
Effectiveness of the Human Oral Microbe Identification Microarray in Identifying Periodontal Pathogens: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
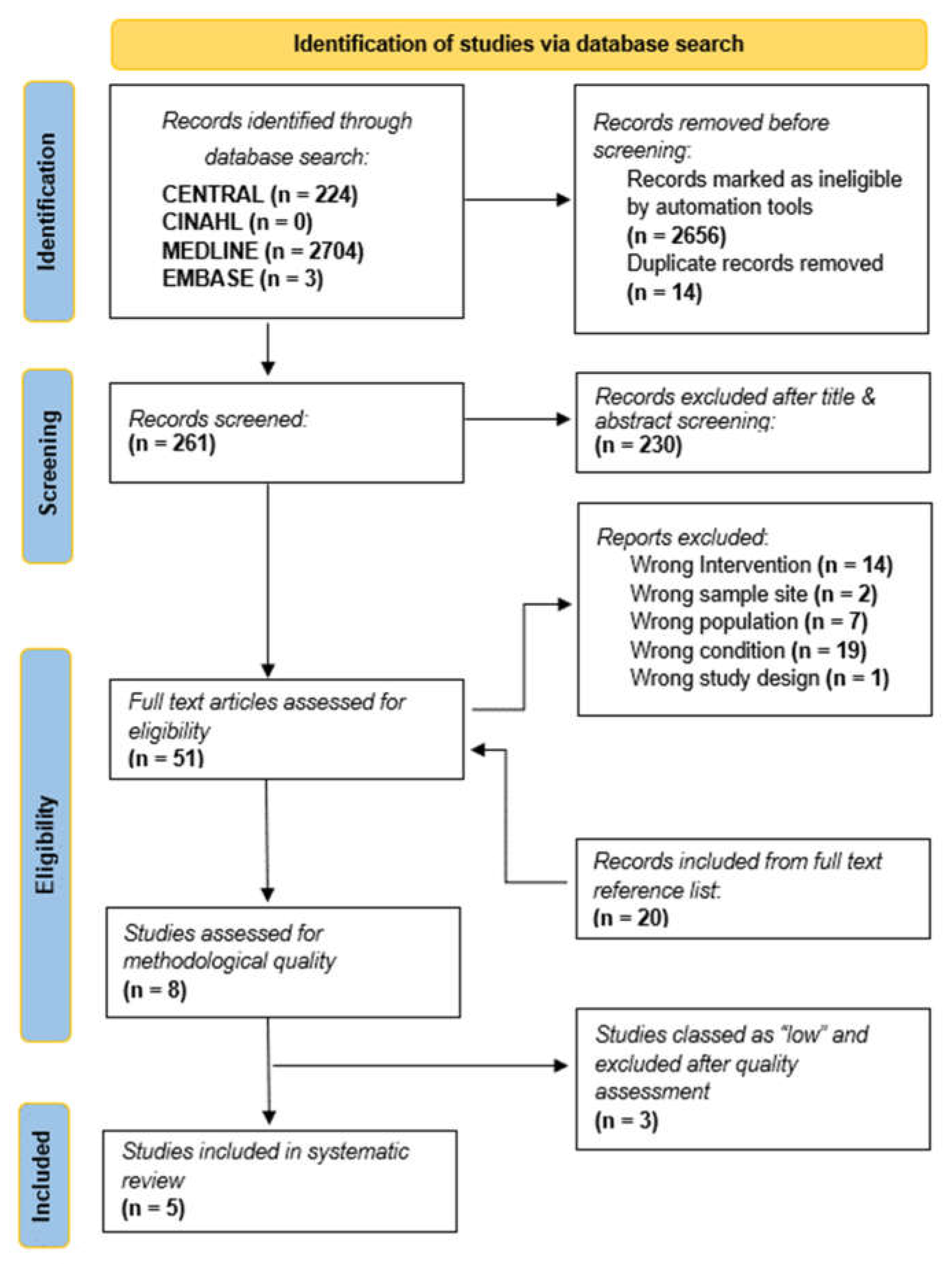
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DGGE | Denaturing Gradient Gel Electrophoresis |
| HOMD | Human Oral Microbe Database |
| HOMIM | Human Oral Microbe Identification Microarray |
| HOMINGS | Human Oral Microbe Identification using Next-Generation Sequencing |
| MESH | Medical Subject Headings |
| PH | Periodontal Health |
| PCR | Polymerase Chain Reaction |
| RP | Refractory Periodontitis |
References
- Muyzer, G.; De Waal, E.C.; Uitterlinden, A.G. Profiling of complex microbial population by DGGE analysis of polymerase chain reaction amplified genes encoding for 16S rRNA. Appl. Environ. Microbiol. 1993, 62, 2676–2680. [Google Scholar]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Casanova, L.; Hughes, F.J.; Preshaw, P.M. Diabetes and periodontal disease: A two-way relationship. Br. Dent. J. 2014, 217, 433–437. [Google Scholar] [CrossRef]
- Persson, G.R. Diabetes and periodontal disease: An update for health care providers. Diabetes Spectr. 2011, 24, 195–198. [Google Scholar] [CrossRef]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J. Clin. Periodontol. 2018, 45, 138–149. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Li, Y.; Cao, Y.; Xue, J.; Zhou, X. The oral microbiome diversity and its relation to human diseases. Folia Microbiol. 2015, 60, 69–80. [Google Scholar] [CrossRef]
- Lourenço, T.G.B.; Heller, D.; Silva-Boghossian, C.M.; Cotton, S.L.; Paster, B.J.; Colombo, A.P.V. Microbial signature profiles of periodontally healthy and diseased patients. J. Clin. Periodontol. 2015, 41, 1027–1036. [Google Scholar] [CrossRef]
- Teeuw, W.J.; Kosho, M.X.; Poland, D.C.; Gerdes, V.E.; Loos, B.G. Periodontitis as a possible early sign of diabetes mellitus. BMJ Open Diabetes Res. Care 2017, 5, e000326. [Google Scholar] [CrossRef]
- Gao, L.; Xu, T.; Huang, G.; Jiang, S.; Gu, Y.; Chen, F. Oral microbiomes: More and more importance in oral cavity and whole body. Protein Cell. 2018, 9, 488–500. [Google Scholar] [CrossRef]
- Yu, G.; Dye, B.A.; Gail, M.H.; Shi, J.; Klepac-Ceraj, V.; Paster, B.J.; Wang, G.Q.; Wei, W.Q.; Fan, J.H.; Qiao, Y.L.; et al. The association between the upper digestive tract microbiota by HOMIM and oral health in a population-based study in Linxian, China. BMC Public Health 2014, 14, 1–7. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS. Med. 2019, 6, e1000097. [Google Scholar]
- Gafan, G.P.; Spratt, D.A. Denaturing gradient gel electrophoresis gel expansion (DGGEGE)–an attempt to resolve the limitations of co-migration in the DGGE of complex polymicrobial communities. FEMS Microbiol. Lett. 2005, 253, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Gafan, G.P.; Lucas, V.S.; Roberts, G.J.; Petrie, A.; Wilson, M.; Spratt, D.A. Statistical analyses of complex denaturing gradient gel electrophoresis profiles. J. Clin. Microbiol. 2005, 43, 3971–3978. [Google Scholar] [CrossRef] [PubMed]
- Seerangaiyan, K.; Jüch, F.; Winkel, E.G. Tongue coating: Its characteristics and role in intra-oral halitosis and general health—A review. J. Breath. Res. 2018, 12, 034001. [Google Scholar] [CrossRef]
- Heller, D.; Helmerhorst, E.J.; Gower, A.C.; Siqueira, W.L.; Paster, B.J.; Oppenheim, F.G. Microbial diversity in the early in vivo-formed dental biofilm. Appl. Environ. Microbiol. 2016, 82, 1881–1888. [Google Scholar] [CrossRef]
- Ahn, J.; Yang, L.; Paster, B.J.; Ganly, I.; Morris, L.; Pei, Z.; Hayes, R.B. Oral microbiome profiles: 16S rRNA pyrosequencing and microarray assay comparison. PLoS. ONE 2011, 6, e22788. [Google Scholar] [CrossRef]
- Freitas, A.O.A.D.; Marquezan, M.; Nojima, M.D.C.G.; Alviano, D.S.; Maia, L.C. The influence of orthodontic fixed appliances on the oral microbiota: A systematic review. Dental. Press. J. Orthod. 2014, 19, 46–55. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, The Cochrane Collaboration; Available online: https://training.cochrane.org/handbook (accessed on 3 July 2022).
- Fujimoto, C.; Maeda, H.; Kokeguchi, S.; Takashiba, S.; Nishimura, F.; Arai, H.; Fukui, K.; Murayama, Y. Application of denaturing gradient gel electrophoresis (DGGE) to the analysis of microbial communities of subgingival plaque. J. Periodontal Res. 2003, 38, 440–445. [Google Scholar] [CrossRef]
- Zijnge, V.; Welling, G.W.; Degener, J.E.; van Winkelhoff, A.J.; Abbas, F.; Harmsen, H.J. Denaturing gradient gel electrophoresis as a diagnostic tool in periodontal microbiology. J. Clin. Microbiol. 2006, 44, 3628–3633. [Google Scholar] [CrossRef]
- Zijnge, V.; Harmsen, H.J.M.; Kleinfelder, J.W.; Van Der Rest, M.E.; Degener, J.E.; Welling, G.W. Denaturing gradient gel electrophoresis analysis to study bacterial community structure in pockets of periodontitis patients. Oral Microbiol. Immunol. 2003, 18, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Zhou, Y.; Li, C.; Li, Y.; Jiang, Y.; Huang, Z.; Liang, J.; Shu, R. Denaturing gradient gel electrophoresis analysis with different primers of subgingival bacterial communities under mechanical debridement. Microbiol. Immunol. 2010, 54, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Mougeot, J.L.C.; Stevens, C.B.; Cotton, S.L.; Morton, D.S.; Krishnan, K.; Brennan, M.T.; Lockhart, P.B.; Paster, B.J.; Bahrani Mougeot, F.K. Concordance of HOMIM and HOMINGS technologies in the microbiome analysis of clinical samples. J. Oral Microbiol. 2016, 8, 30379. [Google Scholar] [CrossRef] [PubMed]
- Colombo, A.P.V.; Boches, S.K.; Cotton, S.L.; Goodson, J.M.; Kent, R.; Haffajee, A.D.; Socransky, S.S.; Hasturk, H.; Van Dyke, T.E.; Dewhirst, F.; et al. Comparisons of subgingival microbial profiles of refractory periodontitis, severe periodontitis, and periodontal health using the human oral microbe identification microarray. J. Periodonl. 2009, 80, 1421–1432. [Google Scholar] [CrossRef]
- Colombo, A.P.V.; Bennet, S.; Cotton, S.L.; Goodson, J.M.; Kent, R.; Haffajee, A.D.; Socransky, S.S.; Hasturk, H.; Van Dyke, T.E.; Dewhirst, F.E.; et al. Impact of periodontal therapy on the subgingival microbiota of severe periodontitis: Comparison between good responders and individuals with refractory periodontitis using the human oral microbe identification microarray. J. Periodontol. 2012, 83, 1279–1287. [Google Scholar] [CrossRef]
- Aspiras, M.B.; Barros, S.P.; Moss, K.L.; Barrow, D.A.; Phillips, S.T.; Mendoza, L.; de Jager, M.; Ward, M.; Offenbacher, S. Clinical and subclinical effects of power brushing following experimental induction of biofilm overgrowth in subjects representing a spectrum of periodontal disease. J. Clin. Periodontol. 2013, 40, 1118–1125. [Google Scholar] [CrossRef]
- Zhou, C.; Trivedi, H.M.; Chhun, N.; Barnes, V.M.; Saxena, D.; Tao, X.; Yihong, L. Using DGGE and 16S rRNA gene sequence analysis to evaluate changes in oral bacterial composition. Chin. J. Dent. Res. 2011, 14, 95–103. [Google Scholar]
- Ireland, A.J.; Soro, V.; Sprague, S.V.; Harradine, N.W.T.; Day, C.; Al-Anezi, S.; Jenkinson, H.F.; Sherriff, M.; Dymock, D.; Sandy, J.R. The effects of different orthodontic appliances upon microbial communities. Orthod. Craniofac. Res. 2014, 17, 115–123. [Google Scholar] [CrossRef]
- Ledder, R.G.; Gilbert, P.; Huws, S.A.; Aarons, L.; Ashley, M.P.; Hull, P.S.; McBain, A.J. Molecular analysis of the subgingival microbiota in health and disease. App. Environ. Microbiol. 2007, 73, 516–523. [Google Scholar] [CrossRef]

{kind=link}
| periodontitis OR periodontal disease OR periodontal infection OR periodontal diseases OR adult periodontitis OR chronic periodontitis OR aggressive periodontitis OR juvenile periodontitis OR localized periodontitis. |
| AND |
| oral microbiota OR oral microbiology OR oral microorganism OR oral microbiome OR oral pathogen OR oral pathogens OR oral biofilm OR red complex OR orange complex OR oral bacteria OR oral bacterial species OR oral subgingival microbiome OR gingivitis OR treponema OR forsythia OR denticola OR actinomycetemcomitans OR buccal mucosa microbiome OR hard palate microbiome OR keratinized gingiva microbiome OR saliva microbiome. |
| AND |
| molecular profiling OR molecular profiling technology OR NGS OR DGGE OR DNA probes OR sequencing OR next-generation sequencing OR metagenomics OR denaturing gradient gel electrophoresis OR culture-based approach OR genetic fingerprinting OR Human Oral Microbe Identification Microarray OR HOMIM OR HOMINGS OR 16S rRNA profiling OR HOMD. |
| Score Protocol | Maximum Score (8 Points) |
|---|---|
| 0.2 |
| 1.2 |
| 0.2 |
| 0.2 |
| 0.6 |
| 0.2 |
| 3.0 |
| - |
| 3.0 |
| 0.2 |
| 0.2 |
| 0.2 |
| Author/ Year | Study Design | Participants | Collection Methods | DNA Extraction | Stats Analysis | Results | Discussion | Total Points/Quality | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Standards | Sample Characterization | Calculation of Sample Size | Ethics | Control of Factors Influencing Collection | |||||||
| Fujimoto et al. 2003 [20] | 0 | 0 | 0.2 | 0 | 0 | 3 | 3 | 0 | 0.2 | 0.2 | 6.6 Moderate |
| Zijnge et al. 2006 [21] | 0.2 | 0 | 0.2 | 0 | 0 | 0 | 3 | 0 | 0.2 | 0.2 | 3.8 Low |
| Zijnge et al. 2003 [22] | 0 | 0.2 | 0.2 | 0 | 0 | 3 | 3 | 0 | 0.2 | 0.2 | 6.8 Moderate |
| Liu et al. 2010 [23] | 0 | 0 | 0.2 | 0 | 0 | 3 | 3 | 0 | 0.2 | 0.2 | 6.6 Moderate |
| Mougeot et al. 2016 [24] | 0 | 0.2 | 0.2 | 0 | 0.2 | 0 | 3 | 0.2 | 0.2 | 0.2 | 4.9 Low |
| Colombo et al. 2009 [25] | 0.2 | 0.2 | 0.2 | 0 | 0.2 | 3 | 3 | 0.2 | 0.2 | 0.2 | 7.4 High |
| Colombo et al. 2012 [26] | 0.2 | 0.2 | 0.2 | 0 | 0.2 | 3 | 3 | 0.2 | 0.2 | 0.2 | 7.4 High |
| Aspiras et al. 2013 [27] | 0.2 | 0.2 | 0.2 | 0 | 0.2 | 0 | 3 | 0.2 | 0.2 | 0.2 | 4.4 Low |
| Author/ Year | Study Design | Participants | Collection Methods | DNA Extraction | Stats Analysis | Conclusion | |
|---|---|---|---|---|---|---|---|
| Sample Standards | General Sample Description | ||||||
| Colombo et al. 2012 [26] | Longitudinal study | No history of systemic disease, periodontal therapy or use of antibiotic therapy within the preceding 6 months. Absence of pregnancy. | 47 subjects over 20 years of age. | After removal of supragingival plaque, subgingival plaque was collected with sterile periodontal curettes from the mesiobuccal aspect of up to 14 teeth in different quadrants. | Universal (Proteinase K and Tween 20). | Mann–Whitney and Chi-square tests to compare differences in demographic and clinical parameters between groups. Wilcoxon signed rank test to compare pre and post therapy. | HOMIM results indicated reduced prevalence of majority of subgingival species in combined and antimicrobial therapy. Results also identified novel species or phylotypes of periodontal pathogens in subjects with refractory periodontitis. |
| Colombo et al. 2009 [25] | Longitudinal study | No history of systemic disease, periodontal therapy or use of antibiotic therapy within the preceding 6 months. Absence of pregnancy. | 67 subjects over 20 years of age. | After removal of supragingival plaque, subgingival plaque was collected with sterile periodontal curettes from the mesiobuccal aspect of up to 14 teeth in different quadrants. | Proteinase K and Tween 20 | Kruskal–Wallis, Mann–Whitney and Chi-square tests to compare differences in clinical parameters among groups. | HOMIM results indicated a greater diversity in subgingival microbiota of subjects with periodontitis at baseline compared to healthy subjects. Results also showed a high frequency of several species not commonly associated with periodontitis at baseline in subjects with refractory periodontitis. |
| Fujimoto et al. 2003 [20] | Not mentioned | Not mentioned | 4 subjects: 2 males and 2 females aged between 18 and 65 years. | Subgingival plaque was collected by insertion of 3 sterile paper points into subgingival lesion pockets, after removal of supragingival plaque with sterile cotton swabs. | Instagene Matrix | n/a | DGGE results were able to reveal dominant microflora. However, due to low sensitivity, DGGE was unable to efficiently detect pathogens with a low abundance. |
| Zijnge et al. 2003 [22] | Not mentioned | No history of systemic disease, periodontal therapy or use of antibiotic therapy within the preceding 6 months. Absence of pregnancy. | 15 adult subjects with minimum of 20 teeth. | After supragingival plaque was removed, subgingival plaque was collected by inserting sterile endodontic absorbing points into the bottom of periodontal pockets. | Phenol/ Chloroform | n/a | DGGE results indicated a change in band profiles before and after treatment of subjects with periodontitis. However, DGGE presented difficulties indicating species based on band positioning. |
| Liu et al. 2010 [23] | Not mentioned | Not mentioned | 6 subjects: four women and two men aged between 29–52 years. | After removal of supragingival plaque, subgingival samples were collected from periodontal pockets using sterile curettes. | TIANGEN kit | Cs = 2j/(a + b) × 100 | DGGE results indicated no change in band pattern before and after treatment for the V3-V5 and V6-V8 region, suggestive of bacterial recolonization. However, recolonization by small numbers of periodontal pathogens would not be identified by this method. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Udoh, S.; Adukwu, E.; Varadi, A.; Saad, S. Effectiveness of the Human Oral Microbe Identification Microarray in Identifying Periodontal Pathogens: A Systematic Review. Appl. Microbiol. 2022, 2, 614-625. https://doi.org/10.3390/applmicrobiol2030047
Udoh S, Adukwu E, Varadi A, Saad S. Effectiveness of the Human Oral Microbe Identification Microarray in Identifying Periodontal Pathogens: A Systematic Review. Applied Microbiology. 2022; 2(3):614-625. https://doi.org/10.3390/applmicrobiol2030047
Chicago/Turabian StyleUdoh, Stephanie, Emmanuel Adukwu, Aniko Varadi, and Saliha Saad. 2022. "Effectiveness of the Human Oral Microbe Identification Microarray in Identifying Periodontal Pathogens: A Systematic Review" Applied Microbiology 2, no. 3: 614-625. https://doi.org/10.3390/applmicrobiol2030047
APA StyleUdoh, S., Adukwu, E., Varadi, A., & Saad, S. (2022). Effectiveness of the Human Oral Microbe Identification Microarray in Identifying Periodontal Pathogens: A Systematic Review. Applied Microbiology, 2(3), 614-625. https://doi.org/10.3390/applmicrobiol2030047