Abstract
In 50% of typical (nonneurogenic) women, at least one urinary tract infection (UTI) will occur, with cystitis being the most common UTI, with about 25% of patients experiencing recurrence. A factor not currently included in UTI risk models is egress of urine from the bladder into the urethra during bladder filling and activities of daily living. Urinary egress, if it occurs, would shorten the distance that bacteria need to travel to gain access to the bladder. Video urodynamics with contrast medium can demonstrate urinary egress; however, the observations can be difficult to conduct. Egress can be expected to be more likely in women with lower urinary tract conditions such as urge and stress incontinence. Treatment of the incontinence also reduces UTI rates and the reduction could, in part, be due to reduced urine egress. If UTI risk remains after incontinence management, then further treatment with pelvic floor exercises and pessaries could be considered to reduce the risk from potential residual urine egress. In summary, urine egress as a risk factor for UTI needs further research and clinical consideration.
1. Introduction
Female micturition is coordinated in the pontine micturition center and is under conscious control. The skeletal urethral sphincter relaxes during voiding [1]. Bladder filling is associated with a closed urethra, which is important in preventing urinary tract infection (UTI) [2]. Women, however, are at greater risk for UTI, with 50% experiencing at least one UTI and about 25% developing recurrence [2,3,4]. Thirteen UTI risk factors have been identified; however, urine egress from the bladder into the urethra during bladder filling is not included in that list [3,4,5]. Urine egress may have been overlooked because it is difficult to measure. This opinion report is about the further consideration of egress as a risk factor for UTI. Not included in this review are neurogenic bladder conditions, such as spinal cord injury, nor patients using catheters [6].
2. Risks for Urinary Tract Infections
Urinary tract infections are usually caused by pathogenic bacteria living in the gut that gradually migrate to the periurethral area. Colonization of the urethra is followed by colonization of the bladder and the onset of resistant biofilms [4,7]. Identification of UTI is demonstrated by a positive urine dipstick for nitrite and leuco-esterase; furthermore, identification of causal organisms with microscopy, culture and urine sensitivity tests as well as antibiotic treatments are important parts of care [4]. Treatment of these infections is becoming more difficult because of antibiotic resistance [5].
Because of the high medical burden, UTI risk models are an important area of medical practice. Thirteen factors have been identified (Figure 1). There is a much higher rate of UTI in women than in men, which is associated with the short female urethra [8,9]. Prior UTI and the presence of biofilms is a risk factor for UTI [2,4]. Coitus is a risk factor because of vigorous pelvic movement and the induction of an overactive bladder (OAB), which can cause incontinence [7]. Urinary incontinence due to OAB or stress incontinence is a major risk factor for UTI [2,10]. Diabetes is a general risk factor for infections [3]. Vaginal infections that include the urethral meatus can result in UTI [4]. Pregnancy and menopause are associated with an increased rate of infections [3]. Personal hygiene practices can be a problem [5]. The short distance between the urethral meatus and the anus is associated with increased UTI risk [4]. Furthermore, the use of contraception and antimicrobials and general health conditions are associated with an increased risk of UTI [2,4,7].
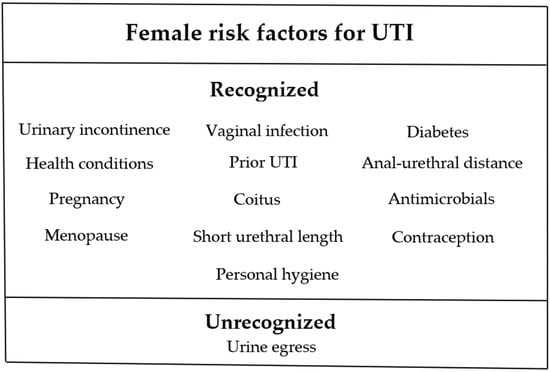
Figure 1.
Thirteen recognized and one unrecognized risk factors for UTI. Urinary incontinence represents various etiologies, each with a different risk factor (see text). Urine egress is the unrecognized risk factor being discussed in this report.
Even with the many factors included in UTI risk models, there remains limited accuracy in predicting when a new infection will occur [2,4]. In addition, risk models have not considered risk from urine egress, a condition in which urine in the bladder enters the urethra during bladder filling and during daily life activities and that is different from the entry of urine into the urethra that occurs during micturition. Our hypothesis is that urine egress is an important UTI risk factor (Figure 1). Egress can be described as the failure of passive and active urethral closure mechanisms [11]. The female urethra is much shorter than that of males, making egress a more significant concern for women. Considering the average adult female urethra measures 3.0 + 0.4 cm, urine egress seems to be an obvious risk factor for UTI since it reduces the distance that bacteria must traverse to gain access to the bladder [7,8,9].
3. Physiology of Urethral Closure and Urine Egress
The physiology of urethral closure suggests a possible mechanism of urine egress. During bladder filling, the urethra primarily remains closed by the passive mechanism of mucosal coaptation, smooth muscle, connective tissue, and vasculature [8,9,11]. Associated with elevated bladder pressures, as occurs with OAB, these passive mechanisms of urethral closure can be compromised, which will increase the likelihood of urine egress. In addition, due to the skeletal urethral sphincter, there is also a urethral closure tone. Skeletal sphincter tone can be reduced by prior parturition, menopause, and prolapse, increasing the likelihood of urine egress [12,13].
4. Diagnosis of Urine Egress
High-quality ultrasound is safe and easy to conduct for the measurement of egress; however, it is limited to observations of an open bladder neck [13]. The preferred method for egress measurement is video urodynamics [12,13]. This diagnostic radiology procedure involves moderately small-diameter catheters (small-diameter catheters have high resistance to passage of the viscous medium) and filling the bladder with radiopaque medium. Detrusor pressure is recorded as bladder pressure minus abdominal pressure. It is important to distinguish between urine in the urethra during micturition and unwanted urine egress into the urethra during bladder filling. During micturition, pathogens are washed out of the urethra, which reduces UTI risk [2,3]. Urine egress during bladder filling, on the other hand, is expected to contribute to UTI risk. Thus, the diagnostic procedure should be conducted at 50 to 70% bladder capacity to avoid the effects of micturition. The diagnostic radiology procedure should include maneuvers such as increased abdominal pressure and cough, which should be carried out in supine and sitting positions to fully assess urine egress [13]. A normal bladder–urethra relationship with no egress on the fluoroscopic screen is indicated by a sharp angle at the junction of the bladder and urethra (Figure 2A). Limited egress is demonstrated by opening of the bladder neck (Figure 2B), and large egress is shown by radiopaque medium being present farther down the urethra toward the meatus (Figure 2C). To complete the video urodynamic procedure, micturition should be observed with further filling of the bladder. Attention should be directed toward urine egress prior to and after voiding. After egress is observed and established as a risk in UTI risk model studies, further research would be needed to determine the best methods to manage egress to reduce UTI risk.

Figure 2.
Illustration of video urodynamics during bladder filling with radiopaque medium for the diagnosis of urine egress. The procedure should be carried out at 50 to 70% cystometric capacity to ensure that observations of urine egress are not associated with micturition (see text). (A) No urine egress is indicated by a normal radiographic bladder neck with a sharp bladder–urethra delineation. (B) A funneled bladder neck indicating limited egress. (C) radiographic medium extending further down the urethra indicates large urine egress. The procedure should include maneuvers such as cough and in sitting and prone positions. Arrow marks the urethral meatus.
Despite the potential for video urodynamics to identify urine egress into the urethra, this diagnostic procedure is often limited by the presence of the pelvic bones and a bladder base that can obscure the bladder neck. For example, the presence of a cystoceles can obscure the bladder–urethra junction [13]. In addition, video urodynamics is seldom used in female clinics because of long procedure times and radiation exposure. Due to the difficulties of conducting video urodynamics, it will probably be conducted first in the research setting.
5. Possible Urine Egress in Clinical Practice
Female lower urinary tract conditions such as urge and stress incontinence may provide insight into urine egress as a possible risk factor for UTI. Urinary incontinence, the unplanned loss of urine, has characteristics similar to urine egress, in that urine is in the urethra at inappropriate times. Urge incontinence due to OAB increases bladder pressure during bladder filling, which can open the bladder neck and urethra, a condition for urine egress [5,10]. A variety of bladder-inhibitory interventions are available for OAB, including anticholinergics and Beta-3-adrenergic agonists as well as neuromodulation, including electrical and magnetic stimulation, pelvic floor muscle training, and behavioral bladder training [7,14]. These interventions decrease bladder pressure, manage incontinence, and reduce UTI risk. The reduced UTI risk could, in part, be due to decreased urine egress. In addition, if UTI risk persists after the incontinence is managed, additional bladder-inhibitory interventions might be considered to reduce possible residual OAB and urine egress to manage the remaining UTI risk [14].
Previous UTIs are associated with lingering biofilms, which is a risk factor for reoccurrence [2,4]. The prior infection, however, may also produce residual OAB and urine egress, and further use of bladder-inhibitory interventions to reduce the continuing UTI risk resulting from these possible factors should be considered. Likewise, for some women, coitus is associated with OAB, incontinence, and UTI risk [4,5]. Urine egress could also possibly be involved in this UTI risk. Thus, the use of bladder-inhibitory medication prior to coitus could be considered to reduce the UTI risk.
Stress incontinence caused by a hypermobile urethral and prolapse are also associated with increased UTI risk [11,12,13]. Treatments for stress incontinence, including pelvic floor exercises, pessaries, or surgical sling procedures, usually manage both the incontinence and the UTI risk [7,13]. After incontinence treatment, however, if UTI risk remains, additional pelvic floor exercises and the use of vaginal pessaries should be considered, which could reduce possible residual urine egress and UTI risk. A limitation of pessary treatment, however, is that they can be irritating and can be associated with increased UTI risk [7,13]. There are many types of pessaries, and different ones would need to be evaluated to reduce UTI risk.
For general UTI risk management, interventions include urine alkalization, vaginal hygiene, preventive antibiotics, and incontinence management [2,3,4]. Additionally, interventions to decrease possible urine egress for UTI risk reduction should also be considered.
6. Conclusions
Urine egress from the bladder into the urethra during bladder filling may be an unrecognized risk factor for UTI. Egress can be diagnosed by high-quality ultrasound and video urodynamics, although these procedures have limitations. Current treatments for urinary incontinence reduce UTI risk, and some of this reduction may be due to decreased urine egress. Thus, if UTI risk persists after incontinence management, then treatment with pelvic floor exercises and pessaries may be warranted to address potential UTI risk from residual urine egress.
Author Contributions
Conceptualization, writing—review and editing: J.W. (James Walter), J.W. (John Wheeler), and A.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank Achim Herms for his guidance with this submission. The current authors are members of an International Neuro-Urology Research Group, which was formed with the goal of fostering research into reducing the risk of UTI.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fowler, C.J.; Griffiths, D.; de Groat, W.C. The neural control of micturition. Nat. Rev. Neurosci. 2008, 9, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: Epidemiology, mechanisms of infection and treatment options. Nat. Rev. Microbiol. 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. The epidemiology of urinary tract infection. Nat. Rev. Urol. 2010, 7, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Franco, A.V. Recurrent urinary tract infections. Best Pract. Clin. Obstet. Gynaecol. 2005, 19, 862–873. [Google Scholar] [CrossRef]
- Kodner, C.M.; Gupton, T.E.K. Recurrent urinary tract infections in women: Diagnosis and management. Am. Fam. Physician 2010, 82, 638–643. [Google Scholar] [PubMed]
- Musco, S.; Giammò, A.; Savoca, F.; Gemma, L.; Geretto, P.; Soligo, M.; Sacco, E.; Del Popolo, G.; Marzi, V.L. How to Prevent Catheter-Associated Urinary Tract Infections: A Reappraisal of Vico’s Theory—Is History Repeating Itself? J. Clin. Med. 2022, 11, 3415. [Google Scholar] [CrossRef] [PubMed]
- Czajkowski, K.; Broś-Konopielko, M.; Teliga-Czajkowska, J. Urinary tract infection in women. Menopause Rev. 2021, 20, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, F.; Tu, L.M.; Carroll, M.S.; Morin, M. Agreement between simple catheter method and 3D transperineal ultrasound for assessing urethral length measurement before stress urinary incontinence treatment. Neurourol. Urodyn. 2018, 37, 2875–2880. [Google Scholar] [CrossRef] [PubMed]
- Kirby, A.C.; Tan-Kim, J.; Nager, C.W. Measurement of dynamic urethral pressures with a high resolution manometry system in continent and incontinent women. Female Pelvic Med. Reconstr. Surg. 2015, 21, 106–110. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Aoki, Y.; Brown, H.W.; Brubaker, L.; Cornu, J.N.; Daly, J.O.; Cartwright, R. Urinary incontinence in women. Nat. Rev. Dis. Primers 2017, 3, 17042–17086. [Google Scholar] [CrossRef] [PubMed]
- Sand, P.K.; Bowen, L.W.; Ostergard, D.R. The prognostic significance of augmentation of urethral closure pressure and functional length. Int. J. Gynaecol. Obstet. 1990, 33, 135–139. [Google Scholar] [CrossRef]
- Herschorn, S. Female pelvic floor anatomy: The pelvic floor supporting structures, and pelvic organs. Rev. Urol. 2004, 6 (Suppl. 5), 2–10. [Google Scholar]
- Ghoniem, G.; Stanford, E.; Kenton, K.; Achtari, C.; Goldberg, R.; Mascarenhas, T.; Parekh, M.; Tamussino, K.; Tosson, S.; Lose, G.; et al. Evaluation and outcome measures in the treatment of female urinary stress incontinence: International Urogynecological Association (IUGA) guidelines for research and clinical practice. Int. Urogynecol. J. Pelvic Floor Dysfunct. 2008, 19, 5–33. [Google Scholar] [CrossRef] [PubMed]
- Khizer, Z.; Sadia, A.; Sharma, R.; Farhaj, S.; Nirwan, J.S.; Kakadia, P.G.; Hussain, T.; Yousaf, A.M.; Shahzad, Y.; Conway, B.R. Drug Delivery Approaches for Managing Overactive Bladder (OAB): A Systematic Review. Pharmaceuticals 2021, 14, 409. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).