


Perfectionism in Children and Adolescents with Eating-Related Symptoms: A Systematic Review and a Meta-Analysis of Effect Estimates

 , , ,
, , ,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
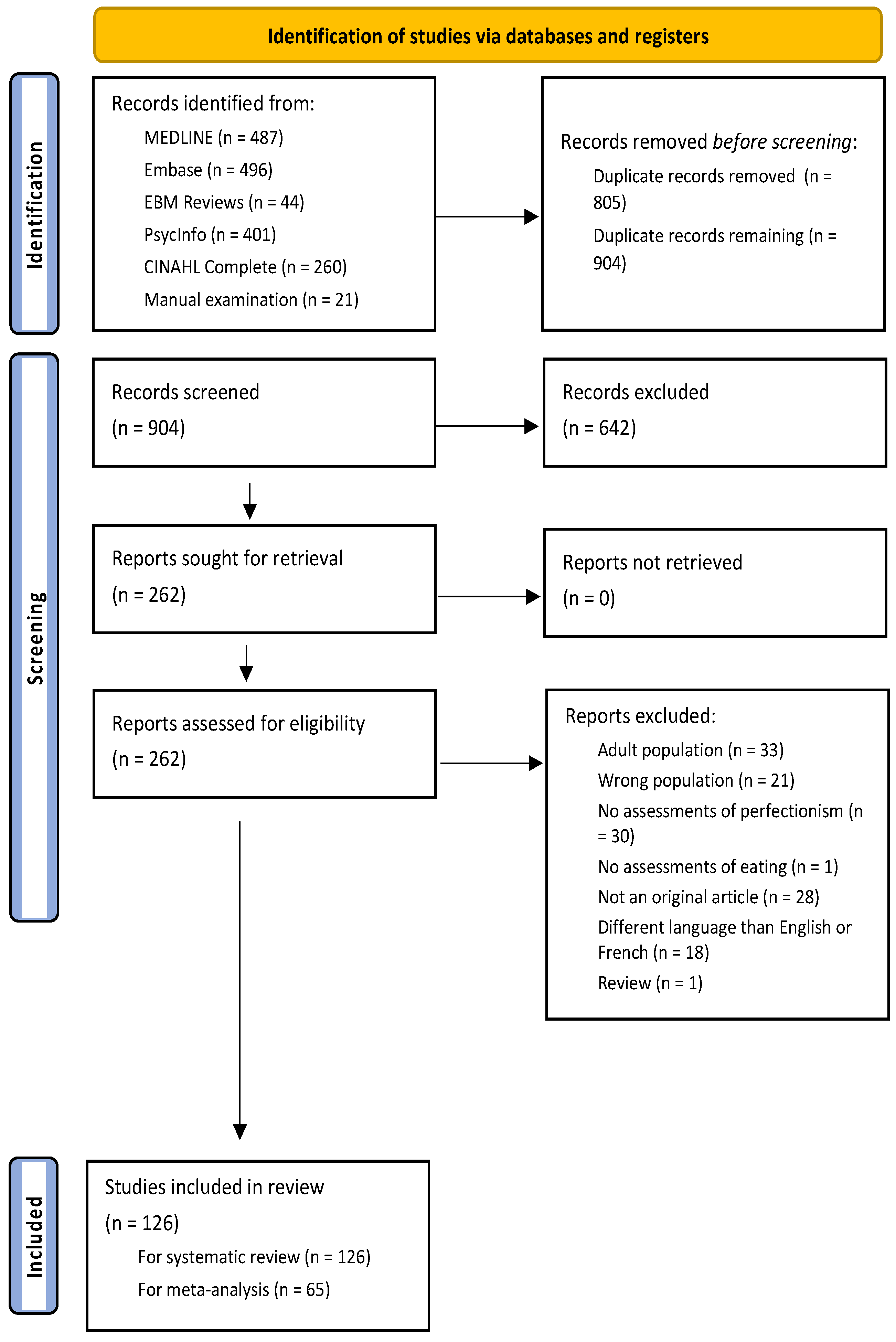
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Statistical Analysis
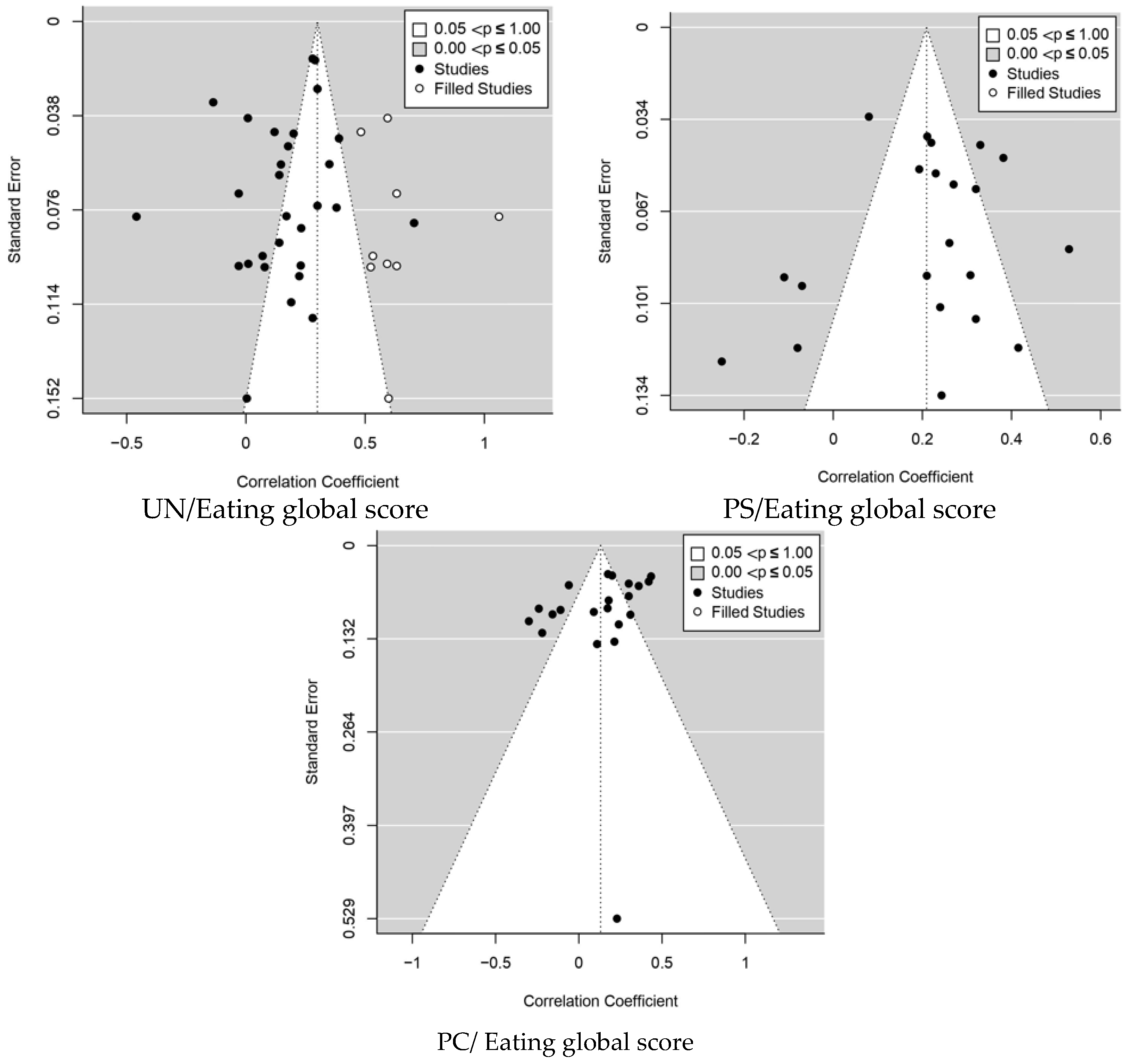
2.4. Publication Bias
3. Results
3.1. Systematic Search and Meta-Analysis Results
3.2. Magnitude of the Relationship between Perfectionism and Eating-Related Symptoms during Childhood and Adolescence
3.2.1. Studies Assessing Eating Disorder Global Score



3.2.2. Studies Assessing Eating-related Symptoms
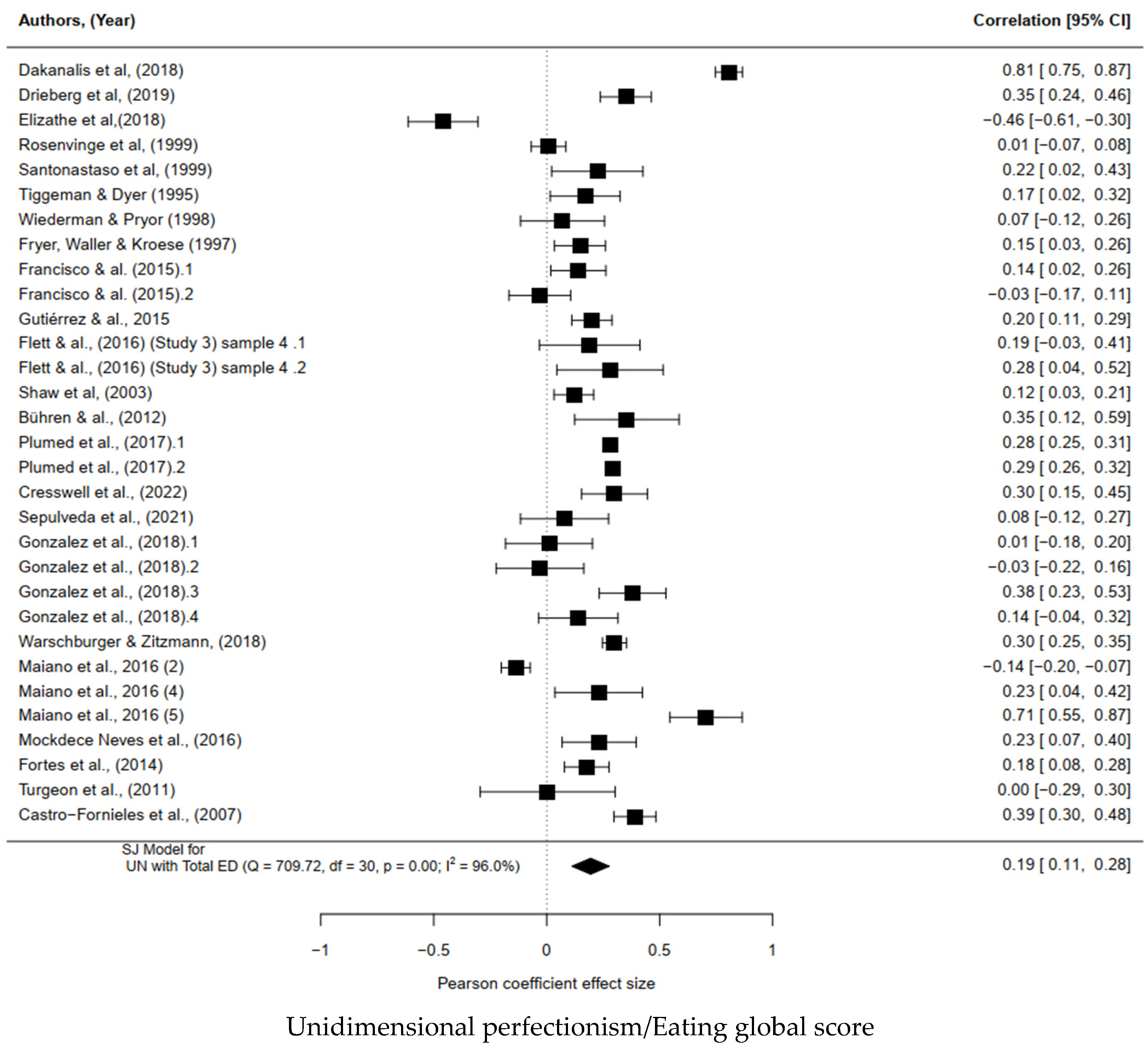
Unidimensional Perfectionism
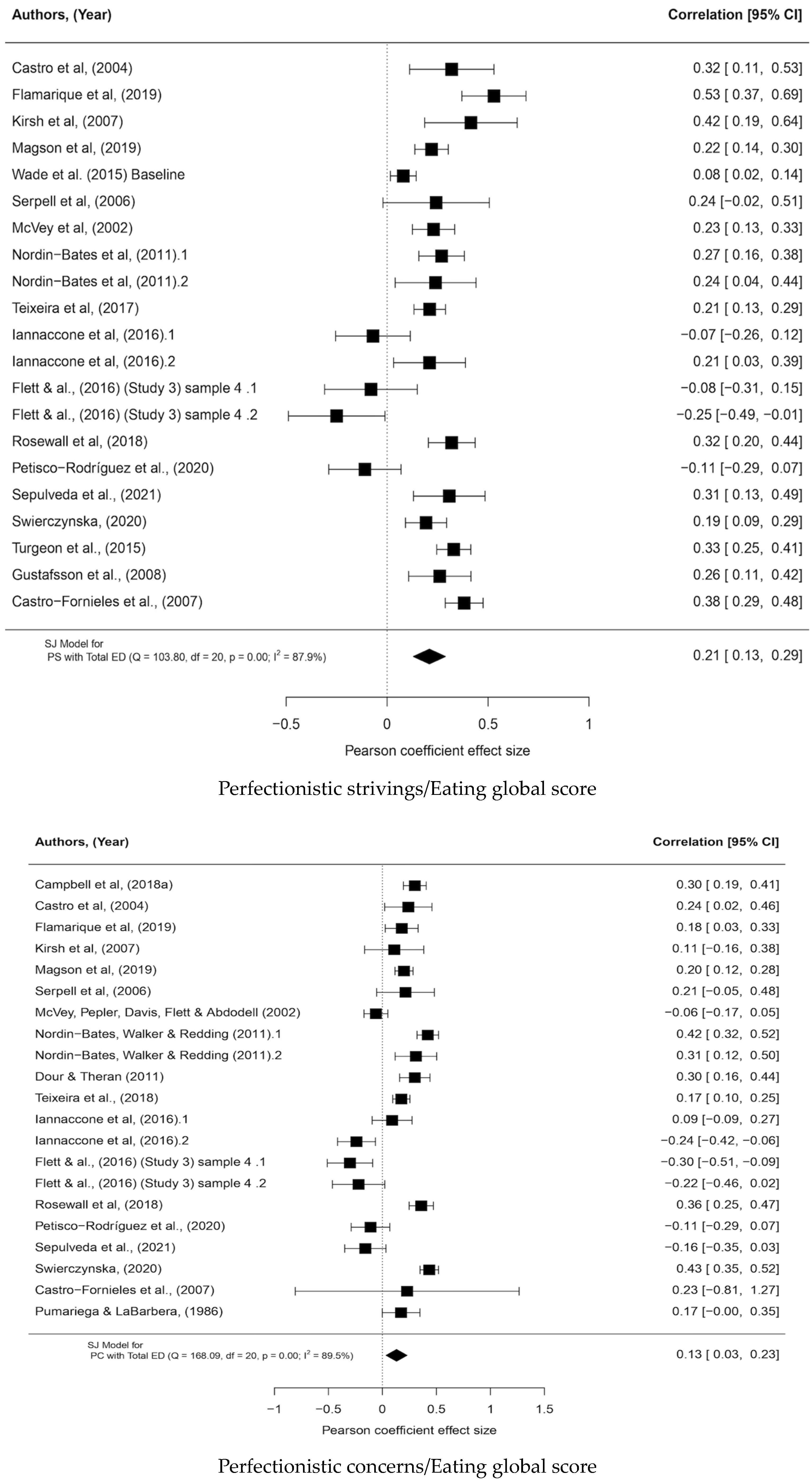
Perfectionistic Strivings
Perfectionistic Concerns
3.2.3. Subgroups Analysis
Associations in Community Samples
Associations in Clinical Samples
Associations in Samples with a Mean Age below 14
Associations in Samples with a Mean Age above 14
3.3. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 68, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.L.; Byrne, S.M.; Oddy, W.H.; Crosby, R.D. DSM-IV-TR and DSM-5 eating disorders in adolescents: Prevalence, stability, and psychosocial correlates in a population-based sample of male and female adolescents. J. Abnorm Psychol. 2013, 122, 720–732. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Marti, C.N.; Rohde, P. Prevalence, incidence, impairment, and course of the proposed DSM-5 eating disorder diagnoses in an 8-year prospective community study of young women. J. Abnorm. Psychol. 2013, 122, 445–457. [Google Scholar] [CrossRef]
- Marzilli, E.; Cerniglia, L.; Cimino, S. A narrative review of binge eating disorder in adolescence: Prevalence, impact, and psychological treatment strategies. Adolesc. Health Med. Ther. 2018, 9, 17–30. [Google Scholar] [CrossRef]
- Larson, N.I.; Neumark-Sztainer, D.; Story, M. Weight control behaviors and dietary intake among adolescents and young adults: Longitudinal findings from Project EAT. J. Am. Diet. Assoc. 2009, 109, 1869–1877. [Google Scholar] [CrossRef]
- McCabe, M.P.; Ricciardelli, L.A. Body image and strategies to lose weight and increase muscle among boys and girls. Health Psychol. 2003, 22, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Strahler, J. Sex differences in orthorexic eating behaviors: A systematic review and meta-analytical integration. Nutrition 2019, 67–68, 110534. [Google Scholar] [CrossRef]
- Smink, F.R.; van Hoeken, D.; Hoek, H.W. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef]
- Marengo, D.; Longobardi, C.; Fabris, M.A.; Settanni, M. Highly-visual social media and internalizing symptoms in adolescence: The mediating role of body image concerns. Comput. Hum. Behav. 2018, 82, 63–69. [Google Scholar] [CrossRef]
- Jaworska, N.; MacQueen, G. Adolescence as a unique developmental period. J. Psychiatry Neurosci. 2015, 40, 291–293. [Google Scholar] [CrossRef]
- Wade, T.D.; Wilksch, S.M.; Paxton, S.J.; Byrne, S.M.; Austin, S.B. How perfectionism and ineffectiveness influence growth of eating disorder risk in young adolescent girls. Behav. Res. Ther. 2015, 66, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Boone, L.; Soenens, B.; Luyten, P. When or why does perfectionism translate into eating disorder pathology? A longitudinal examination of the moderating and mediating role of body dissatisfaction. J. Abnorm. Psychol. 2014, 123, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Sehm, M.; Warschburger, P. Prospective Associations Between Binge Eating and Psychological Risk Factors in Adolescence. J. Clin. Child Adolesc. Psychol. 2018, 47, 770–784. [Google Scholar] [CrossRef] [PubMed]
- Cena, H.; Barthels, F.; Cuzzolaro, M.; Bratman, S.; Brytek-Matera, A.; Dunn, T.; Varga, M.; Missbach, B.; Donini, L.M. Definition and diagnostic criteria for orthorexia nervosa: A narrative review of the literature. Eat. Weight. Disord. 2019, 24, 209–246. [Google Scholar] [CrossRef] [PubMed]
- Curran, T.; Hill, A.P. Perfectionism is increasing over time: A meta-analysis of birth cohort differences from 1989 to 2016. Psychol. Bull. 2019, 145, 410–429. [Google Scholar] [CrossRef]
- Frost, R.O.; Marten, P.; Lahart, C.; Rosenblate, R. The Dimensions of Perfectionism. Cogn. Ther. Res. 1990, 14, 449–468. [Google Scholar] [CrossRef]
- Hewitt, P.L.; Flett, G.L. Perfectionism in the self and social contexts: Conceptualization, assessment, and association with psychopathology. J. Pers. Soc. Psychol. 1991, 60, 456–470. [Google Scholar] [CrossRef]
- Limburg, K.; Watson, H.J.; Hagger, M.S.; Egan, S.J. The Relationship Between Perfectionism and Psychopathology: A Meta-Analysis. J. Clin. Psychol. 2017, 73, 1301–1326. [Google Scholar] [CrossRef]
- Drieberg, H.; McEvoy, P.M.; Hoiles, K.J.; Shu, C.Y.; Egan, S.J. An examination of direct, indirect and reciprocal relationships between perfectionism, eating disorder symptoms, anxiety, and depression in children and adolescents with eating disorders. Eat. Behav. 2019, 32, 53–59. [Google Scholar] [CrossRef]
- Flamarique, I.; Plana, M.T.; Castro-Fornieles, J.; Borràs, R.; Moreno, E.; Lázaro, L. Comparison of Perfectionism Dimensions in Adolescents with Anorexia Nervosa or Obsessive-Compulsive Disorder. Can. Acad. Child Adolesc. Psychiatry 2019, 28, 45–54. [Google Scholar]
- Magson, N.R.; Oar, E.L.; Fardouly, J.; Johnco, C.J.; Rapee, R.M. The Preteen Perfectionist: An Evaluation of the Perfectionism Social Disconnection Model. Child Psychiatry Hum. Dev. 2019, 50, 960–974. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Boone, L.; Vansteenkiste, M.; Soenens, B. Psychological need frustration as a transdiagnostic process in associations of self-critical perfectionism with depressive symptoms and eating pathology. J. Clin. Psychol. 2018, 74, 1775–1790. [Google Scholar] [CrossRef] [PubMed]
- Westerberg, J.; Edlund, B.; Ghaderi, A. Risk and protective factors for disturbed eating: A 7-year longitudinal study of eating attitudes and psychological factors in adolescent girls and their parents. Eat. Weight Disord. 2010, 15, e208–e218. [Google Scholar] [CrossRef]
- Westerberg, J.; Edlund, B.; Ghaderi, A. A 2-year longitudinal study of eating attitudes, BMI, perfectionism, asceticism and family climate in adolescent girls and their parents. Eat. Weight Disord. 2008, 13, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.; Shu, C.Y.; Hoiles, K.J.; Clarke, P.J.F.; Watson, H.J.; Dunlop, P.D.; Egan, S.J. Perfectionism is associated with higher eating disorder symptoms and lower remission in children and adolescents diagnosed with eating disorders. Eat. Behav. 2018, 30, 55–60. [Google Scholar] [CrossRef]
- Santonastaso, P.; Friederici, S.; Favaro, A. Full and partial syndromes in eating disorders: A 1-year prospective study of risk factors among female students. Psychopathology 1999, 32, 50–56. [Google Scholar] [CrossRef]
- Polivy, J.; Herman, C.P. Causes of eating disorders. Annu. Rev. Psychol. 2002, 53, 187–213. [Google Scholar] [CrossRef]
- Vacca, M.; Ballesio, A.; Lombardo, C. The relationship between perfectionism and eating-related symptoms in adolescents: A systematic review. Eur. Eat. Disord. Rev. 2020, 29, 32–51. [Google Scholar] [CrossRef]
- Curzio, O.; Maestro, S.; Rossi, G.; Calderoni, S.; Giombini, L.; Scardigli, S.; Ragione, L.D.; Muratori, F. Transdiagnostic vs. disorder-focused perspective in children and adolescents with eating disorders: Findings from a large multisite exploratory study. Eur. Psychiatry 2018, 49, 81–93. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J. Clin. Epidemiol. 2021, 134, 178–189. [Google Scholar] [CrossRef]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Veritas Health Innovation. H. Covidence Systematic Review Software. 2023. Available online: www.covidence.org (accessed on 2 February 2023).
- Silverii, G.A.; Benvenuti, F.; Morandin, G.; Ricca, V.; Monami, M.; Mannucci, E.; Rotella, F. Eating psychopathology in ballet dancers: A meta-analysis of observational studies. Eat. Weight Disord. 2022, 27, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Chapa, D.A.N.; Johnson, S.N.; Richson, B.N.; Bjorlie, K.; Won, Y.Q.; Nelson, S.V.; Ayres, J.; Jun, D.; Forbush, K.T.; Christensen, K.A.; et al. Eating-disorder psychopathology in female athletes and non-athletes: A meta-analysis. Int. J. Eat. Disord. 2022, 55, 861–885. [Google Scholar] [CrossRef] [PubMed]
- Prnjak, K.; Jukic, I.; Tufano, J.J. Perfectionism, Body Satisfaction and Dieting in Athletes: The Role of Gender and Sport Type. Sports 2019, 7, 181. [Google Scholar] [CrossRef]
- Forsberg, S.; Lock, J. The relationship between perfectionism, eating disorders and athletes: A review. Minerva Pediatr 2006, 58, 525–536. [Google Scholar]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Herzog, R.; Alvarez-Pasquin, M.J.; Diaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, A. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2001; p. 247. [Google Scholar]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- IntHout, J.; Ioannidis, J.P.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med. Res. Methodol. 2014, 14, 25. [Google Scholar] [CrossRef]
- Blum, R.W.; Astone, N.M.; Decker, M.R.; Mouli, V.C. A conceptual framework for early adolescence: A platform for research. Int. J. Adolesc. Med. Health 2014, 26, 321–331. [Google Scholar] [CrossRef]
- Barrett, D.E. The Three Stages of Adolescence. High Sch. J. 1996, 79, 333–339. [Google Scholar]
- Rosenthal, R. The file drawer problem and tolerance for null results. Psychol. Bull. 1979, 86, 638–641. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Garner, D.M.; Olmsted, M.P. Scoring the Eating Disorder Inventory. Am. J. Psychiatry 1986, 143, 680-a. [Google Scholar] [CrossRef] [PubMed]
- Flett, G.L.; Hewitt, P.L.; Besser, A.; Su, C.; Vaillancourt, T.; Boucher, D.; Munro, Y.; Davidson, L.A.; Gale, O. The Child–Adolescent Perfectionism Scale:Development, Psychometric Properties, and Associations With Stress, Distress, and Psychiatric Symptoms. J. Psychoeduc. Assess. 2016, 34, 634–652. [Google Scholar] [CrossRef]
- Hewitt, P.L.; Flett, G.L.; Turnbull-Donovan, W.; Mikail, S.F. The Multidimensional Perfectionism Scale: Reliability, validity, and psychometric properties in psychiatric samples. Psychol. Assess. 1991, 3, 464–468. [Google Scholar] [CrossRef]
- Dakanalis, A.; Colmegna, F.; Zanetti, M.A.; Di Giacomo, E.; Riva, G.; Clerici, M. Evaluation of the DSM-5 Severity Specifier for Bulimia Nervosa in Treatment-Seeking Youth. Child Psychiatry Hum. Dev. 2018, 49, 137–145. [Google Scholar] [CrossRef]
- Elizathe, L.S.; Arana, F.G.; Rutsztein, G. A cross-sectional model of eating disorders in Argentinean overweight and obese children. Eat. Weight Disord. 2018, 23, 125–132. [Google Scholar] [CrossRef]
- Rosenvinge, J.H.; Borgen, J.S.; Börresen, R. The prevalence and psychological correlates of anorexia nervosa, bulimia nervosa and binge eating among 15-yr-old students: A controlled epidemiological study. Eur. Eat. Disord. Rev. 1999, 7, 382–391. [Google Scholar] [CrossRef]
- Tiggemann, M.; Dyer, G.M. Ideal body shape preferences and eating disorder scores in adolescent women. Psychol. Health 1995, 10, 345–347. [Google Scholar] [CrossRef]
- Wiederman, M.W.; Pryor, T. The Relationship Between Substance Use and Clinical Characteristics Among Adolescent Girls with Anorexia Nervosa or Bulimia Nervosa. J. Child Adolesc. Subst. Abuse 1998, 6, 39–47. [Google Scholar] [CrossRef]
- Fryer, S.; Waller, G.; Kroese, B.S. Stress, coping, and disturbed eating attitudes in teenage girls. Int. J. Eat. Disord. 1997, 22, 427–436. [Google Scholar] [CrossRef]
- Francisco, R.; Espinoza, P.; González, M.L.; Penelo, E.; Mora, M.; Rosés, R.; Raich, R.M. Body dissatisfaction and disordered eating among Portuguese and Spanish adolescents: The role of individual characteristics and internalisation of sociocultural ideals. J. Adolesc. 2015, 41, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, T.; Espinoza, P.; Penelo, E.; Mora, M.; González, M.L.; Rosés, R.; Raich, R.M. Association of biological, psychological and lifestyle risk factors for eating disturbances in adolescents. J. Health Psychol. 2015, 20, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Shaw, H.E.; Stice, E.; Springer, D.W. Perfectionism, body dissatisfaction, and self-esteem in predicting bulimic symptomatology: Lack of replication. Int. J. Eat Disord. 2004, 36, 41–47. [Google Scholar] [CrossRef]
- Buhren, K.; Mainz, V.; Herpertz-Dahlmann, B.; Schäfer, K.; Kahraman-Lanzerath, B.; Lente, C.; Konrad, K. Cognitive flexibility in juvenile anorexia nervosa patients before and after weight recovery. J. Neural. Transm. 2012, 119, 1047–1057. [Google Scholar] [CrossRef]
- Plumed, J.; Gimeno, N.; Barberá, M.; Ruiz, E.; Conesa, L.; Rojo-Bofill, L.M.; Livianos, L.; Rojo, L. Teasing as a risk factor for abnormal eating behaviours: A prospective study in an adolescent population. Rev. De Psiquiatr. Y Salud Ment. 2019, 12, 17–27. [Google Scholar] [CrossRef]
- Cresswell, C.; Watson, H.J.; Jones, E.; Howell, J.A.; Egan, S.J. The role of compulsive exercise in the relationship between perfectionism and eating disorder pathology in underweight adolescents with eating disorders. Eat. Behav. 2022, 47, 101683. [Google Scholar] [CrossRef]
- Sepulveda, A.R.; Moreno-Encinas, A.; Martínez-Huertas, J.A.; Anastasiadou, D.; Nova, E.; Marcos, A.; Gómez-Martínez, S.; Villa-Asensi, J.R.; Mollejo, E.; Graell, M. Toward a Biological, Psychological and Familial Approach of Eating Disorders at Onset: Case-Control ANOBAS Study. Front. Psychol. 2021, 12, 714414. [Google Scholar] [CrossRef]
- Gonzalez, M.L.; Penelo, E.; Espinoza, P.; Francisco, R.; Mora, M.; Gutierrez, T.; Raich, R.M. Body dissatisfaction and disordered eating attitudes among adolescents from Portugal and Spain. Behav. Psychol. 2018, 26, 323–335. [Google Scholar]
- Warschburger, P.; Zitzmann, J. The Efficacy of a Universal School-Based Prevention Program for Eating Disorders among German Adolescents: Results from a Randomized-Controlled Trial. J. Youth Adolesc. 2018, 47, 1317–1331. [Google Scholar] [CrossRef] [PubMed]
- Maiano, C.; Morin, A.J.; Monthuy-Blanc, J.; Garbarino, J.-M.; Ninot, G. Development and validity of a very short form of the Eating Disorder Inventory. Compr. Psychiatry 2016, 65, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Mockdece Neves, C.; Meireles, J.F.F.; Carvalho, P.H.B.D.; Almeida, S.S.; Ferreira, M.E.C. Body dissatisfaction among artistic gymnastics adolescent athletes and non-athletes. Braz. J. Kineanthropometry Hum. Perform. 2016, 18, 82–92. [Google Scholar]
- Fortes, L.S.; Cipriani, F.M.; Almeida, S.D.S.; Ferreira, M.E.C. Eating disorder symptoms: Association with perfectionism traits in male adolescents. Rev. De Psiquiatr. Clin. 2014, 41, 117–120. [Google Scholar] [CrossRef][Green Version]
- Turgeon, M.E.; Forget, J.; Senecal, C. Eating disorders, depression, self-esteem and perfectionism in children. Psychol. Pract. 2011, 17, 315–328. [Google Scholar]
- Castro-Fornieles, J.; Gual, P.; Lahortiga-Ramos, F.; Gila, A.; Casulà, V.; Fuhrmann, C.; Imirizaldu, M.; Saura, B.; Martínez, E.; Toro, J. Self-oriented perfectionism in eating disorders. Int. J. Eat. Disord. 2007, 40, 562–568. [Google Scholar] [CrossRef]
- Castro, J.; Gila, A.; Gual, P.; Lahortiga, F.; Saura, B.; Toro, J. Perfectionism dimensions in children and adolescents with anorexia nervosa. J. Adolesc. Health 2004, 35, 392–398. [Google Scholar] [CrossRef]
- Kirsh, G.; McVey, G.; Tweed, S.; Katzman, D.K. Psychosocial Profiles of Young Adolescent Females Seeking Treatment for an Eating Disorder. J. Adolesc. Health 2007, 40, 351–356. [Google Scholar] [CrossRef]
- Serpell, L.; Hirani, V.; Willoughby, K.; Neiderman, M.; Lask, B. Personality or pathology? Obsessive–compulsive symptoms in children and adolescents with anorexia nervosa. Eur. Eat. Disord. Rev. 2006, 14, 404–413. [Google Scholar]
- McVey, G.L.; Pepler, D.; Davis, R.; Flett, G.L.; Abdolell, M. Risk and Protective Factors Associated with Disordered Eating During Early Adolescence. J. Early Adolesc. 2002, 22, 75–95. [Google Scholar] [CrossRef]
- Nordin-Bates, S.M.; Walker, I.J.; Redding, E. Correlates of disordered eating attitudes among male and female young talented dancers: Findings from the UK centres for advanced training. Eat. Disord. 2011, 19, 211–233. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, M.D.; Pereira, A.T.; Marques, M.V.; Saraiva, J.M.; de Macedo, A.F. Eating behaviors, body image, perfectionism, and self-esteem in a sample of Portuguese girls. Braz. J. Psychiatry 2016, 38, 135–140. [Google Scholar] [CrossRef]
- Iannaccone, M.; D’Olimpio, F.; Cella, S.; Cotrufo, P. Self-esteem, body shame and eating disorder risk in obese and normal weight adolescents: A mediation model. Eat. Behav. 2016, 21, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Rosewall, J.K.; Gleaves, D.H.; Latner, J.D. An examination of risk factors that moderate the body dissatisfaction-eating pathology relationship among New Zealand adolescent girls. J. Eat. Disord. 2018, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Petisco-Rodriguez, C.; Sanchez-Sanchez, L.C.; Fernandez-Garcia, R.; Sanchez-Sanchez, J.; Garcia-Montes, J.M. Disordered Eating Attitudes, Anxiety, Self-Esteem and Perfectionism in Young Athletes and Non-Athletes. Int. J. Environ. Res. Public Health 2020, 17, 6754. [Google Scholar] [CrossRef]
- Swierczynska, J. Coexistence of the features of perfectionism and anorexia readiness in school youth. Psychiatr. Pol. 2020, 54, 239–252. [Google Scholar] [CrossRef]
- Turgeon, M.-E.; Forget, J.; Begin, J. Adaptation and psychometric testing of the self-oriented perfectionism subscale of the Positive and Negative Perfectionism Scale. J. Behav. Cogn. Ther. 2015, 25, 148–158. [Google Scholar]
- Gustafsson, S.A.; Edlund, B.; Kjellin, L.; Norring, C. Personal standards, self-evaluation and perceived benefits of thinness in girls and young women with disturbed eating. Eur. Eat. Disord. Rev. 2008, 16, 463–471. [Google Scholar] [CrossRef]
- Dour, H.J.; Theran, S.A. The interaction between the superhero ideal and maladaptive perfectionism as predictors of unhealthy eating attitudes and body esteem. Body Image 2011, 8, 93–96. [Google Scholar] [CrossRef]
- Pumariega, A.J.; LaBarbera, J.D. Eating attitudes and personality variables in a nonclinical sample. Int. J. Eat. Disord. 1986, 5, 285–294. [Google Scholar] [CrossRef]
- Jones, E.J.; Egan, S.J.; Howell, J.A.; Hoiles, K.J.; Mazzucchelli, T.G. An examination of the transdiagnostic cognitive-behavioural model of eating disorders in adolescents. Eat. Behav. 2020, 39, 101445. [Google Scholar] [CrossRef] [PubMed]
- Boone, L.; Vansteenkiste, M.; Soenens, B.; Van der Kaap-Deeder, J.; Verstuyf, J. Self-critical perfectionism and binge eating symptoms: A longitudinal test of the intervening role of psychological need frustration. J. Couns. Psychol. 2014, 61, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.F.; Vitousek, K.M. Personality Variables and Eating Pathology. Psychiatr. Clin. North. Am. 2019, 42, 105–119. [Google Scholar] [CrossRef]
- Smith, M.M.; Vidovic, V.; Sherry, S.B.; Stewart, S.H.; Saklofske, D.H. Are perfectionism dimensions risk factors for anxiety symptoms? A meta-analysis of 11 longitudinal studies. Anxiety Stress Coping 2018, 31, 4–20. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.M.; Sherry, S.B.; Ray, C.; Hewitt, P.L.; Flett, G.L. Is perfectionism a vulnerability factor for depressive symptoms, a complication of depressive symptoms, or both? A meta-analytic test of 67 longitudinal studies. Clin. Psychol. Rev. 2021, 84, 101982. [Google Scholar] [CrossRef]
- Smith, K.E.; Mason, T.B.; Crosby, R.D.; Cao, L.; Leonard, R.C.; Wetterneck, C.T.; Smith, B.E.R.; Farrell, N.R.; Riemann, B.C.; Wonderlich, S.A.; et al. A comparative network analysis of eating disorder psychopathology and co-occurring depression and anxiety symptoms before and after treatment. Psychol. Med. 2019, 49, 314–324. [Google Scholar] [CrossRef]
- Smith, M.M.; Sherry, S.B.; Chen, S.; Saklofske, D.H.; Mushquash, C.; Flett, G.L.; Hewitt, P.L. The perniciousness of perfectionism: A meta-analytic review of the perfectionism-suicide relationship. J. Pers. 2018, 86, 522–542. [Google Scholar] [CrossRef]
- Flament, M.F.; Henderson, K.; Buchholz, A.; Obeid, N.; Nguyen, H.N.; Birmingham, M.; Goldfield, G. Weight Status and DSM-5 Diagnoses of Eating Disorders in Adolescents From the Community. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 403–411.e2. [Google Scholar] [CrossRef]
- Smink, F.R.; van Hoeken, D.; Oldehinkel, A.J.; Hoek, H.W. Prevalence and severity of DSM-5 eating disorders in a community cohort of adolescents. Int. J. Eat. Disord. 2014, 47, 610–619. [Google Scholar] [CrossRef]
- Hudson, J.I.; Hiripi, E.; Pope, H.G., Jr.; Kessler, R.C. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef]
- Rivière, J.; Douilliez, C. Perfectionism, rumination, and gender are related to symptoms of eating disorders: A moderated mediation model. Personal. Individ. Differ. 2017, 116, 63–68. [Google Scholar] [CrossRef]
- Swierczynska, J. The image of perfectionism in youth with diverse structure and intensity of anorexia readiness. Psychiatr. Pol. 2022, 56, 523–534. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.; Charvin, I.; Da Fonseca, D.; Bat-Pitault, F. Day hospital program for anorexia nervosa in children and adolescents: Assessment, management and specific focus on early onset anorexia nervosa. L’Encephale 2022. [Google Scholar] [CrossRef] [PubMed]
- Mohoric, T.; Pokrajac-Bulian, A.; Anic, P.; Kukic, M.; Mohovic, P. Emotion regulation, perfectionism, and eating disorder symptoms in adolescents: The mediating role of cognitive eating patterns. Curr. Psychol. 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Pamies-Aubalat, L.; Quiles Marcos, Y.; Torregrosa Diez, M.S. Psychosocial profile related to disordered eating attitudes in spanish adolescents. Curr. Psychol. A J. Divers. Perspect. Divers. Psychol. Issues 2022, 1–10. [Google Scholar] [CrossRef]
- Pauls, A.; Dimitropoulos, G.; Marcoux-Louie, G.; Singh, M.; Patten, S.B. Psychological characteristics and childhood adversity of adolescents with atypical anorexia nervosa versus anorexia nervosa. Eat. Disord. 2022, 30, 210–222. [Google Scholar] [CrossRef]
- Schilder, C.M.T.; Sternheim, L.C.; Aarts, E.; van Elburg, A.A.; Danner, U.N. Relationships between educational achievement, intelligence, and perfectionism in adolescents with eating disorders. Int. J. Eat. Disord. 2021, 54, 794–801. [Google Scholar] [CrossRef]
- Schlegl, S.; Smith, K.E.; Vierl, L.; Crosby, R.D.; Moessner, M.; Neumayr, C.; Voderholzer, U. Using network analysis to compare diagnosis-specific and age-specific symptom networks in eating disorders. Int. J. Eat. Disord. 2021, 54, 1463–1476. [Google Scholar] [CrossRef]
- Sander, J.; Moessner, M.; Bauer, S. Depression, Anxiety and Eating Disorder-Related Impairment: Moderators in Female Adolescents and Young Adults. Int. J. Environ. Res. Public Health 2021, 18, 2779. [Google Scholar] [CrossRef]
- Welch, H.A.; Agras, W.S.; Lock, J.; Halmi, K.A. Perfectionism, anorexia nervosa, and family treatment: How perfectionism changes throughout treatment and predicts outcomes. Int. J. Eat. Disord. 2020, 53, 2055–2060. [Google Scholar] [CrossRef]
- Obeid, N.; Valois, D.D.; Bedford, S.; Norris, M.L.; Hammond, N.G.; Spettigue, W. Asceticism, perfectionism and overcontrol in youth with eating disorders. Eat. Weight Disord. 2020, 26, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Shu, C.Y.; Watson, H.J.; Anderson, R.A.; Wade, T.D.; Kane, R.T.; Egan, S.J. A randomized controlled trial of unguided internet cognitive behaviour therapy for perfectionism in adolescents: Impact on risk for eating disorders. Behav. Res. Ther. 2019, 120, 103429. [Google Scholar] [CrossRef] [PubMed]
- Blasczyk-Schiep, S.; Adamczewska, K.; Funez Sokola, K. Subclinical eating disorder symptoms and positive vs. negative affect in high school students: The mediating role of self-regulation. Curr. Issues Personal. Psychol. 2019, 7, 120–131. [Google Scholar] [CrossRef]
- Christian, C.; Brosof, L.C.; Vanzhula, I.A.; Williams, B.M.; Shankar Ram, S.; Levinson, C.A. Implementation of a dissonance-based, eating disorder prevention program in Southern, all-female high schools. Body Image 2019, 30, 26–34. [Google Scholar] [CrossRef]
- Ramon-Jarne, F.J.; Jurado, D.; Jimenez-Fernandez, S.; Gutierrez-Rojas, L.; Martinez-Ortega, J.M.; Gurpegui, M. Disordered eating behaviors among Christian and Muslim adolescents in Ceuta, a multicultural town. Psychiatry Res. 2019, 272, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Keery, H.; LeMay-Russell, S.; Barnes, T.L.; Eckhardt, S.; Peterson, C.B.; Lesser, J.; Gorrell, S.; Le Grange, D. Attributes of children and adolescents with avoidant/restrictive food intake disorder. J. Eat. Disord. 2019, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Stornaes, A.V.; Rosenvinge, J.H.; Sundgot-Borgen, J.; Pettersen, G.; Friborg, O. Profiles of Perfectionism Among Adolescents Attending Specialized Elite- and Ordinary Lower Secondary Schools: A Norwegian Cross-Sectional Comparative Study. Front. Psychol. 2019, 10, 2039. [Google Scholar] [CrossRef] [PubMed]
- Cella, S.; Iannaccone, M.; Cotrufo, P. Does body shame mediate the relationship between parental bonding, self-esteem, maladaptive perfectionism, body mass index and eating disorders? A structural equation model. Eat. Weight Disord. 2019, 25, 667–678. [Google Scholar] [CrossRef]
- Morgan-Lowes, K.L.; Clarke, P.J.F.; Hoiles, K.J.; Shu, C.Y.; Watson, H.J.; Dunlop, P.D.; Egan, S.J. The relationships between perfectionism, anxiety and depression across time in paediatric eating disorders. Eat. Behav. 2019, 34, 101305. [Google Scholar] [CrossRef]
- Hurst, K.; Zimmer-Gembeck, M. Family-based treatment with cognitive behavioural therapy for anorexia. Clin. Psychol. 2019, 23, 61–70. [Google Scholar] [CrossRef]
- Gan, W.Y.; Mohamad, N.; Law, L.S. Factors Associated with Binge Eating Behavior among Malaysian Adolescents. Nutrients 2018, 10, 66. [Google Scholar] [CrossRef] [PubMed]
- Izydorczyk, B.; Sitnik-Warchulska, K. Sociocultural Appearance Standards and Risk Factors for Eating Disorders in Adolescents and Women of Various Ages. Front. Psychol. 2018, 9, 429. [Google Scholar] [CrossRef]
- Shahyad, S.; Pakdaman, S.; Shokri, O.; Saadat, S.H. The Role of Individual and Social Variables in Predicting Body Dissatisfaction and Eating Disorder Symptoms among Iranian Adolescent Girls: An Expanding of the Tripartite Influence Mode. Eur. J. Transl. Myol. 2018, 28, 7277. [Google Scholar] [CrossRef] [PubMed]
- van Noort, B.M.; Lohmar, S.K.; Pfeiffer, E.; Lehmkuhl, U.; Winter, S.M.; Kappel, V. Clinical characteristics of early onset anorexia nervosa. Eur. Eat. Disord. Rev. 2018, 26, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Wilksch, S.M.; Paxton, S.J.; Byrne, S.M.; Austin, S.B.; O’Shea, A.; Wade, T.D. Outcomes of three universal eating disorder risk reduction programs by participants with higher and lower baseline shape and weight concern. Int. J. Eat. Disord. 2017, 50, 66–75. [Google Scholar] [CrossRef]
- Levallius, J.; Collin, C.; Birgegard, A. Now you see it, Now you don’t: Compulsive exercise in adolescents with an eating disorder. J. Eat. Disord. 2017, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Vall, E.; Wade, T.D. Predictors and moderators of outcomes and readmission for adolescent inpatients with anorexia nervosa: A pilot study. Clin. Psychol. 2017, 21, 143–152. [Google Scholar] [CrossRef]
- Varela-Besteiro, O.; Serrano-Troncoso, E.; Rodriguez-Vicente, V.; Curet-Santisteban, M.; Conangla-Rosello, G.; Cecilia-Costa, R.; Carulla-Roig, M.; Matali-Costa, J.L.; Dolz-Abadia, M. Suicidal ideation and self-injurious behavior in adolescents with eating disorders. Actas Esp. Psiquiatr. 2017, 45, 157–166. [Google Scholar]
- De Caro, E.F.; Di Blas, L. A prospective study on the reciprocal influence between personality and attitudes, behaviors, and psychological characteristics salient in eating disorders in a sample of non-clinical adolescents. Eat. Disord. 2016, 24, 453–468. [Google Scholar] [CrossRef][Green Version]
- Kerr, C.; Watkins, B.; Jones, F.W. Inflated responsibility and perfectionism in child and adolescent anorexia. Adv. Eat. Disord. 2016, 4, 309–314. [Google Scholar] [CrossRef][Green Version]
- Arcelus, J.; García-Dantas, A.; Sánchez- Martín, M.; Del Río, C. Influence of perfectionism on variables associated to eating disorders in dance students. Rev. Psicol. Deporte 2015, 24, 297–303. [Google Scholar]
- Sehm, M.; Warschburger, P. The Specificity of Psychological Factors Associated with Binge Eating in Adolescent Boys and Girls. J. Abnorm. Child Psychol. 2015, 43, 1563–1571. [Google Scholar] [CrossRef] [PubMed]
- Wade, T.D.; O’Shea, A. DSM-5 unspecified feeding and eating disorders in adolescents: What do they look like and are they clinically significant? Int. J. Eat. Disord. 2015, 48, 367–374. [Google Scholar] [CrossRef]
- Formby, P.; Watson, H.J.; Hilyard, A.; Martin, K.; Egan, S.J. Psychometric properties of the Compulsive Exercise Test in an adolescent eating disorder population. Eat. Behav. 2014, 15, 555–557. [Google Scholar] [CrossRef]
- Goodwin, H.; Haycraft, E.; Meyer, C. Psychological risk factors for compulsive exercise: A longitudinal investigation of adolescent boys and girls. Personal. Individ. Differ. 2014, 68, 83–86. [Google Scholar] [CrossRef]
- Boone, L.; Claes, L.; Luyten, P. Too strict or too loose? Perfectionism and impulsivity: The relation with eating disorder symptoms using a person-centered approach. Eat. Behav. 2014, 15, 17–23. [Google Scholar] [CrossRef]
- Fairweather-Schmidt, A.K.; Wade, T.D. DSM-5 eating disorders and other specified eating and feeding disorders: Is there a meaningful differentiation? Int. J. Eat. Disord. 2014, 47, 524–533. [Google Scholar] [CrossRef]
- Lyman, E.L.; Luthar, S.S. Further Evidence on the “Costs of Privilege”: Perfectionism in High-Achieving Youth at Socioeconomic Extremes. Psychol. Sch. 2014, 51, 913–930. [Google Scholar] [CrossRef]
- Upadhyah, A.; Misra, R.; Parchwani, D.; Maheria, P. Prevalence and risk factors for eating disorders in Indian adolescent females. Natl. J. Physiol. Pharm. Pharmacol. 2014, 4, 153–157. [Google Scholar] [CrossRef]
- Pellicciari, A.; Gualandi, S.; Iero, L.; Monti, M.; Di Pietro, E.; Sacrato, L.; Gualandi, P.; Franzoni, E. Psychometric evaluation of SAFA P Test for eating disorders in adolescents: Comparative validation with EDI-2. Eur. Eat. Disord. Rev. 2012, 20, e108–e113. [Google Scholar] [CrossRef] [PubMed]
- Boone, L.; Soenens, B.; Mouratidis, A.; Vansteenkiste, M.; Verstuyf, J.; Braet, C. Daily fluctuations in perfectionism dimensions and their relation to eating disorder symptoms. J. Res. Pers. 2012, 46, 678–687. [Google Scholar] [CrossRef]
- Ferreiro, F.; Seoane, G.; Senra, C. Gender-related risk and protective factors for depressive symptoms and disordered eating in adolescence: A 4-year longitudinal study. J. Youth Adolesc. 2012, 41, 607–622. [Google Scholar] [CrossRef] [PubMed]
- Wojtowicz, A.E.; von Ranson, K.M. Weighing in on risk factors for body dissatisfaction: A one-year prospective study of middle-adolescent girls. Body Image 2012, 9, 20–30. [Google Scholar] [CrossRef]
- Boone, L.; Soenens, B.; Braet, C. Perfectionism, Body Dissatisfaction, and Bulimic Symptoms: The Intervening Role of Perceived Pressure to be Thin and Thin Ideal Internalization. J. Soc. Clin. Psychol. 2011, 30, 1043–1068. [Google Scholar] [CrossRef]
- Goodwin, H.; Haycraft, E.; Willis, A.M.; Meyer, C. Compulsive exercise: The role of personality, psychological morbidity, and disordered eating. Int. J. Eat. Disord. 2011, 44, 655–660. [Google Scholar] [CrossRef]
- Fan, Y.; Li, Y.; Liu, A.; Hu, X.; Ma, G.; Xu, G. Associations between body mass index, weight control concerns and behaviors, and eating disorder symptoms among non-clinical Chinese adolescents. BMC Public Health 2010, 10, 314. [Google Scholar] [CrossRef]
- Bachar, E.; Gur, E.; Canetti, L.; Berry, E.; Stein, D. Selflessness and perfectionism as predictors of pathological eating attitudes and disorders: A longitudinal study. Eur. Eat. Disord. Rev. 2010, 18, 496–506. [Google Scholar] [CrossRef]
- Bento, C.; Pereira, A.T.; Maia, B.; Marques, M.; Soares, M.J.; Bos, S.; Valente, J.; Gomes, A.; Azevedo, M.H.; Macedo, A. Perfectionism and eating behaviour in Portuguese adolescents. Eur. Eat. Disord. Rev. 2010, 18, 328–337. [Google Scholar] [CrossRef]
- Boone, L.; Soenens, B.; Braet, C.; Goossens, L. An empirical typology of perfectionism in early-to-mid adolescents and its relation with eating disorder symptoms. Behav. Res. Ther. 2010, 48, 686–691. [Google Scholar] [CrossRef]
- Chen, L.J.; Fox, K.R.; Haase, A.M.; Ku, P.W. Correlates of body dissatisfaction among Taiwanese adolescents. Asia Pac. J. Clin. Nutr. 2010, 19, 172–179. [Google Scholar] [PubMed]
- Phillips, R.; Stewart, S.M.; Presnell, K.; Simmons, A.; Kennard, B.D.; Liss, D.; Setliff, S. Psychological variables impacting weight gain rapidity in adolescents hospitalized for eating disorders. Eur. Eat. Disord. Rev. 2010, 18, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Wilksch, S.M.; Wade, T.D. Risk factors for clinically significant importance of shape and weight in adolescent girls. J. Abnorm. Psychol. 2010, 119, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Canals, J.; Sancho, C.; Arija, M.V. Influence of parent’s eating attitudes on eating disorders in school adolescents. Eur. Child Adolesc. Psychiatry 2009, 18, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Custers, K.; Van den Bulck, J. Viewership of pro-anorexia websites in seventh, ninth and eleventh graders. Eur Eat Disord Rev 2009, 17, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, S.A.; Edlund, B.; Kjellin, L.; Norring, C. Risk and protective factors for disturbed eating in adolescent girls—Aspects of perfectionism and attitudes to eating and weight. Eur. Eat. Disord. Rev. 2009, 17, 380–389. [Google Scholar] [CrossRef]
- Wilksch, S.M.; Durbridge, M.R.; Wade, T.D. A preliminary controlled comparison of programs designed to reduce risk of eating disorders targeting perfectionism and media literacy. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 937–947. [Google Scholar] [CrossRef]
- Nilsson, K.; Sundbom, E.; Hagglof, B. A longitudinal study of perfectionism in adolescent onset anorexia nervosa-restricting type. Eur. Eat. Disord. Rev. 2008, 16, 386–394. [Google Scholar] [CrossRef]
- Eddy, K.T.; Tanofsky-Kraff, M.; Thompson-Brenner, H.; Herzog, D.B.; Brown, T.A.; Ludwig, D.S. Eating disorder pathology among overweight treatment-seeking youth: Clinical correlates and cross-sectional risk modeling. Behav. Res. Ther. 2007, 45, 2360–2371. [Google Scholar] [CrossRef]
- Nilsson, K.; Hägglöf, B. Long-term follow-up of adolescent onset anorexia nervosa in northern Sweden. Eur. Eat. Disord. Rev. 2005, 13, 89–100. [Google Scholar] [CrossRef]
- Franko, D.L.; Striegel-Moore, R.H.; Barton, B.A.; Schumann, B.C.; Garner, D.M.; Daniels, S.R.; Schreiber, G.B.; Crawford, P.B. Measuring eating concerns in Black and White adolescent girls. Int. J. Eat. Disord. 2004, 35, 179–189. [Google Scholar] [CrossRef] [PubMed]
- McVey, G.L.; Davis, R.; Tweed, S.; Shaw, B.F. Evaluation of a school-based program designed to improve body image satisfaction, global self-esteem, and eating attitudes and behaviors: A replication study. Int. J. Eat. Disord. 2004, 36, 1–11. [Google Scholar] [CrossRef] [PubMed]
- McCabe, M.P.; Vincent, M.A. The role of biodevelopmental and psychological factors in disordered eating among adolescent males and females. Eur. Eat. Disord. Rev. 2003, 11, 315–328. [Google Scholar] [CrossRef]
- Wiseman, C.V.; Sunday, S.R.; Bortolotti, F.; Halmi, K.A. Primary prevention of eating disorders through attitude change: A two country comparison. Eat. Disord. 2004, 12, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Leung, F.; Wang, J.; Tang, C.W.Y. Psychometric properties and normative data of the Eating Disorder Inventory among 12 to 18 year old Chinese girls in Hong Kong. J. Psychosom. Res. 2004, 57, 59–66. [Google Scholar] [CrossRef]
- Ruggiero, G.M.; Levi, D.; Ciuna, A.; Sassaroli, S. Stress situation reveals an association between perfectionism and drive for thinness. Int. J. Eat. Disord. 2003, 34, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Simmons, J.R.; Smith, G.T.; Hill, K.K. Validation of eating and dieting expectancy measures in two adolescent samples. Int. J. Eat. Disord. 2002, 31, 461–473. [Google Scholar] [CrossRef]
- Tyrka, A.R.; Waldron, I.; Graber, J.A.; Brooks-Gunn, J. Prospective predictors of the onset of anorexic and bulimic syndromes. Int. J. Eat. Disord. 2002, 32, 282–290. [Google Scholar] [CrossRef]
- Wade, T.D.; Lowes, J. Variables associated with disturbed eating habits and overvalued ideas about the personal implications of body shape and weight in a female adolescent population. Int. J. Eat. Disord. 2002, 32, 39–45. [Google Scholar] [CrossRef]
- Cassidy, E.; Allsopp, M.; Williams, T. Obsessive compulsive symptoms at initial presentation of adolescent eating disorders. Eur. Child Adolesc. Psychiatry 1999, 8, 193–199. [Google Scholar] [CrossRef]
- Fulkerson, J.A.; Keel, P.K.; Leon, G.R.; Dorr, T. Eating-disordered behaviors and personality characteristics of high school athletes and nonathletes. Int. J. Eat. Disord. 1999, 26, 73–79. [Google Scholar] [CrossRef]
- Pla, C.; Toro, J. Anorexia nervosa in a Spanish adolescent sample: An 8-year longitudinal study. Acta Psychiatr. Scand. 1999, 100, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H.; Schreiber, G.B.; Lo, A.; Crawford, P.; Obarzanek, E.; Rodin, J. Eating disorder symptoms in a cohort of 11 to 16-year-old black and white girls: The NHLBI growth and health study. Int. J. Eat. Disord. 2000, 27, 49–66. [Google Scholar] [CrossRef]
- Calam, R.; Waller, G. Are eating and psychosocial characteristics in early teenage years useful predictors of eating characteristics in early adulthood? A 7-year longitudinal study. Int. J. Eat. Disord. 1998, 24, 351–362. [Google Scholar] [CrossRef]
- al-Subaie, A.S.; Bamgboye, E.; al-Shammari, S.; al-Sabhan, K.N.; al-Shehri, S.N.; Bannah, A.R. Validity of the Arabic version of the eating disorders inventory (EDI). Br. J. Psychiatry J. Ment. Sci. 1996, 168, 636–640. [Google Scholar] [CrossRef]
- Steiger, H.; Leung, F.Y.K.; Puentes-Neuman, G.; Gottheil, N. Psychosocial profiles of adolescent girls with varying degrees of eating and mood disturbances. Int. J. Eat. Disord. 1992, 11, 121–131. [Google Scholar] [CrossRef]
- Steiger, H.; Puentes-Neuman, G.; Leung, F.Y.K. Personality and family features of adolescent girls with eating symptoms: Evidence for restricter/binger differences in a nonclinical population. Addict. Behav. 1991, 16, 303–314. [Google Scholar] [CrossRef]
- Shore, R.A.; Porter, J.E. Normative and reliability data for 11 to 18 year olds on the eating disorder inventory. Int. J. Eat. Disord. 1990, 9, 201–207. [Google Scholar] [CrossRef]
- Cole, S.H.; Edelman, R.J. Restraint, eating disorders and need to achieve in state and public school subjects. Personal. Individ. Differ. 1987, 8, 475–482. [Google Scholar] [CrossRef]
- Faust, J. Correlates of the Drive for Thinness in Young Female Adolescents. J. Clin. Child Psychol. 1987, 16, 313–319. [Google Scholar] [CrossRef]
- Wells, G.A.; Wells, G.; Shea, B.; Shea, B.; O’Connell, D.; Peterson, J.; Welch Losos, M.; Tugwell, P.; Ga, S.W.; Zello, G.A.; et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Environ. Sci. 2014. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Fourth Edition (DSM-IV); American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Salbach-Andrae, H.; Klinkowski, N.; Holzhausen, M.; Frieler, K.; Bohnekamp, I.; Thiels, C.; Bender, C.; Vandereycken, W. The German version of the Anorectic Behavior Observation Scale (ABOS). Eur. Child Adolesc. Psychiatry 2009, 18, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, K. Conceptualization and Development of the Appearance Perfectionism Scale: Preliminary Evidence for Validity and Utility in a College Student Population. Doctoral Dissertation, University of Michigan, Ann Arbor, MI, USA, 2009. [Google Scholar]
- Slaney, R.B.; Rice, K.G.; Mobley, M.; Trippi, J.; Ashby, J.S. The revised almost perfect scale. Meas. Eval. Couns. Dev. 2001, 34, 130–145. [Google Scholar] [CrossRef]
- Halmi, K.A.; Falk, J.R.; Schwartz, E. Binge-eating and vomiting: A survey of a college population. Psychol. Med. 1981, 11, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Beaudoin, C.; Sainte-Marie, D.M.; Bottamini, G. Traduction et validation canadienne française d’une échelle portant sur l’estime de son corps. Avante 2001, 9, 15–20. [Google Scholar]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Henderson, M.; Freeman, C.P. A self-rating scale for bulimia. The ‘BITE’. Br. J. Psychiatry 1987, 150, 18–24. [Google Scholar] [CrossRef]
- Stice, E. Modeling of eating pathology and social reinforcement of the thin-ideal predict onset of bulimic symptoms. Behav. Res. Ther. 1998, 36, 931–944. [Google Scholar] [CrossRef]
- Conti, M.A.; Cordás, T.A.; Latorre, M.d.R.D.d.O. A study of the validity and reliability of the Brazilian version of the Body Shape Questionnaire (BSQ) among adolescents. Rev. Bras. De Saúde Matern. Infant. 2009, 9, 331–338. [Google Scholar] [CrossRef]
- Thelen, M.H.; Farmer, J.; Wonderlich, S.; Smith, M. A revision of the Bulimia Test: The BULIT--R. Psychol. Assess. 1991, 3, 119–124. [Google Scholar] [CrossRef]
- Cuzzolaro, M.; Vetrone, G.; Marano, G.; Garfinkel, P.E. The Body Uneasiness Test (BUT): Development and validation of a new body image assessment scale. Eat. Weight Disord. 2006, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Flett, G.L.; Hewitt, P.L.; Boucher, D.J.; Davidson, L.A.; Munro, Y. The Child-Adolescent Perfectionism Scale: Development, Validation, and Association with Adjustment; York University: Toronto, ON, Canada, 1992. [Google Scholar]
- Thompson, M.A.; Gray, J.J. Development and validation of a new body-image assessment scale. J. Pers. Assess. 1995, 64, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Maloney, M.J.; McGuire, J.B.; Daniels, S.R. Reliability testing of a children’s version of the Eating Attitude Test. J. Am. Acad. Child Adolesc. Psychiatry 1988, 27, 541–543. [Google Scholar] [CrossRef] [PubMed]
- Bryant-Waugh, R.J.; Cooper, P.J.; Taylor, C.L.; Lask, B.D. The use of the eating disorder examination with children: A pilot study. Int. J. Eat. Disord. 1996, 19, 391–397. [Google Scholar] [CrossRef]
- Collins, M.E. Body figure perceptions and preferences among preadolescent children. Int. J. Eat. Disord. 1991, 10, 199–208. [Google Scholar] [CrossRef]
- Oros, L.B. Medicion del perfeccionismo infantil: Desarrollo y validacion de una escala para ninos de 8 a 13 anos de edad. Rev Iberoam Diagn. Y Eval. Psicol. 2003, 16, 99–112. [Google Scholar]
- Moessner, M.; Fassnacht, D.B.; Bauer, S. Online assessment of eating disorders: The Clinical and Research Inventory for Eating Disorders (CR-EAT). Ment. Health Prev. 2015, 3, 170–177. [Google Scholar] [CrossRef]
- van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Pereira, A.T.; Maia, B.; Bos, S.; Soares, M.J.; Marques, M.; Macedo, A.; Azevedo, M.H. The Portuguese short form of the Eating Attitudes Test-40. Eur. Eat. Disord. Rev. 2008, 16, 319–325. [Google Scholar] [CrossRef][Green Version]
- Garner, D.M.; Garfinkel, P.E. The Eating Attitudes Test: An index of the symptoms of anorexia nervosa. Psychol. Med. 1979, 9, 273–279. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The eating attitudes test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Cooper, Z. The Eating Disorder Examination (12th edition). In Binge Eating: Nature, Assessment, and Treatment; Guilford Press: New York, NY, USA, 1993; pp. 317–360. [Google Scholar]
- Calugi, S.; Ricca, V.; Castellini, G.; Lo Sauro, C.; Ruocco, A.; Chignola, E.; El Ghoch, M.; Dalle Grave, R. The eating disorder examination: Reliability and validity of the Italian version. Eat. Weight Disord. 2015, 20, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Hilbert, A.; Tuschen-Caffier, B.; Karwautz, A.; Niederhofer, H.; Munsch, S. Eating Disorder Examination-Questionnaire. Diagnostica 2007, 53, 144–154. [Google Scholar] [CrossRef]
- Strober, M. The Eating Disorders Family History Interview; University of California: Los Angeles, CA, USA, 1987. [Google Scholar]
- Garner, D.M. Eating Disorder INVENTORY-II Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1991. [Google Scholar]
- Garner, D.M.; Olmstead, M.P.; Polivy, J. Development and Validation of a Multidimensional Eating Disorder Inventory for Anorexia-Nervosa and Bulimia. Int. J. Eat. Disord. 1983, 2, 15–34. [Google Scholar] [CrossRef]
- Ziółkowska, B. Ekspresja Syndromu Gotowości Anorektycznej u Dziewcząt w Stadium Adolescencji; Wydawnictwo Fundacji Humaniora: Poznań, Poland, 2001. [Google Scholar]
- Stice, E.; Agras, W.S. Predicting onset and cessation of bulimic behaviors during adolescence: A longitudinal grouping analysis. Behav. Ther. 1998, 29, 257–276. [Google Scholar] [CrossRef]
- World Health Organization. The ICD 10 Classification of Mental and Behavioural Disorders; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Thompson, J.K.; Heinberg, L.J.; Altabe, M.; Tantleff-Dunn, S. Exacting Beauty: Theory, Assessment, and Treatment of Body Image Disturbance; American Psychological Association: Washington, DC, USA, 1999. [Google Scholar]
- Marsh, H.W.; Trautwein, U.; Ludtke, O.; Koller, O.; Baumert, J. Integration of multidimensional self-concept and core personality constructs: Construct validation and relations to well-being and achievement. J. Pers. 2006, 74, 403–456. [Google Scholar] [CrossRef]
- Hyler, S.E.; Reider, R.O. Personality Diagnostic Questionnaire-Revised.; New York State Psychiatric Institute: New York, NY, USA, 1987. [Google Scholar]
- Hill, R.W.; Huelsman, T.J.; Furr, R.M.; Kibler, J.; Vicente, B.B.; Kennedy, C. A new measure of perfectionism: The Perfectionism Inventory. J. Pers. Assess. 2004, 82, 80–91. [Google Scholar] [CrossRef]
- Stice, E.; Nemeroff, C.; Shaw, H.E. Test of the dual pathway model of bulimia nervosa: Evidence for dietary restraint and affect regulation mecha- nisms. J. Soc. Clin. Psychol. 1996, 15, 340–363. [Google Scholar] [CrossRef]
- Herzog, D.B.; Sacks, N.R.; Keller, M.B.; Lavori, P.W.; von Ranson, K.B.; Gray, H.M. Patterns and predictors of recovery in anorexia nervosa and bulimia nervosa. J. Am. Acad. Child. Adolesc. Psychiatry 1993, 32, 835–842. [Google Scholar] [CrossRef]
- Hewitt, P.L.; Flett, G.L.; Ediger, E. Perfectionism traits and perfectionistic self-presentation in eating disorder attitudes, characteristics, and symptoms. Int. J. Eat. Disord. 1995, 18, 317–326. [Google Scholar] [CrossRef]
- Herman, C.P.; Mack, D. Restrained and unrestrained eating. J Pers 1975, 43, 647–660. [Google Scholar] [CrossRef] [PubMed]
- Fallon, A.E.; Rozin, P. Sex differences in perceptions of desirable body shape. J. Abnorm. Psychol. 1985, 94, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, L. Intrex User’s Manual; Univ Utah: Salt Lake City, UT, USA, 2000. [Google Scholar]
- Thompson, J.K.; Van den Berg, P.; Roehrig, M.; Guarda, A.S.; Heinberg, L.J. The sociocultural attitudes towards appearance scale-3 (SATAQ-3): Development and validation. Int. J. Eat. Disord. 2004, 35, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Sorenson, T.; Schulsinger, F. Use of the Danish adoption register for the study of obesity and thinness. Genet. Neurol. Psychiatr. Disord. 1983, 60, 115–120. [Google Scholar]
- Slade, P.D.; Dewey, M.E.; Kiemle, G.; Clin, M. Update on SCANS: A screening instrument for identifying individuals at risk of developing an eating disorder. Int. J. Eat. Disord. 1990, 9, 583–584. [Google Scholar] [CrossRef]
- First, M.B.; Spitzer, R.; Gibbon, M.; Williams, J.B.W. Structured Clinical Interview for DSM-IV-TR Axis I Disorders; New York State Psychiatric Institute: New York, NY, USA, 2002. [Google Scholar]
- Morgan, J.F.; Reid, F.; Lacey, J.H. The SCOFF questionnaire: Assessment of a new screening tool for eating disorders. BMJ 1999, 319, 1467–1468. [Google Scholar] [CrossRef]
- Berscheid, E.; Walster, E.; Bohrnstedt, G. The happy American body: A survey report. Psychol. Today 1973, 7, 119–131. [Google Scholar]
- Fichter, M.; Quadflieg, N. The structured interview for anorexic and bulimic disorders for DSM-IV and ICD-10 (SIAB-EX): Reliability and validity. Eur. Psychiatry 2001, 16, 38–48. [Google Scholar] [CrossRef]
- Petersen, A.C.; Schulenberg, J.E.; Abramowitz, R.H.; Offer, D.; Jarcho, H.D. A self-image questionnaire for young adolescents (SIQYA): Reliability and validity studies. J. Youth Adolesc. 1984, 13, 93–111. [Google Scholar] [CrossRef]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Hohlstein, L.A.; Smith, G.T.; Atlas, J.G. An application of expectancy theory to eating disorders: Development and validation of measures of eating and dieting expectancies. Psychol. Assess. 1998, 10, 49–58. [Google Scholar] [CrossRef]
- Conti, L. Repertorio Delle scale di Valutazione in Psichiatria; SEE: Florence, Italy, 2002. [Google Scholar]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. The Clinical Perfectionism Questionnaire; Department of Psychiatry, University of Oxford: Oxford, UK, 2003. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Livet, A.; Navarri, X.; Pomerleau, P.P.; Champagne, S.; Yunus, F.M.; Chadi, N.; McVey, G.; Conrod, P. Perfectionism in Children and Adolescents with Eating-Related Symptoms: A Systematic Review and a Meta-Analysis of Effect Estimates. Adolescents 2023, 3, 305-329. https://doi.org/10.3390/adolescents3020022
Livet A, Navarri X, Pomerleau PP, Champagne S, Yunus FM, Chadi N, McVey G, Conrod P. Perfectionism in Children and Adolescents with Eating-Related Symptoms: A Systematic Review and a Meta-Analysis of Effect Estimates. Adolescents. 2023; 3(2):305-329. https://doi.org/10.3390/adolescents3020022
Chicago/Turabian StyleLivet, Audrey, Xavier Navarri, Philippe Pétrin Pomerleau, Sébastien Champagne, Fakir Md Yunus, Nicholas Chadi, Gail McVey, and Patricia Conrod. 2023. "Perfectionism in Children and Adolescents with Eating-Related Symptoms: A Systematic Review and a Meta-Analysis of Effect Estimates" Adolescents 3, no. 2: 305-329. https://doi.org/10.3390/adolescents3020022
APA StyleLivet, A., Navarri, X., Pomerleau, P. P., Champagne, S., Yunus, F. M., Chadi, N., McVey, G., & Conrod, P. (2023). Perfectionism in Children and Adolescents with Eating-Related Symptoms: A Systematic Review and a Meta-Analysis of Effect Estimates. Adolescents, 3(2), 305-329. https://doi.org/10.3390/adolescents3020022