Abstract
The purpose of this study is to describe the prevalence, trends, and associations of the use of outpatient prescription non-narcotic analgesics and proton pump inhibitors (PPIs) in Taiwan from 2010 to 2021. We identified the most commonly prescribed analgesics and PPIs, including paracetamol (acetaminophen) and nonsteroidal anti-inflammatory drugs (NSAIDs), in outpatient departments according to the data from Taiwan National Health Insurance Research Database and Taiwan’s NHI Annual Statistical Report. This study shows that the traditional non-selective NSAIDs take the largest proportion of usage, representing over 60% of the annual usage of non-narcotic analgesics. Acetaminophen is the second and takes over 30% of annual usage. The selective COX-2 (coxibs) takes less than 10% of usage, but its use is growing rapidly. This study also shows that the annual usage of PPIs is growing rapidly and is not decreasing with the use of selective COX-2. The findings in this study can help us to focus on the most commonly prescribed drugs to investigate the prescription pattern of NSAIDs and PPIs, especially the combined use of selective COX-2 and PPIs, in future study.
1. Introduction
Non-narcotic analgesics, also known as non-opioid analgesics or non-addictive analgesics, are widely used in outpatient prescriptions as a preferred, safe, and effective first-line therapy for mild-to-moderate acute and chronic pain. Non-narcotic analgesics encompass paracetamol (acetaminophen) and nonsteroidal anti-inflammatory drugs (NSAIDs). In addition to pain relief and fever reduction, NSAIDs also have anti-inflammatory effects; therefore, the outpatient use of NSAIDs is growing rapidly [1]. However, NSAIDs have the risk of adverse gastrointestinal effects (ulceration and bleeding), and so they are often combined with the use of gastrointestinal protection drugs, such as proton pump inhibitors (PPIs) [2]. This not only places a greater burden on Taiwan’s National Health Insurance (NHI) drug expenditures, but also induces several different forms of kidney injury, including hemodynamically mediated acute kidney injury (AKI) and acute interstitial nephritis (AIN) [3]. Since drug expenditures account for 25 percent of total Taiwan’s NHI expenditures, and as the treatment expenses of acute kidney failure and chronic kidney disease have been the largest proportion of Taiwan’s NHI annual outpatient expenditures over a long period of time, it is important to understand the prescription patterns of non-narcotic analgesics and gastrointestinal protection drugs to prevent these nephrotoxic drugs from causing kidney damage to patients [4].
We want to investigate the following questions: (1) What were the trends in outpatient prescription of non-narcotic analgesics and PPIs under Taiwan’s NHI from 2010 to 2021? (2) Does the usage of PPIs decrease with the use of the selective COX-2? (3) What are the most commonly prescribed analgesics and PPIs according to annual usage in recent years? (4) Are these analgesics used in combination with the PPIs? (5) What are their prescription patterns? We conduct a two-step study to answer these research questions. In study 1, we list all the non-narcotic analgesics and PPIs. We rate the risk of adverse gastrointestinal effects of each non-narcotic analgesic and calculate the annual usage of each type of analgesics and PPIs using data from Taiwan’s NHI Annual Statistical Report from 2010 to 2021. We describe the prevalence and trends of the use of non-narcotic analgesics and PPIs. Then, we identify the most commonly prescribed analgesics and PPIs in recent years. This study mainly focuses on study 1 and tries to answer the research question (1), (2), and (3). Working with study 2, we use the list of the most commonly prescribed analgesics and PPIs to search the outpatient prescriptions in Taiwan’s NHI Research Database. We will collect the prescription data for these drugs, including the international classification of disease (ICD), the dosage, the demographic characteristics of the patients, and the cities in which a hospitals are. We will use these data to analyze the prescription patterns of the most commonly prescribed analgesics and how they are used in combination with PPIs? Study 2 will use the result of study 1 to answer the research question (4) and (5).
2. Materials and Methods
2.1. Data Source
We conducted a literature review in order to list all the commonly used non-narcotic analgesics included in Taiwan’s NHI drug reimbursement. These drugs can be searched in Taiwan’s NHI drug database [5] and can be used in outpatient prescriptions. We used the nationwide drug usage data in Taiwan’s NHI Annual Statistical Report [6] from 2010 to 2021 to calculate the annual usage of each type of analgesics and PPIs.
2.2. Definitions of Variables
Non-narcotic analgesics encompass paracetamol (acetaminophen) and non-steroidal anti-inflammatory drugs (NSAIDs). All these drugs have both analgesic and antipyretic properties, and they are widely used to manage mild-to-moderate pain conditions. However, they also have the disadvantages of the potential for gastrointestinal (GI) and renal toxicity. Paracetamol (acetaminophen) is considered to be a safe analgesic/antipyretic compound and its side effects are less severe than those of the NSAIDs. Accordingly, it is widely accepted that paracetamol is particularly suitable for patients at high risk of developing gastrointestinal (GI) ulcers or bleeds. At high doses, it is believed that paracetamol may induce upper GI symptoms such as abdominal pain/discomfort, nausea or vomiting [7]. Therefore, we identify the risk of gastrointestinal (GI) toxicity of paracetamol as low.
NSAIDs are categorized as traditional ‘non-selective COX-1/COX-2′ NSAIDs and selective cyclooxygenase COX-2 inhibitors (also known as coxibs). Mucosal injury in the gastrointestinal (GI) tract is the most common adverse effect associated with NSAIDs. Patients who receive long-term treatment with a traditional non-selective NSAID have an approximate five-fold higher risk of peptic ulcer disease compared to non-users. The increased risk of gastrointestinal complications associated with non-selective NSAIDs promotes the development of newer COX-2 inhibitors (coxibs); patients receiving selective COX-2 inhibitors have significantly lower risk of GI toxicity than those receiving non-selective NSAIDs. Due to the high risks of GI side effects of traditional NSAIDs, patients at increased risk of GI complications should receive either a non-selective NSAID with proton pump inhibitors (PPIs), or a COX-2-selective inhibitor alone [1,8]. Therefore, we identify the risk of GI toxicity of the traditional non-selective NSAIDs as high, and that of the selective COX-2 inhibitors as low.
In Table 1, we list all the non-narcotic analgesics, including paracetamol (acetaminophen), traditional non-selective NSAIDs, and selective COX-2 inhibitors (coxibs) [9,10], and also list all the proton pump inhibitors (PPIs), that are approved by the United States Food and Drug Administration (FDA) and are included in Taiwan’s NHI drug reimbursement [11,12]. The drugs are organized by name alphabetically:

Table 1.
Non-narcotic analgesics and PPIs under Taiwan’s NHI drug reimbursement.
3. Results
We used the drugs in Table 1 and the nationwide drug usage data in Taiwan’s NHI Annual Statistical Report for 12 years from 2010 to 2021 to summarize the annual usage amount of one paracetamol variety, 18 non-selective NSAIDs, three selective COX-2 drugs, and six PPIs in Table 2. We compared the results by category and by each drug to show the prescription trends of each category of the non-narcotic analgesics and PPIs, and to identify the most commonly prescribed drugs in each category.
Table 2.
The annual usage amount of non-narcotic analgesics and PPIs.
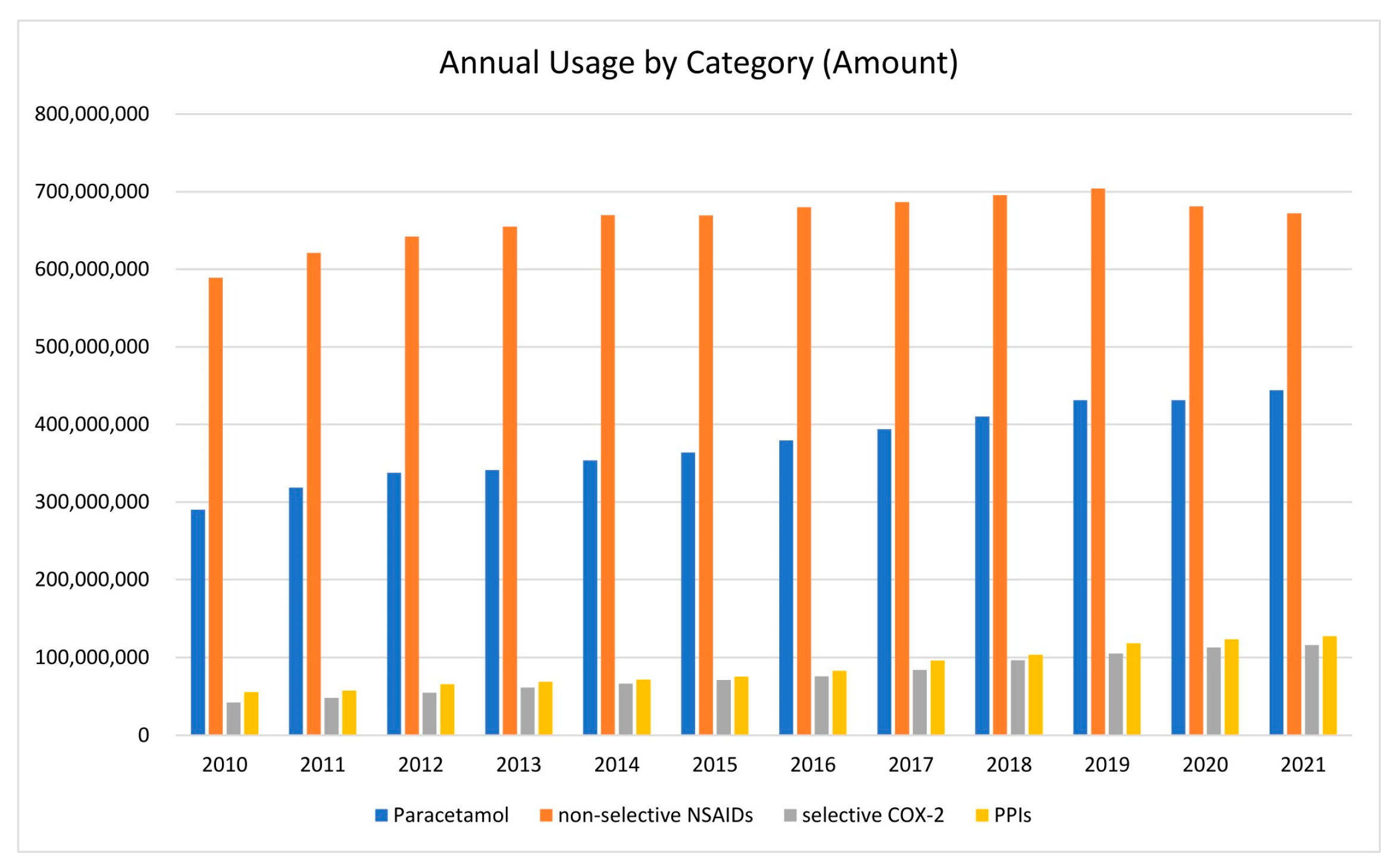
3.1. Annual Usage by Category
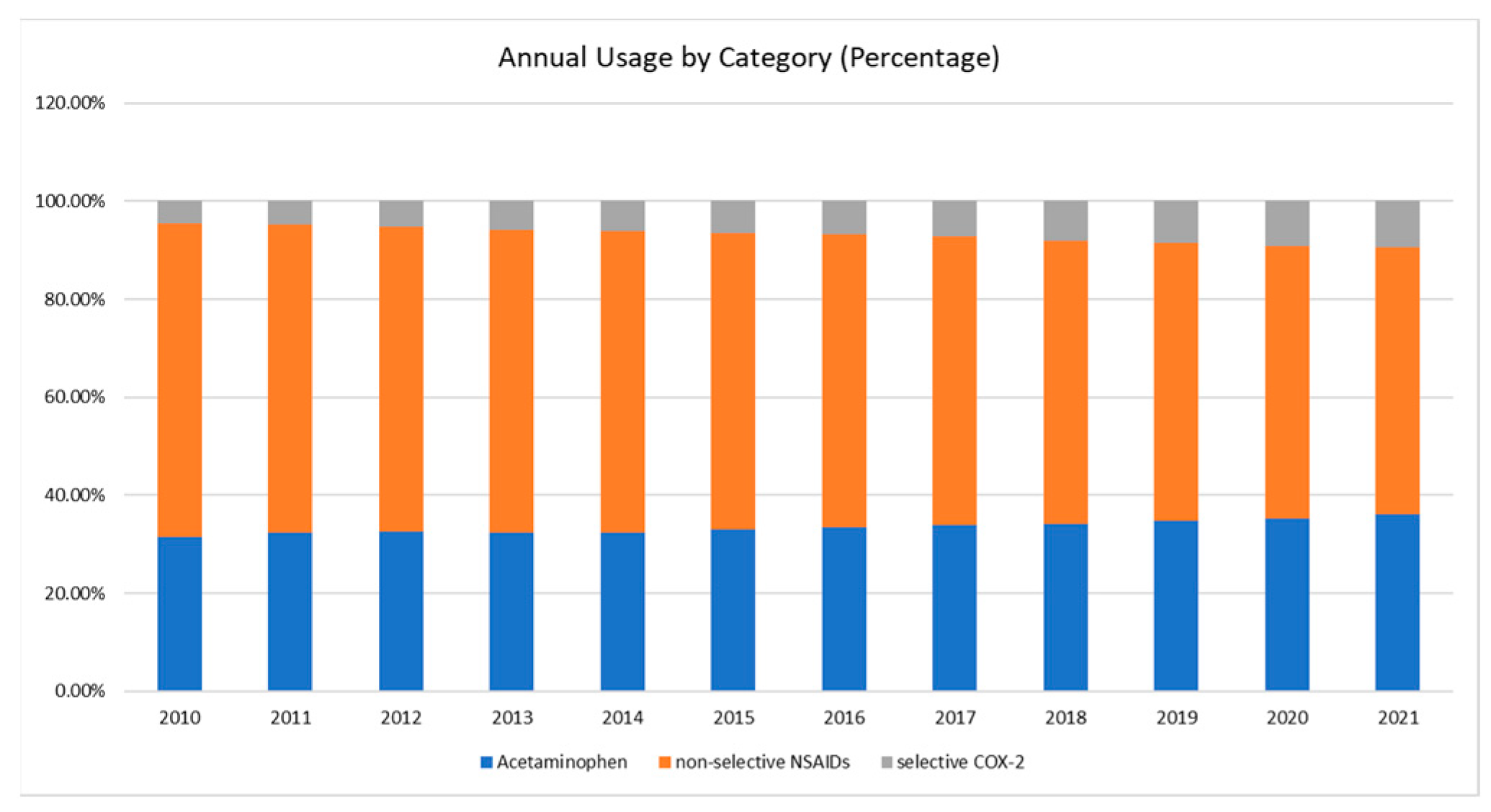
We compared annual usage by each category to find the prescription trends shown in Figure 1. Figure 1 shows that the non-selective NSAIDs are the largest in usage, acetaminophen is the second most used, and selective COX-2 (coxibs) have the smallest use in non-narcotic analgesics. Figure 1 also shows that all the analgesics and PPIs are increasing in amount each year; only the non-selective NSAIDs decreased from 2020 to 2021. We illustrated the annual usage of the non-narcotic analgesics in percentage terms in Figure 2, which shows the portions of the three categories clearly.
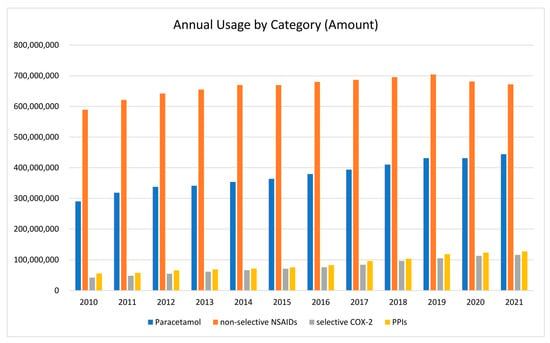
Figure 1.
Annual usage by each category in amount from 2010 to 2021.
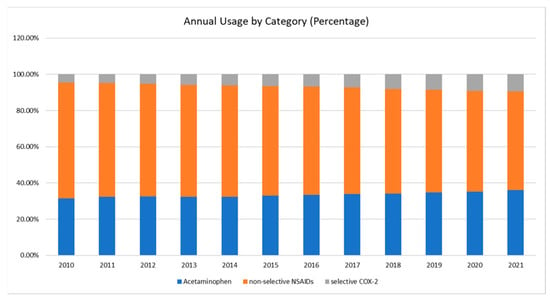
Figure 2.
Annual usage of the non-narcotic analgesics in percentage from 2010 to 2021.
3.2. Annual Growth Rate by Category
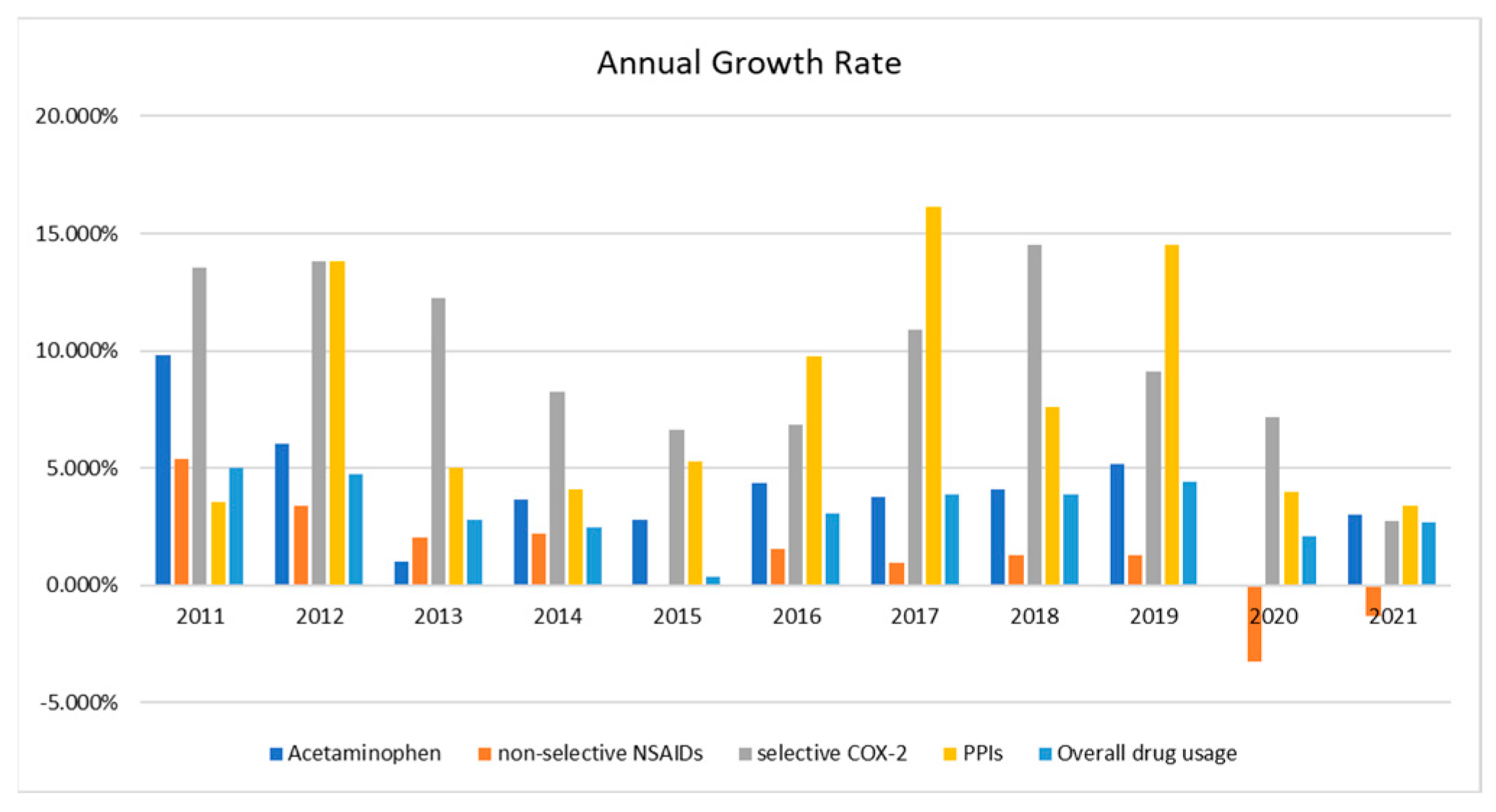
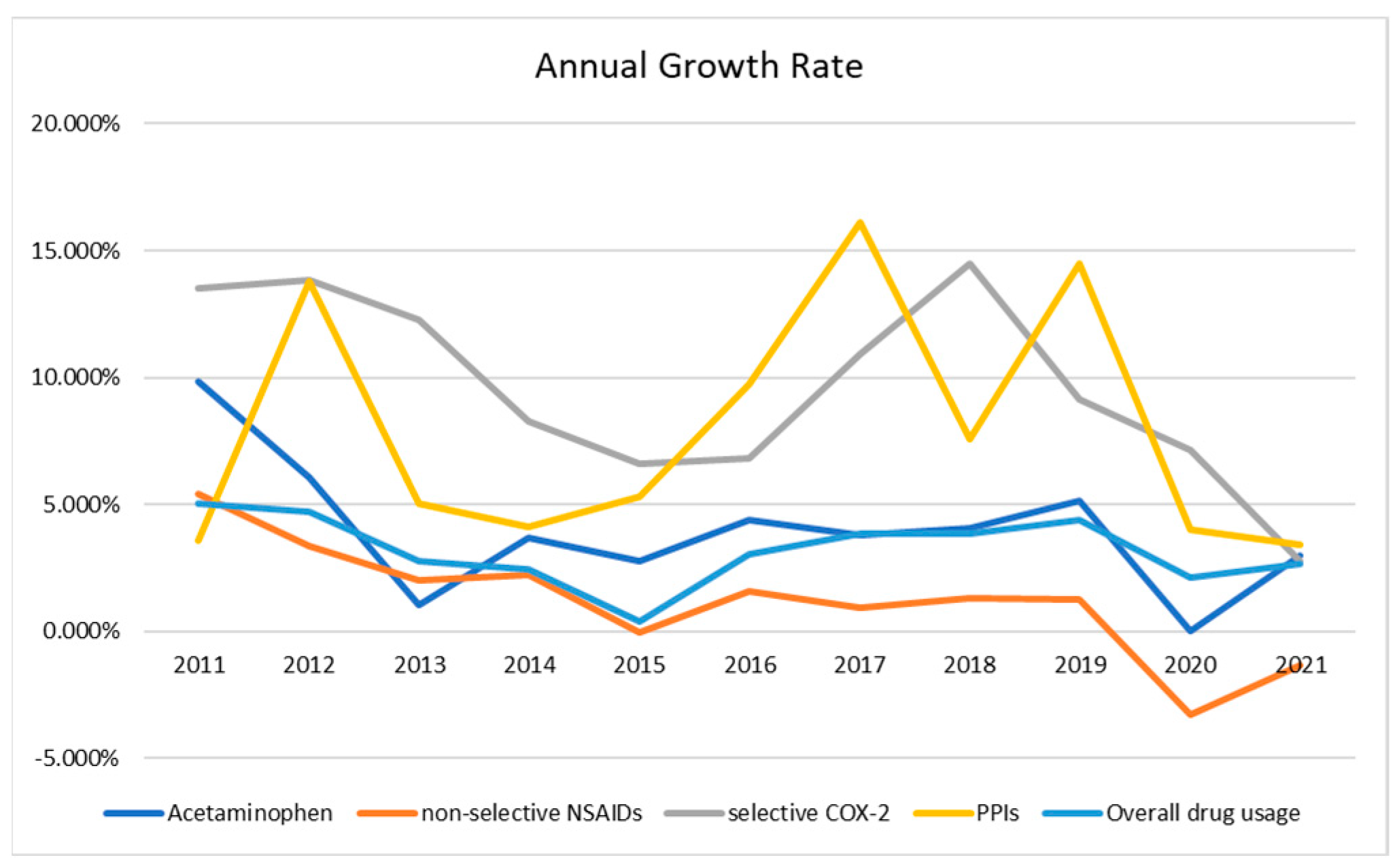
We calculated the annual growth rate of usage by each category, and we also listed the growth rate of the annual usage of all drugs as an overall trend to see how the usage of non-narcotic analgesics and PPIs varies compared with the overall trend of all drug usage. The result is illustrated in Figure 3. We could see drug usage increasing every year; only the non-selective NSAIDs decreased in 2020 and 2021. Figure 4 shows the trends in a line graph. We see that the annual growth rates of selective COX-2 and PPIs are greater than those the overall drug usage, the growth rate of acetaminophen is closer to the overall trend, and the growth rate of non-selective NSAIDs is lower than the overall growth rate.
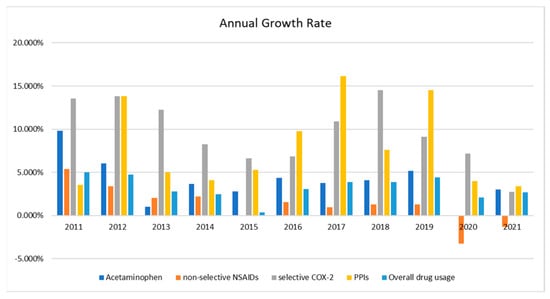
Figure 3.
The annual growth rate of usage by each category and overall drug usage.
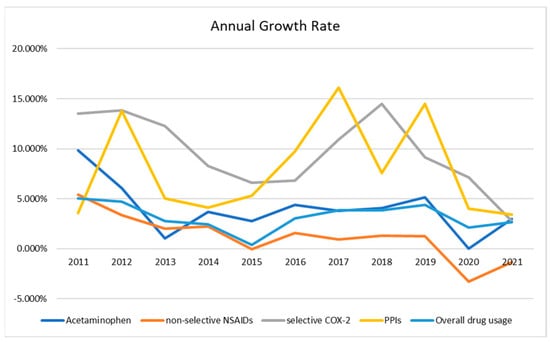
Figure 4.
The annual growth rate of usage by each category and overall drug usage by line graph.
3.3. Annual Use Percentage of Each Drug
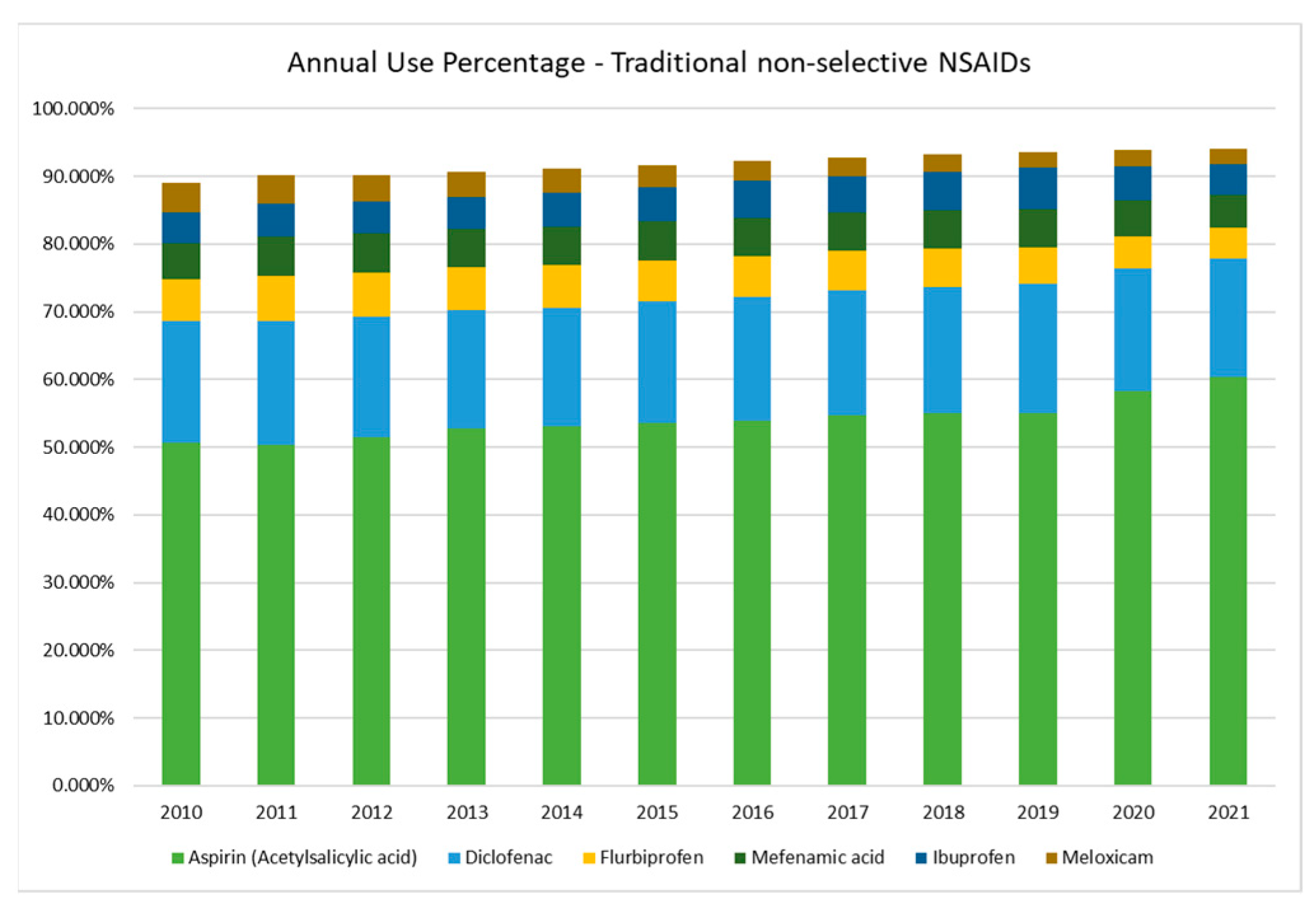
We calculated the use percentage of each drug in three categories of the traditional non-selective NSAIDs, the selective COX-2, and the PPIs. We found there are some drugs in a dominant position in the traditional non-selective NSAIDs. Thus, we illustrated the six most dominant non-selective NSAIDs, covering over 90% of the usage in 18 drugs, in Figure 5. Aspirin (acetylsalicylic acid) takes the largest proportion, with over 50% of annual usage. Diclofenac is the second largest at about 18% of usage. Flurbiprofen, mefenamic acid, ibuprofen, and meloxicam follow, with use rates of around 5% or less.
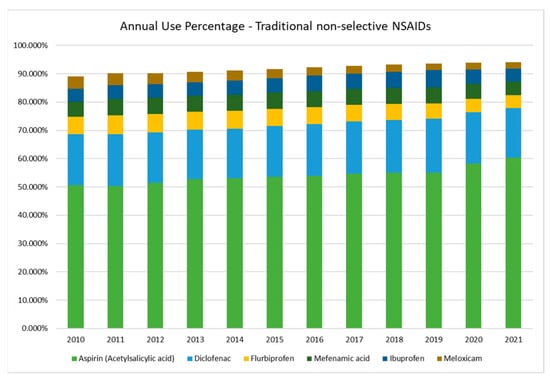
Figure 5.
The annual use percentage of six traditional non-selective NSAIDs.
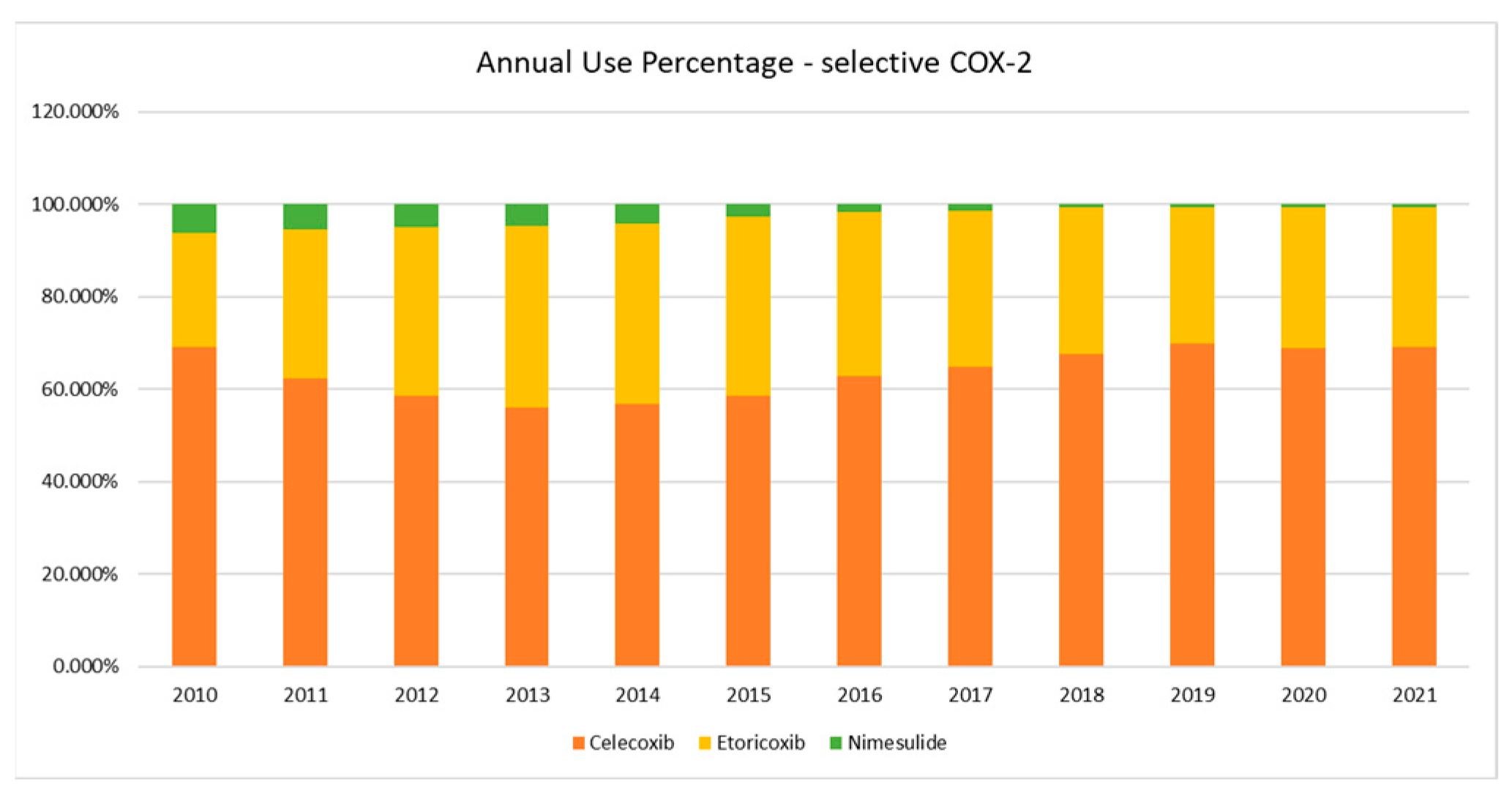
In Figure 6, there are three drugs in the selective COX-2 (coxibs). Celecoxib takes over 60% of annual selective COX-2 usage. Etoricoxib is the second largest, taking over 20% of usage. Nimesulide is the third, with usage of less than one percent in recent years.
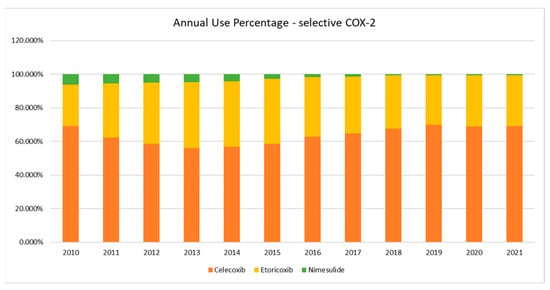
Figure 6.
The annual use percentage of three selective COX-2 (coxibs).
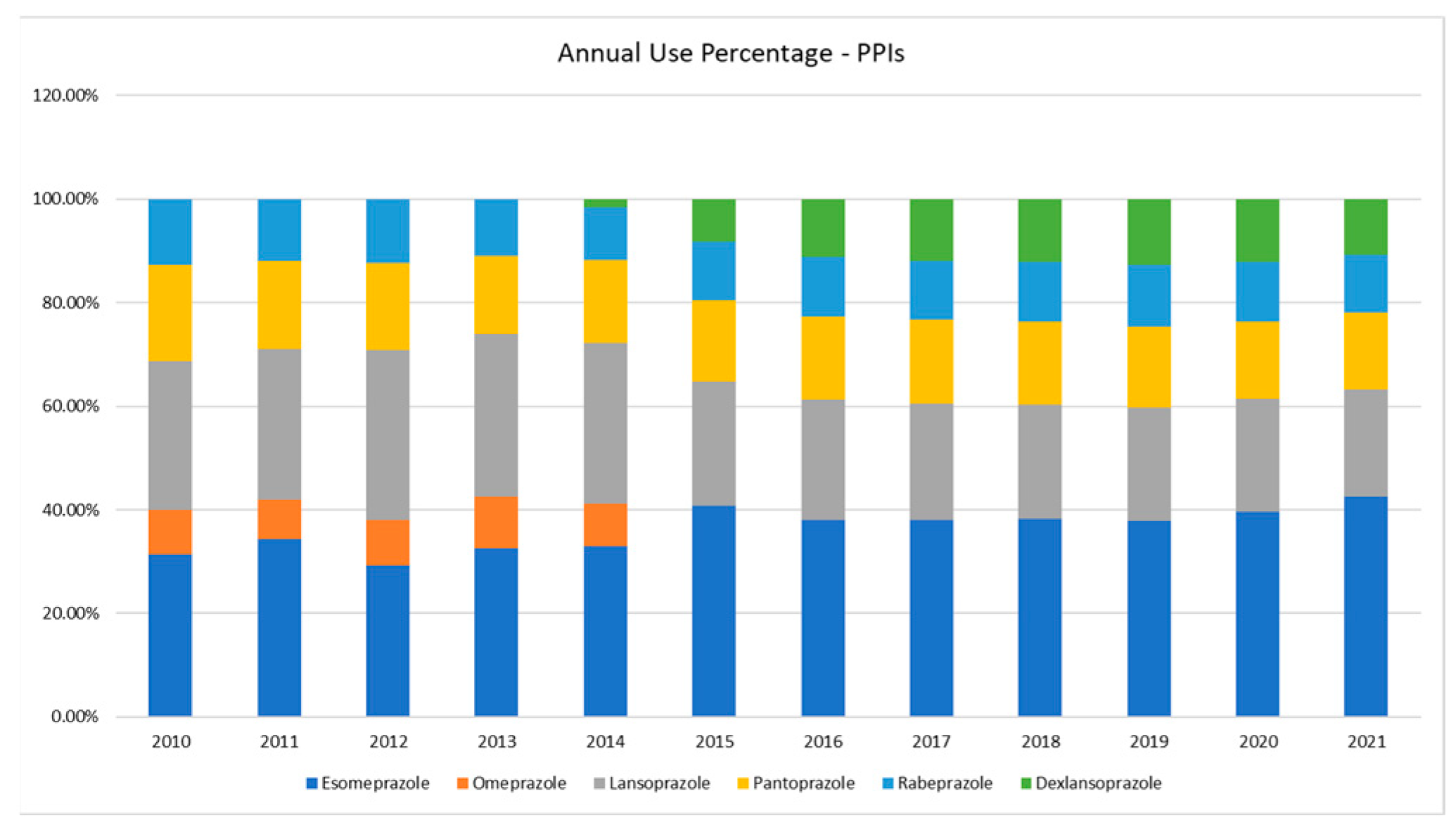
Six PPIs are illustrated in Figure 7. Esomeprazole takes the largest proportion of the usage of PPIs. The usage of Omeprazole in Taiwan’s NHI Annual Statistical Report has been aggregated with Esomeprazole since 2015. The proportion of Esomeprazole/Omeprazole accounts for around 40% of the annual PPIs usage. Lansoprazole is the second largest, taking over 20% of usage. Pantoprazole and rabeprazole are the third and the fourth, with under 20% use. It is remarkable that the usage of dexlansoprazole is increasing rapidly. The usage proportion of dexlansoprazole has taken over 10% of usage since 2016. There is only one drug, paracetamol (acetaminophen), in the paracetamol category, and so there is no need to figure the graph.
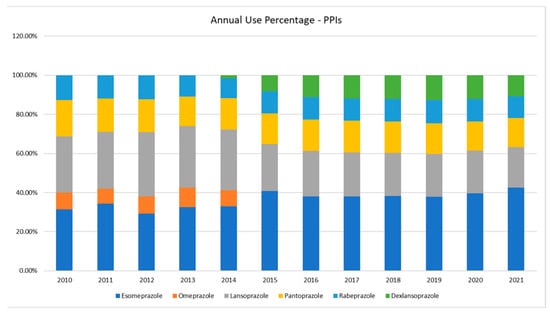
Figure 7.
The annual use percentage of six PPIs.
4. Discussion
Figure 1 and Figure 2 help us to answer the question of the prevalence and the trend of non-narcotic analgesics. The traditional non-selective NSAIDs take the largest proportion of usage over 60%, which is twice as many as the acetaminophen. The selective COX-2 (coxibs) takes the smallest proportion of the non-narcotic analgesics usage, but grows rapidly. In Figure 4, we can see the selective COX-2 has the highest annual growth rate. The annual growth rate of acetaminophen is also greater than the annual growth of overall drug usage. The traditional non-selective NSAIDs show a lower annual growth rate. Their use had been decreasing since 2020. The reason for this could be that the selective COX-2 are taking the place of the traditional non-selective NSAIDs. Although NSAIDs are widely used, acetaminophen still takes an important place—one-third of non-narcotic analgesic usage. It is noteworthy that the PPIs also have a high growth rate of annual usage over the growing trend of overall drug usage. This means the usage of PPIs did not decrease with the use of the selective COX-2 (coxibs). The result implies that it is necessary to further investigate the prescription pattern of the NSAIDs and PPIs, especially the combined use of selective COX-2 (coxibs) and PPIs.
Figure 5, Figure 6 and Figure 7 help us to answer the question of what the most commonly prescribed non-narcotic analgesics and PPIs in Taiwan’s NHI are. Aspirin (Acetylsalicylic acid), diclofenac, flurbiprofen, and mefenamic acid are the four most commonly prescribed traditional non-selective NSAIDs. They take over 80% of the annual usage. Aspirin takes the largest proportion, at over 50%. Celecoxib and etoricoxib are the two most commonly prescribed selective COX-2 (coxibs). They take 90% of the selective COX-2 usage. Esomeprazole/omeprazole, lansoprazole, and pantoprazole are the four most commonly prescribed PPIs. They take over 80% of the annual PPI usage.
This study gives us two important findings. The usage of PPIs is not decreasing with the use of the selective COX-2 (coxibs); on the contrary it is increasing rapidly. It is necessary to investigate the prescription pattern of the NSAIDs and PPIs, especially the combined use of selective COX-2 (coxibs) and PPIs. We identify the most commonly prescribed NSAIDs and PPIs in Taiwan’s NHI. We can focus on these drugs to investigate the prescription pattern of the NSAIDs and PPIs using Taiwan National Health Insurance Research Database in future research.
Author Contributions
Writing—original draft, I.-W.L.; Validation, J.C.Y.; Writing—review & editing, I.-W.L.; Supervision, J.-S.C.; Project Administration, C.-N.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by a grant from the Clinical Trial Center of Kaohsiung Medical University Hospital (grant no. H111095).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are openly available in Taiwan’s NHI Annual Statistical Report (https://www.nhi.gov.tw/Content_List.aspx?n=5AA7CAFFF61CB16D&topn=5FE8C9FEAE863B46, accessed on 1 July 2023).
Acknowledgments
We thank the Center for Medical Informatics and Statistics of Kaohsiung Medical University for providing administrative support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sjøgren, P.; Elsner, F.; Kaasa, S. Non-opioid analgesics. In Oxford Textbook of Palliative Medicine; Cherny, N., Fallon, M., Kaasa, S., Portenoy, R.K., Currow, D.C., Eds.; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Meng, Q.; Zhang, Z.; Li, F.; Li, J.; Wang, N.; Guo, Z.; Wang, J.; Ye, X.; Li, Y. The prescription patterns and safety profiles of oral non-steroidal anti-inflammatory drugs in China: An 8-year real-life analysis. Ann. Palliat. Med. 2021, 10, 2224–2237. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Donnan, P.T.; Bell, S.; Guthrie, B. Non-steroidal anti-inflammatory drug induced acute kidney injury in the community dwelling general population and people with chronic kidney disease: Systematic review and meta-analysis. BMC Nephrol. 2017, 18, 256. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.-C.; Wang, J.T.-H.; Chen, T.-Y.; Peng, C.-H. Digital Health Care in Taiwan; Springer Nature: Berlin, Germany, 2022. [Google Scholar]
- Taiwan’s NHI Drug Database. Available online: https://www.nhi.gov.tw/QueryN_New/QueryN/Query1 (accessed on 1 July 2023).
- Taiwan’s NHI Annual Statistical Report. Available online: https://www.nhi.gov.tw/Content_List.aspx?n=5AA7CAFFF61CB16D&topn=5FE8C9FEAE863B46 (accessed on 1 July 2023).
- Bannwarth, B. Gastrointestinal safety of paracetamol: Is there any cause for concern? Expert Opin. Drug Saf. 2004, 3, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Tai, F.W.D.; McAlindon, M.E. Non-steroidal anti-inflammatory drugs and the gastrointestinal tract. Clin. Med. 2021, 21, 131. [Google Scholar] [CrossRef]
- Bonnesen, K.; Schmidt, M. Recategorization of non-aspirin nonsteroidal anti-inflammatory drugs according to clinical relevance: Abandoning the traditional NSAID terminology. Can. J. Cardiol. 2021, 37, 1705–1707. [Google Scholar] [CrossRef] [PubMed]
- Ghlichloo, I.; Gerriets, V. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs); StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ahmed, A.; Clarke, J.O. Proton Pump Inhibitors (PPI); StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Strand, D.S.; Kim, D.; Peura, D.A. 25 years of proton pump inhibitors: A comprehensive review. Gut Liver 2017, 11, 27. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).