš Krivec. 2023. "Better COVID-19 Outcomes in Children with Good Asthma Control" Applied Microbiology 3, no. 4: 1204-1213. https://doi.org/10.3390/applmicrobiol3040083
APA StyleRodman Berlot, J., Aldeco, M., Lepej, D., Praprotnik, M., Šetina Šmid, S., Zver, A., & Krivec, U. (2023). Better COVID-19 Outcomes in Children with Good Asthma Control. Applied Microbiology, 3(4), 1204-1213. https://doi.org/10.3390/applmicrobiol3040083