Abstract
Background/Objectives: Systemic arterial hypertension (SAH) is a multifactorial condition strongly associated with increased morbidity and mortality. This study aimed to investigate the prevalence of SAH and its associated factors among female workers in a large company in Southern Brazil. Methods: A cross-sectional study was conducted with a sample of 451 female workers aged 18 years or older. Blood pressure (BP) was measured using an automated digital upper-arm device. SAH was defined as systolic BP and/or diastolic BP ≥ 140/90 mmHg or the use of antihypertensive medications. Prevalence ratios were estimated using Poisson regression with robust variance. Results: The mean age of the sample was 35 ± 10 years. The prevalence of SAH was 27.7% (95% CI: 23.6–31.9). Among workers with obesity (BMI ≥ 30 kg/m2), the prevalence of SAH reached 42.8%. In multivariable-adjusted models, workers aged ≥41 years had a 48% higher probability of having SAH (PR = 1.48; 95% CI: 1.01–2.18) compared with younger women (18–30 years). Conversely, a 52% lower probability of SAH was observed among workers with higher monthly per capita income (>2 minimum wages) compared with those earning <1 minimum wage (PR = 0.48; 95% CI: 0.28–0.80). Obesity was associated with an 85% increased probability of SAH (PR = 1.85; 95% CI: 1.30–2.47). Conclusions: The findings of this study revealed that SAH is prevalent in this specific population of female workers, particularly among older women and those with obesity.
1. Introduction
Systemic arterial hypertension (SAH) is a multifactorial clinical condition, defined as a persistent elevation of blood pressure levels ≥ 140 and/or 90 mmHg [1]. Within the spectrum of cardiovascular diseases, SAH and its consequences—such as stroke, coronary artery disease, heart failure, chronic kidney disease, and peripheral vascular disease—represent the leading causes of morbidity and mortality worldwide [2].
Epidemiological data indicate that, in 2015, the global prevalence of SAH was 24.1% among men and 20.1% among women, with the number of adults with SAH increasing from 594 million in 1975 to 1.3 billion in 2015 [3]; moreover, the number of individuals aged 30–79 years with SAH nearly doubled between 1990 and 2019 [4]. In the United States, between 2017 and 2018, the prevalence of SAH among adults was 45.4%, affecting 51% of men and 39.7% of women [5]. In Brazil, according to the National Health Survey, the self-reported prevalence of SAH among adults was 21.4% [6]; however, the prevalence was estimated at 32.3% when blood pressure measurements and the use of antihypertensive medication were considered (BP ≥ 140/90 mmHg and/or use of antihypertensive medication) [7,8]. Furthermore, a cross-sectional study conducted in Brazilian capitals with data from the Surveillance System for Risk Factors and Protection for Chronic Diseases by Telephone Survey (VIGITEL) reported a prevalence of approximately 24% among the general adult population from 2006 to 2019 [9].
Previous studies have reported heterogeneous prevalence rates of SAH among Brazilian workers. In Rio Grande do Sul, prevalence reached 10.3% among industrial workers, including 9.4% among women [10], while female cleaning workers in Bahia showed 13.6% [11]. Higher estimates were reported in Paraná, with 26% among higher education employees, predominantly women [12], and in Minas Gerais, with 21.8% among healthcare workers [13]. The highest prevalence was observed in Recife, Pernambuco, at 36.6% [14].
SAH is a complex condition influenced by multiple risk factors, which can be categorized as non-modifiable or modifiable. Non-modifiable factors include sociodemographic characteristics and family history [10], whereas modifiable risk factors comprise behaviors and conditions that can be directly targeted, such as smoking, excessive alcohol consumption, unhealthy dietary patterns, elevated body mass index (BMI), high salt intake, physical inactivity, and both occupational and non-occupational stress [15,16,17]. Additionality, obesity is strongly associated with SAH and is considered one of its main determinants. Both conditions are highly prevalent and often coexist independently, significantly increasing the risk of cardiovascular complications. Excess weight commonly leads to elevated blood pressure, whereas weight loss is typically associated with its reduction [18].
Given the increasing prevalence of SAH in recent years and the influence of socioeconomic, behavioral, environmental, and health-related factors, the present study aimed to investigate the prevalence of SAH and its associated factors in a specific population of female workers employed at a large company in Southern Brazil. Despite increasing global attention to cardiovascular health disparities, evidence regarding SAH and its determinants among female workers in occupational settings in Latin America remains limited. Female workers constitute an important and expanding segment of the labor force. Therefore, this study addresses a relevant public health concern by examining the prevalence and associated factors of SAH in a specific female occupational group in Southern Brazil, thereby contributing novel evidence and helping fill an important gap in the regional and occupational health literature.
2. Materials and Methods
2.1. Study Design
This was a cross-sectional, occupation-based study conducted with a sample of adult female workers from different shifts in a business group located in Southern Brazil. The study is part of a broader research project entitled “Health Conditions of Female Shift Workers: Longitudinal Study of Women’s Occupational Health (ELO-SAÚDE)”. The primary objective was to investigate and analyze the health conditions and characteristics of female workers from this company. The study was submitted to and approved by the Research Ethics Committee of the University of Vale do Rio dos Sinos (CAAE no. 53762521.7.0000.5344/approval no. 5681627). All participants provided informed consent in accordance with the Brazilian National Health Council Resolution 466/2012 and with the Helsinki Declaration.
2.2. Sample and Sampling
All female employees of a business group specializing in the manufacture of household plastic products, located in Southern Brazil, aged 18 years or older, were considered eligible for the study. Inclusion criteria required women to be at least 18 years old and working fixed shifts. Exclusion criteria comprised pregnant women, those in the postpartum period, and those employed for less than three months. Both industrial plant (production) workers and administrative staff were included, all of whom had an approximately 40-h weekly workload. Production employees worked six days per week with one day of rest, whereas administrative staff worked five days per week with two rest days. The production sector primarily consisted of machine operators responsible for operating and monitoring manufacturing equipment, as well as production workers who performed manual tasks such as finishing, assembling, labeling, and packaging plastic household utensils. These activities were characterized by low to moderate physical demands and exposure to ergonomic stressors related to repetitive motions and sustained postures. In contrast, administrative workers primarily performed computer-based activities in a predominantly seated position, involving low physical demand but prolonged static posture and limited variation in movement.
2.3. Data Collection and Instruments
Data were collected between August 2022 and February 2023 using a standardized, pre-coded, and pre-tested questionnaire administered through face-to-face workplace interviews. The questionnaire addressed demographic, socioeconomic, occupational, behavioral, health, and anthropometric characteristics. Interviewers underwent training prior to data collection, which included a pilot study of 21 interviews conducted before the start of fieldwork. Quality control was ensured through interviewer supervision and verification of 10% of the collected data, with partial questionnaire re-administration via telephone to assess response consistency. Data quality was verified by randomly repeating 10% of the interviews via telephone using a simplified questionnaire focused on stable variables (e.g., education level). No discrepancies were identified, indicating reliable data collection. Data coding was carried out by the interviewers under the supervision of the research coordination team.
2.4. Outcome: Systemic Arterial Hypertension (SAH)
Blood pressure was measured using an automated digital upper-arm device (OMRON®, model HEM 7200, OMRON Healthcare, São Paulo, Brazil). Participants were instructed to remain seated, silent, and at rest for at least five minutes before measurement. Blood pressure was taken twice, at different times, with a minimum interval of five minutes between readings; the mean of the two measurements was used for analysis. Women were classified as having SAH if they presented systolic and/or diastolic blood pressure ≥ 140/90 mmHg or reported the use of antihypertensive medications [1,4].
2.5. Covariates (Associated Factors)
For this study, variables were selected based on demographic, socioeconomic, occupational, behavioral, and health characteristics of female workers in Southern Brazil. Demographic variables included age in completed years and categorized into approximately 10-year age groups: 18–30, 31–40, and ≥41 years; self-reported skin color, classified as White or Other (mixed-race, Black, Indigenous, Asian); and marital status, categorized as living with or without a partner. Socioeconomic variables included per capita household income, calculated as the total monthly income of all household members divided by the number of residents. Income was expressed in units of the national minimum wage in 2022 (BRL 1212.00) and categorized based on the sample mean into <1, 1–2, and >2 minimum wages; educational attainment was measured in years of schooling and categorized based on the sample median as ≤8, 9–11, and >11 years. Occupational characteristics included work shift, determined according to reported start and end times, and classified as day shift (06:00–22:00) or night shift (22:00–06:00); length of employment was reported in months and categorized based on the sample median as ≤12, 13–36, and >36 months; job role, refers to the position held at the time of the interview, categorized as factory (production) or administrative work; and occupational stress, measured using the Job Stress Scale—short version, validated in Brazilian Portuguese [19].
Behavioral variables included leisure-time physical activity, assessed by the question “In the past week, did you engage in any physical activity for leisure, sports, or exercise, excluding commuting?”; self-reported sleep quality, measured by the question “During the past month, how would you rate your overall sleep?” with response options grouped as very good/good or poor/very poor; daily meal frequency was assessed based on the reported number of meals usually consumed per day (including breakfast, morning snack, lunch, afternoon snack, dinner, evening snack, and midnight snack) and categorized according to the sample median as ≤3 or >3 meals per day; smoking status, categorized as never smoked, former smoker, or current smoker; and alcohol consumption (no—no intake or intake less than once per week; yes—at least once per week in the previous year). Health-related variables included Body mass index (BMI), calculated as weight (in kilograms) divided by height (in meters) squared, was assessed using the mean of two body weight measurements obtained with a digital scale (OMRON®, model HN-289, OMRON Healthcare, São Paulo, Brazil) and two height measurements obtained with a portable stadiometer (BALMAK®, model EST-223, BALMAK, São Paulo, Brazil); general obesity (BMI ≥ 30 kg/m2) was classified according to World Health Organization (WHO) criteria [20]; and self-rated health was measured using a five-point Likert scale, with responses categorized as excellent, very good, good, fair, or poor.
2.6. Statistical Analysis
Data entry was performed in duplicate using EpiData version 3.1 to minimize potential typing errors. Statistical analyses were conducted using Stata version 12 (StataCorp, College Station, TX, USA). Categorical variables were presented as absolute and relative frequencies, and numerical variables were expressed as mean (standard deviation [SD]) and median (interquartile range [IQR]). Prevalence estimates were calculated and reported with their respective 95% confidence intervals (95% CI).
For the bivariate analysis, Pearson’s chi-square test was applied, with p-values for heterogeneity in dichotomous categorical variables and for linear trend in ordinal categorical variables. The t-test was used for comparison of means, whereas the Mann–Whitney test was used for comparison of distributions. Unadjusted and adjusted (multivariable) analysis was performed using Poisson regression with robust variance to estimate prevalence ratios (PR) and their corresponding 95% CIs. Variable selection followed a forward stepwise conceptual framework [21], structured into three hierarchical levels: distal (demographic and socioeconomic variables), intermediate (behavioral and occupational variables), and proximal (health-related variables). Only variables with a significance level of p ≤ 0.20 in the bivariate analysis were included and retained in the multivariable analysis, which comprised four analytical models: Model I: unadjusted analysis; Model II: adjusted for distal level variables (age, marital status, and income); Model III: adjusted by model II (age and income) + intermediate level variables (physical activity, job role, and occupational stress); Model IV: adjusted for models II and III (age, income, and physical activity) + proximal level variables (general obesity and self-perception of health). Variables that remained statistically significant at the 5% level (p ≤ 0.05) after Poisson regression were considered associated with the outcome. An additional analysis was conducted to explore the correlation between BMI and systolic and diastolic blood pressure. The non-normal distribution of systolic and diastolic blood pressure and BMI was assessed and confirmed using the Shapiro–Wilk test (p < 0.001). Therefore, Spearman’s rank correlation coefficient (r) was applied to examine the association between these non-normally distributed continuous variables.
3. Results
Of the 546 eligible female workers, 452 were interviewed after accounting for losses and refusals, yielding a response rate of 82.8%. Thus, the final analytical sample consisted of 451 female workers, as one participant was excluded due to missing data on blood pressure. The mean age of the workers was 35.1 ± 10.1 years. As shown in Table 1, the majority of participants self-identified as white (69.6%), worked the day shift (78.3%), did not engage in leisure-time physical activity (71.6%), reported very good/good sleep quality, had never smoked (75.6%), did not reported alcohol consumption (70.1%), did not present occupational stress (78%), had been employed by the company for more than 36 months (49.5%), worked in the factory/production sector (78.9%), and rated their health between good and excellent (73%). On the other hand, approximately 30% of the workers were classified with obesity.

Table 1.
Overall sample characteristics and prevalence of systemic arterial hypertension (SAH) according to characteristics among female workers of a large company in Southern Brazil, 2022 (N = 451).
The overall prevalence of SAH was 27.7% (95% CI: 23.6–31.9). Table 1 presents SAH prevalence according to sample characteristics. Prevalence increased with age, as older workers showed higher rates of SAH (33.6%), as did those with lower income (33.1%), those not engaged in leisure-time physical activity (30.3%), and those with poorer self-rated health (36.4%). The highest prevalence was observed among female workers with obesity (42.8%), whereas the lowest was found among those with higher income (15.7%). Female workers with SAH had a higher median age than those without SAH (37 years, IQR: 29–43 vs. 34 years, IQR: 26–41; p = 0.038). Similarly, those with SAH showed a higher mean BMI than those without SAH (29.8 kg/m2, SD = 6.4 vs. 27.2 kg/m2, SD = 4.9; p < 0.001) (Table 1).
Table 2 shows unadjusted and adjusted prevalence ratios for SAH, according to variables with a p-value ≤ 0.20 in the bivariate analysis. After adjustment, workers aged ≥41 years had a 48% higher probability of having SAH compared with those aged 18–30 years (PR = 1.48; 95% CI: 1.01–2.18). Regarding income, participants with per capita household income > 2 minimum wages had a 52% lower probability of SAH compared with those earning <1 minimum wage (PR = 0.48; 95% CI: 0.28–0.80). At the proximal level, obesity remained significantly associated with SAH, as female workers with obesity had an 85% higher probability of SAH compared with those without obesity (PR = 1.85; 95% CI: 1.30–2.47). Conversely, the association between self-rated health and SAH lost statistical significance after multivariable adjustment.
Table 2.
Unadjusted and adjusted models of multivariate analysis for systemic arterial hypertension (SAH) among female workers of a large company in Southern Brazil, 2022 (N = 451).
Figure 1 illustrates the distribution of systolic and diastolic blood pressure values according to body mass index (BMI). A positive correlation was observed, with higher BMI corresponding to higher systolic (r = 0.386; p < 0.001) and diastolic (r = 0.436; p < 0.001) blood pressure.
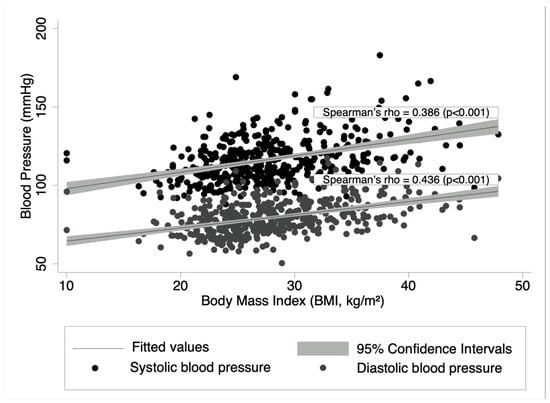
Figure 1.
Distribution (correlation) of systolic and diastolic blood pressure levels according to body mass index (BMI) among female workers of a large company in Southern Brazil, 2022 (N = 451).
4. Discussion
The present study investigated the prevalence of systemic arterial hypertension (SAH) and its associated factors among female workers employed in a large company in Southern Brazil. The findings of this study revealed that SAH is prevalent in this specific population. SAH was significantly more common among older participants, those with lower household income, and women with obesity. In addition, a clear positive association was observed between body mass index (BMI) and both systolic and diastolic blood pressure, underscoring the contribution of excess body weight to elevated cardiovascular risk in this population.
A prevalence of 27.7% (95% CI: 23.6–31.9) was identified in this occupational group. The SAH prevalence reported here is consistent with findings from other occupational settings in Brazil. For example, a population-based study among employees at a higher education institution in Paraná found a prevalence of 26%, predominantly among women [12]. Similar values were observed among urban cleaning and footwear industry workers in Salvador, Bahia (24%) [11], and among healthcare workers in Minas Gerais (21.8%) [13]. Conversely, higher prevalence estimates have been documented, such as 36.6% among workers in Recife, Pernambuco [14], suggesting regional heterogeneity and the potential influence of occupational, environmental, and socioeconomic contexts.
When compared to data from the general population, the SAH prevalence identified in this sample of female workers is also comparable. Previous data from the VIGITEL survey reported a prevalence of approximately 24% among the general Brazilian adult population [9]. Also, according to the 2023 VIGITEL survey, the prevalence of SAH in the adult population was 27.9%, including a prevalence of 33% in Porto Alegre (capital city of Rio Grande do Sul State) [22]. This convergence suggests that occupational exposure in this group may not differ substantially from population-wide determinants of SAH, while also highlighting that female workers in the industrial and administrative sectors are not exempt from the broader epidemiological burden of SAH in Brazil.
Previous studies have consistently demonstrated an association between older age and a higher likelihood of SAH [13,14,23,24]. A cross-sectional study involving 727 industrial workers in the metropolitan region of Recife, Pernambuco, showed that participants aged ≥40 years had a 72% higher probability of SAH (PR = 1.72; 95% CI: 1.24–2.39) compared to younger individuals [14]. Similarly, a study conducted among 490 healthcare workers in high-complexity services in Minas Gerais reported 160% increased odds of SAH among those aged ≥40 years (OR = 2.60; 95% CI: 1.30–5.00) [13]. Furthermore, a large cross-sectional investigation of 4818 Brazilian industrial workers indicated an even stronger association, with individuals aged 40–49 years presenting 180% higher odds of SAH (OR = 2.80; 95% CI: 2.30–3.42) relative to their younger counterparts [24].
The observed relationship between advancing age and increased SAH risk can be explained by biological changes inherent to the aging process. Among these are the stiffening of the aortic wall and the progressive increase in peripheral vascular resistance, both of which contribute to higher blood pressure levels over time [23]. The results of the present study, which demonstrate a significant association between older age and SAH among female workers, are therefore consistent with previous evidence in the literature, reinforcing the well-established role of aging as a key determinant of cardiovascular risk [13,14,23,24].
The relationship between income level and SAH has also been documented in the literature [10,25,26]. A cross-sectional study involving 20,792 industrial workers in Rio Grande do Sul reported that those with lower monthly earnings (<BRL 1201) had a 40% higher probability of SAH (PR = 1.40; 95% CI: 1.09–1.79) compared with higher-income workers [10]. Similarly, a study conducted with 606 nursing professionals in an emergency hospital in Porto Alegre found that individuals earning up to BRL 1200 had 65% higher odds of SAH (OR = 1.65; 95% CI: 1.20–2.28) relative to those earning above this threshold [26]. In contrast, another investigation reported that workers earning between two and four minimum wages had a 29% increased risk of SAH compared with those earning four or more minimum wages, although this association was not statistically significant in adjusted models (PR = 1.29; 95% CI: 0.71–2.36) [25].
The relationship between socioeconomic status and the development of SAH is complex. However, it is widely recognized that individuals with higher income are more likely to have access to healthcare services and to adopt healthier lifestyles. These may include lower smoking prevalence, greater engagement in physical activity, and healthier dietary habits, which collectively reduce the risk of SAH [25]. In this regard, the findings of the present study are consistent with previous evidence, reinforcing the notion that higher income acts as a protective factor against SAH.
Previous research has consistently identified obesity as a major factor strongly associated with SAH. A prior study reported a 148% higher probability of SAH among individuals with obesity (PR = 2.48; 95% CI: 1.86–3.30) [14]. Similarly, a cross-sectional study involving 1339 workers from 30 companies demonstrated 120% increased odds of SAH among those with elevated body mass index (BMI ≥ 25 kg/m2) (OR = 2.20; 95% CI: 1.30–3.60) [27]. In another study conducted with university professors in Viçosa, Minas Gerais, individuals with BMI > 24.49 kg/m2 exhibited 175% higher odds of SAH (OR = 2.75; 95% CI: 1.26–6.06) compared with their counterparts of normal weight [28].
The association between obesity and SAH can be explained by multiple interrelated pathophysiological mechanisms. These include the risk of chronic kidney injury due to renal compression by adipose tissue, activation of the renin–angiotensin–aldosterone system, and increased sympathetic nervous system activity. Additional mechanisms involve hyperinsulinemia and insulin resistance—both of which may contribute to elevated sympathetic tone, enhanced renal sodium reabsorption, endothelial dysfunction, altered angiotensin II receptor regulation, and impaired natriuretic peptide activity. Other contributing factors include obstructive sleep apnea, activation of the leptin–melanocortin pathway, and genetic predisposition [29].
When evaluating the distribution of systolic blood pressure (SBP) and diastolic blood pressure (DBP) according to body mass index (BMI) in this population, both measures of blood pressure increased proportionally with higher BMI. Notably, DBP appeared to be more strongly influenced by BMI than SBP. A study conducted in Presidente Prudente, São Paulo, similarly identified a relationship between BMI, SBP, and DBP, showing that higher BMI values were associated with higher blood pressure levels. Consistent with the present findings, that study used Pearson’s correlation coefficient and demonstrated that DBP was more strongly correlated with BMI (r = 0.226) than SBP (r = 0.205) [30]. Comparable results were observed in a study of 123 women aged 18–50 years in India, where the correlation coefficients for DBP and SBP with BMI were 0.35 and 0.30, respectively [31]. Conversely, other studies have reported different patterns. For instance, research conducted in Vitória, Espírito Santo, found that SBP was more strongly associated with BMI than DBP [32]. Similarly, a cross-sectional study in Aracaju, Sergipe, observed a stronger correlation between BMI and SBP compared to DBP [33].
A possible explanation for the greater elevation of DBP compared with SBP in relation to BMI may lie in the hypothesis that specific workplace characteristics influence peripheral vascular resistance, leading to more pronounced changes in DBP [34,35,36]. Psychological stress in the occupational setting can trigger hyperactivation of the sympathetic nervous system, increasing vascular tone and resistance through heightened catecholamine secretion, which directly impacts DBP [34]. Moreover, the mechanisms linking SAH to increased body mass share similarities with those associated with obesity mediated by occupational stress, thereby synergistically contributing to the development of SAH [37,38]. In addition, higher BMI, reflecting greater adipose tissue accumulation, may induce endothelial dysfunction, cardiac structural alterations, and arterial stiffness. These changes increase vascular resistance without proportionally affecting cardiac output, which could explain why DBP is more substantially influenced by BMI than SBP [39,40]. Nevertheless, further research—particularly in populations of female workers—is warranted to confirm this hypothesis and clarify the mechanisms underlying the differential effects of BMI on SBP and DBP.
SAH arises from the interaction of multiple determinants, including socioeconomic factors (age and income) [41,42], behavioral factors (dietary patterns) [43], psychological factors (occupational stress) [44], and biological factors (obesity) [45]. Socioeconomic disadvantage can heighten psychosocial stress responses, as lower income may increase vulnerability to occupational stress [42], particularly among women who, in addition to work responsibilities, often assume primary responsibility for household financial management [46]. Advancing age may further diminish the individual’s capacity to cope with and adapt to challenging or stressful work environments [41]. Dietary patterns are likewise influenced by socioeconomic and psychosocial contexts. Limited financial resources may encourage the consumption of low-cost, ultra-processed foods high in sugar and fat, increasing cardiometabolic risk [43]. In contrast, adequate income may facilitate access to foods of higher nutritional quality [43]. Additionally, occupational stress may promote the consumption of highly palatable, energy-dense foods as a coping mechanism, driven by hyperactivation of the hypothalamic–pituitary–adrenal axis and subsequent cortisol elevation [44]. Collectively, these socioeconomic, psychosocial, and behavioral pathways converge to promote weight gain, increases in BMI, and the development of obesity [45,47], a condition that constitutes a major biological risk factor for the onset of SAH [45].
This study has several notable strengths. First, it employed previously tested and validated instruments to assess SAH and other covariates, thereby ensuring methodological rigor. Additionally, interviewers underwent systematic selection and training, which enhanced the consistency and reliability of data collection. Another important strength lies in the use of a robust conceptual framework for multivariable analysis, allowing for appropriate adjustment of the results for potential confounding factors. Despite these advantages, certain limitations must be acknowledged when interpreting the findings. As this is a cross-sectional study, its findings do not allow for causal inferences between SAH and the associated risk factors. Nonetheless, because the study is part of the broader ELO-SAÚDE longitudinal project, future phases of data collection may provide opportunities to examine changes in blood pressure and the development of SAH over time, which could help clarify temporal patterns among these associations. This study was conducted in a single company in southern Brazil and included only female workers, which limits the external validity of the findings to other populations and geographic contexts. Therefore, future research involving multiple companies and/or occupational sectors would be valuable to enhance the generalizability of the results. Moreover, all participants were employed in fixed work shifts, which restricts comparisons with workers in rotating or intermittent schedules. Caution is also required when contrasting these findings with studies that include predominantly male populations, as sex-related differences in the prevalence of SAH are well documented. Another limitation is the lack of information on potential confounders, such as dietary sodium intake, general (non-occupational) stress, and the use of oral contraceptives. Including and analyzing these variables in future investigations would enhance the comprehensiveness of the findings and contribute to a more robust understanding of the observed associations. Finally, as with all occupational health studies, the results should be interpreted in light of the potential “healthy worker effect.” For example, only 7.5% of participants in this study reported smoking, a proportion substantially lower than that observed in the general population. This suggests that the study population may represent a healthier subgroup of workers, which could lead to an underestimation of the prevalence of SAH and its associated risk factors, as individuals with poorer health are less likely to remain employed. Nevertheless, even when considering this potential limitation, it is noteworthy that the prevalence estimates reported here are consistent with previously published regional and national population-based data [9,22].
The findings of this study have practical implications for workplace health promotion and surveillance. Given that SAH is prevalent among these female workers, workplace-based strategies could include implementing routine blood pressure screening programs, promoting regular physical activity and healthy eating initiatives, and developing stress-management and mental health support activities. Such measures may be particularly relevant within the company and occupational context in which these women are employed, where organizational support can play a central role in improving cardiovascular health outcomes. From a broader public health perspective, our results highlight the need for policies that integrate cardiovascular risk monitoring into occupational health services, particularly for female worker populations. Future research should further investigate potential causal pathways, assess the effectiveness of tailored workplace interventions, and explore how structural and psychosocial factors within occupational environments shape cardiovascular risk among women.
5. Conclusions
The present study identified that SAH is prevalent among female workers in a company located in southern Brazil, particularly among older women and those with obesity. Given the substantial burden of SAH among women with obesity, these findings underscore the need for heightened attention to this association within the broader context of women’s occupational health. The factors identified may help define priority groups for workplace-based SAH prevention strategies, particularly targeting female industrial workers with comorbidities, those in lower-income positions, and older individuals. Collectively, these results reinforce the recognition of SAH as a major public health challenge in Brazil, extending beyond the general population to include occupational settings. Moreover, they highlight the critical interplay of socioeconomic disadvantage, aging, and obesity in shaping women’s vulnerability to SAH, suggesting that workplace interventions to reduce cardiovascular risk should prioritize these high-risk subgroups.
Author Contributions
Y.G.M., I.S.K., J.C.d.S., H.C.A., A.G. and M.T.A.O. designed the study and contributed to analysis, data interpretation, and preparation and writing of the manuscript. H.C.A., I.S.K. and J.C.d.S. designed the study, supervised the field work and data collection, and contributed to preparation of manuscript. Y.G.M., H.C.A., A.G. and M.T.A.O. drafted the paper and conducted all analyses. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Council of Technological and Scientific Development (CNPq, grant n. 406161/2021-6). The funders had no role in the study design, data collection, analysis, decision to publish, or the preparation and approval of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Committee of University do Vale do Rio dos Sinos (CAAE no. 53762521.7.0000.5344/Approval no. 5681627 in 7 March 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
M.T.O. received research productivity grants from the Brazilian Council for Scientific and Technological Development—CNPq (process numbers 307175/2017-0 and 303977/2022-1). A.G. received a post-doctoral fellowship from CNPq (process n. 102282/2024-2).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| SAH | Systemic Arterial Hypertension |
| BP | Blood Pressure |
| PR | Prevalence Ratio |
| CI | Confidence Interval |
| BMI | Body Mass Index |
| OR | Odds Ratio |
| SBP | Systolic Blood Pressure |
| DBP | Diastolic Blood Pressure |
References
- Malachias, M.V. 7th Brazilian guideline of arterial hypertension: Presentation. Arq. Bras. Cardiol. 2016, 107 (Suppl. S3), XV–XIX. [Google Scholar] [CrossRef]
- Jardim, P.C.B.V. The Brazilian Society of Cardiology and Hypertension: It’s Time for Action. Arq. Bras. Cardiol. 2018, 111, 343–344. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in blood pressure from 1975 to 2015: A pooled analysis of 1479 population-based measurement studies with 19.1 million participants. Lancet 2017, 389, 37–55. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Ostchega, Y.; Fryar, C.D.; Nwankwo, T.; Nguyen, D.T. Hypertension Prevalence Among Adults Aged 18 and Over: United States, 2017–2018; NCHS Data Brief; National Center for Health Statistics: Hyattsville, MD, USA, 2020; pp. 1–8.
- Andrade, S.S.d.A.; Stopa, S.R.; Brito, A.S.; Chueri, P.S.; Szwarcwald, C.L.; Malta, D.C. Self-reported hypertension prevalence in the Brazilian population: Analysis of the National Health Survey, 2013. Epidemiol. Serv. Saúde 2015, 24, 297–304. [Google Scholar] [CrossRef]
- Barroso, W.K.S.; Rodrigues, C.I.S.; Bortolotto, L.A.; Mota-Gomes, M.A.; Brandao, A.A.; Feitosa, A.D.M.; Machado, C.A.; Poli-de-Figueiredo, C.E.; Amodeo, C.; Mion Junior, D.; et al. Brazilian Guidelines of Hypertension—2020. Arq. Bras. Cardiol. 2021, 116, 516–658. [Google Scholar] [CrossRef] [PubMed]
- Malta, D.C.; Goncalves, R.P.F.; Machado, I.E.; Freitas, M.I.F.; Azeredo, C.; Szwarcwald, C.L. Prevalence of arterial hypertension according to different diagnostic criteria, National Health Survey. Rev. Bras. Epidemiol. 2018, 21, e180021. [Google Scholar] [CrossRef]
- Caldeira, T.C.M.; Sereno, A.C.R.A.; Soares, M.M.; Maia, E.G.; Claro, R.M. Trend in hypertension prevalence and health behaviors among the brazilian adult population: 2006–2019. Obesities 2023, 3, 145–154. [Google Scholar] [CrossRef]
- Xavier, P.B.; Garcez, A.; Cibeira, G.H.; Germano, A.; Olinto, M.T.A. Factors associated with the occurrence of arterial hypertension in industry workers of state of Rio Grande do Sul, Brazil. Arq. Bras. Cardiol. 2021, 117, 484–491. [Google Scholar] [CrossRef]
- Ribeiro Junior, U.E.S.; Fernandes, R.C.P. Hypertension in Workers: The Role of Physical Activity and its Different Dimensions. Arq. Bras. Cardiol. 2020, 114, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Spekalski, M.V.S.; Bobato, G.R.; Cabral, L.P.A.; Fadel, C.B.; Krum, E.A.; Bordin, D. Prevalence and factors associated to arterial hypertension in workers at a higher education institution. Rev. Saude Publica Do Paraná 2022, 5, 1–13. [Google Scholar] [CrossRef]
- Pereira, S.G.S.; Silva Junior, R.F.D.; Ribeiro, C.; Barbosa, H.A.; Torres, J.; Silva, C. Factors associated with prehypertension and hypertension among healthcare workers working in high-complexity services. Cien. Saude Colet. 2021, 26, 6059–6068. [Google Scholar] [CrossRef]
- Vasconcelos, F.N.d.; Canuto, R.; Guilherme, R.C.; Clark, S.G.F.; Lira, P.I.C.d. Worker’s systemic arterial hypertension. Braz. J. Dev. 2020, 6, 70695–70708. [Google Scholar] [CrossRef]
- Ivicevic Uhernik, A.; Kralj, V.; Cukelj, P.; Brkic-Bilos, I.; Erceg, M.; Benjak, T.; Stevanovic, R. Undiagnosed hypertension in Croatia. Croat. Med. J. 2023, 64, 4–12. [Google Scholar] [CrossRef] [PubMed]
- de Araújo Couto, H.; Vieira, F.L.H.; Lima, E.G. Work stress and arterial hypertension. Rev. Bras. Hipertens. 2007, 14, 112–115. [Google Scholar]
- Vital, T.; Silva, I.d.O.; Paz, F.d.N. Arterial hypertension and work-related risk factors: A literature review. Res. Soc. Dev. 2020, 9, e905975085. [Google Scholar] [CrossRef]
- Cunha, C.L.P. Obesity-Induced Hypertension. Arq. Bras. Cardiol. 2023, 120, e20230391. [Google Scholar] [CrossRef]
- Alves, M.G.; Chor, D.; Faerstein, E.; Lopes Cde, S.; Werneck, G.L. Short version of the “job stress scale”: A Portuguese-language adaptation. Rev. Saude Publica 2004, 38, 164–171. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Health Organization. In Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; WHO Library Cataloguing-in-Publication Data: Geneva, Switzerland, 2000; Available online: https://iris.who.int/handle/10665/42330 (accessed on 28 August 2024).
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M.T. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef]
- BRAZIL. Ministry of Health. [Vigitel Brazil 2006–2023: Self-Reported Morbidity and Self-Assessment of Health Status: Surveillance of Risk and Protective Factors for Chronic Diseases by Telephone Survey: Estimates of Frequency and Sociodemographic Distribution of Self-Reported Morbidity and Health Self-Assessment in the Capitals of the 26 Brazilian States and the Federal District Between 2006 and 2023]; 2023. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/vigitel_2006_2023_morbidade_autoavaliacao.pdf (accessed on 20 February 2025).
- Malta, D.C.; Bernal, R.T.I.; Andrade, S.; Silva, M.; Velasquez-Melendez, G. Prevalence of and factors associated with self-reported high blood pressure in Brazilian adults. Rev. Saude Publica 2017, 51, 11s. [Google Scholar] [CrossRef]
- Vinholes, D.B.; Bassanesi, S.L.; Chaves Junior, H.C.; Machado, C.A.; Melo, I.M.F.; Fuchs, F.D.; Fuchs, S.C. Association of workplace and population characteristics with prevalence of hypertension among Brazilian industry workers: A multilevel analysis. BMJ Open 2017, 7, e015755. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, A.M.; Assunção, A.Á. Job strain and arterial hypertension in nursing professionals from the municipal healthcare network in Belo Horizonte, Minas Gerais, Brazil. Rev. Bras. Saúde Ocup. 2016, 41, e6. [Google Scholar] [CrossRef][Green Version]
- Urbanetto Jde, S.; Prado Lima Figueiredo, A.E.; da Silva Gustavo, A.; Bosi de Souza Magnago, T.S.; Pinheiro da Costa, B.E.; Poli-de-Figueiredo, C.E. Arterial hypertension in nursing personnel of an emergency hospital. Int. J. Nurs. Pract. 2015, 21, 433–442. [Google Scholar] [CrossRef]
- Sarno, F.; Bandoni, D.H.; Jaime, P.C. Overweight and hypertension in workers from companies benefited by the Worker Food Program (WFP). Rev. Bras. Epidemiol. 2008, 11, 453–462. [Google Scholar] [CrossRef]
- Moreira, O.C.; Oliveira, R.A.R.d.; Andrade Neto, F.; Amorim, W.; Oliveira, C.E.P.; Doimo, L.A.; Amorim, P.R.d.S.; Laterza, M.C.; Monteiro, W.D.; Marins, J.C.B. Association between cardiovascular risk and hypertension in universities professors. Rev. Bras. Educ. Fís. Esporte 2011, 25, 397–406. [Google Scholar] [CrossRef]
- Rezende, T.C.G.D.; Christovam, É.R.; de Paula, M.N.; dos Santos Silva, I.T. Obesity-induced hypertension: A literature review. J. Arch. Health 2024, 5, e1788. [Google Scholar] [CrossRef]
- da Silva, N.T.; Giacon, T.R.; da Costa, M.P.; Vitor, A.L.R.; Vanderlei, L.C.M. Prevalence and correlation between obesity, arterial hypertension, and physical activity practice. Colloq. Vitae 2011, 3, 32–36. [Google Scholar] [CrossRef]
- Dua, S.; Bhuker, M.; Sharma, P.; Dhall, M.; Kapoor, S. Body mass index relates to blood pressure among adults. N. Am. J. Med. Sci. 2014, 6, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Pires, R.C.; do Amaral Gomes, P.H.; Correa, M.M.; Pires, L.C.; da Silva, J.B.L. Association of anthropometric indices with arterial hypertension in adults participating in educational events. Braz. J. Health Rev. 2020, 3, 15253–15259. [Google Scholar] [CrossRef]
- Lima, J.d.S.; Bezerra, L.A.; Gomes, R.M.O.P.; Fontes, A.A.B.; Noronha, V.F.C.M.; de Jesus, J.B.; Lima, S.O.; Cruz, J.F. Correlation between anthropometric indicators of obesity and blood pressure levels. Braz. J. Health Rev. 2021, 4, 14725–14735. [Google Scholar] [CrossRef]
- Chen, Y.; Juvinao-Quintero, D.; Velez, J.C.; Munoz, S.; Castillo, J.; Gelaye, B. Personal and work-related burnout is associated with elevated diastolic blood pressure and diastolic hypertension among working adults in chile. Int. J. Environ. Res. Public Health 2023, 20, 1899. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, R.; Lima Filho, E.C.; Fischer, F.M.; Moreira Filho, D.C. Diastolic blood pressure associated with accumulated work time among drivers and collectors. Rev. Saude Publica 1993, 27, 363–372. [Google Scholar] [CrossRef]
- Schnall, P.L.; Pieper, C.; Schwartz, J.E.; Karasek, R.A.; Schlussel, Y.; Devereux, R.B.; Ganau, A.; Alderman, M.; Warren, K.; Pickering, T.G. The relationship between’job strain,’workplace diastolic blood pressure, and left ventricular mass index: Results of a case-control study. JAMA 1990, 263, 1929–1935. [Google Scholar] [CrossRef]
- Solovieva, S.; Lallukka, T.; Virtanen, M.; Viikari-Juntura, E. Psychosocial factors at work, long work hours, and obesity: A systematic review. Scand. J. Work Environ. Health 2013, 39, 241–258. [Google Scholar] [CrossRef]
- Shariq, O.A.; McKenzie, T.J. Obesity-related hypertension: A review of pathophysiology, management, and the role of metabolic surgery. Gland Surg. 2020, 9, 80–93. [Google Scholar] [CrossRef]
- Grassi, G.; Seravalle, G.; Dell’oro, R. Sympathetic activation in obesity: A noninnocent bystander. Hypertension 2010, 56, 338–340. [Google Scholar] [CrossRef]
- Lobato, N.S.; Filgueira, F.P.; Akamine, E.H.; Tostes, R.C.; Carvalho, M.H.; Fortes, Z.B. Mechanisms of endothelial dysfunction in obesity-associated hypertension. Braz. J. Med. Biol. Res. 2012, 45, 392–400. [Google Scholar] [CrossRef]
- Grosch, J.W.; Caruso, C.C.; Rosa, R.R.; Sauter, S.L. Long hours of work in the U.S.: Associations with demographic and organizational characteristics, psychosocial working conditions, and health. Am. J. Ind. Med. 2006, 49, 943–952. [Google Scholar] [CrossRef]
- Sun, W.; Wu, H.; Wang, L. Occupational stress and its related factors among university teachers in China. J. Occup. Health 2011, 53, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Lenz, A.; Olinto, M.T.; Dias-da-Costa, J.S.; Alves, A.L.; Balbinotti, M.; Pattussi, M.P.; Bassani, D.G. Socioeconomic, demographic and lifestyle factors associated with dietary patterns of women living in Southern Brazil. Cad. Saude Publica 2009, 25, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Canuto, R.; Garcez, A.; Spritzer, P.M.; Olinto, M.T.A. Associations of perceived stress and salivary cortisol with the snack and fast-food dietary pattern in women shift workers. Stress 2021, 24, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.K.; Mohammed, R.A. Obesity: Prevalence, causes, consequences, management, preventive strategies and future research directions. Metabol. Open 2025, 27, 100375. [Google Scholar] [CrossRef] [PubMed]
- Canazaro, B.C.; Aguiar, O.B.; Moreno, A.B.; Alves, M.G.M.; Fonseca, M. Association between job stress and quality of life in nutritionists working in public hospitals in Rio de Janeiro, Brazil. Cien. Saude Colet. 2022, 27, 1951–1963. [Google Scholar] [CrossRef] [PubMed]
- Backes, V.; Bairros, F.; Cafruni, C.B.; Cummins, S.; Shareck, M.; Mason, K.; Dias-da-Costa, J.S.; Olinto, M.T.A. Food environment, income and obesity: A multilevel analysis of a reality of women in Southern Brazil. Cad. Saude Publica 2019, 35, e00144618. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).