Abstract
Background: Hallux rigidus (HR) is a common forefoot disorder, and surgical treatment is typically guided by the severity of the condition, as defined by the Coughlin and Shurnas four-grade classification. This study aimed to compare clinical and functional outcomes in patients undergoing first metatarsophalangeal joint arthrodesis (FMTPJA) with or without the use of an interfragmentary (IF) screw in addition to a dorsal plate. Methods: We retrospectively evaluated a cohort of patients who underwent surgery with a FMTPJA, dividing patients in two groups: patients who underwent FMTPJA through dorsal plate associated with an interfragmentary screw (WIS group) and patients who underwent FMTPJA through dorsal plate without an interfragmentary screw (WOIS group). The primary outcomes were analyzed using the FAAM score and FAAM sport score. Secondary outcomes included VAS, patient satisfaction, recovery time to return to sports, and the level of postoperative sports activity compared to preoperative levels. Results: In paired analyses, the WOIS group showed statistically significant improvements in both the FAAM and FAAM sport scores (p = 0.01). In contrast, the WIS group showed significant improvement only in the FAAM sport score (p = 0.01), while the FAAM score did not reach statistical significance (p = 0.42). Multivariate analysis revealed that a higher preoperative FAAM score predicted a higher postoperative FAAM score (p = 0.75), while the use of an IF screw was associated with a lower expected postoperative FAAM score (p = 0.25). Increased BMI and older age were significantly associated with lower postoperative FAAM scores. Conclusions: Both surgical techniques led to significant clinical improvements. However, patients in the WOIS group showed a trend toward faster recovery and higher postoperative sports activity levels, particularly in the athletic population. Although no statistically significant differences were found between groups overall, these findings suggest potential benefits of avoiding an IF screw in selected patients. Further prospective studies are warranted to better delineate the clinical impact of screw usage in FMTPJA.
1. Introduction
Hallux Rigidus (HR) is a common forefoot disorder affecting the great toe, characterized primarily by the loss of dorsiflexion and progressive osteophyte formation at the first metatarsophalangeal joint (FMTPJ). It results in great toe arthritis and a typical dorsal bunion [1]. It is the second most common pathology affecting the FMTPJ after Hallux Varus (HV) and the most common form of osteoarthritis in the foot and ankle region [2].
The etiology of HR is poorly understood. Among the biomechanical causes, many theories on the HR etiology have been proposed, including first ray hypermobility, type of footwear, occupation, mismatch between the metatarsal head and articular surface of the proximal phalanx as a flat or chevron-shaped joint, second ray metatarsal length exceeding that of the first ray, tight Achilles tendon, HV interphalangeus, pes planovalgus or cavus foot posture, HV, metatarsus adductus, and metatarsus primus elevatus [3,4,5,6].
The most common cause for unilateral HR is believed to be acute trauma or repetitive microtrauma. Other non-biomechanical causes are metabolic disorders, neuromuscular causes, rheumatic causes, congenital causes, and iatrogenic causes.
The increased load on the FMTPJ creates limitations in common daily activity and sports. Patients tend to compensate for the altered weightbearing offloading the first ray and the medial column with subsequent pain on the lateral aspect of the foot [7].
The most used and more comprehensive grading system is represented by Coughlin and Shurnas’ four-grade classification:
Grade 0: stiffness and dorsiflexion of 40–60 degrees (loss of 10–20%); normal radiographic findings.
Grade 1: mild pain at extremes of motion and dorsiflexion of 30–40 degrees (20–50% lost); mild dorsal osteophyte and normal joint space on X-Ray.
Grade 2: moderate pain at extremes of motion and dorsiflexion of 10–30 degrees (50–75% lost); moderate dorsal osteophyte and no more than 25% of dorsal joint space involvement on lateral view on X-ray.
Grade 3: significant stiffness and near constant pain, pain at extreme ROM but not at mid-range and dorsiflexion of 10 degrees or less (75–100% lost); severe dorsal osteophyte and more than 25% of dorsal joint space involvement on lateral view on X-Ray.
Grade 4: same ad grade 3 with pain at the midrange of passive motion.
First metatarsophalangeal joint arthrodesis (FMTPJA) is the current “gold standard” of treatment for advanced arthritis of the great toe (grade III-IV according to Coughlin and Shurnas’s classification) and has demonstrated consistently good results in the literature [8].
FMTPJA has better outcomes compared to total arthroplasty [9], hemiarthroplasty [10], interpositional arthroplasty or cheilectomy [11]. The bone fusion guarantees better reduction in pain, shorter hospital stays, lower revision rates, and faster return to normal activity [12].
The technique is frequently used for managing the eventual complications deriving from other surgical treatments. The procedure can be easily performed under 5 mm of bone defect when a direct fusion is possible. If the defect is between 5 and 10 mm, the fusion requires a bone re-balancing of the lateral metatarsal bones; beyond 10 mm, a bone graft is needed to reduce the gap in the length of the first metatarsal. In fact, with an excessive shortening of the first ray, lateral pain occurs due to secondary transfer metatarsalgia, as the weight-bearing is transferred laterally to the lesser metatarsal. The result is an unbalanced metatarsal cascade [13].
Fixation options vary widely and include staples, dorsal locking plates, two cross screws, and dorsal locking plates plus lag screw. Kirschner wires are considered obsolete nowadays.
FMTPJA is a valid procedure for HV in patients affected by rheumatoid arthritis, concomitant HR, failures of HV surgical procedures, and HV in the elderly [14].
The FMTPJA should also be considered as the treatment of choice in rheumatoid arthritis, gout, and post traumatic arthritis affecting the great toe. It is also considered in selected cases of severe HV (with or without signs of degenerative joint disease), with a rather increased intermetatarsal and HV angle, concomitant medial column instability, transfer metatarsalgia, or when seen in elderly patients [15].
FMTPJA is a reliable option for revision after failure of surgical treatment of hallux valgus [16].
The FMTPJA is commonly performed in case of a failed previous HV correction which resulted in recurrent deformity, iatrogenic hallux varus, or avascular necrosis, as well as for salvage after a failed resectional and replacement arthroplasties or failed cheilectomy [17]. We included previous failed HV and hallux varus surgery in our study.
2. Material and Methods
2.1. Study Design and Setting
A retrospective observational study according to the PROCESS guidelines was conducted at three different Italian Hospitals between January 2013 and December 2023. The study respects national ethical standards and the Declaration of Helsinki. Written informed consent for surgical and clinical data collection for scientific purposes was obtained from all patients at the admission and before surgery according to institutional protocol.
Patient demographics and data were recorded in a computerized database.
Inclusion criteria:
- -
- Patient with HR Grade 3–4 according to Coughlin and Shurnas classification;
- -
- Patients of at least 18 years who underwent primary FMTPJA;
- -
- Patients who agreed to sign a consent form to participate in the study;
- -
- Minimum of 12 months of follow up;
- -
- Revision surgery (failed of previous HV surgery) or relapsing HV;
- -
- Hallux varus;
- -
- Rheumatoid arthritis.
Excluding criteria:
- -
- Patients affected by infectious diseases;
- -
- Patients affected by neoplastic diseases.
The main indication for FMTPJA was end-stage osteoarthritis with a failure of conservative treatments.
Three surgeons with deep expertise in foot and ankle surgery performed all the surgical procedures.
Patients were assigned into two groups:
- -
- With interfragmentary screw group (WIS): patients who underwent FMTPJA through dorsal plate associated with an interfragmentary screw (IFS);
- -
- Without interfragmentary screw group (WOIS): patients who underwent FMTPJA with dorsal plate without IFS.
The primary outcomes were analyzed using the Foot and Ankle Ability Measure (FAAM) score and FAAM sport score. The secondary outcomes analyzed were visual analog scale (VAS), patient’s satisfaction, months needed to return to sports activities and post operative sport’s practice level compared to preoperative level.
No patients were lost to follow-up or died.
Clinical Evaluation
All the patients underwent physical examination before surgery. They had a relatively consistent clinical presentation including stiffness asymmetrically affecting dorsiflexion, pain, swelling, altered gait preferring supination of sub-tarsal joint, painful dorsal bump, and FMTPJ pain.
Radiological Evaluation
Weight-bearing AP, lateral, and supine oblique radiographs have been obtained to confirm the diagnosis, to assess the grade of osteoarthritis, and to plan the surgical procedure. We evaluated all the cases as Grade 4 considering clinical and radiological features. We also assessed the osteophytes position and the native axis, considering the possible use of allo/autograft in case of short first MT and unbalanced MT cascade after surgery.
2.2. Surgical Technique
A subarachnoid anesthesia was administered in all cases. All patients received 2 g of Cefazolin intravenously as antibiotic prophylaxis before surgery, unless contraindicated [18]. The patient was placed in the supine position with the foot at the edge of the table. The entire procedure was performed using a thigh tourniquet.
The surgical approach to the FMTPJ was made through a dorsal midline skin incision, which allowed for an expansive approach. Care was taken to preserve the dorsal medial cutaneous nerve, and the extensor hallucis longus tendon was isolated and retracted laterally.
The joint capsule was incised longitudinally along the line of the skin incision, directly down to the bone. The medial and lateral collateral ligaments were released on both sides. The soft tissue was reflected and protected; the proximal phalanx, metatarsal, and sesamoids were debrided, and osteophytes were removed using an osteotome and scalpel.
Cup and cone reamers were used to prepare the convex and concave surfaces of the metatarsal and phalanx. A guide wire was inserted into the center of the articular surface, and reaming began after fluoroscopic confirmation.
The joint was reduced and checked via fluoroscopy. We aimed for 0°, 5°, or 10° of dorsiflexion relative to the floor, 0° of rotation, and 5° of valgus, considering the patient’s demands and anticipated future footwear, such as high heels.
In the WIS group, an interfragmentary headless compression screw, with a diameter of 3.5 mm, was placed across the MTPJ from distal medial to proximal lateral, to achieve interfragmentary and cross-joint compression (Figure 1). The locking plate was then applied dorsally as a neutralization plate. In the WOIS group, interfragmentary compression was achieved through the oval hole in the same locked dorsal plate (Figure 2).

Figure 1.
Postoperative X rays in the WIS group in two projections: Anteroposterior (a) and Lateral (b).
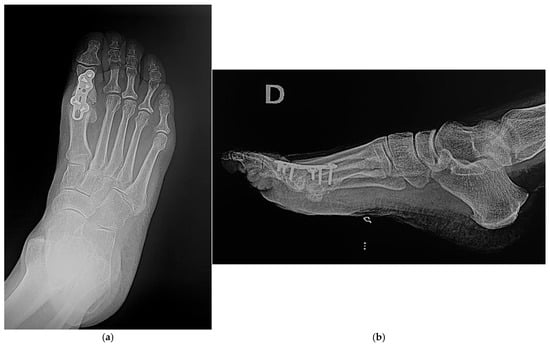
Figure 2.
Postoperative X rays in the WOIS group in two projections: Anteroposterior (a) and Lateral (b).
Fluoroscopic images were obtained to verify the correct positioning of the plate and screws. Meticulous hemostasis was maintained to prevent postoperative hematoma and reduce complications. The tissues were copiously irrigated, and the layers were closed separately.
2.3. Postoperative Care
All patients were allowed immediate progressive weight bearing in an off-loading boot, rigid-soled post-surgical shoe for 6 weeks. After this period, full weight bearing is permitted with regular footwear. Sequential AP, lateral, and oblique radiographs should be obtained to monitor healing at the fusion site and to ensure that the position of the reconstruction remains appropriate.
3. Results
A total of 27 patients were considered eligible according to the inclusion and exclusion criteria and were finally enrolled for this study. A total of 16 patients were assigned to the WIS group, and 11 patients were assigned to the WOIS group.
Anagraphic data regarding patients enrolled for this study can be found in Table 1.

Table 1.
Population’s anagraphic data, preoperative diagnosis, operating time, and complication rate. WIS: Patients treated with interfragmentary screw; WOIS: patients treated without interfragmentary screw; BMI: Body Mass Index; F: female; M: male.
A total of 12 surgeries were performed on the right foot and 15 surgeries on the left foot. Of the 27 enrolled patients who underwent FMTPJA, 15 patients presented a diagnosis of relapsing HV, 11 patients presented HR, and only 1 patient presented a diagnosis of hallux varus.
We noticed a statistically significant higher prevalence of patients with a diagnosis of relapsing HV in the WIS group compared to the WOIS group (p value: 0.02).
Out of the 27 FMTPJA performed, 24 were performed using a dorsi-flexed plate while the remaining three arthrodesis were performed using a plate at 0° of dorsi-flexion. All patients included in the WIS group were treated with 1 IFS. A total of 18 patients out of the 27 patients enrolled did not practice any sport, and the remaining 9 patients practiced amatorial sports activities with a higher functional demand. The sports activities practiced by the athletic population include pilates, stationary cycling, and water aerobics. All these activities were considered comparable in terms of functional demands.
The mean time from the onset of symptoms to surgery was 9.88 years (±7.41) with no statistically significant difference between the two groups (p value: 0.9). A total of 18 patients had previously received surgery on the affected foot, with no statistically significant difference in revision surgery between the two groups. The mean operating time was 91.67 min (±16.78). The overall preoperative VAS was 6.65 (±2.60), the preoperative VAS was 6.07 (±3.2) in the WIS group and 7.45 (±1.44) in the WOIS group. The overall postoperative VAS was 1.62 (±2.72); the WIS group presented a mean VAS of 1.87 (±2.9), while the WOIS group reported a mean VAS of 1.3 (±2.5) (Table 2). (p value: 0.5).
Table 2.
Clinical and functional outcomes; WIS: Patients treated with interfragmentary screw; WOIS: patients treated without interfragmentary screw; Pre op: pre-operative; Post op: post operative; FAAM Score: Foot and Ankle Ability Measure; VAS: Visual Analogue Scale.
The functional outcome was mainly evaluated using the FAAM score and FAAM sports score. The overall mean preoperative FAAM score was 0.70 (or 70%) ± 0.13. The WIS group presented a mean preoperative FAAM score of 0.72 (±0.14) while the WOIS group presented a mean preoperative FAAM score of 0.65 (±0.09); (p value: 0.1). The overall mean postoperative FAAM score was 0.81 (±0.20), the WIS group presented a mean postoperative FAAM score of 0.77 (±0.23). On the other hand, the WOIS group presented a mean postoperative FAAM Score of 0.85 (±0.16). This difference is not statistically significant (p value: 0.3). Of the nine patients practicing sport at an amateur level, three patients belonged to the WIS group and six patients belonged to the WOIS group. The overall preoperative FAAM sports score was 0.37 (±0.17); the WIS group presented a mean preoperative FAAM sports score of 0.29 (±0.18), while the mean preoperative FAAM sports score in the WOIS group was 0.42 (±0.15). The overall postoperative FAAM sports score was 0.84 (±0.12); the WIS group presented a postoperative FAAM sports score of 0.87 (±0.1) and the WOIS group presented a postoperative FAAM sports score of 0.81 (±0.13) (Table 2). Finally, we made a paired analysis comparing the preoperative FAAM score to the post operative FAAM score and the preoperative FAAM sports score to the postoperative FAAM sports score. From the paired analysis of the overall population, we noticed a statistically significant improvement in both the FAAM score (p value: 0.01) and FAAM sports score (0.001).
We also made a further distinction between the paired WIS group and paired WOIS group and it emerged that only the paired WOIS group had a statistically significant improvement in both the FAAM score (p value: 0.0123) and FAAM sports score (p value 0.0184). On the other hand, the paired WIS group presented a statistically significant improvement in the FAAM sports score (p value: 0.0175), while the improvement of the FAAM score was not statistically significant ( p value: 0.4213) (Table 2).
Patients practicing amateur sport could return to their sport activities after 4.33 months (±1.83), the WIS group returned to sport activities after 4.4 months (±2.5) while the WOIS group after 4.2 months (±1.2). During the follow up visits, patients were asked to express their capacity of practicing their usual sport activity by providing a number from 0 (inability to practice their sport) to 10 (practice the sport at the same level as before the onset of the symptomatology); the overall mean value was 8.08 (±3.09). The WIS group of patients reported a mean score of 6.17 (±3.7). while the WOIS group presented a mean score of 10 (±0). This result is statistically significant (p value: 0.03). Finally, we performed a multivariate analysis to better understand what factors influenced the postoperative FAAM score the most including the preoperative FAAM Score (FAAM T0), the usage of a screw, the Body Mass Index and patient’s age.
By the data we collected it emerged that an increase in the FAAM T0 determines an expected increase in the postoperative FAAM score (p value: 0.75), while the usage of a screw to perform the arthrodesis provides an expected lower postoperative FAAM Score (p value: 0.25).
On the other hand, when a patient’s BMI and age increase there is a statistically significant reduction in the postoperative FAAM Score; so, the lower the BMI and the younger the patients, the better the postoperative FAAM score (Table 3).
Table 3.
Multivariate analysis to evaluate the main determinants of the post operative FAAM score; FAAM T0: Pre-operative Foot and Ankle Ability Measure; BMI: Body Mass Index.
We observed four complications: one pseudoarthrosis, two wound dehiscences, and one neurological damage. Only four patients removed the means of synthesis.
Radiologic Results
The x-rays were examined for union (at least 3 bridging cortices), time to union, hardware failure, or other radiographic complications. Only one patient belonging to the WIS group presented pseudoarthrosis at the latest follow up visit.
The mean preoperative HV angle was 36.6° in the WIS group and 32.8° in the WOIS group. The mean postoperative HV angle was 14.1° in the WIS group and 16.8° in the WOIS group without a statistically significant difference between the two groups (p value: 0.2)
The mean preoperative intermetatarsal angle was 16.7° in the WIS group and 15.4° in the WOIS group, while the mean postoperative intermetatarsal angle was 11.3° in the WIS group and 10.2° in the WOIS group. Also, in this case, no statistically significant difference was observed in the two groups (p value: 0.4).
The mean postoperative dorsiflexion angle was 32.1° in the WIS group and 31.4° in the WOIS group (p value: 0.5). At 12 months after surgery, the radiographic control showed that the dorsiflexion angle was 29.6° in the WIS group and 27.3° in the WOIS group (p value: 0.12).
The WIS group showed a minor modification of the dorsiflexion angle over months, while the WOIS group reported a major decrease in dorsiflexion angle compared to the pre-operative.
4. Discussion
Hallux alignment is fundamental after FMTPJA since more than 50% of body weight is transferred through the hallux during the cycle gait. The incorrect position of the joint modifies the weight-bearing, resulting in overloading the lesser metatarsals with consequent hyperkeratosis and further biomechanical derangement.
Correct joint preparation, good compression, and rigid stabilization are the keys to achieving good clinical results.
In 1993, Curtis et al. concluded that the use of conical reamers in preparation of the bone with a supplementary lag screw provides stronger fixation than other techniques of plantar joint fixation such as K wires, plates, or interfragmentary screws. He stated a single lag screw fixation is significantly stronger than a dorsal plate alone [19].
In 2010, Kumar et al. demonstrated high rates of osseous fusion using a low-profile dorsal titanium plate with contoured dorsiflexion angles of 5 to 10 degrees and a lag screw [20].
Dening et al. evaluated FMTPJ bone fusion at 6 weeks in different subgroups of patients treated with different fixation methods to identify the clinically superior one. The joint was fixed using one of the following methods: an oblique cannulated self-tapping lag screw positioned from medially to laterally, two crossed cannulated self-tapping lag screws, a pre-contoured dorsal plate or a pre-contoured dorsal plate augmented with a plantar 2.7 mm, cannulated, self-tapping lag screw. The result was better for the FMTPJA performed with a low-contoured dorsal plate alone with a fusion rate of 100% [21].
A significant reduction in interfragmentary motion and faster fracture healing was demonstrated when an interfragmentary lag screw was used in a locking plate construct. According to Claes LE et al., a compression screw with a neutralization plate is a more stable and less flexible construct than sole bridge plating, leading to faster fracture healing since interfragmentary screws limit interfragmentary movement [22].
In our study, we found no statistically significant differences in the union rates between the WIS group and WOIS group.
Only one patient with a diagnosis of relapsing hallux valgus belonging to the WIS group presented a nonunion of the FMTPJ at the latest follow-up visit. In our study, the union rate was 93% in the WIS group and 100% in the WOIS group.
The interfragmentary compression screw allows joint compression while the dorsal plate acts as a locked plate granting a more secure fixation with a reduced need for non-weight-bearing protection.
A 2 mm axial interfragmentary movement is usually assumed as a critical value above which the bone formation process may be delayed or even suppressed since the opening and transverse displacements between the metatarsal bone and proximal phalanx bones generate a state of tension and shear in the callus area resulting in four times lower vascularization and two times lower bone formation compared to compression strain obtained with a stable arthrodesis [23].
In a study on the stability of FMTPJA using a lag screw in addition to a medial plate, Daszkiewicz K et al. reported that the lag screw increases stiffness and reduces transverse displacements enhancing the healing process of the FMTP joint arthrodesis since stiffer fixation is advantageous for smaller gaps arthrodesis. On the other hand, an excessively stiff arthrodesis using an IFS with a displacement lesser than 0.1 mm may suppress the bone growth delaying bone healing underneath the locking plate [24].
In our study, we only reported one case of nonunion in a female patient belonging to the WIS group. This patient presented a BMI of 18.37, no surgical site infections, no radiological signs of osteoporosis and no past medical history of systemic conditions predisposing to nonunion, so an excessively stiff arthrodesis may be the reason behind the one case of nonunion reported.
Brent Cone et al. [25] examined the union rate and dorsiflexion ranges in 99 patients undergoing FMTPJ fusion. They reported the use of an IFS in addition to a dorsal plate is associated with a significantly lower reduction in the dorsiflexion angle compared to FMTPJ fusion using only the dorsal plate and no significant differences in union rates between the two groups.
This data aligned with our results since patients treated with dorsal plate and IFS presented a lower reduction in the dorsiflexion angle.
In 2024, E. García-Jarabo et al., in a retrospective study, found better results in terms of complications and consolidation rates in patients treated with IFS and locking plate to perform the arthrodesis compared to those cases in which the IFS was not used, with the degree of dorsiflexion being a risk factor for developing pseudarthrosis; this result is consistent with the previous literature, though E García-Jarabo et al. did not use a functional score to investigate the return to sport activity [26].
Through the data collected, it emerged that patients belonging to the WOIS group present a better FAAM score than patients belonging to the WIS group, with no statistically significant difference between the two groups. On the other hand, the WIS group presented a better FAAM sports score compared to the WOIS group even though the WOIS group reported a higher level of sport practice compared to the WIS group. Even if these data may seem to be at odds with each other, they can be explained by the fact that the interfragmentary screw may cause discomfort in patients practicing sport activities. This study has several limitations, first the retrospective aspect of the study represents a limitation itself. Another limitation is represented by the relatively small number of patients included in this study. Also, the follow up period does not allow for a proper evaluation of long term outcomes and complications. The study was conducted in three different centers over a period of 10 years, which prevents a fully standardized assessment of the outcomes. To mitigate this effect, all procedures were performed by experienced foot and ankle surgeons using standardized techniques. Finally, we compared the outcomes of FMTPJA in patients with different diagnoses, so the heterogeneity of the starting diagnosis represents a limitation of the study.
5. Conclusions
In this study, we found a statistically significant clinical improvement after surgery in both the WIS and WOIS group with no statistically significant differences between the two groups. In the WIS group, we found a higher prevalence of patients with a relapsing HV since the IFS may help to better handle deformity, though revision surgery is not a criterion of choice between IFS utilization. In addition, in post operational recurrences, the use of IFS may be recommended for its capacity to maintain dorsiflexion angle and improve stability.
Finally, this study suggests a faster recovery and a higher sport’s practice level in the sportive population treated without IF screw, although the sample size of the patients practicing sports activities is small. Further studies should be conducted to deepen the two surgical techniques for FMTPJA.
Author Contributions
Conceptualization and methodology, R.V., F.F. and G.M. (Giulio Maccauro); validation, G.M. (Guglielmo Miele); formal analysis, R.V., P.R., G.M. (Guglielmo Miele) and A.D.F.; investigation, G.M. (Guglielmo Miele), S.P., A.d.S. and A.S.; writing—original draft preparation, G.M. (Guglielmo Miele), P.R., S.P. and A.d.S.; writing—review and editing, G.M. (Guglielmo Miele), P.R. and A.S.; visualization, G.M. (Guglielmo Miele), S.P., A.d.S. and A.D.F.; supervision, G.M. (Giulio Maccauro), R.V., A.S., P.R. and A.D.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Orthopedic and Traumatology Institute of Università Cattolica del Sacro Cuore—Roma. As this is approval from the Review Board of Orthopedic and Traumatology Institute, there is no code. The approval date is the session of 22 June 2023.
Informed Consent Statement
Written informed consent was provided by the patient (and/or his/her parents) for permission to receive therapy and to publish this case series.
Data Availability Statement
Datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request (dr.andreadefazio@gmail.com).
Acknowledgments
All the authors approved the submitted version (and version substantially edited by journal staff that involves the author’s contribution to the study) and agree to be personally accountable for the author’s own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and documented in the literature.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HV | Hallux Valgus |
| HR | Hallux rigidus |
| FMTPJ | First metatarsophalangeal joint |
| FMTPJA | First metatarsophalangeal joint arthrodesis |
| WOIS | Without interfragmentary screw |
| WIS | With interfragmentary screw |
| IFS | Interfragmentary screw |
| FAAM | Foot and Ankle Ability Measure |
| VAS | Visual analog scale |
References
- Acker, A.S.; Mendes de Carvalho, K.A.; Hanselman, A.E. Hallux Rigidus: Update on Conservative Management. Foot Ankle Clin. 2024, 29, 405–415. [Google Scholar] [CrossRef]
- Moberg, E. A simple operation for hallux rigidus. Clin. Orthop. Relat. Res. 1979, 142, 55–56. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, M.J.; Shurnas, P.S. Hallux rigidus: Grading and long-term results of operative treatment. J. Bone Jt. Surg. Am. 2003, 85, 2072–2088. [Google Scholar] [CrossRef] [PubMed]
- Drago, J.J.; Oloff, L.; Jacobs, A.M. A comprehensive review of hallux limitus. J. Foot Surg. 1984, 23, 213–220. [Google Scholar] [PubMed]
- Yee, G.; Lau, J. Current concepts review: Hallux rigidus. Foot Ankle Int. 2008, 29, 637–646. [Google Scholar] [CrossRef]
- Bingold, A.C.; Collins, D.H. Hallux rigidus. J. Bone Jt. Surg Br. 1950, 32-B, 214–222. [Google Scholar] [CrossRef]
- Shurnas, P.S. Hallux rigidus: Etiology, biomechanics, and nonoperative treatment. Foot Ankle Clin. 2009, 14, 1–8. [Google Scholar] [CrossRef]
- Deland, J.T.; Williams, B.R. Surgical management of hallux rigidus. J. Am. Acad. Orthop. Surg. 2012, 20, 347–358. [Google Scholar] [CrossRef]
- Gibson, J.N.; Thomson, C.E. Arthrodesis or total replacement arthroplasty for hallux rigidus: A randomized controlled trial. Foot Ankle Int. 2005, 26, 680–690. [Google Scholar] [CrossRef]
- Raikin, S.M.; Ahmad, J.; Pour, A.E.; Abidi, N. Comparison of arthrodesis and metallic hemiarthroplasty of the hallux metatarsophalangeal joint. J. Bone Jt. Surg. Am. 2007, 89, 1979–1985, Erratum in: J. Bone Jt. Surg. Am. 2008, 90, 384. [Google Scholar] [CrossRef]
- Emmons, B.R.; Carreira, D.S. Outcomes Following Interposition Arthroplasty of the First Metatarsophalangeal Joint for the Treatment of Hallux Rigidus: A Systematic Review. Foot Ankle Orthop. 2019, 4, 2473011418814427. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McNeil, D.S.; Baumhauer, J.F.; Glazebrook, M.A. Evidence-based analysis of the efficacy for operative treatment of hallux rigidus. Foot Ankle Int. 2013, 34, 15–32. [Google Scholar] [CrossRef]
- Winters, B.S.; Czachor, B.; Raikin, S.M. Metatarsophalangeal Fusion Techniques with First Metatarsal Bone Loss/Defects. Foot Ankle Clin. 2015, 20, 479–491. [Google Scholar] [CrossRef]
- Tourné, Y.; Saragaglia, D.; Zattara, A.; Maire, J.P.; Picard, F.; Montbarbon, E.; Charbel, A. Hallux valgus in the elderly: Metatarsophalangeal arthrodesis of the first ray. Foot Ankle Int. 1997, 18, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Koutsouradis, P.; Savvidou, O.D.; Stamatis, E.D. Arthrodesis of the first metatarsophalangeal joint: The “when and how”. World J. Orthop. 2021, 12, 485–494. [Google Scholar] [CrossRef]
- Grimes, J.S.; Coughlin, M.J. First metatarsophalangeal joint arthrodesis as a treatment for failed hallux valgus surgery. Foot Ankle Int. 2006, 27, 887–893. [Google Scholar] [CrossRef]
- Schuh, R.; Trnka, H.J. First metatarsophalangeal arthrodesis for severe bone loss. Foot Ankle Clin. 2011, 16, 13–20. [Google Scholar] [CrossRef]
- Ziranu, A.; Lillo, M.; Fantoni, M.; Maffulli, N.; Maccauro, G. Single dose cefazolin is safe and effective for pre-operative prophylaxis in orthopaedic oncology. J. Biol. Regul. Homeost. Agents 2018, 32 (Suppl. S1), 45–49. [Google Scholar] [PubMed]
- Curtis, M.J.; Myerson, M.; Jinnah, R.H.; Cox, Q.G.; Alexander, I. Arthrodesis of the first metatarsophalangeal joint: A biomechanical study of internal fixation techniques. Foot Ankle 1993, 14, 395–399. [Google Scholar] [CrossRef]
- Kumar, S.; Pradhan, R.; Rosenfeld, P.F. First metatarsophalangeal arthrodesis using a dorsal plate and a compression screw. Foot Ankle Int. 2010, 31, 797–801. [Google Scholar] [CrossRef]
- Dening, J.; van Erve, R.H. Arthrodesis of the first metatarsophalangeal joint: A retrospective analysis of plate versus screw fixation. J. Foot Ankle Surg. 2012, 51, 172–175. [Google Scholar] [CrossRef]
- Horn, C.; Döbele, S.; Vester, H.; Schäffler, A.; Lucke, M.; Stöckle, U. Combination of interfragmentary screws and locking plates in distal meta-diaphyseal fractures of the tibia: A retrospective, single-centre pilot study. Injury 2011, 42, 1031–1037. [Google Scholar] [CrossRef]
- Claes, L.E.; Meyers, N. The direction of tissue strain affects the neovascularization in the fracture-healing zone. Med. Hypotheses 2020, 137, 109537. [Google Scholar] [CrossRef]
- Daszkiewicz, K.; Rucka, M.; Czuraj, K.; Andrzejewska, A.; Łuczkiewicz, P. Effect of lag screw on stability of first metatarsophalangeal joint arthrodesis with medial plate. PeerJ 2024, 12, e16901. [Google Scholar] [CrossRef]
- Cone, B.; Staggers, J.R.; Naranje, S.; Hudson, P.; Ingram, J.; Shah, A. First Metatarsophalangeal Joint Arthrodesis: Does the Addition of a Lag Screw to a Dorsal Locking Plate Influence Union Rate and/or Final Alignment after Fusion. J. Foot Ankle Surg. 2018, 57, 259–263. [Google Scholar] [CrossRef]
- García-Jarabo, E.; Alonso-Tejero, D.; Ramos-Ramos, L.M.; Hernanz-González, Y.; Rico, J.V.Y. Better results in consolidation of hallux metatarsophalangeal arthrodesis with dorsal plate and interfragmentary compression screw. Rev. Esp. Cir. Ortop. Traumatol. 2024, 68, 351–357, (In English, Spanish). [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).