Abstract
Introduction: Over the past 40 years, there has been a significant increase in the global prevalence of childhood obesity, which is associated with an increased risk of heart problems and the earlier onset of heart diseases. Objective: The aim of this research is to assess the prevalence of obesity and its risk factors in children and adolescents among students from the second and third cycle and secondary education of a school grouping in the interior of Portugal. Materials and Methods: The sample was collected from a school grouping in Alcains, among attending students from the fifth to the twelfth grade. The sample consisted of a total of 156 students aged between 10 and 18 years. A questionnaire was proposed, and blood pressure measurement and lipid profile evaluation were performed for each individual. The collection and statistical treatment of data for this study required a submission and authorization request to the Ethics Committee of the Polytechnic Institute of Castelo Branco, followed by authorization from the school group’s administration. Results: The percentage of elevated BMI was 30.8%, and was higher in males. A higher prevalence of hypertension (37.8%), elevated triglyceride levels in students who did not exercise outside of school, and in individuals who consumed larger amounts of meat, who also showed a higher prevalence of lower-than-expected high-density lipoprotein (HDL) cholesterol levels, were observed. Discussion: A high percentage of elevated BMI, high blood pressure levels, and changes in lipid profile were observed among high school students in this school in the interior of Portugal, as has been observed in other studies. Conclusions: It is essential to conduct more studies, screenings, and investigations that can identify these cases early, in order to mitigate risk factors.
1. Introduction
Over the past three decades, the global prevalence of obesity has surged, becoming a major health concern worldwide, with a particularly rapid increase in cases of morbid obesity [1,2]. Excess body weight is associated with a heightened risk of heart problems and an earlier onset of cardiovascular diseases. Notably, there has been a substantial rise in childhood obesity across the world over the last 40 years. In Portugal, there has been a constant change in the prevalence of overweight and childhood obesity, which is tending to increase [3].
Obesity is a complex, chronic disease characterized by excessive fat accumulation that can impair health. The diagnosis of overweight and obesity is determined by measuring an individual’s weight and height to calculate the body mass index (BMI): weight (kg)/height2 (m2). Obesity and excess weight primarily result from an imbalance between food intake and energy expenditure, a discrepancy influenced by genetic, metabolic, environmental, behavioral, social, and cultural factors [4,5,6].
Weight issues often begin in childhood and can worsen into adulthood, potentially leading to conditions such as type 2 diabetes and heart disease. A lack of physical activity also elevates the risk of developing chronic diseases. Primary and primordial prevention is crucial to reduce the prevalence of obesity in the long term, with controlling obesity currently being the main challenge [5]. Therefore, promoting the maintenance of a healthy body weight throughout life is essential to prevent adverse consequences. Encouraging healthy lifestyles should start with a balanced diet and regular physical activity as early as possible to maintain weight and adiposity within desirable limits. Upon diagnosing obesity, a comprehensive lifestyle change should be initiated, encompassing dietary adjustments and increased physical activity [7,8,9].
Understanding the risk factors associated with adolescent obesity is particularly important. Adolescence is a critical developmental period where habits and behaviors are formed that often carry into adulthood. Identifying and addressing these factors early can help mitigate the risk of chronic diseases later in life. Research in this area can provide valuable insights into effective prevention strategies and inform public health policies aimed at reducing obesity rates [10].
Moreover, the increasing prevalence of obesity places a significant burden on healthcare systems and economies due to the associated healthcare costs and productivity losses. Studies on the risk factors for obesity among adolescents can help identify high-risk groups and develop targeted interventions, thereby improving health outcomes and reducing the economic impact of obesity [11,12,13].
Research into the risk factors for adolescent obesity is essential for developing effective prevention and intervention strategies. By understanding and addressing these factors, we can promote healthier lifestyles, reduce the incidence of obesity-related diseases, and alleviate the long-term economic burden on society [14,15].
2. Materials and Methods
This research is part of a project entitled Teen Without Risk (TWR), a school-based intervention project that focuses on the health and well-being of children and adolescents, promoting health education within the school community in schools in the Beira Baixa and Beira Alta regions. The scientific supervisor, Professor Dr. Patrícia Coelho, is the research coordinator of the project.
For the implementation of the study protocol and data collection, it was essential to obtain informed consent from the parents or guardians. The questionnaire requested information about the level of education, physical exercise habits, dietary habits, and the presence of a family history of cerebrocardiovascular disease among immediate family members. The variables obtained through the questionnaire, the blood pressure assessment, and the anthropometric data of each individual were coded using the Statistical Package for the Social Sciences (SPSS) program. After data collection and variable coding, a quantitative and qualitative descriptive analysis was conducted to test the hypotheses among the variables under study. The normality distribution of the sample was tested using the Kolmogorov–Smirnov test, confirming that non-parametric tests should be used.
Study Protocol and Data Collection
A meeting was held to present the study and clarify the informed consent, which was signed by the parents or guardians, or by the student themselves if they were of legal age. The questionnaire filled out by each student requested information about their level of education, physical exercise habits, smoking habits, alcohol consumption, dietary habits, and the presence of a family history of heart disease among immediate family members. The application of the questionnaire by the research team had been previously validated in a similar population.
On the day of the assessment, information regarding age, weight, and height was collected, and the body mass index (BMI) was calculated using the formula of dividing the weight by the square of the height. The BMI of the individuals was classified according to percentile tables for sex and age. According to the Directorate General of Health, an individual is considered obese if their BMI is above the 95th percentile (P95); overweight if their BMI is between the 85th and 95th percentiles (P85–P95); has an adequate weight if their BMI is below the 85th percentile (P85) and above the 5th percentile (P5); and has a lower-than-expected BMI if it is below the 5th percentile (P5) (Directorate General of Health).
For the blood pressure assessment, it was mandatory for the minor to have a rest period of at least five minutes and to adopt the correct position (sitting with their back supported, legs uncrossed, feet flat on the floor, and the chosen arm for the assessment relaxed and supported on a table with the palm facing up at heart level). The cuff size used was always adjusted to the circumference of each child’s arm. Before proceeding to inflation, the cuff had to be centered on the brachial artery. Systolic blood pressure (SBP) and diastolic blood pressure (DBP), measured in millimeters of mercury (mmHg), were assessed using an automatic method with the help of an automatic sphygmomanometer. An Omron blood pressure monitor was used. According to the Guidelines of the European Society of Hypertension, after the assessment, the blood pressure classification was made according to percentiles for age, sex, and height (Table 1).

Table 1.
Classification of hypertension in children and adolescents.
For the assessment of the lipid profile in children and adolescents, an appropriate device that operates by collecting capillary blood was used—Lux: Professional Monitoring of Lipids, Glucose and Hemoglobin. Following the collection of values for total cholesterol, HDL cholesterol, LDL cholesterol, and triglycerides, they were classified according to the reference values from the NCEP Expert Panel on Cholesterol Levels in Children [16] (Table 2 and Table 3).
Table 2.
Reference value classification for lipids and lipoproteins in children and adolescents—Directorate General of Health [17].
Table 3.
Reference values for blood glucose according to the Directorate General of Health.
3. Results
The sample for this study consists of 156 individuals spanning various educational stages, from the fifth grade (2° cycle) to secondary education (12° cycle) (Table 4).
Table 4.
Distribution of students by grade level attended.
The individuals who participated in this study range in age from 10 to 18 years old, with the age group of 13 to 14 years being the most frequent in this sample (Figure 1).
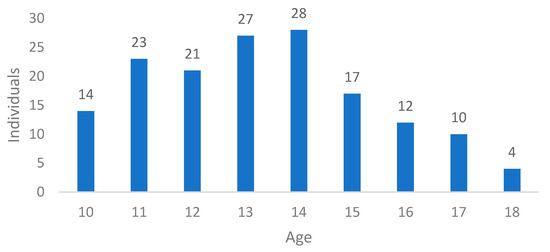
Figure 1.
Distribution of ages of individuals.
In this sample, 82 (47%) individuals were male and 74 (53%) were female (Figure 2).
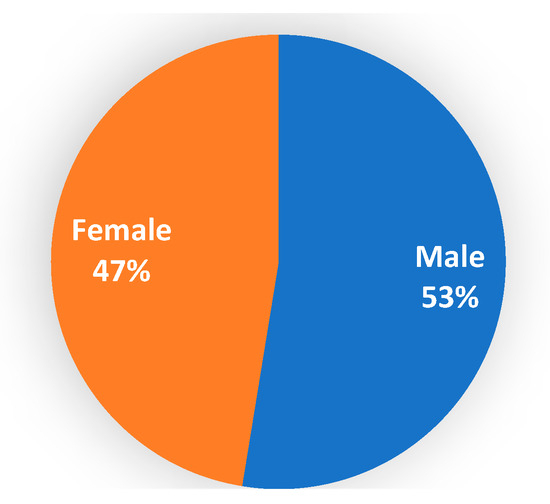
Figure 2.
Distribution of gender among individuals.
The average weight of this population is 55.09 kilograms (kg), with a minimum of 28 kg and a maximum of 108 kg, and a standard error of 13.959. Regarding height, the average was 1.60 meters (m), ranging from 1.32 m to 1.82 m, with a standard error of 10.868.
In terms of body mass index (BMI), it was found that 27 students (17.3%) were overweight, predominantly males. Ten boys and eleven girls were classified as obese (13.5%), while one student (0.6%) had a BMI below the expected range. The remaining students (68.6%) had a BMI within the normal range (Figure 3).
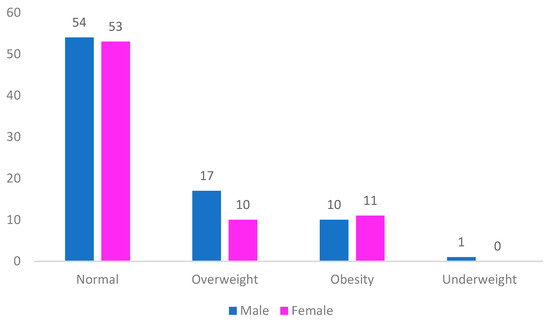
Figure 3.
Distribution of BMI among individuals by gender.
In the analysis of the group of individuals who are overweight and obese, 7.7% (n = 12) and 9% (n = 14), respectively, almost all eat meat. Among those who almost always eat meat in their meals, 10.3% (n = 16) have high blood pressure, 7.7% (n = 12) are overweight, and 6.4% (n = 10) are obese.
Regarding the frequency of physical exercise among individuals, 69 students (44.2%) reported only exercising during physical education classes at school, while the remaining 55.8% of individuals engage in physical exercise both at school and outside school. Among those who exercise beyond physical education classes, 19 students (12.2%) exercise once a week, 36 students (23.1%) exercise twice a week, 18 students (11.5%) exercise three times a week, and 14 students (9%) exercise daily (Figure 4).
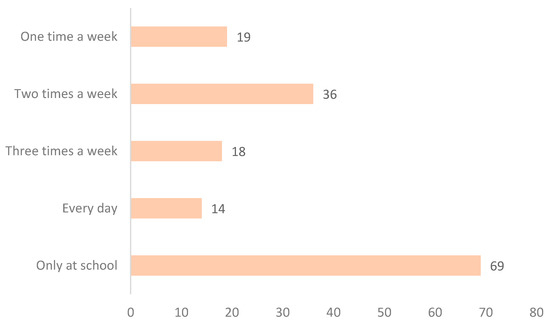
Figure 4.
Distribution of frequency of physical exercise practice.
Regarding the study of hereditary factors, 48.7% (n = 76) of students report having direct family members with diabetes, and 36.5% (n = 57) report having direct family members with hypertension (HTA).
It was found that 31.4% have more than one type of cerebrocardiovascular disease in direct ancestors, with 24.4% of students (n = 38) having direct family members who have suffered a stroke (AVC), 6.4% (n = 10) having direct family members who have suffered a myocardial infarction (EAM), and 0.6% (n = 1) having a direct family member who has suffered both a stroke and a myocardial infarction.
Males show a higher prevalence of family history with one or more cerebrocardiovascular disease. Using the Chi-square test, it was observed that there is no statistically significant relationship between family history and gender (p = 0.060).
Total Cholesterol Assessment: According to the lipid profile evaluation, it was concluded that 95.5% (n = 149) of students had acceptable levels of total cholesterol, 3.9% (n = 6) had borderline–high levels, and 0.6% (n = 1) had high levels of total cholesterol. Females (3.2%) showed a higher percentage of altered cholesterol levels compared to males (1.3%), with the majority being female. Among students with borderline–high total cholesterol, 1.3% were obese, while the remaining percentage had a normal or below-normal BMI.
High-Density Lipoprotein (HDL) Assessment: It was observed that 28.2% (n = 44) of students had acceptable levels of HDL cholesterol, 9.6% (n = 15) had borderline–high levels, and 62.2% (n = 97) had reduced levels of HDL cholesterol. Specifically, 40.4% (n = 63) were males and 31.4% (n = 49) were females. A Chi-square test showed a marginally significant relationship between HDL cholesterol and gender (p = 0.055). Among students who were overweight and obese, 14.1% and 9%, respectively, had reduced HDL values. In terms of dietary habits, students who consumed higher amounts of meat tended to have lower HDL levels, and among those with low HDL levels, 62.3% (n = 43) only engaged in physical exercise during physical education classes.
Low-Density Lipoprotein (LDL) Assessment: When evaluating LDL cholesterol levels, 92.3% (n = 144) of students had acceptable levels, 6.4% (n = 10) had borderline–high levels, and 1.3% (n = 2) had high levels of LDL cholesterol. Individuals who were overweight and obese had LDL values within the normal range.
3.1. Triglyceride Assessment
According to the lipid profile evaluation, it was found that 66% of students (n = 103) had acceptable triglyceride levels, 27.6% (n = 43) had borderline–high levels, and 6.4% (n = 10) had high triglyceride levels. Females showed a higher percentage of borderline–high and high triglyceride levels compared to males. However, this relationship was not statistically significant (p = 0.551).
Increased triglyceride levels were associated with obesity, and were present in 1.9% of students who were overweight or obese.
3.2. Blood Pressure Evaluation
Based on the assessment of blood pressure values and analysis using appropriate percentiles for sex, age, and height, it was found that 37.8% (n = 59) of students had blood pressure values above normal, while 62.2% (n = 97) had a normal blood pressure. Among those with elevated blood pressure values, 17.3% (n = 27) had hypertension (HTN), 11.5% (n = 18) had HTN stage 1, and 9% (n = 14) had HTN stage 2 (Figure 5).
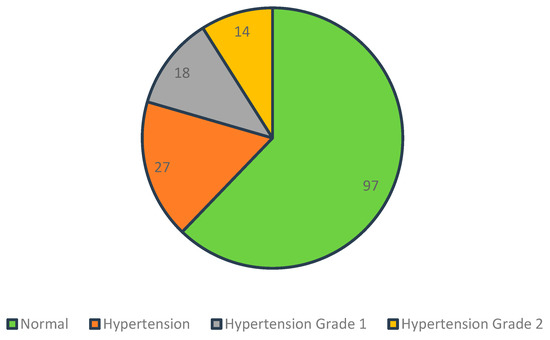
Figure 5.
Blood pressure classification.
Male individuals show a higher prevalence of high blood pressure (10.9% vs. 6.4%) and stage 2 hypertension (5.8% vs. 3.2%). However, stage 1 hypertension is more prevalent in females (3.8% vs. 7.7%).
In the group of students with stage 1 hypertension and stage 2 hypertension, 7.7% (n = 12) and 3.8% (n = 6), respectively, do not engage in physical exercise outside of school. Among students with stage 1 hypertension, 7.7% (n = 12) almost always eat meat, as do 6.4% (n = 10) of students with stage 2 hypertension.
Of the individuals who are overweight, 1.9% have hypertension, 2.6% with stage 1 hypertension.
In the analysis of the group of individuals who are overweight, 3.2% rarely eat vegetables in their meals, while 1.9% of individuals who rarely eat vegetables in their meals are obese.
4. Discussion
The study of cerebrocardiovascular pathology and its risk factors in society is of enormous importance, considering the high rates of morbidity and mortality associated with these conditions. Healthy habits should be implemented early in children and young people to reduce the prevalence of these pathologies in the future of modern societies [1,7,8]. The sample for this study consists of 156 individuals from different educational levels between the second cycle and secondary education, with 53% of participants being male and 47% being female.
In the analysis of this study, it was observed that the percentage of individuals with overweight was 17.3%, which is lower than what was found in two studies conducted in Portugal by Ribeiro et al. (28.3%) and Cabral et al. (18%) [18,19]. Conversely, the percentage of obese youths (13.5%) in this study was higher than the studies by Ribeiro et al. [18] and Cabral et al. Thus, in the study by Cabral et al. [19], the percentage of individuals with a normal BMI was higher (74.9%) than what was found in this study (68.6%). On the other hand, other studies observed different values [20,21]. These discrepancies can be attributed to different dietary patterns and lifestyles between Chinese and Portuguese societies.
Zhang et al. found that the highest percentage of overweight students was observed in males, which was also seen in the studied sample [22]. Conversely, Muhihi et al. [23], in studying high BMI, found it was more prevalent in females, as did Mohan et al. [24], differing from the data observed in the group of overweight students in the present study. Regarding the relationship between hypertension (HTA) and BMI, Ribeiro et al. [18] and Rodrigues et al. [25] found a statistically significant relationship between BMI and HTA, contrary to what was observed (p = 0.657), as well as in the study by Cabral et al. [19].
In this study, the highest percentages of hypertensive students were in the group with normal BMI, which was also seen in the study by Cabral et al. [19]. Conversely, Zhang et al. [22] and Figueirinha et al. [26] found that elevated systolic and diastolic blood pressure were more present in the group of obese students. According to Marrodán et al. [27], it was found that the majority of students had normal blood pressure levels, which was observed in this study (60.1%), with 38.8% of individuals having elevated blood pressure values, contrary to what was observed in the study by Cabral et al. [19].
Indeed, these high rates of overweight at these ages may be related to eating habits, which are extremely important for general health, influencing body weight, cerebrocardiovascular health, and emotional well-being. Several factors can harm eating habits, such as the availability and easy access to highly processed foods, lack of nutritional education, and sociocultural issues.
In this study, lipid profile alterations were found, with reduced HDL and altered triglyceride values observed in the studies by Reuter et al. [28], Cabral et al. [19], and Cunha et al. [29], which present lower percentages of reduced HDL levels compared to the study in question. In the study by Manios et al. [30], 1.8% of individuals had higher than expected triglyceride levels and 8.4% had reduced HDL levels, contrary to the alarming percentages of 62.2% and 34%, respectively, observed in this school. Supporting these results, Gabriella et al. [31] found a percentage of 52.7% of individuals with reduced HDL levels. The study by Cabral et al. found a higher percentage of altered triglyceride levels than this study [19].
In Portugal, there is still a significant consumption of red meats, cured cheeses, and sausages, promoting the increase in fatty acids and lipids, leading to arterial wall stiffness and poor cardiac function. According to Cunha [32] and Cabral et al. [19], females showed a higher prevalence of elevated total cholesterol (TC) and triglyceride levels than males, as observed in these students. According to Mach et al. [33], high concentrations of LDL in the blood vessels can lead to the adherence of these lipoproteins to the intima of the arteries, leading to the formation of atheroma plaques, which subsequently cause atherosclerosis. In this study, it was observed that individuals with HTA (5.7%) had altered LDL values, showing a statistically significant relationship between assessed blood pressure and LDL cholesterol (p = 0.0001), disagreeing with the study by Cabral et al., which did not find this relationship [19].
Addressing health literacy in children and adolescents is fundamental for developing healthier lifestyle changes, promoting health growth throughout life. Regarding the presence of known heart disease, 1.9% of individuals in this study had it, disagreeing with the results obtained by Ribeiro et al., 2019 [20], who did not find individuals with this pathology. In the case of type 2 diabetes mellitus, no individuals with this pathology were found in this study, agreeing with the results of Ribeiro et al., 2019 [20]. Conversely, the study by Cabral et al., 2022 [19] found individuals with this pathology.
The group of students with a family history of cerebrocardiovascular disease and diabetes constitutes 67.9%, which is much higher than the prevalence of students with a family history of heart disease in studies conducted by Ribeiro et al., 2019 [20] (40.9%), Okpokowuruk et al. [34] and Kurnianto et al. [35]. Based on the observed results, the importance of considering family history to assess the individual risk of developing cerebrocardiovascular pathologies is highlighted, reinforcing the need for preventive interventions and management strategies tailored to these factors.
Figueirinha et al. [26] found that the majority of participants had a family history of HTA, observing a statistical significance in the relationship between family history and blood pressure, contrary to what was observed in the study conducted in this school grouping in the interior of Portugal (p = 0.068). This discrepancy can be attributed to the lack of sample representativeness in relation to the population, as the sample in the study by Figueirinha et al. was a convenience sample [26]. It is essential to conduct more studies, screenings, and investigations that can identify these cases early, as well as the factors that potentiate obesity to mitigate risks. Therefore, primary health care in schools about the risk factors for these pathologies is crucial, especially in the follow-up of children at potential risk.
5. Conclusions
In conclusion, addressing the risk factors for adolescent obesity is crucial for mitigating the growing global health crisis associated with obesity. This study has highlighted the multifaceted nature of obesity, influenced by genetic, metabolic, environmental, behavioral, social, and cultural factors. By identifying these risk factors early, especially during the critical developmental period of adolescence, we can implement effective prevention and intervention strategies that can significantly reduce the prevalence of obesity and its associated health complications, such as type 2 diabetes and cardiovascular diseases.
Our findings reveal a high percentage of elevated BMI, lipid profile alterations, and high blood pressure within the adolescent population. Key risk factors such as a family history of cerebrocardiovascular disease, sedentary lifestyle, and poor dietary habits play a significant role in the increase in weight, blood pressure, and lipid profile alterations in young individuals. These insights emphasize the necessity for targeted public health initiatives to address these issues early on.
The importance of this study extends beyond immediate health benefits. By informing future development policies, our research can help shape comprehensive strategies that promote healthier lifestyles among adolescents. These strategies may include educational programs focused on nutrition and physical activity, community-based interventions to encourage active living, and policies aimed at reducing the consumption of unhealthy foods.
Moreover, investing in preventative measures can alleviate the long-term economic burden on healthcare systems caused by obesity-related diseases. By fostering an environment that supports healthy choices from a young age, we can pave the way for a healthier future generation, ultimately reducing the prevalence of chronic diseases and improving overall public health outcomes.
This study’s cross-sectional nature limits its ability to establish causal relationships between identified risk factors and obesity. This design only provides a snapshot at one point in time, making it difficult to determine whether the risk factors led to obesity or if obesity influenced these risk factors. Longitudinal studies are needed to better understand the temporal dynamics and causality. The study population may not be representative of all adolescents, particularly those from different geographic regions, socioeconomic backgrounds, or cultural contexts. This limitation restricts the generalizability of the findings to broader populations, indicating the need for more diverse and inclusive research to ensure that the results are applicable to a wider demographic.
Therefore, this study not only contributes to the understanding of adolescent obesity but also serves as a foundation for the development of robust, evidence-based policies aimed at combating this pervasive issue. By prioritizing the health of young individuals, we can ensure a healthier, more productive future for our society.
Author Contributions
Conceptualization, P.C. and F.R.; methodology, P.C.; software, E.T.C.; validation, P.C. and F.R.; investigation, M.D.; data curation, E.T.C. and S.M.; writing—original draft preparation, M.D.; writing—review and editing, P.C.; visualization, F.R. and S.M.; supervision, P.C.; project administration, P.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The collection and analytical treatment of data for this study required submission and authorization from the Ethics Committee under code number 28/CE-IPCB/2021, followed by approval from the School Cluster Directorate. Given the study’s human nature, the entire research team respected and ensured compliance with all principles outlined in the Helsinki Declaration. All participants and their guardians had the opportunity to address any questions related to the project’s development. Throughout the process, collected data were coded to protect the identity of individuals.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is not available due to ethical or privacy restrictions.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Leggio, M.; Lombardi, M.; Caldarone, E.; Severi, P.; D’Emidio, S.; Armeni, M.; Bravi, V.; Bendini, M.G.; Mazza, A. The relationship between obesity and hypertension: An updated comprehensive overview on vicious twins. Hypertens. Res. 2017, 40, 947–963. [Google Scholar] [CrossRef] [PubMed]
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Freitas, A.I.; Moreira, C.; Santos, A.C. Time trends in prevalence and incidence rates of childhood overweight and obesity in Portugal: Generation XXI birth cohort. Int. J. Obes. 2019, 43, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.-P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: Summary of the evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef] [PubMed]
- van Sluijs, E.M.F.; Ekelund, U.; Crochemore-Silva, I.; Guthold, R.; Ha, A.; Lubans, D.; Oyeyemi, A.L.; Ding, D.; Katzmarzyk, P.T. Physical activity behaviours in adolescence: Current evidence and opportunities for intervention. Lancet 2021, 398, 429–442. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, L.; Sun, L.; Wang, B.; Yuan, Y.; Gao, H.; Fu, L. Relative children’s lipid accumulation with hypertension in Chinese children and adolescents. BMC Public Health 2021, 21, 1884. [Google Scholar] [CrossRef] [PubMed]
- Gomes, I. A obesidade e a hipertensão arterial em idade pediátrica—A propósito de uma população em crescimento. Rev. Port. Cardiol. 2017, 36, 707–708. [Google Scholar] [CrossRef] [PubMed]
- Direcção-Geral Da Saúde, R.J.; Rito, A.; Breda, J. Catalogação na Fonte: Portugal. Ministério da Saúde. Instituto Nacional de Saúde Doutor Ricardo Jorge e Outro Guia de Avaliação do Estado Nutricional Infantil e Juvenil/Instituto Nacional de Saúde Doutor Guia de Avaliação do Estado Nutricional Infantil e Juvenil. Available online: https://www.insa.min-saude.pt/ (accessed on 10 April 2024).
- Lurbe, E.; Agabiti-Rosei, E.; Cruickshank, J.K.; Dominiczak, A.; Erdine, S.; Hirth, A.; Invitti, C.; Litwin, M.; Mancia, G.; Pall, D.; et al. 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. J. Hypertens. 2016, 34, 1887–1920. [Google Scholar] [CrossRef]
- Soczewka, M.; Kędzia, A.; Skowrońska, B.; Niechciał, E. Importance of diet in children and adolescents with obesity and asthma. Pediatr. Endocrinol. Diabetes Metab. 2024, 30, 91–96. [Google Scholar] [CrossRef]
- Qiao, Y.; Zhu, D.; Zhao, M.; Magnussen, C.G.; Xi, B. Adverse childhood experience, adopting a healthy lifestyle in adulthood, and risk of cardiovascular diseases. J. Affect. Disord. 2024, 362, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Iyun, O.B.; Okobi, O.E.; Nwachukwu, E.U.; Miranda, W.; Osemwegie, N.O.; Igbadumhe, R.; Olawoye, A.; Oragui, C.C.; Osagwu, N.A. Analyzing Obesity Trends in American Children and Adolescents: Comprehensive Examination Using the National Center for Health Statistics (NCHS) Database. Cureus 2024, 16, e61825. [Google Scholar] [CrossRef] [PubMed]
- Mohamad, R.M.A.; Alhawiti, W.M.; Alshehri, W.A.; Alhaj Ali, R.M.; Alhakami, S.T.; Alatawi, M.M.; Almutairi, A.A.; Al Atawi, E.S.; Alkhaibari, D.G.; Saleh, R.M.; et al. Assessment of Adolescents’ Overweight and Obesity Risk Factors Among Alabnaa Schools in Tabuk City, Saudi Arabia. Cureus 2024, 16, e61533. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Ji, Y.; Dong, Y.; Li, Z.; Zhang, Y. The impact of family factors and communication on recreational sedentary screen time among primary school-aged children: A cross-sectional study. BMC Public Health 2024, 24, 1733. [Google Scholar] [CrossRef] [PubMed]
- Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. Pediatrics 2011, 128 (Suppl. 5), S213–S256. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.S.; Samuel, J.P.; Samuels, J.A. Prevalence of Hypertension in Children. Hypertension 2019, 73, 148–152. [Google Scholar] [CrossRef]
- Ribeiro, I.; Coelho, P.; Pereira, A. Estudo de Pressão Arterial em Crianças e Adolescentes; Revista Científica da Escola Superior de Saúde Dr. Lopes Dias: Castelo Branco, Portugal, 2019. [Google Scholar]
- Cabral, E.; Coelho, P.; Barbas, F. Estudo da pressão arterial e do perfil lipídico em crianças e adolescentes. In ANAIS I Seven International Medical and Nursing Congress; Seven Publicações: São José dos Pinhais, Brazil, 2022; Available online: https://repositorio.ipcb.pt/bitstream/10400.11/8104/1/Anais%20do%20Evento%20I%20Seven.pdf (accessed on 10 April 2024).
- Ononamadu, C.J.; Ezekwesili, C.N.; Onyeukwu, O.F.; Umeoguaju, U.F.; Ezeigwe, O.C.; Ihegboro, G.O. Comparative analysis of anthropometric indices of obesity as correlates and potential predictors of risk for hypertension and prehypertension in a population in Nigeria. Cardiovasc. J. Afr. 2017, 28, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Fan, Z.; Liao, Z.; Zong, X.; Zhang, S. Differences in prevalence of prehypertension and hypertension in children and adolescents in the eastern, central and western regions of China from 1991–2011 and the associated risk factors. PLoS ONE 2019, 14, e0210591. [Google Scholar] [CrossRef]
- Zhang, Q.; Yang, L.; Zhang, Y.; Zhao, M.; Liang, Y.; Xi, B. Hypertension Prevalence Based on Three Separate Visits and Its Association with Obesity Among Chinese Children and Adolescents. Front. Pediatr. 2019, 7, 307. [Google Scholar] [CrossRef]
- Muhihi, A.J.; Njelekela, M.A.; Mpembeni, R.N.M.; Muhihi, B.G.; Anaeli, A.; Chillo, O.; Kubhoja, S.; Lujani, B.; Maghembe, M.; Ngarashi, D. Elevated blood pressure among primary school children in Dar es salaam, Tanzania: Prevalence and risk factors. BMC Pediatr. 2018, 18, 54. [Google Scholar] [CrossRef]
- Mohan, B.; Verma, A.; Singh, K.; Singh, K.; Sharma, S.; Bansal, R.; Tandon, R.; Goyal, A.; Singh, B.; Chhabra, S.T.; et al. Prevalence of sustained hypertension and obesity among urban and rural adolescents: A school-based, cross-sectional study in North India. BMJ Open 2019, 9, e027134. [Google Scholar] [CrossRef]
- Rodrigues, P.R.M.; Pereira, R.A.; Gama, A.; Carvalhal, I.M.; Nogueira, H.; Rosado-Marques, V.; Padez, C. Body adiposity is associated with risk of high blood pressure in Portuguese schoolchildren. Rev. Port. Cardiol. 2018, 37, 285–292. [Google Scholar] [CrossRef]
- Figueirinha, F.; Herdy, G.V.H. High Blood Pressure in Pre-Adolescents and Adolescents in Petrópolis: Prevalence and Correlation with Overweight and Obesity. Int. J. Cardiovasc. Sci. 2017, 30, 243–250. [Google Scholar] [CrossRef]
- Marrodán Serrano, M.D.; Cabañas Armesilla, M.D.; Carmenate Moreno, M.M.; de Espinosa, M.G.-M.; López-Ejeda, N.; Martínez Álvarez, J.R.; Prado Martínez, C.; Romero-Collazos, J.F. Association between adiposity and blood pressure levels between the ages of 6 and 16 years. Analysis in a student population from Madrid, Spain. Rev. Esp. Cardiol. 2013, 66, 110–115. [Google Scholar] [CrossRef]
- Reuter, C.P.; Rodrigues, S.T.; Barbian, C.D.; de Castro Silveira, J.F.; de Borba Schneiders, L.B.; Soares, S.S.; Burgos, L.T.; Burgos, M.S. Pressão arterial elevada em escolares: Fatores sociodemográficos e bioquímicos associados. Rev. Port. Cardiol. 2019, 38, 195–201. [Google Scholar] [CrossRef]
- del Bosco Brunetti Cunha, E.; Fagundes, R.P.; Scalabrin, E.E.; Herai, R.H. Evaluation of Lipid Profile in Adolescents. Int. J. Cardiovasc. Sci. 2018, 31, 367–373. [Google Scholar]
- Manios, Y.; Karatzi, K.; Protogerou, A.D.; Moschonis, G.; Tsirimiagou, C.; Androutsos, O.; Lionis, C.; Chrousos, G.P. Prevalence of childhood hypertension and hypertension phenotypes by weight status and waist circumference: The Healthy Growth Study. Eur. J. Nutr. 2018, 57, 1147–1155. [Google Scholar]
- Silva Sidrônio, M.G.; Jeronimo Barros, G.; Trajano, G.A.; Da Silva, A.A.; de Melo, T.R. Análise do Perfil Lipídico de Crianças e Adolescentes em Escola Pública de Natal-RN Análise Do Perfil Lipídico De Crianças E Adolescentes Em Escola Pública De Natal-Rn. 2018, Volume 3322. Available online: https://editorarealize.com.br/artigo/visualizar/40711 (accessed on 10 April 2024).
- da Cunha, C.L.P. Hipertensão Induzida pela Obesidade. Arq. Bras. Cardiol. 2023, 120, e20230391. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Wiklund, O.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188, Erratum in Eur. Heart J. 2020, 41, 4255. [Google Scholar] [CrossRef] [PubMed]
- Okpokowuruk, F.S.; Akpan, M.U.; Ikpeme, E.E. Prevalence of hypertension and prehypertension among children and adolescents in a semi-urban area of Uyo Metropolis, Nigeria. Pan Afr. Med. J. 2017, 28, 303. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kurnianto, A.; Kurniadi Sunjaya, D.; Ruluwedrata Rinawan, F.; Hilmanto, D. Prevalence of Hypertension and Its Associated Factors among Indonesian Adolescents. Int. J. Hypertens. 2020, 2020, 4262034. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).