Abstract
The purpose of this study was to examine the predictive value of phase angle (PhA) in chronic spinal cord injury (SCI). This study includes 104 participants (52 for each group) of SCI patients and healthy subjects (HS) treated at the Indian Spinal Injury Centre (ISIC, New Delhi, India) between October 2020 and March 2021 A cross-sectional study was operated Bioelectrical Impedance Analysis (BIA) at 50 kHz and measured the prognostic effect of PhA on participants. An independent-sample t-test was used to estimate PhA between groups. Receiver Operating Characteristic (ROC) curves predicted the PhA cutoff and Youden’s index. There was a significant difference in PhA of gender, with p < 0.0001, a difference (2.40), 95% confidence interval (CI) (2.10 to 2.80), median (4.70) for the SCI group, and (7.1) for HS, respectively. In contrast, PhA was significantly different in males with p < 0.0001, a difference (2.60), 95% CI (3.00 to 2.10), median (5.0) for SCI, and (7.30) for HS, respectively. Similarly, PhA was significantly different in females, with p < 0.0001, a difference (1.9881), 95 % CI of difference (1.3565 to 2.6197), median (6.60) for SCI, and (4.40) for HS, respectively, as well as PhA cutoff values for SCI (female ≤ 4.4°; male ≤ 4.7°). The outcomes indicate a difference between groups of people with SCI and HS across the groups of gender, with a lower PhA in people with SCI.
1. Introduction
The prevalence of traumatic spinal cord injuries (SCI) in road traffic accidents (RTA) and falls has grown significantly over the past few decades, especially among young individuals [1]. Individuals with SCI have an effective functional disability of their upper and lower limbs, significantly impacting their everyday routine [2,3]. With immobility, persons with SCI lose a lot of skeletal muscle mass (SMM), significantly below the level of the injury. This reduces resting energy expenditure and increases total body and visceral fat mass [4,5]. Persons with SCI are predisposed to muscular atrophy, immobility, and increased fat penetration due to lack of physical activity [6]. Thus, according to clinical evidence, adverse changes in body composition after an acute SCI might significantly impact therapy, total body energy metabolism, muscle architecture, components, and health condition [7,8]. Therefore, a simple technique for assessing changes in body composition in persons with SCI in outpatient settings is required. There are few useful and practical techniques for estimating SCI patients’ BC changes [7,9]. Non-invasive approaches for assessing BC in people with SCI are essential for clinical rehabilitation. These techniques, which include “Bioelectrical Impedance Analysis (BIA), Dual-X Ray Absorptiometry (DXA), Anthropometric Index, Magnetic Resonance Imaging (MRI), Waist Circumference, and Computed Tomography (CT),” are deemed more appropriate for investigative purposes [10,11,12]. BIA, which provides a straightforward estimation of BC, is now widely utilized in routine health assessments. BIA measures the electrical resistance of different tissues (e.g., fat, muscle, bone) simply by applying a low current to the body [13,14,15,16]. The phase angle (PhA) is one of the most therapeutically relevant bioimpedance factors evaluated with BIA. The PhA(θ) is described as =(X/R), the angle between the resistance of intracellular water (ICW) and extracellular water (ECW) and reactance (cell-membrane-specific resistance). It is classified as a marker of cellular membranes function and is often used to measure nutritional status and the risk of developing differential diagnoses [17,18,19]. A study by Li et al. found that the SCI group had a lower reactance and PhA than the HS group, revealing that these changes might be related to alterations in muscle structure and inherent properties [20].
Furthermore, the PhA may be considered an indicator of the water distribution of ICW and ECW compartments, which is quite a sensitive predictor of malnutrition [21]. The PhA is proven to be a prognostic sign in numerous clinical situations, including HIV infection, liver cirrhosis, COPD, dialysis, and sepsis [22,23]. Consequently, more research is critical for understanding the variations in BC between SCI and healthy subjects, raw impedance, hydration, and mass distribution. The present study aimed to determine the predictive value of phase angle alterations in SCI compared to healthy subjects using the BIA method.
2. Materials and Methods
Study Participants
After written permission and informed consent, 104 participants were recruited for this study, which was conducted between October 2020 and March 2021 in Indian Spinal Injuries Centre (ISIC, New Delhi, India). The study was authorized by the institutional Ethics Committee (IEC) (Ref: ISIC/RP/2020/008). Our research enrolled patients above 18 years, ISNCSCI-AIS A, B, C, and those who were injured for at least six months. The study also excluded people with cancer, COPD, CKD, pregnancy, and chronic illnesses that cause weight loss or muscle loss. Hence, healthy subjects were chosen from among hospital staff and members of the surrounding community.
2.1. Bioelectrical Impedance Analysis
PhA was measured using BIA techniques (biodynamics BIA450, Shoreline, DC, USA). Additionally, to eliminate measurement mistakes, all measurements were obtained by the same investigator. Patients were instructed to take a five-minute break, and drink no caffeine or alcohol before their test. Wrist and hand sensors were attached to the patient’s right arm, while the ankle and foot sensors were connected to the right foot. A sensor wire was used to link the monitor to the electrodes. The device sent an 80 µA low-frequency (50 kHz) electric current across the organism, measuring the resistance given by human tissues.
2.2. Anthropometry
Each participant’s weight (kg) and height (cm) were measured. The weight of people with SCI was determined using Metis Electronic Weighing Scale, in which the individual was pulled to the weighing machine while seated in a wheelchair. The participants’ weights were calculated after deducting the weight of the empty wheelchair. The physiotherapist measured the patients’ heights (cm) while they lay on the bed.
2.3. Statistical Analysis
MedCalc Statistical Software was performed (“MedCalc Software version 18.11.3 bvba, Ostend, Belgium, 2019”). Independent samples (“Mann–Whitney t-test”) and “Shapiro–Wilk t-test” were applied for non-normality data distributions and normality data distribution, respectively, to compare the PhA groups. With mean, standard deviation (SD), 95% confidence interval (CI), and median representing the data, p-values < 0.05 were considered significant. Moreover, the receiver operating characteristic curve (AUC) was used to determine the discriminatory ability of PhA for individuals with SCI as the outcome variable. DeLong’s test was used to assess the significance of AUC variance between PhA. The optimal cutoff parameters were estimated using the maximum Youden’s index (sensitivity + specificity − 1) and the optimal grouping of sensitivity and specificity [24]. ROC curve analysis was carried out on a gender-balanced sample of SCI and HS to determine their sensitivity.
3. Results
Characteristics of the participants
This research included 104 participants (52 for each group). The anthropometric and bioimpedance traits of people with SCI and HS are shown in Table 1. On average, participants has experienced injury for 2.40 (2.63) years. The clinical and demographic characteristics of a person with SCI are determined by the ISNCSCI-AIS classifications (A, B, C) and the degree of the lesion (16 tetraplegia, 36 paraplegia). There were 41 males and 11 females in the SCI group, whereas there were 39 males and 13 females in the HS group.

Table 1.
Anthropometric and bioimpedance characteristics for participants.
Our results indicated that there was a significantly higher difference between genders (p < 0.0001, difference (2.40), 95% CI (2.10 to 2.80), median (4.70)) for the SCI group, and (7.1) for HS, respectively, as shown in Table 2 and Figure 1c Meanwhile, the PhA of males between SCI and HS groups has a significantly higher difference (p-value of <0.0001, difference (2.60), 95% CI (3.00 to 2.10), median (5.0) for SCI, and (7.30)) for HS, respectively, as shown in Table 2 and Figure 1a In contrast, the Shapiro–Wilk t-test was applied for normality distribution. There was a significant difference in female PhA among SCI and HS (p < 0.0001, difference (1.9881), 95 % CI (1.3565 to 2.6197), standard error (SE) (0.3046), mean (SD) 6.61 (0.53) for HS, and 4.62 (0.93), for SCI), as shown in Table 2 and Figure 1b The results show that the PhA of SCI begins to decrease after the injury.
Table 2.
Summary of comparison group for the phase angle between SCI and HS.
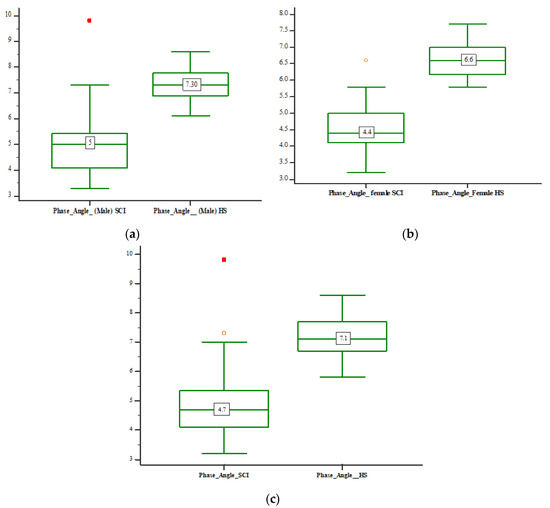
Figure 1.
Box and whisker plot of PhA comparison between SCI and HS participants: (a). Box and whisker plot of PhA comparison between males SCI and HS (b). Box and whisker plot of PhA comparison between females of SCI and HS (c). Box and whisker plot of PhA comparison between gender of SCI and HS.
The results indicate that patients with SCI have a lower predictive ability for PhA (male: AUC = 1.0, 95% CI = 0.914–1.000; female: AUC = 1.0, 95% CI = 0.715–1.000). Meanwhile, PhA of HS were high (male: AUC = 1.0, 95% CI = 0.910–1.0000; female: AUC = 1.0, 95% CI = 0.753–1.000). The AUC of PhA of individuals with SCI and HS in both males and females were significant with a p-value (p < 0.0001), and sensitivity and specificity = 100%. The cutoff points of PhA were ≤4.7° in males and 4.4° in females with SCI, respectively. In contrast, the cutoff points of PhA of the HS group were ≤6.9° in males and ≤6.3° in females, respectively, as shown in Table 3. Our results show that people with SCI have a low predictive PhA cutoff value for SCI. Accordingly, these results should be considered while carrying out therapeutic nutrition and rehabilitation in individuals with SCI.
Table 3.
Predictive ability of BC parameter for PhA and SCI and HS cutoff points.
4. Discussion
This investigation aimed to identify the predictive value of PhA in people with SCI using BIA. Our findings revealed a statistically significant gender difference, with p < 0.0001. Simultaneously, male PhA was significantly different between the SCI and HS groups, with a p < 0.0001. In contrast, between SCI and HS, there was a significant difference in female PhA, with p < 0.0001. Our investigation found that PhA of SCI is low regarding gender, being lower in females than in HS, and it decreases post-injury, as shown in Figure 1 Hence, following SCI, bone and muscle atrophy are significant, and the severity of an injury or the length of time since an accident may influence outcomes [25]. Even though the mechanism behind these outcomes is not entirely known, PhA may serve as a global predictor of physiologic alterations in disability since it also indicates physical performance [26,27], physical exercise activities, and nutritional status [28]. Basile and colleagues discovered an independent linear relationship between PhA and decreased muscle mass and strength [29].
Furthermore, PhA may be a beneficial bioelectrical diagnostic tool for detecting a high risk of muscle tissue loss in SCI. To our knowledge, no prior research has studied PhA determinants in persons with SCI using BIA estimates of body composition segments obtained from techniques that are deemed standard in SCI. Regardless, The bioimpedance PhA has been shown to be clinically relevant in predicting people with SCI. In addition, a ROC analysis indicated that the predictive ability of male and female PhA in individuals with SCI was statistically significant (p < 0.0001, AUC = 1.000), and the cutoff points were ≤4.7° for males, and ≤4.4° for females, respectively, as shown in Table 3 and Figure 2a, Figure 3a. In contrast, the predictive ability of the PhA of males and females for HS was statistically significant, with (p < 0.0001, AUC = 1.000), and the cutoff points were ≤6.9° for males and ≤6.3° for females, respectively, as shown in Table 3 and Figure 2b, Figure 3b. The current investigation findings highlighted the use of PhA as a regular evaluation in community-based medical assessment and provided efficient and relatively predictive cutoff values for detecting persons with SCI. Hence, SCI with a low PhA is more likely to suffer from disability because of the risk of injury based on the cutoff point (male, ≤4.7°; female, ≤4.4°).
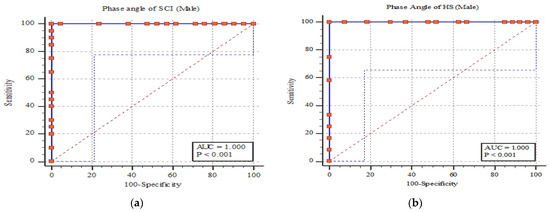
Figure 2.
The PhA ROC curve for SCI and HS participants: (a) shows the ROC curve of PhA for SCI males; (b) shows the ROC curve of PhA for HS males.
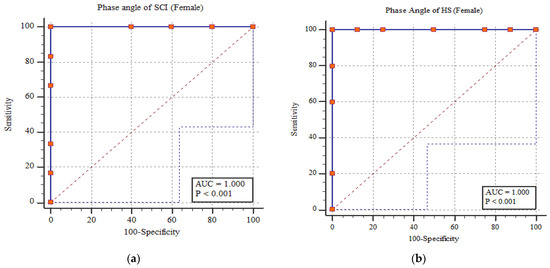
Figure 3.
The PhA ROC curve for SCI and HS participants: (a) shows the ROC curve of PhA for SCI females; and (b) shows the ROC curve of PhA for HS females.
Interestingly, the PhA cutoff point obtained in this investigation was similar to that of elderly adults (male, ≤4.95°; female, ≤4.35°). The results show that old age is related to a loss of muscle mass similar to that in people with SCI. Apart from its efficacy as a prognostic marker of survival, as previously reported [30], our findings corroborate the PhA-predictive potential for adverse health outcomes in persons with SCI. Moreover, PhA was extensively verified in patient groups for diseases such as cancer and hemodialysis to predict illness prognosis [31,32], diminished quality of life, malnutrition, and higher mortality [33]. As a result, PhA is used as a general health and nutritional status indicator [34,35]. Nevertheless, our study indicated that PhA has the predictive ability to detect muscle mass and a performance decrease in individuals with SCI. The PhA reflects the balance between cellular hydration and mass. A low PhA value is related to cell membrane injury and deaths, whereas a high PhA value is linked to normal cellular membranes or cellular function [36]. The PhA is determined by the tissue’s characteristics, cell size, function, and cellularity. Furthermore, PhA is identified as a cellular healthiness indicator. However, the predictive significance of PhA varies depending on the clinical situation [37,38]. The present research calculated PhA using a BIA assessment approach absent regression equivalences.. PhA may be a beneficial option for predicting the early stages of muscle mass loss in individuals with SCI. It overcomes the limitation inherent in conventional BIA parameter accuracy calculation through regression equations. However, these protocols are specific to Indian society. We must interpret the existing results, which cannot be generalized to include other nations. This is one of the drawbacks of our examination. Additionally, we included a small sample size of individuals with SCI from a single center since the baseline evaluation was conducted at our center and might limit the generalizability and practical applicability. Further investigations may be required with large sample sizes from multiple centers to find prognostic PhA values in persons with SCI.
5. Conclusions
We confirmed that the PhA of SCI differs via gender, with females having a lower PhA than healthy subjects. We discovered that the bioimpedance PhA accurately predicts the abilities of persons with SCI to identify muscle mass and performance deterioration. Furthermore, we recommended optimal PhA cutoff values for persons with SCI (female ≤ 4.4°; male ≤ 4.7°) to identify patients for preventative therapy in society medical assessment. BIA-derived PhA results created a realistic alternative to operating muscle mass to monitor the risk of adverse health events and analyze the efficacy of therapies in spinal cord injury.
Author Contributions
Conceptualization, M.A., K.P. and H.S.C.; methodology, M.A. and K.P.; software, M.A.; validation, M.A.; formal analysis, M.A., K.P. and H.S.C.; investigation, M.A. and H.S.C.; resources, H.S.C.; writing—original draft preparation, M.A., K.P. and H.S.C.; writing—review and editing, M.A., K.P. and, H.S.C.; supervision, K.P. and H.S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Indian Spinal Injury Centre approved the above study: Institutional Ethics Committee, with reference no (Ref: ISIC/RP/2020/008).
Informed Consent Statement
All volunteers gave their informed consent before taking part in the research.
Data Availability Statement
Data are contained within the article.
Acknowledgments
We want to thank “Indian Spinal Injury Centre (ISIC)” for their cooperation in completing this examination and go to all participants in this study. The author’s greatest appreciation goes to the Senior Research Associate, Rajesh Sharawat, at ISIC for their valuable support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chhabra, H.S.; Arora, M. Demographic profile of traumatic spinal cord injuries admitted at Indian spinal injuries Centre with special emphasis on mode of injury: A retrospective study. Spinal Cord 2012, 50, 745–754. [Google Scholar] [CrossRef]
- Anderson, K.D.; Fridén, J.; Lieber, R.L. Acceptable benefits and risks associated with surgically improving arm function in individuals living with cervical spinal cord injury. Spinal Cord 2009, 47, 334–338. [Google Scholar] [CrossRef] [Green Version]
- Gorla, J.I.; Costae Silva, A.D.A.; Borges, M.; Tanhoffer, R.A.; Godoy, P.S.; Calegari, D.R.; Santos, A.D.O.; Ramos, C.D.; Nadruz Junior, W.; Cliquet Junior, A. Impact of wheelchair rugby on body composition of subjects with tetraplegia: A pilot study. Arch. Phys. Med. Rehabil. 2016, 97, 92–96. [Google Scholar] [CrossRef]
- Abilmona, S.M.; Sumrell, R.M.; Gill, R.S.; Adler, R.A.; Gorgey, A.S. Serum testosterone levels may influence body composition and cardiometabolic health in men with spinal cord injury. Spinal Cord 2019, 57, 229–239. [Google Scholar] [CrossRef]
- Gorgey, A.S.; Martin, H.; Metz, A.; Khalil, R.E.; Dolbow, D.R.; Gater, D.R. Longitudinal changes in body composition and metabolic profile between exercise clinical trials in men with chronic spinal cord injury. J. Spinal Cord Med. 2016, 39, 699–712. [Google Scholar] [CrossRef] [Green Version]
- Gorgey, A.S.; Gater, D.R. Prevalence of Obesity After Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2007, 12, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Cirnigliaro, C.M.; La Fountaine, M.F.; Emmons, R.; Kirshblum, S.C.; Asselin, P.; Spungen, A.M.; Bauman, W.A. Prediction of limb lean tissue mass from bioimpedance spectroscopy in persons with chronic spinal cord injury. J. Spinal Cord Med. 2013, 36, 443–453. [Google Scholar] [CrossRef] [Green Version]
- Gater, D.R.; Clasey, J.L. Body composition assessment in spinal cord injury clinical trials. Top. Spinal Cord Inj. Rehabil. 2006, 11, 36–49. [Google Scholar] [CrossRef]
- de Groot, S.; Kouwijzer, I.; Baauw, M.; Broeksteeg, R.; Valent, L.J. Effect of self-guided training for the HandbikeBattle on body composition in people with spinal cord injury. Spinal Cord Ser. Cases 2018, 4, 1–7. [Google Scholar] [CrossRef]
- Eriks-Hoogland, I.; Hilfiker, R.; Baumberger, M.; Balk, S.; Stucki, G.; Perret, C. Clinical assessment of obesity in persons with spinal cord injury: Validity of waist circumference, body mass index, and anthropometric index. J. Spinal Cord Med. 2011, 34, 416–422. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, E.; Alonso, K.C.; Jr, A.C. Body composition assessment by bioelectrical impedance analysis and body mass index in individuals with chronic spinal cord injury. J. Electr. Bioimpedance 2016, 7, 2–5. [Google Scholar] [CrossRef]
- Silveira, S.L.; Ledoux, T.A.; Robinson-Whelen, S.; Stough, R.; Nosek, M.A. Methods for classifying obesity in spinal cord injury: A review. Spinal Cord 2017, 55, 812–817. [Google Scholar] [CrossRef]
- Lukaski, H.C.; Bolonchuk, W.W. Estimation of body fluid volumes using tretrapolar bioelectrical impedance measurements. Aviat. Space Environ. Med. 1988, 59, 1163–1169. [Google Scholar]
- Desport, J.C.; Preux, P.M.; Bouteloup-Demange, C.; Clavelou, P.; Beaufrère, B.; Bonnet, C.; Couratier, P.P. Validation of bioelectrical impedance analysis in patients with amyotrophic lateral sclerosis. Am. J. Clin. Nutr. 2003, 77, 1179–1185. [Google Scholar] [CrossRef] [Green Version]
- Sarhill, N.; Walsh, D.; Nelson, K.; Homsi, J.; Komurcu, S. Bioelectrical impedance, cancer nutritional assessment, and ascites. Support. Care Cancer 2000, 8, 341–343. [Google Scholar] [CrossRef]
- Aldobali, M.; Urooj, S.; Pal, K. Applications of Bioelectrical Impedance Analysis in Diagnosis of Diseases: A Systematic Review. J. Clin. Diagn. Res. 2021, 15, 1–6. [Google Scholar] [CrossRef]
- Tanaka, S.; Ando, K.; Kobayashi, K.; Hida, T.; Seki, T.; Hamada, T.; Ito, K.; Tsushima, M.; Morozumi, M.; Machino, M.; et al. The decrease in phase angle measured by bioelectrical impedance analysis reflects the increased locomotive syndrome risk in community-dwelling people: The Yakumo study. Mod. Rheumatol. 2019, 29, 496–502. [Google Scholar] [CrossRef]
- Aldobali, M.; Pal, K. Bioelectrical Impedance Analysis for Evaluation of Body Composition: A Review. In Proceedings of the 2021 International Congress of Advanced Technology and Engineering (ICOTEN), Taiz, Yemen, 4–5 July 2021. [Google Scholar]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis—Clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef]
- Li, L.; Shin, H.; Stampas, A.; Li, X.; Zhou, P. Electrical impedance myography changes after incomplete cervical spinal cord injury: An examination of hand muscles. Clin. Neurophysiol. 2017, 128, 2242–2247. [Google Scholar] [CrossRef]
- Schwenk, A.; Eschner, W.; Kremer, G.; Ward, L.C. Assessment of intracellular water by whole body bioelectrical impedance and total body potassium in HIV-positive patients. Clin. Nutr. 2000, 19, 109–113. [Google Scholar] [CrossRef]
- Gupta, D.; Lammersfeld, C.A.; Burrows, J.L.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Hoffman, S.; Lis, C.G. Bioelectrical impedance phase angle in clinical practice: Implications for prognosis in advanced colorectal cancer. Am. J. Clin. Nutr. 2004, 80, 1634–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faisy, C.; Rabbat, A.; Kouchakji, B.; Laaban, J.P. Bioelectrical impedance analysis in estimating nutritional status and outcome of patients with chronic obstructive pulmonary disease and acute respiratory failure. Intensive Care Med. 2000, 26, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Hajian-Tilaki, K. Receiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluation. Casp. J. Intern. Med. 2013, 4, 627–635. [Google Scholar]
- Giangregorio, L.; McCartney, N. Bone loss and muscle atrophy in spinal cord injury: Epidemiology, fracture prediction, and rehabilitation strategies. J. Spinal Cord Med. 2006, 29, 489–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, Y.; Buehring, B.; Krueger, D.; Anderson, R.M.; Schoeller, D.A.; Binkley, N. Electrical Properties Assessed by Bioelectrical Impedance Spectroscopy as Biomarkers of Age-related Loss of Skeletal Muscle Quantity and Quality. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1180–1186. [Google Scholar] [CrossRef] [Green Version]
- Uemura, K.; Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Kim, M.J.; Kurita, S.; Ishii, H.; Shimada, H. Predictivity of bioimpedance phase angle for incident disability in older adults. J. Cachexia Sarcopenia Muscle 2020, 11, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Dittmar, M. Reliability and Variability of Bioimpedance Measures in Normal Adults: Effects of Age, Gender, and Body Mass. Am. J. Phys. Anthropol. 2003, 122, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Basile, C.; Della-Morte, D.; Cacciatore, F.; Gargiulo, G.; Galizia, G.; Roselli, M.; Curcio, F.; Bonaduce, D.; Abete, P. Phase angle as bioelectrical marker to identify elderly patients at risk of sarcopenia. Exp. Gerontol. 2014, 58, 43–46. [Google Scholar] [CrossRef]
- Wilhelm-Leen, E.R.; Hall, Y.N.; Horwitz, R.I.; Chertow, G.M. Phase angle, frailty and mortality in older adults. J. Gen. Intern. Med. 2014, 29, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Beberashvili, I.; Azar, A.; Sinuani, I.; Kadoshi, H.; Shapiro, G.; Feldman, L.; Sandbank, J.; Averbukh, Z. Longitudinal changes in bioimpedance phase angle reflect inverse changes in serum IL-6 levels in maintenance hemodialysis patients. Nutrition 2014, 30, 297–304. [Google Scholar] [CrossRef]
- Norman, K.; Wirth, R.; Neubauer, M.; Eckardt, R.; Stobäus, N. The bioimpedance phase angle predicts low muscle strength, impaired quality of life, and increased mortality in old patients with cancer. J. Am. Med. Dir. Assoc. 2015, 16, 173.e17–173.e22. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Bansal, S.; Morgado, M.; Dev, R.; Chisholm, G.; Bruera, E. Phase angle for prognostication of survival in patients with advanced cancer: Preliminary findings. Cancer 2014, 120, 2207–2214. [Google Scholar] [CrossRef] [Green Version]
- Barbosa-Silva, M.C.G.; Barros, A.J.D.; Post, C.L.A.; Waitzberg, D.L.; Heymsfield, S.B. Can bioelectrical impedance analysis identify malnutrition in preoperative nutrition assessment? Nutrition 2003, 19, 422–426. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Chumlea, W.C.; Roche, A.F. Bioelectric impedance phase angle and body composition. Am. J. Clin. Nutr. 1988, 48, 16–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gigante, A.; Gasperini, M.L.; Rosato, E.; Navarini, L.; Margiotta, D.; Afeltra, A.; Muscaritoli, M. Phase angle could be a marker of microvascular damage in systemic sclerosis. Nutrition 2020, 73, 110730. [Google Scholar] [CrossRef]
- Anja, B.W.; Danielzik, S.; Dörhöfer, R.P.; Later, W.; Wiese, S.; Müller, M.J. Phase angle from bioelectrical impedance analysis: Population reference values by age, sex, and body mass index. J. Parenter Enter. Nutr. 2006, 30, 309–316. [Google Scholar]
- Kim, J.; Park, H.J.; Sim, W.S.; Lee, S.; Kim, K.; Kim, W.J.; Lee, J.Y. Predictive value of the phase angle for analgesic efficacy in lumbosacral transforaminal block. J. Clin. Med. 2021, 10, 240. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).